Scanning Electron Micrograph of a breast cancer cell. Credit: NIH
Breast cancer and diabetes have long been suspected to have some kind of relationship, but now new research in Nature Cell Biology reveals how breast cancer cells sabotage insulin production to fuel their own cravings for glucose.
Diabetes risk begins to increase two years after a breast cancer diagnosis, and by 10 years post-diagnosis, the risk is 20% higher in breast cancer survivors than in age-matched women without breast cancer.
But these epidemiological linkages are not clear-cut or definitive, and some studies have found no associations at all. In the paper, a research team describe a possible biological mechanism connecting the two diseases, in which breast cancer suppresses the production of insulin, resulting in diabetes, and the impairment of blood sugar control promotes tumour growth.
“No disease is an island because no cell lives alone,” said corresponding study author Shizhen Emily Wang, PhD, professor of pathology at UC San Diego School of Medicine. “In this study, we describe how breast cancer cells impair the function of pancreatic islets to make them produce less insulin than needed, leading to higher blood glucose levels in breast cancer patients compared to females without cancer.”
The researchers name the culprit as extracellular vesicles (EV), which carry DNA, RNA, proteins, fats and other materials between cells, a sort of cargo communication system.
The cancer cells were found to be secreting microRNA-122 into the vesicles. When vesicles reach the pancreas, Prof Wang said, they can enter the islet cells, offload their miR-122 cargo and damage the islets’ critical function in maintaining a normal blood glucose level.
“Cancer cells have a sweet tooth,” Prof Wang said. “They use more glucose than healthy cells in order to fuel tumor growth, and this has been the basis for PET scans in cancer detection. By increasing blood glucose that can be easily used by cancer cells, breast tumors make their own favorite food and, meanwhile, deprive this essential nutrient from normal cells.”
Feeding mice slow-releasing insulin pellets or an SGLT2 inhibitor restored normal control of glucose in the presence of a breast tumour, in turn suppressed the tumour’s growth.
“These findings support a greater need for diabetes screening and prevention among breast cancer patients and survivors,” remarked Prof Wang, noting that a miR-122 inhibitor is currently in clinical trial as a potential treatment for chronic hepatitis C. It has been found to be effective in restoring normal insulin production and suppressing tumour growth in mouse models of breast cancer.
“These miR-122 inhibitors, which happen to be the first miRNA-based drugs to enter clinical trials, might have a new use in breast cancer therapy,” Prof Wang posited.
Judge Edwin Cameron, Inspecting Judge of Correctional Services, writes about the need for healthcare professionals working in prisons should be shifted to the Department of Health.
Our country’s healthcare system is a cumbersome double-deckerbus: on top are those of us who have access of some kind to private healthcare (a high estimate is around 27% of the population). The great majority of necessity rely on public healthcare. But, within public healthcare, there is a further divide, an overlooked layer at the very lowermost – the healthcare afforded to people in prison.
During apartheid, healthcare for those inside prison and in police custody was used as a “tool of manipulation and coercion”. There was medical negligence, poor quality care, false medical and autopsy reports, and warped medical ethics. (Bram Fischer, in his dying days, received no treatment for his crippling cancer).
Some doctors and other medics were complicit in abuses, turning a blind eye to what was happening before them.
The Truth and Reconciliation Commission (TRC) Special Hearings on Prisons showed how basic access to medical treatment was used to punish. Henry Magkothi recounted how difficult it was to gain access on Robben Island to the hospital. “The doctor didn’t come often enough and even then there were so many obstacles they placed in your way.”
Not only did doctors have to have security clearance to work in prisons, but there were split institutional loyalties. Some health professionals were employed by the Department of Health and others by the Department of Prisons (now the Department of Correctional Services — DCS). This led to a dilemma of “dual obligations”, where the lines of authority for healthcare and custodial care were blurred. Health professionals owed loyalty to their patients (the inmates). But they had obligations to, and pressure from, their employers (the prison authorities).
Healthcare must be separated from prison administration
This blighted history led Dr Judith van Heerden, an expert in this area, to recommend to the TRC that prison healthcare “must be separated completely from custodial care”. All healthcare professionals in prisons “should be appointed, paid and responsible to the Department of Health” – and no longer to the prison authorities.
The TRC embraced this sound advice in its recommendations. It suggested that: the Department of Health should assume control over prison healthcare; prison health responsibilities and obligations should be clearly defined with an independent line of authority.
These recommendations accord with international guidelines. The UN Mandela Rules entail a demarcation between healthcare and custodial care; there shall be “full clinical independence”. Healthcare professionals “shall not have any role in the imposition of disciplinary sanctions or other restrictive measures”. And clinical decisions may only be taken by healthcare professionals “and may not be overruled or ignored by non-medical prison staff”.
Experts have underscored the importance of providing health services in prison that are separate from the prison administration. The World Health Organisation and the United Nations Office on Drugs and Crime note that healthcare professionals should act “completely independent of prison authorities” and in “alignment with public health services.”
Furthermore, the Association for the Prevention of Torture advocates for the “integration of the prison health service into the national health service” to guard the “professional and ethical independence of the health staff” and “provide recourse to an independent body in case of conflicts.”
Did democratic South Africa heed this advice? No.
Medical ethicist Professor Solomon Benatar observes that the Department of Health “began to dismantle the District Surgeon Services” and “[i]t became possible for DCS to appoint nurses and other medical staff to deliver healthcare” in our prisons.
This is evident in the plain wording of the Correctional Services Act of 1998. Section 12(1) states that DCS “must provide, within its available resources, adequate health care services” and section 12(2)(b) outlines that medical treatment “must be provided by a correctional medical practitioner, medical practitioners or by a specialist or health care institution or person or institution identified by such correctional medical practitioner”. And according to section 12(3), if an inmate opts to be “visited and examined by a medical practitioner of [their] choice” it is “subject to the permission of the Head of Centre”.
Post-apartheid, healthcare in prisons is still not independent. Benatar slates this “retrogressive step”; “diverting some responsibilities for healthcare away from the Department of Health” and towards DCS, diminishes the “loyalty of some health professionals” as it ranks “allegiance to prison authorities higher than professional responsibility to patients.”
A special duty of care
In his book Health and Health Promotion in Prisons, Professor Michael Ross states that depriving inmates of liberty does not mean we may deprive them of access to healthcare. On the contrary, their deprivation of liberty means we owe them a “special duty of care”. Critically, Ross acknowledges that we provide “good care to bad people because we are professional, and because we, and they, are human” and if bad care is given “the humanity we degrade is also ours, not only theirs”.
Those in prison should have the same quality of healthcare as the public outside. This is the “equivalence of care” principle. It means that you don’t add poor healthcare treatment on top of imprisonment to punish. As I have written before, “prison health affects our health” and “equivalence of care” should be considered a minimum threshold. In light of the higher mortality rates in prisons; government may have to provide higher standards of healthcare in prisons.
We know that injuries and the use of anti-depressants are warning signs of trouble. Many cases of claimed abuse (especially sexual violations, assaults, use of force and torture) are reported to nurses and doctors. Later, investigators, both internal and external, rely on medical reports. Ross emphasises that one must ensure health assessments of inmates are based on medical criteria and inmates ought to trust their healthcare providers and feel safe to report and speak out about abuse.
In addition, nurses, psychologists and other medical practitioners play a role in how prisons are run. For example, they are expected to visit inmates in segregation (sometimes in solitary confinement). The Act provides that segregation “must be discontinued” if medical practitioners determine that “it poses a threat to the health of the inmate”.
Further, independent healthcare can provide another significant layer of independent monitoring over our closed-off prisons.
Two parallel healthcare systems are not advisable. Does DCS have adequate training facilities to ensure training and updates on clinical care for clinicians on its payroll? The Judicial Inspectorate for Correctional Services (JICS), which I head, believes not. DCS clinicians often miss out on training opportunities. Further, DCS’s data systems are standalone – they are not linked to the Department of Health’s facilities (connecting them would ensure continuity of care when inmates are released).
And a heartening thought – why not allocate community service doctors to prisons? This would alleviate costs and skills scarcity.
The state of healthcare in our prisons
Grievously, our prisons are a microcosm of all our country’s social ills. This is true of healthcare, but perhaps it is worse, since, notoriously, prisons are epidemiologic pumps for the spread of infectious viruses and diseases.
The 2020-2021 annual report of the Judicial Inspectorate for Correctional Services paints an agonising picture of the state of prison healthcare.
Inmates do not get regular access to nurses and doctors, clinics in prisons are cramped and there is limited privacy for consultations, correctional officials are not always available to escort inmates to healthcare facilities, medications are not always dispensed on time, some medications have expired, health check-ups and screenings upon admission are not always conducted and medical files are not always updated.
Healthcare professionals in prisons, especially psychologists and social workers, are working with a desperate population. In the single year covered in the report, JICS reported 86 hunger strikes, 66 attempted suicides and 27 suicides. According to DCS’s annual report “suicide is the leading cause of [unnatural] deaths in correctional facilities”.
JICS’s recent quarterly report lists 40 unnatural deaths. We don’t know the cause of most; seemingly healthy inmates died. This requires JICS’s close investigative scrutiny of the post-mortem and medico-legal documents, which are in the hands of DCS and sometimes mysteriously go missing.
Further, there were 113 deaths as a result of natural causes, including pneumonia, cancer, meningitis, septicaemia and asthma. Could some of these deaths have been avoided with early detection, close monitoring and regular access to medical assistance? JICS thinks so.
JICS is also alarmed by the 116 declared state patients in prison; these are individuals whom the courts have found are suffering from mental unwellness challenges. As they wait indefinite periods for a transfer to a psychiatric hospital, they are wrongly housed in correctional facilities. State patients should not be a DCS responsibility. JICS has raised its voice on this: correctional facilities are not conducive for state patients, and correctional officials and fellow inmates are not trained to properly accommodate them.
To end off
While inspecting prisons, I have met passionate nurses and committed doctors. Prisons are tough, dangerous and complicated places. I acknowledge that DCS has worked hard to progress in dealing with Covid, HIV and TB behind bars. But we have to do better.
We need institutional reform. Healthcare professionals working in prisons ought to be independent of DCS. This means shifting all healthcare professionals to the Department of Health and ensuring proper channels of authority and oversight within prisons. In addition, healthcare professionals need specific and ongoing training for the prison environment. We also need more healthcare professionals working in prisons – and they must be accessible, proactive and willing to speak out.
That takes us back to where we started. Our Department of Health must be well-resourced, well-capacitated and well-run – and healthcare professionals must be trained and supported and have job security. And this goes to the heart of whether we have a capable state, strong institutions and a culture of accountability.
Judge Cameron is Inspecting Judge of Correctional Services.
Views expressed are not necessarily those of GroundUp.
Scanning Electron Micrograph image of a human T cell. Credit: NIH/NIAID
While T cells are the body’s warriors against infection, without rest and maintenance T cells can die, leaving their hosts more susceptible to pathogens, researchers reported in the journal Science.
“We may have to change how we teach T cell biology,” said Professor Lieping Chen, who is the senior author of the study.
T cells remain in a quiescent state until pathogens are detected, but the molecular mechanisms of this state were previously unknown.
In the new study, researchers showed that a protein known as CD8a – which is found in a subset of T cells called CD8 cells – is crucial to keeping the cells in this dormant state. When scientists deleted this protein in mice, the protective CD8 cells were unable to enter a quiescent state and died, leaving the host vulnerable to infections.
Further, they identified another protein, PILRa, that provides a biochemical signal to CD8a. By disrupting this protein pair, both “memory” CD8 cells – previously been exposed to pathogens – and naïve cells died because they lacked the ability to stay in a quiescent state.
The researchers hope that understanding why this resting state is crucial to maintenance and survival of T cells can lead to improved immune system function.
Chen noted that as people age they tend to lose both naïve and memory T cells, making older individuals more susceptible to infections. It is possible that the inability of T cells to remain in a quiescent state could lead to people becoming more susceptible to infections and cancer, the authors suggest.
An Australian study published in Allergy, has identified the key immunological changes that support the remission of peanut allergy in children, a discovery that could pave the way to new, more targeted treatments.
The research showed, for the first-time, that specific gene networks are rewired to drive the transition from peanut allergy to clinical remission following a combination treatment of a probiotic and peanut oral immunotherapy.
The study found that this network reprogramming essentially shuts down the allergic immune response that was responsible for causing a food allergy.
Lead researcher, Professor Mimi Tang of Murdoch Children’s Research Institute, said this was the first study to map the complex gene to gene communication and connectivity underlying clinical remission of peanut allergy.
“The immunological changes leading to remission of peanut allergy were largely unknown,” she said. Previous studies had mostly focused on examining the levels of gene expression, without also exploring how genes interact with each other. But genes don’t work in isolation; instead, biological responses are controlled by large numbers of genes communicating with each other, so it made sense to look at these interactions more closely.
“What we found was profound differences in network connectivity patterns between children who were allergic and those who were in remission. These same changes were also seen when we compared gene networks before and after immunotherapy in the children who achieved remission following immunotherapy.”
The randomised controlled trial involved 62 peanut allergic children, ages 1–10, who received a combination treatment of a probiotic and oral immunotherapy (gradual introduction of the allergen) or a placebo. Following 18 months of treatment, 74% taking the combination treatment achieved remission compared with 4% in the placebo group.
The peanut oral immunotherapy that was used in combination with the probiotic in the trial was PRT120, a lead candidate from biotech company Prota Therapeutics.
The team led by Professor Tang also recently showed in a separate trial that two treatments — the combination probiotic and peanut oral immunotherapy treatment and the peanut oral immunotherapy alone — were highly effective at inducing remission and desensitisation. About half of the treated children achieved remission, which allowed them to stop treatment and safely eat peanut freely.
Murdoch Children’s Dr Sarah Ashley said while oral immunotherapy could successfully induce desensitisation and remission, desensitisation often waned after treatment ended or even during ongoing maintenance dosing.
“Certain changes in the allergen-specific immune cells, called Th2 cells, are critical to achieving lasting remission,” she said. Th2 cells are essential for generating allergen-specific antibodies and the development of food allergy. We found that the Th2 signalling that drives allergy is ‘turned off’ in children in remission.”
Food allergy is a global public health concern, affecting 10% of infants and 5–8% of children.
South Africa’s medicines regulator has officially terminated the special dispensation to use Ivermectin as a treatment for COVID, stating that “there is currently no credible evidence to support a therapeutic role for Ivermectin” in the treatment of the disease.
On Monday 30 May, the South African Health Products Regulatory Authority (SAHPRA) officially withdrew its authorisation [PDF], bringing to end something of a saga which saw vocal proponents pitched against the scientific and regulatory establishment.
The antiparasitic Ivermectin gained considerable notoriety as the COVID pandemic went on, based on preliminary studies that seemed to demonstrate its effectiveness. Pressure born out of desperation for some kind of treatment led to SAHPRA – amidst its own apparent misgivings – granting compassionate use authorisation under strict guidelines in January 2021. Use was allowed under Section 21 guidelines without having to wait for Section 21 authorisation, which was misinterpreted as full authorisation by some media sources.
The social media furore and misinformation surrounding Ivermectin led to dangerous instances of COVID self-treatment, with hospitalisations and even deaths reported.
In its terribly botched response to COVID, Brazil adopted Ivermectin on a mass scale, and essentially became a living laboratory for its effectiveness. Despite even administering Ivermectin as prophylaxis, Brazil’s health system was overwhelmed with COVID patients during the surge caused by the Gamma variant.
Studies turned up scant evidence in favour of Ivermectin’s effectiveness, with serious flaws and even outright data fabrication were picked up in a number of studies that seemed to show a significant benefit – even flying right through the peer review process only to be picked up at a later stage. This lead to a major meta-analysis by Hill et al. showing a effectiveness instead being retracted, which SAHPRA noted in its decision.
Finally, the I-TECH and the Together randomised clinical trials of 2021 showed no effect. Like hydroxychloroquine before it, Ivermectin prescribing was found to be driven by political interests. Thus, Ivermectin quietly disappeared from the media as viable antivirals such as Paxlovid came into the market.
The termination comes after a distinct decline in demand for Ivermectin use in South Africa, with no new applications for importation of unregistered Ivermectin products place since August 2021. SAHPRA also noted a marked decline in the number of health facilities applying for permission to hold bulk stock after August 2021.
Furthermore, no individual named patient applications have been approved since December 2021. Finally, there was little in the way of reporting of outcomes achieved by the treating healthcare providers.
The latest COVID seroprevalence survey shows that nearly every adult in South Africa has either been vaccinated or had COVID. For many, it’s both.
The study analysed blood from over 3000 blood donors. It was conducted by the South African National Blood Service, which is responsible for blood donations in eight provinces, and the Western Cape Blood Service.
The researchers estimated that by March 2022, before the fifth wave which appears to have peaked in the last few weeks, 98% of adults had some detectable antibodies, whether from COVID or from vaccination. This means that only 2% had neither been vaccinated nor been infected.
Only 10% had been vaccinated but not infected by COVID.
(Note: The study has been published as a preprint and has not been peer-reviewed.)
What the survey tested for
Blood samples were collected and tested from 3395 consenting donors from all provinces in mid-March 2022. While blood donors are not precisely representative of the population, the researchers have argued that the study is representative enough.
This is the first time the blood services researchers have been able to look for two types of antibodies.
One test indicates if a sample has antibodies to the nucleocapsid proteins (anti-nucleocapsid antibodies). These antibodies develop if someone is infected, but won’t develop after a person receives a vaccine only (at least not those vaccines currently available in South Africa).
The other test indicates if the sample has antibodies to the spike protein (anti-spike antibodies). These antibodies develop when someone has been infected or has been vaccinated (or both).
Using these two tests together, researchers can, for the first time, evaluate the proportion of the population that has been vaccinated and not infected.
Results
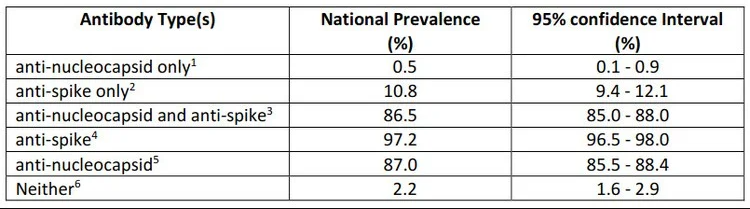
After weighting the results to reflect national demographics, the researchers found that a mere 2% of the population had neither anti-spike nor anti-nucleocapsid antibodies. These are people who have likely never had COVID nor been vaccinated.
10% had only anti-spike antibodies. These are people who were likely vaccinated, but never infected.
The researchers noted that there is “an increasing incidence of reinfection” with the omicron wave.
Blood service survey is the best we have
The blood services have been regularly testing blood samples from donors throughout the pandemic, looking at the presence of anti-nucleocapsid antibodies.
While other surveys might be more representative of the population than the blood donor ones, these have been infrequently published or published long after the survey was conducted. By contrast the blood donor surveys are relatively affordable and quick to publish. Also, as far as we are aware, it is the only survey repeatedly testing the same group of people, so that comparisons across time are possible.
Past blood surveys
The blood services’ survey from samples taken in May 2021 estimated that 47% of the adult population had previously been infected.
The next survey of blood samples was taken in November 2021 after the delta wave. This was just before the omicron wave. The researchers estimated that about 70% of people had been infected.
The latest survey indicates that about 87% of people have been infected.
The previous surveys found that levels of infection differed by province. Now these differences have “largely disappeared as prevalence appears to have saturated”.
Differences across race
There are significant differences in rates of infection when different races are compared.
The November survey showed that about 80% of black donors and 40% of white donors had been infected with COVID.
In the latest survey the proportion of white and Asian donors that only have anti-spike antibodies (indicating vaccination but no infection) was higher than black and coloured donors.
The researchers suggest that “white donors are both unusually likely to avail themselves of vaccination, and they are unusually able to avoid exposure, for instance by working predominantly from home, [and] living in smaller family units.”
Daily vitamin D supplements do not seem to prevent the development of type 2 diabetes in people already at high risk of the condition, according to a Japanese trial published by The BMJ.
While no clinically meaningful effect was seen in high risk adults, the results hinted that there may be a benefit for people with insufficient insulin secretion.
Type 2 diabetes affects around 480 million people worldwide, and is predicted to increase to 700 million by 2045. Another half a billion people have impaired glucose tolerance or pre-diabetes (higher than normal blood sugar levels that, if left untreated, can develop into type 2 diabetes).
Weight loss and exercise can lower the risk of progression to type 2 diabetes, but are difficult to sustain, so new strategies are needed to tackle the problem.
An association between vitamin D deficiency and an increased risk of future diabetes has been shown in some studies, but trials of vitamin D supplements for preventing type 2 diabetes show inconsistent results.
To address this knowledge gap, researchers therefore set out to assess whether eldecalcitol (an active form of vitamin D used to treat osteoporosis in Japan) could reduce the risk of developing type 2 diabetes among people with impaired glucose tolerance.
The study involved 1256 Japanese adults with impaired glucose tolerance with an average age of 61 years; 46% were women, and 59% had a family history of type 2 diabetes.
Participants were randomly assigned to receive either a standard daily dose of eldecalcitol (630 participants) or placebo (626 participants) and were assessed for diabetes every three months over a three-year follow-up period.
During this period, the researchers found no meaningful differences between groups in those who developed diabetes (12.5% in the eldecalcitol group and 14% in the placebo group) or whose blood sugar levels returned to normal (23% in the eldecalcitol group and 20% in the placebo group).
However, after adjusting for 11 potentially influential factors, including age, sex, blood pressure, body mass index, and family history of diabetes, the results suggested that eldecalcitol might prevent type 2 diabetes in pre-diabetic patients with insufficient insulin secretion. But this finding remains unclear and the researchers say further work is needed before any firm conclusions can be made.
They did, however, find a significant increase in both lower back and hip bone mineral densities among those taking eldecalcitol compared with placebo.
No significant difference in serious adverse events was seen between the two groups.
The researchers acknowledge some uncertainties, such as whether the dose of eldecalcitol used was appropriate for preventing diabetes, and whether the results apply to all ethnicities. Nevertheless, this was a large trial with regular follow-up and high adherence to treatment, suggesting that the findings are robust.
As such, they say: “Although treatment with eldecalcitol did not significantly reduce the incidence of diabetes among people with pre-diabetes, the results suggested the potential for a beneficial effect of eldecalcitol on people with insufficient insulin secretion.” And they call for further research to determine whether vitamin D is beneficial to people with pre-diabetes.
This new trial was well conducted and results are consistent with two other recent trials, said Tatiana Christides at Queen Mary University of London in a linked editorial.
However, several questions remain, she writes, including whether vitamin D supplementation may be more effective for particular populations, and whether longer duration of treatment or younger age at initiation might be more beneficial.
Until further data are available from high quality randomized trials, she suggests healthcare professionals “should continue to discuss with patients the musculoskeletal health benefits of vitamin D and support them to achieve and maintain lifestyle changes that, although challenging to sustain, are known to decrease development of type 2 diabetes.”
A study published in eLife reveals how the brains of humans and other primates under anaesthesia differ from mammals such as mice, with the visual cortex in primates being isolated from certain effects.
Anaesthesia still holds mysteries for modern science. Electroencephalography (EEG) studies show that, during anaesthesia, the brain is put into a deep sleep-like state in which periods of rhythmic electrical activity alternate with periods of complete inactivity. This state is called burst-suppression. Until now, it was unclear where exactly this state happens in the brain and which brain areas are involved.
Shedding light on the phenomenon would help better understand how the brain functions under anaesthesia. To this end, researchers used functional magnetic resonance imaging (fMRI) to study the precise spatial distribution of synchronously working brain regions in anaesthetised humans, long-tailed macaques, common marmosets and rats. They were able to show for the first time that the areas where burst-suppression is evident differ significantly in primates and rodents. While in rats large parts of the cerebral cortex synchronously show the burst-suppression pattern, in primates individual sensory regions, such as the visual cortex, are excluded from it.
“Our brain can be thought of as a full soccer stadium when we are awake,” explained Nikoloz Sirmpilatze, lead author of the study. “Our active neurons are like tens of thousands of spectators all talking at once. Under anaesthesia, however, neuronal activity is synchronised. You can measure this activity using EEG as uniform waves, as if all the spectators in the stadium were singing the same song. In deep anaesthesia, this song is repeatedly interrupted by periods of silence. This is called burst-suppression. The deeper the anaesthesia, the shorter the phases of uniform activity, the bursts, and the longer the periodically recurring inactive phases, the so-called suppressions.”
The phenomenon is caused by many different anaesthetics, some of which vary in their mechanisms of action. And burst-suppression is also detectable in coma patients. However, it is not known whether this condition is a protective reaction of the brain or a sign of impaired functioning. It has also been unclear where in the brain burst-suppression occurs and which brain areas are involved, as localisation by EEG alone is not possible.
To answer this question, the researchers fMRI. In the first part of the study, the researchers established a system to evaluate fMRI data in humans, monkeys and rodents in a standardised manner using the same method. To do this, they used simultaneously-measured EEG and fMRI data from anaesthetised patients that had been generated in a previous study. “We first looked to see whether the burst-suppression detected in the EEG was also visible in the fMRI data and whether it showed a certain pattern,” says Nikoloz Sirmpilatze. “Based on that, we developed a new algorithm that allowed detecting burst-suppression events in the experimental animals using fMRI, without additional EEG measurement.”
The researchers then performed fMRI measurements in anaesthetised long-tailed macaques, common marmosets and rats. In all animals, they were able to detect and precisely localise burst-suppression as a function of anesthetic concentration. The spatial distribution of burst-suppression showed that in both humans and monkey species, certain sensory areas, such as the visual cortex, were excluded from it. In contrast, in the rats, the entire cerebral cortex was affected by burst-suppression.
“At the moment, we can only speculate about the reasons,” said Nikoloz Sirmpilatze, who was awarded the German Primate Center’s 2021 PhD Thesis Award for his work. “Primates orient themselves mainly through their sense of sight. Therefore, the visual cortex is a highly specialised region that differs from other brain areas by special cell types and structures. In rats, this is not the case. In future studies, we will investigate what exactly happens in these regions during anaesthesia to ultimately understand why burst-suppression is not detectable there with fMRI.”
Susann Boretius, senior author of the study adds: “The study not only raises the question of the extent to which rodents are suitable models for many areas of human brain research, especially when it comes to anaesthesia, but the results also have many implications for neuroscience and the evolution of neural networks in general.”
The human brain usually stores memories in groups so that the recollection of one significant memory triggers the recall of others connected by time. With ageing, the brain gradually loses this ability to link related memories.
Now, researchers have discovered a key molecular mechanism behind this memory linking, and also identified a way to restore this brain function in middle-aged mice. They also found an anti-HIV drug that can do this.
Published in Nature, the findings suggest a new method for strengthening human memory in middle age and a possible early intervention for dementia.
“Our memories are a huge part of who we are,” explained Professor Alcino Silva. “The ability to link related experiences teaches how to stay safe and operate successfully in the world.”
The team from UCLA focused on a gene called CCR5 that encodes the CCR5 receptor – the same one that HIV hitches a ride on to infect brain cells, resulting in memory loss in AIDS patients.
In previous work, Prof Silva’s lab showed that CCR5 expression reduced memory recall.
In the current study, Prof Silva and his colleagues discovered a central mechanism underlying mice’s ability to link their memories of two different cages. Using a tiny microscope, the researchers observed neurons firing and creating new memories in the brains of the mice.
They found that boosting CCR5 gene expression in the brains of middle-aged mice interfered with memory linking, with animals forgetting the connection between the two cages.
Mice with the CCR5 gene knocked out were able to link memories that normal mice could not.
Proof Silva had previously studied the anti-HIV drug maraviroc, which inhibits the entry of HIV into human cells. His lab discovered that maraviroc also suppressed CCR5 in the brains of mice.
“When we gave maraviroc to older mice, the drug duplicated the effect of genetically deleting CCR5 from their DNA,” said Prof Silva. “The older animals were able to link memories again.”
The finding suggests that maraviroc could be used off-label to help restore middle-aged memory loss, as well as reverse the cognitive deficits caused by HIV infection.
“Our next step will be to organise a clinical trial to test maraviroc’s influence on early memory loss with the goal of early intervention,” said Prof Silva. “Once we fully understand how memory declines, we possess the potential to slow down the process.”
All of this raises a question: what’s the purpose of a gene that interferes with the brain’s ability to link memories?
“Life would be impossible if we remembered everything,” said Prof Silva. “We suspect that CCR5 enables the brain to connect meaningful experiences by filtering out less significant details.”
A new study appearing in The Lancet Oncology suggests that a targeted radiation therapy is as effective as standard care for patients with lung cancer brain metastasis.
The findings suggests that patients could benefit from this targeted approach as it is known to have have fewer negative cognitive consequences.
In non-small-cell (NSLC) lung cancer, about 57% of patients present with metastatic disease, and 20% present with brain metastases. Brain metastasis is currently treated with whole brain radiation therapy, which targets the entire brain. While this approach treats even microscopic tumours, it results in memory problems and decreases cognitive function. The alternative, stereotactic radiosurgery, spares healthy brain tissue by precisely targeting the tumour, has been shown to have less severe cognitive consequences but has not yet been studied in patients with small cell lung cancer that has metastasised to the brain.
“For many years, it made sense to treat these patients with whole brain radiation because their survival was quite poor,” said Karolina Gaebe, a research student in Dr Sunit Das’s lab, who led the study.
“For them, long-term consequences of the treatment were not as crucial as reducing the impact of disease in the short-term. But now, as treatments for their lung cancer have improved, these patients are surviving much longer.”
The researchers set out to learn more after noticing patients with longer survival times were also living with severe cognitive impairments due to the treatments for their brain metastases. They wanted to understand whether a more targeted brain radiation regimen might be as beneficial for these patients, as has been demonstrated for most other cancer types.
As a first step, they undertook this meta-analysis, reviewing current literature to examine survival and brain outcomes following stereotactic radiosurgery for patients with small cell lung cancer that had spread to the brain. The team analysed data from 31 studies and included 18 130 patients, the largest cohort of small cell lung cancer patients with brain metastases to be studied so far.
The next steps are to conduct a large clinical trial to investigate cognitive outcome differences between stereotactic radiosurgery and whole brain radiation therapy for such patients.
“Because this is a meta-analysis, we can’t use this as absolute evidence that all patients should be treated in this way,” Dr Das said. “But essentially, this means that we need to challenge our standing worldwide paradigms for treating patients with this disease and revisit the idea that these patients should receive whole brain radiation therapy.”