Despite new diagnostic methods and expanded vaccination programmes, many children in Uganda continue to suffer from severe brain infections. This is shown in a new study from Karolinska Institutet, published in The Lancet Regional Health – Africa. The researchers’ analysis highlights simple clinical signs that can help healthcare providers more quickly identify children at high risk of death.
The study followed 212 children aged 0 to 12 who were treated for suspected central nervous system infections at two hospitals in southwestern Uganda. Fifteen per cent of the children died during hospitalisation, and 18 per cent were discharged with neurological disabilities such as seizures or muscle weakness. Malaria and the bacterium Streptococcus pneumoniae were the most commonly identified causes.
Simple observations can provide crucial information
“Our results show that even in settings where advanced diagnostics are not always available, simple clinical observations can provide crucial information about which children are in greatest need of rapid care,” says Phuthumani Mlotshwa, doctoral student at the Department of Global Public Health and the study’s first author.
The infections were caused by several different microorganisms. Malaria was detected in 20 per cent of the children, and bacteria in the cerebrospinal fluid in 11 per cent. For nearly half of the cases, no specific pathogen could be identified, which the researchers say underscores the need for improved diagnostic tools.
“The combination of high mortality and significant disabilities among survivors shows that we need to strengthen prevention, diagnostics, and follow-up,” says Giulia Gaudenzi, researcher at the same department and the study’s senior author.
Most children with a severely broken wrist can be treated without surgery, according to a major NIHR-funded UK trial led by researchers at the University of Oxford. The findings suggest that a non-surgical, cast-first approach delivers similar long-term recovery while reducing the risks associated with surgery and costs.
Broken wrists are among the most common injuries in children accounting for about half of children’s fractures. Severely displaced distal radial fractures, where the bones move out of place, are often routinely treated with surgery. However – unlike adults – children have a remarkable ability to straighten broken bones, in a process called remodelling.
Researchers questioned whether a plaster cast would achieve the same long-term result without exposing children to the risks of an operation.
Professor Matt Costa, senior author and Professor, Orthopaedics Trauma Surgery at the Kadoorie Institute, University of Oxford said: ‘These fractures can look very severe on an X-ray, which has traditionally led to surgery to straighten the bone. But because children’s bones are still growing, they have a remarkable capacity to heal. Until now, there has been limited high-quality evidence on whether surgery was always necessary.’
The CRAFFT trial (Children’s Radius Acute Fracture Fixation Trial) was funded by the National Institute for Health and Care Research (NIHR) and supported by the NIHR Biomedical Research Centre: Oxford. It recruited 750 children aged 4–10 from 49 hospitals across the UK. Participants were randomly assigned to receive either surgical fixation or treatment with a plaster cast.
Patients were measured at regular intervals against a set of criteria. At three months, children who had surgery reported slightly better arm function, but the difference between groups was very small. By six and 12 months, there was no difference in recovery, suggesting that early advantages with surgery do not persist.
There were complications following surgery, including infections, scarring and nerve irritation. Non-surgical treatment, which avoids anaesthesia and operative intervention, was shown to reduce NHS costs by around £1,600 per patient on average.
The trial was designed with input from families, who helped define what level of improvement would be meaningful enough to warrant surgery. The observed difference between treatments fell below this threshold.
Professor Dan Perry, NIHR Research Professor and Children’s Orthopaedic Surgeon at Alder Hey Children’s Hospital and the University of Liverpool, and lead author, said: ‘It is astonishing that children have the ability to grow bent, broken bones straight again. It really is a superpower that is unique to children. From both a clinical and health system perspective, these findings are important. Adoption of these results could reduce the number of children exposed to the risks of anaesthesia and surgery, and ease pressure on healthcare services without compromising recovery.’
The results, published in The Lancet, support wider adoption of a cast-first approach for most children with these injuries.
Recently published research from the University of Oklahoma and the University of Tulsa proposes a new model to explain why nightmares can persist over time in children and how therapy can be designed to break that cycle.
The study, published in Frontiers in Sleep, introduces the DARC-NESS model, a mnemonic for the factors that can keep a child stuck in chronic nightmares. At the centre of the model is “nightmare efficacy,” or the idea that children can learn skills to rid themselves of nightmares and restore good sleep.
“The DARC-NESS model looks at the mechanisms of what is maintaining nightmares, as well as the mechanisms that can break the cycle of nightmares,” said Lisa Cromer, PhD., a professor of psychology at the University of Tulsa and a volunteer child psychiatry faculty member at the OU School of Community Medicine in Tulsa. “It’s a child’s response to a nightmare that causes the chronic nightmares to happen, which means if we can learn to respond to nightmares differently, then we can interrupt that cycle. It’s empowering to understand that we can take steps to master our dreams.”
Rather than focusing only on the content of a nightmare, the model encourages clinicians to consider a broader set of factors, including how a child interprets the dream, worries about going to sleep, experiences anxiety at bedtime and copes after waking.
That information can help guide a personalized treatment plan instead of a one-size-fits-all approach. For some children, treatment may focus on reducing bedtime anxiety. Others may benefit from improving sleep habits or participating in exposure-based therapy, such as describing, writing about or drawing the nightmare and then working with a clinician to “rewrite” it.
“We believe we have created a way to conceptualize why nightmares persist and how we can better treat them in kids,” said OU Health child and adolescent psychiatrist Tara Buck, MD, an associate professor at the OU School of Community Medicine in Tulsa. “What’s unique about the model is that it’s customisable to what the patient needs, and it focuses on what the patient can control. We look for the potential intervention points and target those in a collaborative way with patients and their families.”
Unlike insomnia, in which people fear they won’t sleep, children with chronic nightmares are afraid they will sleep. According to Buck, helping children build confidence in their ability to address nightmares can have benefits far beyond sleep.
“Self-efficacy is at the heart of the model,” she said. “When children feel empowered to do something about the nightmares, they begin to see how things are interconnected – because they’re sleeping better, they have more energy, they go to school more consistently and their parents report improved behaviour.”
The model is designed for use by a range of clinicians, including therapists and pediatricians. For many years, health care providers either assumed that nightmares couldn’t be treated or that they would go away if an underlying trauma or mental health condition were addressed. However, that’s not always the case.
“We’ve worked with children who have been in mental health treatment for a long time and their nightmares are still persistent,” Buck said. “There is a need for a nightmare treatment model to help children when their nightmares are recurrent and distressing.”
“A nightmare is a bad dream that you wake up from,” Cromer said. “If you don’t wake up, then the brain is doing its job of resolving the fear of the dream. But if a child does wake up, they’re trying to escape the nightmare. And when a child wakes up, they’re not able to resolve the nightmare, which actually exacerbates the problem. That’s why nightmares are so important to treat.”
Strong evidence ties early language difficulties to later adjustment challenges. Can environmental factors make these problems worse? In a new study, FAU researchers, in collaboration with Aarhus University in Denmark, find that unsupervised or “solo” screen time worsens the behavioural and emotional challenges confronting young children with limited language skills. A total of 546 4- to 5-year-old children from 24 childcare centres in Denmark were followed for six months. Investigators assessed their language abilities, behavioural adjustment and the amount of time the children spent watching screens alone.
The study findings, published in the journal Research on Child and Adolescent Psychopathology, found that solitary screen time acts as an amplifier, exacerbating conduct problems in children with poor communication skills and low productive vocabulary. The results highlight the critical role of the home learning environment in early childhood development. For children who struggle with language skills, time spent alone with a screen is time not spent mitigating risks through healthy social engagement with parents or friends.
Early problems with language can have a lasting negative impact on social and emotional development. Building on this foundation, a new groundbreaking study from Florida Atlantic University and Aarhus University in Denmark tests the hypothesis that unsupervised, solitary screen time during early childhood increases the likelihood that language difficulties will lead to socioemotional difficulties.
The study, published in Research on Child and Adolescent Psychopathology , found that pathways from poor communication skills and low productive vocabulary to later adjustment problems were particularly strong among preschool- and kindergarten-aged children who averaged at least 10 to 30 minutes of solitary screen time per day across the course of a week.
Study participants were 546 4- and 5-year-olds (264 girls, 282 boys) attending 24 population-based childcare centers across 13 municipalities in Denmark. Teachers completed assessments twice of child adjustment difficulties, such as conduct and emotional problems, over the course of about six months during a single school year. At the outset, teachers administered standardized tests of child language abilities, including communication skills and productive vocabulary. Parents reported on solitary screen time, which was defined as the average number of hours per week that children spent alone viewing handheld devices or television, excluding screen time supervised by or consumed with an adult.
Consistent with several previous studies, there were longitudinal associations from oral language problems to later adjustment difficulties. Across the six-month period, poor communication skills and high levels of solitary screen time separately predicted escalating emotional difficulties.
Unique to this study was the finding that solo screen time magnified problems arising from language difficulties. Associations from low productive vocabulary and poor communication skills to increases in conduct problems were strongest among children whose parents reported that their children were well above average in solitary screen time exposure.
“Unsupervised screen time forecloses opportunities for social engagement that might mitigate the behavioral risks that follow from language problems,” said Brett Laursen, Ph.D., senior author and a professor of psychology in FAU’s Charles E. Schmidt College of Science.
Laursen uses an economics model to explain the results. Economists define opportunity costs as losses attached to a choice. If an adult stays up late with a book, the opportunity cost of reading is a good night’s sleep.
“The opportunity costs of solitary screen time can be particularly steep for vulnerable youth. Children have a finite number of free time hours in a day,” said Laursen. “Every hour a child spends alone with a device is an hour they aren’t engaged in social interactions that boost language skills. It is an hour not spent practicing the social and emotional skills required to build friendships. Screens don’t demand compromise, sharing or dialogue – the exact skills that children with communication difficulties need to practice.”
Young children learn language from in-person interactions – very little is acquired from video screens. Further, electronic media cannot replace the rich social experiences children gain from play and engagement with peers.
“Young children with limited language skills are already at risk for social and emotional challenges,” said Molly Selover, lead author and an FAU doctoral student in psychology. “There is little reason to expect that screens help children overcome the adaptive challenges posed by oral language problems and many reasons to suspect that they make matters worse.”
Excessive screen use by young children is widespread: the World Health Organization recommends no more than one hour per day for children ages 2 to 5, yet a global review found that two-thirds of households exceed this limit. In the United States, about half of young children spend more than two hours a day on screens during the week, with even higher use on weekends. Of course, both content and supervision matter.
For children ages 2 to 5, the American Psychological Association encourages parents to limit screen time to no more than one hour per day and to co-view and interact with their children during this time rather than using the screen as a babysitter. They also note that the quality of the content on screens is extremely important, perhaps more important than the total amount of time spent viewing.
The authors say that high caliber content has documented benefits for children, especially as children get older. Unfortunately, when left to their own devices, many young children prefer fast-paced, brief and highly stimulating content, some of which may be age-inappropriate.
“Electronic media is as an integral component of the home learning environment; many children spend more time with tablets and phones than with toys, books and friends,” said Selover. “Like other home environment risks, solitary screen time poses a unique peril to young children with heightened vulnerabilities. Adults tend to think of screens as pleasant distractions and may use them as convenient babysitters. But for preschool children with language vulnerabilities, unsupervised screen time is not benign – it can be an active barrier to well-being.”
The authors acknowledge that their findings may not be popular. Screens are a ubiquitous part of everyday life. Nevertheless, they encourage parents to carefully scrutinize how young children engage screens.
“The findings matter because they show that an all-too-common environmental risk – elevated solitary screen time – can worsen behavioural and conduct challenges for children who face an already difficult developmental path,” Selover said.
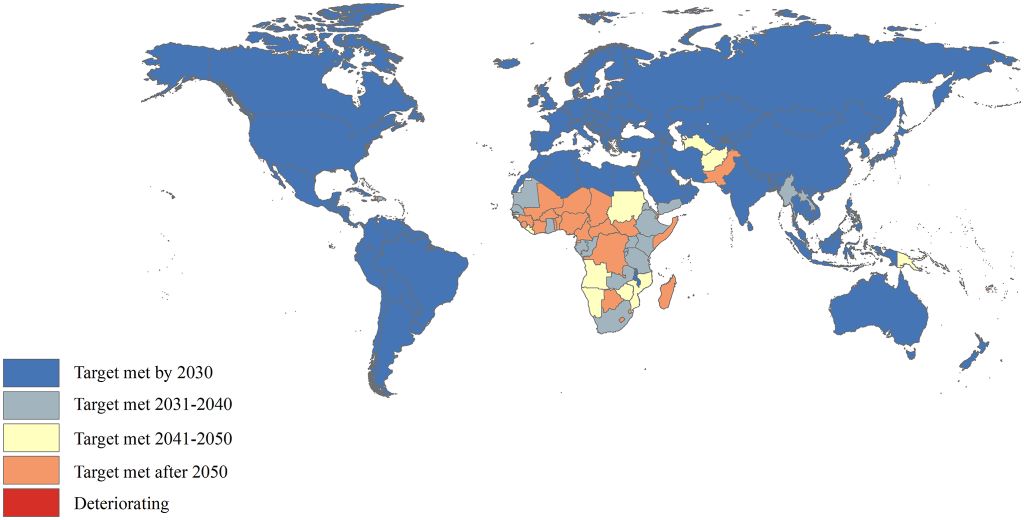
Despite a 63% drop in under-five deaths since 1990, more than a quarter of countries won’t reach the UN’s 2030 child mortality target on time, with sub-Saharan Africa lagging the most
Years in which the U5MR reduction target is expected to be achieved. U5MR: under-5 mortality rate. Image credit: Cao et al., 2026, PLOS One, CC-BY 4.0
A new study tracking global progress on child mortality finds that the world will miss a key United Nations (UN) health target by at least five years at current rates, with the burden falling heavily on Sub-Saharan Africa. The findings are published on April 1, 2026, in the open-access journal PLOS One by Min Liu of Peking University, Beijing, China, and colleagues.
The UN’s Sustainable Development Goal 3.2 calls for all countries to reduce the mortality rate for children under five to fewer than 25 deaths per 1000 live births by 2030. As that deadline approaches, there has been no comprehensive assessment of where countries stand.
In the new study, researchers used data from the UN to analyse annual under-five death counts and mortality rates from 1990 to 2023 across 200 countries and territories. They calculated the rate of change in mortality over time and used those trends to project when those countries still above the target threshold would be expected to reach it.
The researchers found that globally, under-five deaths fell by 63% over the study period – from nearly 13 million in 1990 to 4.78 million in 2023 – and the mortality rate dropped by an average of 3.18% per year. However, the global rate still stands at 36.72 deaths per 1000 live births, well above the SDG target, and is not projected to reach the target until 2035. 133 countries have already met the target and nine more are on track to do so by 2030. However, 58 countries will miss the deadline, including 25 that are not projected to reach the target until after 2050, and Dominica, where under-five deaths have risen. More than four-fifths of all under-five deaths worldwide are concentrated in just two regions: Sub-Saharan Africa, where the mortality rate remains at 68.82 deaths per 1000 live births and is not projected to meet the SDG target until 2055, and Central and Southern Asia.
The study is limited by the assumption that trends over the last two decades will continue unchanged. Data quality was also poor in some conflict-affected regions and low-income countries, the very places where child mortality is highest.
The authors conclude that to meet UN targets, policymakers must focus on scaling up proven interventions – including skilled birth attendance, postnatal care, vaccination, improved nutrition, and treatment for common childhood illnesses – in every community, and especially in Sub-Saharan Africa.
M-CHAT does not catch all children with autism in the neonatal high-risk group, shows a study from Karolinska Institutet published in JAMA Network Open. The researchers see a need to supplement the test with other assessment methods.
Children born very prematurely or with complications are screened at the age of two for early signs of autism using the M-CHAT questionnaire. In a new national study, researchers at Karolinska Institutet have investigated how well the test works in this high-risk group. The study includes 2178 children born in Sweden between 2013 and 2019 and compares M-CHAT results with later clinical diagnoses of autism.
The researchers found that the test was highly accurate in ruling out autism, but that many children with autism were still missed. The sensitivity was 62%, while the specificity – the ability to identify children without autism – was 91%. In total, 12% of the children received a positive M-CHAT result and 6% were later diagnosed with autism.
“The results show that M-CHAT works relatively well to rule out autism, but that it does not catch all children who later receive a diagnosis. In this high-risk group, more tools are therefore needed to detect children who need further investigation early,” says Ulrika Ådén, professor at the Department of Women’s and Children’s Health.
Children born extremely prematurely had both the highest proportion of positive test results and the most autism diagnoses. The researchers also saw that girls had fewer positive test results than boys, and that linguistic factors could affect the outcome – the test had higher specificity in families that spoke a Scandinavian language.
“Overall, the study shows that other developmental difficulties, such as motor or sensory problems, can affect how M-CHAT is interpreted. This needs to be taken into account when healthcare works with early screening,” says Ulrika Ådén.
In emergency medicine, triage differentiates patients who require immediate attention from those who can safely wait for care. When it comes to children’s mental or behavioural health, however, triage scores were found to be inaccurate in two-thirds of the cases when compared to the level of care the child actually received during their emergency visit, according to a new study published in JAMA Network Open. Under-triage, or assignment of a lower severity score than the level of care that was needed, was more likely for children who were Black, Hispanic, and those who preferred Spanish compared to English.
“Our study was the first to examine rates of mis-triage in paediatric emergency departments when children present for mental or behavioural health concerns,” said lead author Jennifer Hoffmann, MD, MS, emergency medicine physician and researcher at Ann & Robert H. Lurie Children’s Hospital of Chicago and Assistant Professor of Pediatrics at Northwestern University Feinberg School of Medicine. “When triage determination is wrong, there might be a risk to patient and staff safety, or resources might be diverted from kids in greater need. Especially with the ongoing youth mental health crisis, and as we continue to see more and more children with these issues in the emergency department, our ability to accurately distinguish levels of urgency upon arrival becomes even more critical. We need to refine triage tools to be more accurate and equitable so that they will work for all children who walk through our doors seeking care.”
Dr Hoffmann and colleagues analysed 74 564 visits for mental or behavioural health complaints among children 5-17 years of age presenting to one of 15 U.S. emergency departments participating in the Pediatric Emergency Care Applied Research Network (PECARN) Registry. The study focused on the Emergency Severity Index (ESI), the triage system used in over 90% of U.S. emergency departments.
The most frequently presenting primary mental health diagnosis groups were depressive disorders (25% of visits) and suicide or self-injury (23% of visits). Aggressive behavior occurred in 24% of the visits.
Over-triage, which involves assigning a higher severity triage score than the level of care the child received throughout their emergency visit, was found in more than half (57%) of visits, while under-triage occurred in approximately 1 in 12 visits (8%). Over-triage was more likely during visits by younger patients and Black patients compared to White patients. Under-triage was more likely among visits by Black and Hispanic patients compared to White patients, as well as in visits with a language preference of Spanish relative to English.
“The main message for parents is to advocate for your child. If you are worried that your child is at risk of harming themselves or others while they are waiting, tell the nurse immediately,” Dr. Hoffmann advised.
“Underlying drivers for inequities in triage may include implicit bias, which refers to unconscious stereotypes or attitudes,” said Dr Hoffmann. “Clinicians need education on recognizing their own biases, in order to avoid undue influence on the care they provide. Using automated tools or artificial intelligence (AI) to augment the nurse’s assignment of triage scores might help achieve a more objective assessment, although these strategies require further testing. We also need to make interpretation services in the emergency department more readily accessible to families who prefer a language other than English. Ultimately, accurate and equitable triage systems are needed to match children with the right care at the right time, particularly during times of resource strain.”
A new Cochrane review finds that chlorhexidine likely cuts umbilical cord infection rates by about 29% in low- and middle- income countries, and may reduce newborn deaths.
Umbilical cord care is a key part of newborn hygiene that helps prevent infection and promotes healthy healing. According to the World Health Organization (WHO), approximately 2.3 million newborn babies died in 2023, with the highest burden in low- and middle-income countries (LMICs).
Cord care practice varies widely around the world, shaped by local culture, healthcare infrastructure and available resources.
In settings with adequate obstetric care and low neonatal mortality, current WHO guidelines recommend dry cord care, involving keeping the stump clean and dry without antiseptics. In settings with higher neonatal mortality, the guidelines recommend daily application of 4% chlorhexidine for a week.
Antiseptic cord care offers protection
The researchers systematically reviewed 18 randomised controlled trials involving 143 150 newborns to evaluate whether applying antiseptics to the umbilical cord stump reduces infection, death, or delays cord separation compared to no treatment. The review covered antiseptics including 4.0% chlorhexidine (CHX), 70% alcohol, silver sulfadiazine, and povidone iodine.
The findings show that applying chlorhexidine to newborns’ umbilical cords likely reduces the number of infections from around 87 to 62 per 1000 newborns and the numbers of deaths may fall from around 18 to 15 per 1000 newborns in LMICs. Chlorhexidine likely also delays the time it takes for the cord stump to fall off by one to two days.
Only one study from a high-income country evaluated chlorhexidine. Evidence for preventing the bacterial infection omphalitis and its effect on cord separation was very uncertain, meaning conclusions cannot be drawn for these settings at this time.
“In many parts of the world, newborns are still born into environments where hygiene conditions are poor. Simple and accessible cord-care interventions can significantly reduce infections in these settings, which is critical given the large share of neonatal deaths linked to infection.”
– Dr Aamer Imdad, University of Iowa
Evidence for alcohol use in LMICs was very uncertain for both infection prevention and cord separation time. In high-income countries, moderate-certainty evidence suggests alcohol delays cord separation by approximately 1.6 days, but no studies reported on mortality or omphalitis in these settings.
Umbilical cord care should be contextualised to local settings
Dry cord care remains the recommended approach in countries with adequate obstetric care and low neonatal mortality. The authors explain that in many places, clean and dry cord care may be sufficient, while in others antiseptic approaches can reduce infection risk. The key is choosing interventions that match the realities families and health systems face.
“Our findings broadly support current World Health Organization guidance, but they also underline an important point: these interventions are not necessarily universal solutions. The benefits depend strongly on the context in which babies are born. What works best depends on local circumstances.”
– Professor Zulfiqar Ahmed Bhutta, Centre for Global Child Health in Canada and Aga Khan University in Pakistan
Many studies did not share individual patient data, which the authors say would have helped answer some remaining questions more clearly. Greater and timely data sharing could greatly strengthen transparency and in-depth scientific analysis for policy.
Children living with obesity but showing no signs of metabolic complications still have a significantly increased risk of developing type 2 diabetes, high blood pressure, and abnormal blood lipid levels later in life. A new study from the Karolinska Institutet, published in JAMA Pediatrics, also shows that these children benefit greatly from obesity treatment.
“There has been a debate about whether children with normal blood and liver values and normal blood pressure might not need treatment for their obesity. Our study shows that this assumption is incorrect,” says Claude Marcus, professor at the Department of Clinical Science, Intervention and Technology, Karolinska Institutet.
The study included just over 7200 children aged 7–17 who had begun obesity treatment in Sweden and were followed up until age 30. The researchers compared children with so-called metabolically healthy obesity (MHO), children with obesity and impaired cardio-metabolic risk markers (MUO), and peers from the general population.
A clearly increased risk
By age 30, 9% of the children with MHO had developed type 2 diabetes, compared with 17% of those with MUO and 0.5% in the control group. Similar patterns were observed for high blood pressure (11% in the MHO group, 18% in the MUO group, and 4% in the control group) and abnormal blood lipids (5 and 13%, respectively, compared to 1% in the general population).
“Even children with obesity who show no signs of cardiometabolic impact have a clearly increased risk of future diseases. This means that normal blood pressure and the absence of abnormal blood test results are not sufficient protection against future morbidity,” says Emilia Hagman, associate professor at the Department of Clinical Science, Intervention and Technology, Karolinska Institutet, and the paper’s corresponding author.
All children need treatment
All children in the study received support for healthier lifestyle habits, and the researchers also investigated whether the treatment response affected the risk of future illness in the different groups. A good treatment response during childhood was linked to a reduced risk of all the diseases studied. The effect was equally significant in both the MHO and MUO groups.
“Our results suggest that all children with obesity need treatment, even if they appear completely healthy upon examination,” says Claude Marcus.
The study is based on data from the national quality registry BORIS and several Swedish health data registries. The research was funded by, among others, the Center for Innovative Medicine, the Ollie and Elof Ericsson Foundation, and the Freemason Foundation for Children’s Welfare. Several of the researchers report compensation from companies unrelated to this work. See the scientific article for a complete list of conflicts of interest.
A major UK-led clinical trial has found that a treatment commonly used to help premature babies breathe offers no benefit for infants on life support with severe bronchiolitis – a seasonal viral illness that hospitalises thousands of babies each year.
Funded by a partnership between the UK’s UKRIMedical Research Council (MRC) and National Institute for Health and Care Research (NIHR), and by Chiesi Farmaceutici SpA, Italy, the Bronchiolitis Endotracheal Surfactant Study (BESS) trial is the largest-ever randomised study of surfactant for bronchiolitis.
Bronchiolitis occurs when a virus – most commonly respiratory syncytial virus (RSV) – infects a baby’s lungs. There is currently no specific treatment for RSV infection, and the illness can be especially severe in premature and newborn infants. Babies with bronchiolitis have reduced levels of surfactant in their lungs, a condition similar to that seen in babies born prematurely. Because surfactant is routinely used to help premature infants breathe more easily, the study team set out to determine whether this therapy could also benefit babies hospitalised with bronchiolitis.
The study ran across 15 children’s hospitals in England, Scotland, and Northern Ireland and involved 232 critically ill babies. However, surfactant did not reduce the time they needed to be on a ventilator (life-support breathing machine).
Professor Calum Semple OBE, the study’s lead from the University of Liverpool and Alder Hey Children’s NHS Foundation Trust, said: “The treatment was safe, but it didn’t make any difference to how long babies stayed on ventilators. We had hoped that surfactant might speed up recovery for these very sick babies, but the evidence doesn’t support this.”
Bronchiolitis is the leading reason why babies are admitted to hospital in the UK during winter. It typically affects babies under one year old and can be especially severe in those born prematurely. While most of the twenty-five thousand babies admitted will recover with oxygen and fluids, around a thousand of the most unwell require intensive care and a ventilator to support their breathing. Currently, there is no other treatment for bronchiolitis, but a vaccine is now being offered to the mother-to-be in the last months of pregnancy.
The BESS trial was designed to give families and clinicians clear answers. It ran over six winter seasons from 2019 to 2024.
Professor Semple added: “While we continue to research better ways to care for these sick babies, I urge Mums-to-be to accept the offer of the RSV vaccine during pregnancy, which will protect their newborn babies from severe bronchiolitis.”
The researchers emphasise that surfactant therapy remains essential for premature newborn babies and advocate for further studies to explore targeted treatments for bronchiolitis.