A study published in Rheumatology & Autoimmunity challenges the assumption that achieving clinical remission in rheumatoid arthritis is sufficient, showing that patient-reported outcomes vary significantly by drug class even when disease activity is comparable.
Investigators found that patients taking TNF inhibitors reported better energy levels, mood, and emotional wellbeing than those taking older conventional drugs, while IL-6 and JAK inhibitors showed particular advantages for patients’ physical functioning. These differences persisted even after accounting for how well the underlying inflammation was controlled.
The study provides real-world evidence that different drug classes offer distinct advantages across quality-of-life domains, supporting a more nuanced, patient-centred approach to treatment selection rather than a one-size-fits-all strategy.
“Despite achieving clinical remission, patients with rheumatoid arthritis may still experience symptoms such as fatigue, sleep disturbances, and mental or communication issues compared with healthy individuals, highlighting the importance of evaluating patient-reported outcomes as a composite measure of treatment efficacy,” the authors wrote.
They noted that the study arrives at a moment when regulators are pushing for patient-reported outcomes to be formally incorporated into drug approvals and reimbursement decisions, and when artificial intelligence–based tools are beginning to use multiple data streams to match the right drug to the right patient.
The University of Tasmania’s Menzies Institute for Medical Research has found that commonly prescribed medication, Diacerein, does not improve knee osteoarthritis symptoms, following a national study.
Diacerein, a medication derived from plants such as rhubarb and aloe vera, has long been recognised for its anti-inflammatory properties and is commonly used to treat osteoarthritis in Europe and Asia.
Led by Associate Professor Dawn Aitken, head of the Musculoskeletal Research Group at Menzies, the DICKENS trial is the largest study globally to investigate Diacerein’s ability to reduce pain in people with knee osteoarthritis who also have inflammation within the joint (effusion synovitis).
“We designed this large trial to test Diacerein in a group of osteoarthritis patients who we thought would have the best chance at benefiting from the drug and found that it did not improve pain or function or decrease local knee inflammation.
“We were hoping that if the drug was effective, it could be included on the Australian Register of Therapeutic Goods (ARTG) as an approved treatment for osteoarthritis in Australia,” Associate Professor Aitken said. “Unfortunately, it’s back to the drawing board to find more effective drug therapies.”
Osteoarthritis is the most common form of arthritis, affecting one in five Australians over the age of 45 and is a major cause of pain, disability, and joint replacement surgery. Despite its widespread burden, very few effective drug treatments exist.
Associate Professor Aitken said the publication of the trial in JAMA Internal Medicine – one of the world’s most prestigious medical journals – highlighted both the significance and rigour of the work.
“While the findings weren’t what we expected or hoped for, publishing this work in JAMA Internal Medicine reinforces the global importance of high-quality research, and we are proud that Menzies is contributing to the global effort to better understand and treat osteoarthritis.”
Associate Professor Aitken is hopeful that other promising drugs in the development stage will become available to bring relief to those suffering chronic pain, but highlighted that non-drug therapies are available.
“Chronic pain has a huge impact on the lives of those who live with it, and the lack of effective drug treatments is frustrating.
“While we currently lack drug treatments for chronic pain, we know that the most effective therapies include education, exercise, weight management and psychological support.”
Despite these findings, patients should not stop taking Diacerein without talking to their treating doctor first.
For GPs, solutions for treating osteoarthritis are frustratingly limited – it’s like the weather, everyone talks about it but nobody does anything about it. While standard care can relieve symptoms, there is currently no way to regenerate the actual lost cartilage in the joints. Some experimental treatments have proven successful in animal models and in petri dishes, but those are still many years away from being approved and available on the market.
But what if there was a currently available drug that could be repurposed? Since overweight and obesity worsen osteoarthritis symptoms by placing excess strain on weight-bearing joints, GLP-1 agonists such as semaglutide have proven that they can help by promoting rapid weight loss, as demonstrated by the STEP-9 trial.
Research into GLP-1s has now revealed that they may offer a whole constellation of other benefits, such as a potential reduction in stroke risk. Now, it appears that GLP-1 agonists may have a direct effect on osteoarthritis independent of weight loss. In our podcast, we look at a recently published article in Cell Metabolism that suggests that GLP-1 agonists might go beyond just the weight loss – promote actual cartilage regrowth by jumpstarting the joint cells’ energy processing pathways. We also explore some of the caveats of potentially using GLP-1 agonists in this way, such as a lack of understanding of the long term effects, as well as the well-documented occurrence of muscle loss.
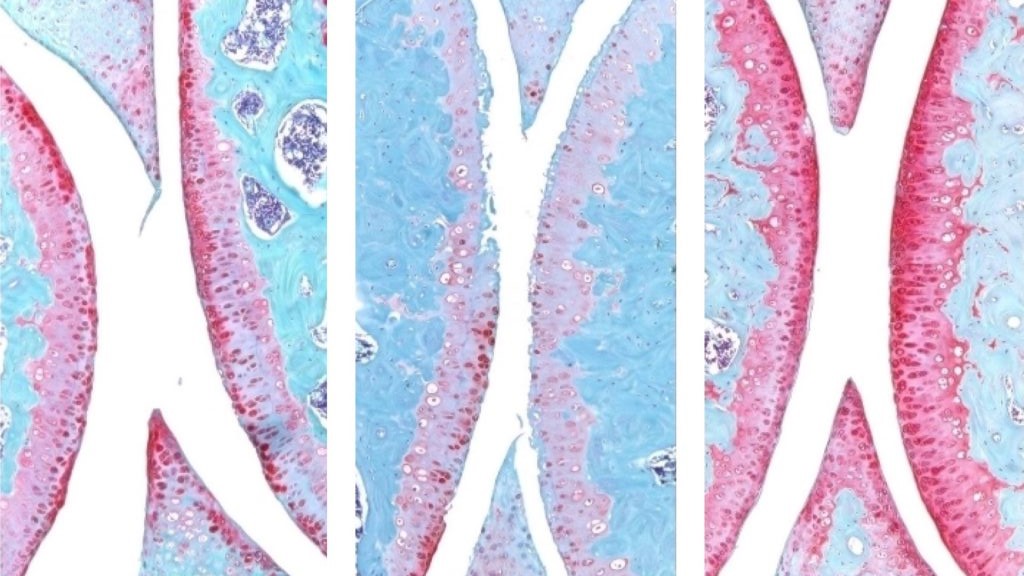
The knee joint of a young mouse (left), aged mouse (middle) and treated aged mouse (right). The red indicates cartilage. Credit: Nidhi Bhutani
An injection that blocks the activity of a protein involved in ageing reverses naturally occurring cartilage loss in the knee joints of old mice, a Stanford Medicine-led study has found. The treatment also prevented the development of arthritis after knee injuries mirroring the ACL tears often experienced by athletes or recreational exercisers. An oral version of the treatment is already in clinical trials with the goal of treating age-related muscle weakness.
Samples of human tissue from knee replacement surgeries – which include both the extracellular scaffolding, or matrix, in the joint as well as cartilage-generating chondrocyte cells – also responded to the treatment by making new, functional cartilage.
The study results suggest it may be possible to regenerate cartilage lost to ageing or arthritis with an oral drug or local injection, rendering knee and hip replacement unnecessary.
The treatment directly targets the cause of osteoarthritis, a disease for which no drug can slow down or reverse its progress; the primary treatments for osteoarthritis are pain control and surgical replacement of the affected joints.
The protein, 15-PGDH – termed a gerozyme due to its increase in prevalence as the body ages – is a master regulator of ageing. Gerozymes, identified by the same researchers in 2023, also drive the loss of tissue function. They are a major force behind age-related loss of muscle strength in mice. Blocking the function of 15-PGDH with a small molecule results in an increase in old animals’ muscle mass and endurance. Conversely, expressing15-PGDH in young mice causes their muscles to shrink and weaken. The gerozyme has also been implicated in the regeneration of bone, nerve and blood cells.
In each of these tissues, regeneration is due to increases in the proliferation and specialisation of tissue-specific stem cells. However, chondrocytes change their patterns of gene expression to assume a more youthful state without the involvement of stem cells.
“This is a new way of regenerating adult tissue, and it has significant clinical promise for treating arthritis due to ageing or injury,” said Helen Blau, PhD, professor of microbiology and immunology. “We were looking for stem cells, but they are clearly not involved. It’s very exciting.”
“Millions of people suffer from joint pain and swelling as they age,” Bhutani said. “It is a huge unmet medical need. Until now, there has been no drug that directly treats the cause of cartilage loss. But this gerozyme inhibitor causes a dramatic regeneration of cartilage beyond that reported in response to any other drug or intervention.”
There are three main types of cartilage in the human body. One, elastic cartilage, is soft and flexible and forms structures like the outer ear. A second, fibrocartilage, is dense and tough, absorbing shock in areas such as between the spinal vertebrae. The third, hyaline cartilage, is smooth and glossy, providing a low-friction surface for lubrication and flexibility in joints like the ankles, hips, shoulders and parts of the knee. Hyaline cartilage, also known as articular cartilage, is the cartilage most commonly affected by osteoarthritis.
Osteoarthritis occurs when a joint is stressed by ageing, injury or obesity. The chondrocytes begin to release pro-inflammatory molecules and to break down collagen, which is the primary structural protein of cartilage. When collagen is lost, the cartilage thins and softens; the accompanying inflammation causes the joint swelling and pain that are hallmarks of the disease. Under normal circumstances, articular cartilage rarely regenerates. Although some populations of putative stem or progenitor cells capable of generating cartilage have been identified in bone, attempts to identify similar populations of cells in the articular cartilage have been unsuccessful.
Previous research from Blau’s lab has shown that a molecule called prostaglandin E2 is essential to muscle stem cell function. 15-PGDH degrades prostaglandin E2. Inhibiting 15-PGDH activity, or increasing levels of prostaglandin E2, supports the regeneration of damaged muscle, nerve, bone, colon, liver and blood cells in young mice.
Blau, Bhutani and their colleagues wondered if 15-PGDH might also play a role in ageing cartilage and joints. They wanted to find out if a similar pathway contributes to cartilage loss from ageing or in response to injury. When they compared the amount of 15-PGDH in the knee cartilage in young versus old mice, they saw that, as in other tissues, levels of the gerozyme increased about two-fold with age.
They next experimented with injecting old animals with a small molecule drug that inhibits 15-PGDH activity – first into the abdomen, which affects the entire body, then directly into the joint. In each case, the knee cartilage, which was markedly thinner and less functional in older animals as compared with younger mice, thickened across the joint surface. Further experiments confirmed that the chondrocytes in the joint were generating hyaline, or articular, cartilage, rather than less-functional fibrocartilage.
“Cartilage regeneration to such an extent in aged mice took us by surprise,” Bhutani said. “The effect was remarkable.”
Addressing ACL tears
Similar results were observed in animals with knee injuries like the ACL tears that frequently occur in people participating in sports such as soccer, basketball and skiing that require sudden pivoting, stopping or jumping. While the tears can be surgically repaired, about 50% of people develop osteoarthritis in the injured joint within about 15 years.
The researchers found that a series of injections twice a week for four weeks of the gerozyme inhibitor after injury dramatically reduced the chance that osteoarthritis develops in the mice. Animals treated with a control drug had levels of 15-PGDH that were twice as high as in their uninjured peers, and they developed osteoarthritis within four weeks.
The animals treated with the gerozyme inhibitor also moved more typically and put more weight on the paw of the affected leg than did untreated animals.
“Interestingly, prostaglandin E2 has been implicated in inflammation and pain,” Blau said. “But this research shows that, at normal biological levels, small increases in prostaglandin E2 can promote regeneration.”
A closer investigation of the chondrocytes in the joints of old mice and young mice showed that old chondrocytes expressed more detrimental genes involved in inflammation and the conversion of hyaline cartilage to unwanted bone, and fewer genes involved in cartilage development.
The researchers were also able to pinpoint subcategories of old chondrocytes that change their patterns of gene expression after treatment. One, which expresses 15-PGDH and genes involved in cartilage degradation, decreased in prevalence from 8% to 3% after treatment. Another, which does not express 15-PGDH but does express genes involved in the production of fibrocartilage, also decreased in prevalence: from 16% to 8% after treatment. A third population, which does not make 15-PGDH and which expresses genes involved in hyaline cartilage formation and the maintenance of the extracellular matrix necessary for its function, increased in prevalence after treatment from 22% to 42%. The findings indicate an overall shift in gene expression after treatment to a more youthful cartilage composition – without the involvement of stem or progenitor cells.
Finally, the researchers studied human cartilage tissue removed from patients with osteoarthritis undergoing total knee replacements. Tissue treated with the 15-PGDH inhibitor for one week exhibited lower levels of 15-PGDH-expressing chondrocytes and lowered cartilage degradation and fibrocartilage genes than control tissue and began to regenerate articular cartilage.
“The mechanism is quite striking and really shifted our perspective about how tissue regeneration can occur,” Bhutani said. “It’s clear that a large pool of already existing cells in cartilage are changing their gene expression patterns. And by targeting these cells for regeneration, we may have an opportunity to have a bigger overall impact clinically.”
Blau added, “Phase 1 clinical trials of a 15-PGDH inhibitor for muscle weakness have shown that it is safe and active in healthy volunteers. Our hope is that a similar trial will be launched soon to test its effect in cartilage regeneration. We are very excited about this potential breakthrough. Imagine regrowing existing cartilage and avoiding joint replacement.”
Photo by Towfiqu barbhuiya: https://www.pexels.com/photo/person-feeling-pain-in-the-knee-11349880/
Gout is the most common form of inflammatory arthritis, with worldwide prevalence of approximately 4%. The accumulation of monosodium urate crystals in gout leads to the clinical manifestations of the disease and if left inadequately treated, leads to chronic arthritis with joint damage. Due to its anti-inflammatory properties, colchicine, an alkaloid drug derived from the autumn crocus plant, is commonly used in the management of gout for both prophylaxis and treatment of gout flares.
A recent study on colchicine’s potential benefit for cardiovascular disease noted that participants who were taking the drug had fewer joint replacements than those taking a placebo. Since colchicine is commonly used in gout, researchers wondered if colchicine would lower risk of joint replacement in those with gout as well. Further, because osteoarthritis is the most common reason for joint replacement, and because osteoarthritis and gout can occur together, researchers wondered if colchicine could lower the risk of joint replacement in those with both gout and osteoarthritis.
A new study from Boston University Chobanian & Avedisian School of Medicine has found that people with gout who were prescribed colchicine had a modest 12% risk of joint replacement compared to those who did not receive the drug. Additionally, those with both gout and osteoarthritis who took colchicine had a 23% lower risk of needing joint replacement.
While it would have been ideal for a clinical trial to address the question of whether colchicine reduces the need for joint replacement in gout, it was not readily feasible to conduct such a trial of adequate sample size and duration. Therefore, the researchers used real-world evidence from a UK population-based database in which they identified people with gout, and then divided that pool into those who were newly prescribed colchicine and those who were not. They then assessed the frequency of knee and hip replacement in both groups.
According to the researchers, these findings suggest that colchicine may have benefits beyond symptom relief alone. “This observation could have broad implications for duration of colchicine use in gout, which is often limited to just the first six months of getting started on a urate-lowering therapy or limited to treatment of flares,” explains corresponding author Tuhina Neogi, MD, PhD, Professor of Rheumatology and professor of medicine at the school.
Additionally, Neogi believes these findings have implications for potential benefits of colchicine for osteoarthritis irrespective of gout, which is the most common form of arthritis and a leading reason for joint replacement surgery. “Prior trials of colchicine in osteoarthritis have been largely negative, but they likely have been too small and had too short a duration to detect potential effects,” adds Neogi who also is chief of rheumatology at Boston Medical Center.
Early treatment for people at high risk of developing rheumatoid arthritis can delay the disease for several years.
Photo by Towfiqu barbhuiya: https://www.pexels.com/photo/person-feeling-pain-in-the-knee-11349880/
Treating people who are at high risk of rheumatoid arthritis (RA) can delay the onset of the disease for several years, with benefits also continuing well after treatment has stopped. A new trial has shown that one year of treatment with the drug abatacept, a biologic therapy that targets immune cell activation, reduced progression to rheumatoid arthritis in people at high risk.
The new King’s College London study, published in The Lancet Rheumatology, builds on results from a trial reported by King’s researchers in 2024.
While the original trial followed 213 participants from the UK and the Netherlands for two years, the new study reports outcomes from an extended follow-up period of between four and eight years, making it one of the longest follow-up studies of its kind in people at risk of RA.
RA is a chronic autoimmune condition affecting around half a million people in the UK. It develops when the immune system mistakenly attacks the joints, causing pain, swelling, fatigue and long-term disability.
People at risk of developing the condition also often stop working before the disease starts, which creates employment instability and has economic consequences.
While effective treatments exist for people with established RA, there is currently no licensed therapy that can prevent the disease from developing in those at risk.
The researchers found that the benefits of just 12 months of abatacept therapy persisted well beyond the treatment period. People who received the drug took significantly longer to develop RA than those given placebo, with disease onset delayed by up to four years beyond the treatment period.
Although the drug did not permanently prevent RA, the findings show that early treatment can alter the course of the disease by postponing its development, potentially reducing the number of years people live with symptoms and complications.
Intervening early in people at high risk of RA can have lasting benefits. We have shown that this approach is safe and can prevent disease while patients are on treatment as well as substantially relieve symptoms. Importantly, it can also delay the onset of RA for several years, even after treatment has stopped. This could reduce how long people live with symptoms and complications, drastically improving their quality of life.
Professor Andrew Cope, Professor of Rheumatology in the Centre for Rheumatic Diseases at King’s College London
The study also showed that abatacept was most effective in individuals at highest risk of developing RA, identified through a blood test detecting specific autoantibodies. While these participants were at highest risk of progressing to RA they were also much more likely to benefit from early intervention.
During the at-risk phase, treatment with abatacept reduced symptoms such as joint pain and fatigue and improved overall wellbeing. But once treatment stopped, symptom levels became similar between the treatment and placebo groups, suggesting that continued immune modulation may be required to sustain symptom control.
The study found that abatacept was safe, with similar rates of serious adverse events in both the treatment and placebo groups, and no safety concerns linked to the drug.
The researchers suggest the latest findings provide evidence that early, targeted immune treatment can delay RA in people at highest risk, supporting further research into preventive approaches for autoimmune disease.
Cedars-Sinai investigators may have figured out why certain immunosuppressive treatments don’t work well in rheumatoid arthritis. In a study published inScience Immunology, scientists traced the problem to specific changes that occur in immune cells within the joints as the disease progresses.
The findings could lead to more effective therapies for the incurable autoimmune disease.
“Our discoveries point to the importance of the tissue environment in worsening rheumatoid arthritis and driving resistance to antirheumatic medications,” said Nunzio Bottini, MD, PhD, director of the Kao Autoimmunity Institute at Cedars-Sinai, professor of Medicine and corresponding author of the study.
Rheumatoid arthritis causes chronic inflammation in the joints. In other forms of autoimmune arthritis, inflammation can be relieved by targeting interleukin-17, one of several proteins that can contribute to joint inflammation.
In experiments involving human rheumatoid arthritis tissues and laboratory mice, investigators showed that, over time, the immune cells that produce interleukin-17 gradually stop making it. This finding helps explain why IL-17-targeted treatments do not work well against established rheumatoid arthritis.
“These immune cells can also change in ways that make them more aggressive and able to sustain inflammation even without interleukin-17,” Bottini said.
Changes to the immune cells appear to be driven by synoviocytes – nonimmune cells that produce the lubricating synovial fluid in the joints, according to the study.
Bottini said that the Department of Computational Biomedicine at Cedars-Sinai, particularly the laboratory of Kyoung Jae Won, PhD, played a key role in the study by contributing critical work in spatial biology, an emerging field that studies how cells function within their tissue environments.
The findings carry significant implications for treating rheumatoid arthritis, according to Joyce So, MD, PhD, chief genomics officer at Cedars-Sinai and medical director of the newly established Center for Genomic Medicine at Cedars-Sinai Guerin Children’s.
“This important new insight contributes to shifting the paradigm of how we understand rheumatoid arthritis progression and why IL-17 treatments haven’t worked as well as expected,” So said. “Only with a precise understanding of the biological mechanisms of disease can effective, precision therapies be developed. In the meantime, clinicians can help patients in early or presymptomatic stages make the most of treatments that may lose effectiveness over time.”
Methotrexate, a common medication used to treat rheumatoid arthritis, has a newly recognised useful secondary effect to lower blood pressure and potentially reduces the risk of heart disease in people with this condition.
A new study, led by Flinders University and Southern Adelaide Local Health Network (SALHN) researchers, has shown that methotrexate significantly lowers blood pressure when compared to another arthritis drug, sulfasalazine. The findings, published in Annals of Medicine, mark the first clear evidence of this effect in newly diagnosed patients.
Occurring in about one in 100 people, rheumatoid arthritis (RA) is a common autoimmune disease which leads to inflammation and pain in the connective tissue of a patient’s joints.
Over six months, the South Australian and Italian researchers followed 62 newly diagnosed adults who had not yet started treatment.
Half were given methotrexate and the other half received sulfasalazine. Researchers then measured their blood pressure, joint inflammation, and stiffness in their arteries at the beginning of the study, then again after one and six months.
Lead author of the study, Professor Arduino Mangoni, from Flinders University’s College of Medicine and Public Health, and SALHN’s Department of Clinical Pharmacology, says they wanted to see if methotrexate could lower systolic blood pressure, which indicates how much pressure your blood is exerting against artery walls when your heart beats.
“We found that methotrexate lowered systolic blood pressure by an average of 7.4mmHg compared with people taking sulfasalazine,” says Professor Mangoni, Strategic Professor of Clinical Pharmacology.
“This kind of reduction is considered meaningful because even a small drop in blood pressure can lower the risk of serious heart problems like heart attacks and strokes.”
Interestingly, this benefit did not seem to be linked to changes in either arthritis symptoms or the stiffness of arteries, suggesting that it might be helping the heart in other ways, like calming inflammation or improving how blood vessels work.
Professor Arduino says the findings are exciting because they show methotrexate might do more than just treat rheumatoid arthritis.
“We’ve known for a while that methotrexate helps with inflammation, but now we’re seeing that it may also help lower blood pressure, which is a major risk factor for heart disease,” he says.
“This could be a big step forward in how we care for people with rheumatoid arthritis.”
The researchers also looked at how genetics might play a role in how well methotrexate works and found that certain genetic traits made some people more likely to experience a drop in blood pressure while taking the drug.
“In short, if someone has specific gene variants, methotrexate might add a heart health benefit to its usual role in treating rheumatoid arthritis by the positive effect on blood pressure,” he says.
The researchers say that this opens the door to more personalised treatment options, where doctors could use genetic testing to predict who might benefit most from methotrexate’s heart-protective effects.
Study coordinator and medical scientist, Dr Sara Tommasi, says that although more research is needed to confirm these findings and understand exactly how methotrexate lowers blood pressure, the results are promising.
“The results suggest that this well-known arthritis drug could also play a role in protecting heart health, especially in people who are at higher risk due to inflammation,” says Dr Tommasi from the College of Medicine and Public Health and South Adelaide Local Health Network.
Features of immune system ageing can be detected in the earliest stages of rheumatoid arthritis (RA), even before clinical diagnosis, a new study has found which provides at-risk individuals with hope for early intervention.
The research led by academics at the University of Birmingham, delivered through the National Institute for Health and Care Research (NIHR) Birmingham Biomedical Research Centre, and published in the journal eBioMedicineshows that individuals with joint pain or undifferentiated arthritis already exhibit signs of a prematurely aged immune system, suggesting that immune ageing may play a direct role in the development of RA.
The study involved 224 participants across various stages of RA development and was funded by FOREUM and the European League Against Rheumatism (EULAR). It represents one of the most comprehensive analyses of immune ageing in RA to date.
Researchers found that patients with early immune ageing features were more likely to develop RA. These findings could lead to the development of predictive tools that identify at-risk individuals and enable timely treatment.
“We’ve discovered that immune ageing isn’t just a consequence of rheumatoid arthritis—it may be a driver of the disease itself,” said Dr Niharika Duggal, senior author of the study and Associate Professor in Immune Ageing at the University of Birmingham. “We found that people in the early stages of rheumatoid arthritis ie, before a clinical diagnosis show signs of faster immune system ageing.
“These findings suggest we might be able to intercept the disease development in at-risk individuals and prevent it from developing by using treatments that slow ageing, such as boosting the body’s natural process for clearing out damaged cells (autophagy).”
Key Findings
Hallmarks of immune ageing, including reduced naïve T cells and thymic output, were observed in patients with early joint symptoms.
An elevated IMM-AGE score revealed accelerated immune ageing in patients before RA diagnosis.
Elevated levels of inflammatory markers (such as IL-6, TNFα, and CRP) were found in preclinical stages.
Advanced ageing features, including senescent T cells and inflammatory Th17 cells, appeared only after RA was fully established.
The study suggests that targeting ageing pathways could offer new strategies to prevent RA. Future research should determine whether geroprotective drugs such as spermidine (autophagy booster), senolytics (clearance of senescent cells) and metformin (attenuates inflammation and boosts autophagy) may help slow or halt disease progression in high-risk individuals.
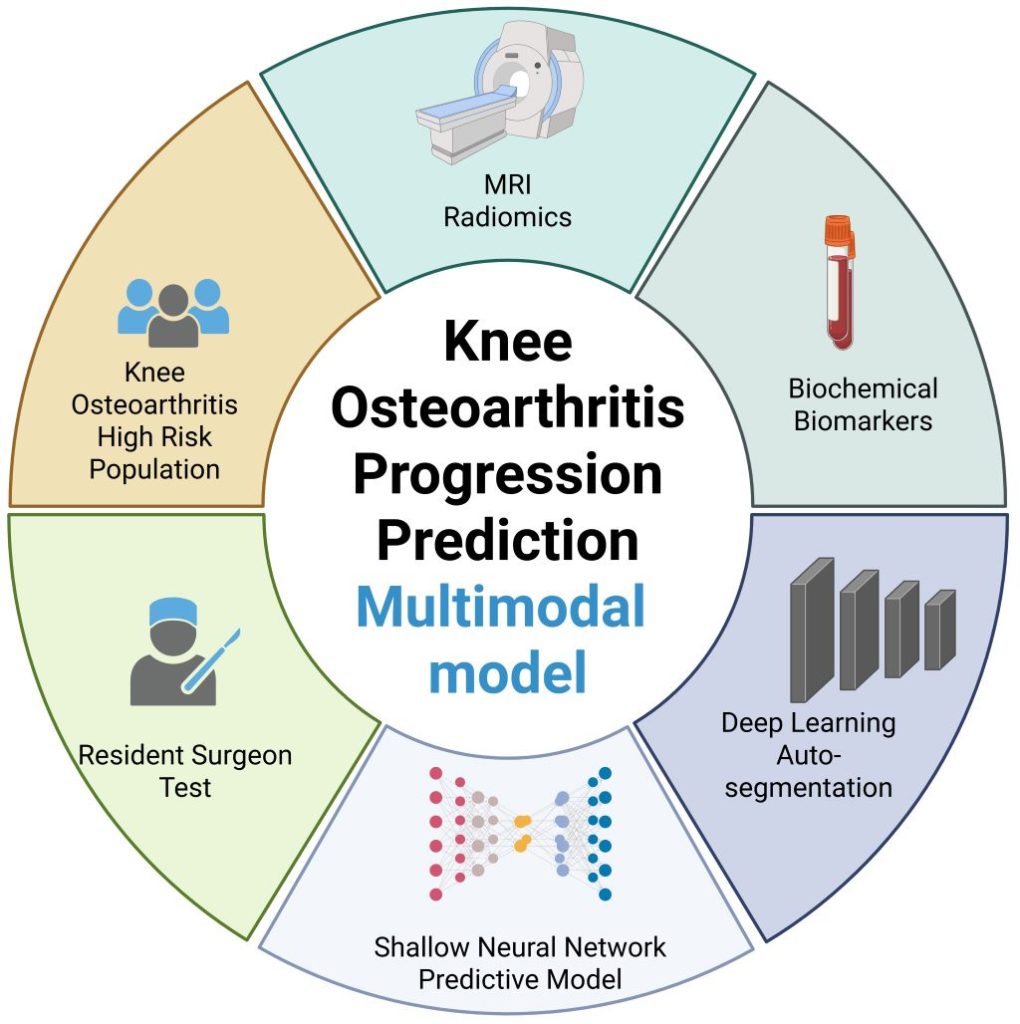
New model that combines MRI, biochemical, and clinical information shows potential to enhance care
Illustration highlighting the integration of MRI radiomics and biochemical biomarkers for knee osteoarthritis progression prediction. Created with Biorender.
Image credit: Wang T, et al., 2025, PLOS Medicine, CC-BY 4.0
An artificial intelligence (AI)-assisted model that combines a patient’s MRI, biochemical, and clinical information shows preliminary promise in improving predictions of whether their knee osteoarthritis may soon worsen. Ting Wang of Chongqing Medical University, China, and colleagues present this model August 21st in the open-access journal PLOS Medicine.
In knee osteoarthritis, cartilage in the knee joint gradually wears away, causing pain and stiffness. It affects an estimated 303.1 million people worldwide and can lead to the need for total knee replacement. Being able to better predict how a person’s knee osteoarthritis may worsen in the near future could help inform more timely treatment. Prior research suggests that computational models combining multiple types of data – including a patient’s MRI results, clinical assessments, and blood and urine biochemical tests – could enhance such predictions.
The integration of all three types of information in a single predictive model has not been widely reported. To address that gap, Wang and colleagues utilized data from the Foundation of the National Institutes of Health Osteoarthritis Biomarkers Consortium on 594 people with knee osteoarthritis, including their biochemical test results, clinical data, and a total of 1,753 knee MRIs captured over a 2-year timespan.
With the help of AI tools, the researchers used half of the data to develop a predictive model combining all three data types. Then, they used the other half of the data to test the model, which they named the Load-Bearing Tissue Radiomic plus Biochemical biomarker and Clinical variable Model (LBTRBC-M).
In the tests, the LBTRBC-M showed good accuracy in using a patient’s MRI, biochemical and clinical data to predict whether, within the next two years, they would experience worsening pain alone, worsening pain alongside joint space narrowing in the knee (an indicator of structural worsening), joint space narrowing alone, or no worsening at all.
The researchers also had seven resident physicians use the model to assist their own predictions of worsening knee osteoarthritis, finding that it improved their accuracy from 46.9 to 65.4 percent.
These findings suggest that a model like LBTRBC-M could help enhance knee osteoarthritis care. However, further model refinement and validation in additional groups of patients is needed.
The authors add, “Our study shows that combining deep learning with longitudinal MRI radiomics and biochemical biomarkers significantly improves the prediction of knee osteoarthritis progression—potentially enabling earlier, more personalized intervention.”
The authors state, “This work is the result of years of collaboration across multiple disciplines, and we were especially excited to see how non-invasive imaging biomarkers could be leveraged to support individualized patient care.”
Co-author Prof. Changhai Ding notes, “This study marks a step forward in using artificial intelligence to extract meaningful clinical signals from complex datasets in musculoskeletal health.”