New platform paves the way for patient-specific lenses in a single visit to the optometrist
A breakthrough combination of new silicone materials and advanced 3D printing technology developed by University of Waterloo researchers could transform how contact lenses are manufactured.
The award-winning innovation can produce patient-specific contact lenses in as little as 20 minutes, paving the way for specialised lenses to be designed, manufactured and dispensed during a single visit to the optometrist. The technology is described in the journal Materials and Design.
Most contact lenses are manufactured in a limited range of sizes and shapes rather than being custom-made for each person’s eye. While soft lenses are suitable for many wearers, patients with irregularly shaped corneas often require rigid lenses to achieve clear vision. Finding the right fit can require several appointments over weeks or months before patients receive lenses that fit properly and provide the function they need.
Researchers in Waterloo’s Department of Chemistry developed the digital manufacturing platform to address these challenges.
“We are very excited about this work because it brings us closer to contact lenses that are truly personalized,” said Dr Shirley Tang, professor in Waterloo’s Department of Chemistry. “Our technology produces lenses with patient-specific surfaces for a precise fit while delivering the optical clarity and mechanical performance expected of commercial contact lenses.”
The platform combines custom lens design software, a newly developed silicone material, and advanced manufacturing techniques.
Silicone is widely used in contact lenses because it is safe, biocompatible and highly oxygen permeable. However, conventional silicone materials are generally not compatible with 3D printing. To overcome this barrier, the Waterloo team developed a new hydrophilic silicone formulation specifically designed for additive manufacturing while maintaining the properties required for contact lens applications.
“Our software designs a lens with an inner surface that precisely matches the patient’s cornea and an outer surface that provides the required vision correction,” said Dr Sayan Ganguly, Chemistry research associate at Waterloo. “The novel hydrophilic silicone material we created, combined with our manufacturing process, produces smooth, transparent lenses that are comfortable to wear.”
Because 3D-printed objects are built layer by layer, tiny stair-step imperfections can form on curved surfaces and reduce optical clarity and wearer comfort. To address this issue, the team developed an ultra-thin, non-contact coating process that smooths the surface without altering the customised shape of the lens or compromising its optical performance.
Laboratory testing confirmed the lenses are biocompatible and the team is preparing for in vivo studies. Researchers have filed a provisional patent for the hydrophilic silicone material and are preparing a full patent application.
Working with the Centre for Vision and Eye Research (CEVR), a joint research institute of the University of Waterloo and the Hong Kong Polytechnic University, the researchers are advancing the technology toward commercialization.
The project recently received a Gold Medal at the Shanghai International Exhibition of Inventions in June 2026.
Sudden unexpected postnatal collapse during the first week of life is rare but can have deleterious consequences. A new study from Karolinska Institutet shows that the condition is more common than previously estimated and highlights measures that may reduce the risk.
Sudden unexpected postnatal collapse (SUPC) occurs when an apparently healthy newborn suddenly stops breathing and collapses during the first week of life. In a new study, published in the journal Acta Paediatrica, researchers investigated how common the condition is and when it occurs.
The researchers analysed approximately 483 000 births at seven maternity units in Stockholm between 2002 and 2022 and identified 149 cases of SUPC. This corresponds to 31 cases per 100 000 live births.
“It is important to remember that this is a very rare condition. According to our findings, it affects around 30 infants each year in Sweden, and two to four of these cases lead to death. Most cases occur during the infant’s first day of life,” says the study’s senior author, Eric Herlenius, paediatrician at Karolinska University Hospital and Professor of Paediatrics at the Department of Women’s and Children’s Health, Karolinska Institutet.
The study found that 81 per cent of collapses occurred during the first 24 hours after birth, with half taking place within four hours of delivery. Seven per cent of affected infants died and 26 per cent sustained permanent neurological injuries. Two-thirds of the cases occurred while the infant was sharing a bed with a parent.
“Skin-to-skin contact is important for newborn infants, but parents need to ensure that the baby’s airways are always clear and visible. Adults should not fall asleep while holding their baby skin to skin, and infants should not sleep in the same bed as their parents during the first three months of life,” says Eric Herlenius
The researchers point out that SUPC still lacks a specific diagnostic code, making the condition difficult to monitor. According to the researchers, this may have contributed to an underestimation of its true incidence.
Reviewed medical records
To identify cases, the researchers reviewed electronic medical records of infants born after at least 35 weeks of pregnancy. The records were searched for symptoms suggestive of collapse, such as episodes of apnoea, bluish skin discolouration, or sudden loss of muscle tone. Each suspected case was then assessed according to internationally established criteria for SUPC.
Since 2011, the researchers have also collected urine samples from affected infants and compared them with samples from healthy infants of the same age. They found higher levels of a prostaglandin E2 metabolite in infants who experienced SUPC during the first days of life, the same period during which most collapses occurred
“We believe that clearer guidelines for safe skin-to-skin care and safe sleep environments are needed and could help reduce the number of cases further,” says Eric Herlenius.
At the same time, the researchers aim to improve understanding of the biological mechanisms underlying the condition, including the elevated levels of prostaglandin E2 metabolite observed in some affected infants. By studying the relationship between these levels and the brainstem’s control of breathing, the researchers hope to gain a better understanding of why some newborns develop SUPC and, in some cases, sudden unexpected death.
Several tools are currently used to assess the health of older people and their risk of future health problems, but it is unclear which ones perform best. A new study published in BMC Medicine compares seven widely used geriatric assessment tools. The results show that a relatively simple tool developed by researchers at Karolinska Institutet – can be just as reliable as more advanced and comprehensive approaches.
As populations age, healthcare systems face growing challenges in identifying older adults at increased risk of declining health, care dependency, and other adverse outcomes. Although numerous assessment tools have been developed for this purpose, few studies have directly compared their ability to predict a broad range of health outcomes.
In the current study, researchers analysed data from 3108 people aged 60 years and over who participated in the Swedish National study on Aging and Care in Kungsholmen, SNAC-K. Participants were followed for up to six years.
The researchers compared seven different assessment tools commonly used in healthcare and research. They evaluated how well each tool predicted a broad range of outcomes, including formal care use, nursing home admission, hospitalisation, dementia, disability, injurious falls, quality of life, and death. The results showed that three tools – the Health Assessment Tool (HAT), Intrinsic Capacity (IC) and the Frailty Index – consistently performed best across outcomes.
The simpler tool, HAT, combines a small number of measures that are relatively easy to collect in clinical practice, including an individual’s ability to manage everyday activities, cognitive function, walking speed, and number of chronic conditions.
“Our findings suggest that relatively simple tools that capture multiple dimensions of health can effectively identify older people at increased risk of future health decline and support clinical decision-making,” says Amaia Calderón-Larrañaga, the study’s senior author and senior researcher at the Aging Research Centre, and director of the TraCeDem research centre at Karolinska Institutet.
The study also found that several widely used tools, which are often endorsed by guidelines, performed less well for certain outcomes compared to HAT, IC, and the Frailty Index.
The researchers note that the findings should be interpreted with some caution. Participants in the study were, on average, healthier and more highly educated than the general older population, which may influence how well the results generalise to other settings.
See the scientific article for information on funding and potential conflicts of interest.
Mycobacterium tuberculosis drug susceptibility test. Photo by CDC on Unsplash
By Elri Voigt
Being a researcher who studies tuberculosis in the lab is one thing, having the TB bug in your lungs is quite another. Spotlight sat down with two of a relatively small number of people who have experienced both.
One morning in April, Constance Schreuder, a senior medical technologist at a large research group at the University of Cape Town, was called into the campus’s occupational health office. “I was thinking, did I do something wrong?” she recalls.
When she got to the office, she says the doctor immediately opened the window behind him. She wondered “what is going on now?”.
The doctor told her that she has tested positive for the very illness she’s been studying at the South African Tuberculosis Vaccine Initiative (SATVI) for over two decades.
Part of Schreuder’s job involves working with post-mortem samples and tissues, as well as clinical trial samples sent from different TB research sites.
“We always protect ourselves by wearing the correct PPE [personal protective equipment]. So, we’re always safety first,” she says. “I was actually exposed [to TB] in the office where I sit. After all the years that I’ve been working in the lab.”
TB, caused by Mycobacterium tuberculosis, is typically spread when someone with the bacterium in their lungs coughs it up and those droplets are inhaled by others. The droplets are just the right size to hang suspended in the air, allowing TB to survive in a room for several hours.
Schreuder was confused by the diagnosis because she didn’t, and still does not, feel ill at all. She had been tested two months prior as a precaution after a PhD student in the lab had been diagnosed with TB and gotten very sick.
Her initial test results looked good. She had produced a sputum sample, a thick phlegm from the lungs, which was sent to the lab for molecular testing (using the GeneXpert platform). The test came back negative for TB DNA. She had also had a chest X-ray done, which showed no signs of TB in her lungs.
It was another test result that raised the alarm. In addition to the GeneXpert test, her sputum sample had been sent to be cultured. This involves putting the sample into a special tube, called a Mycobacteria Growth Indicator Tube (MGIT), and attempting to grow the bacteria if any is present. If TB bacteria has grown after around 50 days, then it means the TB bug was present in the sample. In Schreuder’s case, the TB bacteria did grow, although the bacterial count was low, a result in-keeping with her lack of symptoms.
Although she was sceptical of the result and wondered about a potential laboratory error, Schreuder’s thoughts immediately went to her close contacts – her 81-year-old mom who she sees on weekends, her pregnant daughter who lives nearby, and her son who lives with her. What did this mean for them, she wondered.
No one else from the office who had been tested showed any sign of TB disease, although Schreuder says that not everyone’s sputum sample had been cultured due to the cost of the test.
Only about one in ten people who are exposed to the bacterium will become sick with TB. In most people, the immune system contains and eventually starves the bacterium to death. In others, however, the bug survives inside the body and eventually causes illness, weeks, months, or even years later.
A silent form of TB
Schreuder very likely has what is called asymptomatic TB. This is a state where the bug is active in someone’s body, but it is not, or not yet, resulting in symptoms. There are many unknowns about this state, how much it actually contributes to TB transmission and how best to test for and treat it.
While there is much uncertainty about the prevalence of asymptomatic TB, some rough numbers exist. South Africa’s first National TB prevalence survey found that just over half of the participants with TB that was confirmed through molecular testing, did not report having any TB symptoms.
Schreuder says that she knew about TB symptoms but was under the impression that people had to show at least some symptoms if they were ill.
She says she was issued with a sick note, was told by the doctor at the occupational health office to go to a public healthcare sector clinic to get treatment, and that she was booked off for the next 14 days. People who are ill with TB generally become non-infectious after having taken TB treatment for around two weeks.
South Africa’s TB treatment guidelines does not recommend different treatment courses based on whether or not someone has symptoms. That means that Schreuder has to take the full six-month course of TB treatment.
‘I thought it was something very serious’
Schreuder’s experience is one side of the coin, the other side is a story from the same lab, one that may seem more familiar.
Tatenda Bvudzijena, an energetic young student, says he came to do his PhD at the SATVI lab because of the world class research that he felt he could learn a lot from. He shares an office space with several staff members at SATVI, including Schreuder. It was his TB diagnosis that had prompted the staff to get tested.
Bvudzijena describes himself as hard-working, so it was very unusual when he started feeling too tired to complete laboratory work near the end of 2025. He was finishing up the second year of his PhD at the time. He says he tried taking some vitamin B, but it didn’t help. Then he started to develop some of the typical symptoms of TB, persistent cough and weight-loss. The cough didn’t go away after he treated it with over-the-counter medicines.
“I had those coughing symptoms, then they disappear for a while, then it comes back again. It’s oscillating…coming back, stopping, coming back again,” he says.
Bvudzijena says a private sector doctor told him he might have asthma, but none of the medication he was prescribed – anti-inflammatories, cough syrup, antibiotics, and asthma pills – worked.
Meanwhile, he kept getting sicker.
“That’s when I was like, ‘no, this is not helping’. By that time, I had chest pains and I was losing a lot of weight,” Bvudzijena says. “I just remember back then I used to wear like a size 32 jeans…then I was wearing size 28…I was less than 55kg, but I used to be like 70kg,” he recalls.
He says he was starting to panic since the pain in his chest felt sharp. Gesturing to an area underneath his ribs on his left, he says: “I thought it was something very serious.” He adds: “At first I thought, maybe I could be having lung cancer, because I used to vape.”
Then, one Monday morning in February, Bvudzijena went to see another private sector doctor. This time he was immediately sent to get a TB test and a chest X-ray. “Your chest X-ray is showing symptoms suggestive of TB”, the doctor told him two days later.
Bvudzijena says he was both scared and relieved. He was relieved because TB can be cured and he did not have something incurable but also scared because seeing his own chest X-rays, he realised he was quite sick with TB.
Bvudzijena has to take the same six months course of treatment as Schreuder.
What taking TB treatment is like
In South Africa, “typical” or drug susceptible pulmonary (of the lungs) TB in adults is treated with a six-month treatment course – consisting of four drugs for two months and then two drugs for the next four months.
TB is mostly treated in the public healthcare sector, so even if someone has medical aid or access to private sector healthcare, they might still go to public sector facilities to get treatment.
TB treatment and diagnosis is covered under the minimum prescribed benefits for medical aid members. According to a notice by the Council for Medical Schemes, TB treatment can be made available to members of medical aid schemes through public sector clinics, but they should be given the option of getting their treatment through the private sector. Whether they can get treatment in the private sector is likely to depend on whether they can find a private sector doctor comfortable with treating TB and a pharmacy that stocks TB medicines.
Still showing no symptoms of TB when she started treatment, Schreuder says she was surprised to learn from the package insert that came with the medicine that the pills must be taken on an empty stomach. The initial two months is five tablets per day (dosage depends on a person’s weight), she explains grimacing.
She has had some side effects. At first, it was only constipation and her urine turning orange, a side effect of rifampicin, one of the four antibiotics used to treat drug-susceptible TB. But by the second month of taking the medication, she also started experiencing muscle and joint pains as well as burning feet.
Schreuder will start on the less intensive four remaining months of the course soon, when the regimen drops from four down to two antibiotics. But she worries about what the drugs might be doing to her body.
With TB already taking its toll on Bvudzijena, he says he started treatment knowing that he had to be serious about taking it as prescribed.
“I was in that situation whereby you know you’re very sick and based on the chest X-rays I was seeing, this [TB disease] was intensive. So like I had to take meds, I had to,” he says, tapping his finger on the table for emphasis.
He says he was surprised by the size of the tablets, eyes wide as he describes them. “They’re big! I’ve never seen something like that. It was my first time seeing a pill for TB,” he says.
For Bvudzijena, the side effects have been relatively mild, a runny stomach and a skin rash, as well as joint pain when he started the two-drug phase of treatment.
He says he started feeling better soon after starting treatment, got his appetite back, and his TB symptoms disappeared completely.
Two clinics, two different treatment experiences
But before they could start taking their treatment, Bvudzijena and Schreuder had to get access to the drugs, which was easier said than done.
Bvudzijena, upon getting his chest X-ray, says he was told nothing other than he needed to go to Groote Schuur Hospital. So he went, only to find that because Groote Schuur Hospital’s waiting rooms employ a triage system – where patients who are in the most critical condition are seen first – he’d likely have to wait several hours.
So, he left and later went to a doctor at another private hospital and got referred to see a specialist at that hospital. He says the specialist would have only been able to see him a week later. At his wits end, he went to campus health, who put him in touch with a nurse at a nearby public sector clinic.
Once at that clinic, he says he was well taken care of, got given a little green card, identifying him as a TB patient. This card is his ticket to travelling through the clinic quickly and not having “to wait in a long queue wearing a mask”.
“My only problem was from being diagnosed to getting help,” he says.
Schreuder, after being booked off, had Googled the nearest public sector clinic that offers TB treatment. The next day, on a rainy Friday, she drove from her home in Cape Town’s Northern Suburbs to a clinic in the Durbanville area. She wore a clean mask she had found in a bag, a remnant of the COVID-19 pandemic.
“I actually was there 06:30 in the morning because I wanted to just get it over with and start with this medication because they say if you drink it for 14 days, then you’re not infectious anymore,” she says.
At the clinic, she says she was taken to a separate room to wait by herself, as it turns out for five hours. Eventually she says she was helped by a nurse, who filled out her paperwork and took another sputum sample.
Another hour later, she says she left with six packs of TB medication, enough for the first month of treatment. But she had to stop at a private sector pharmacy on the way home because the clinic was out of vitamin B6, which she had been told to take to help with the potential side effect of “pins and needles in your hands and feet”.
Her frustrations with the system would mount. At a subsequent clinic visit Schreuder discovered that her phone number hadn’t been captured, meaning she hadn’t received the test results from her second sputum test. When she asked for her TB medicines to be dispensed to her ahead of time since she was already at the clinic, she says she was told the medicines were out of stock.
When she arrived for her next appointment at 12:00 on a Friday in May, she says the clinic seemed empty. When she eventually found a nurse, she claims the nurse told her she was only working until 12:00, and that the rest of the staff had left to attend a party for someone who had resigned, and that Schreuder must come back on Monday. A frustrated Schreuder says she didn’t accept this and eventually the nurse agreed to give her the medication.
“What’s worrying for me,” says Schreuder, “is, I said to her, ‘I work in this clinical trial lab where we want to find a cure for TB. But are we going to reach a TB free world if it [the health system] works like this?’.”
What needs to change?
Both Bvudzijena and Schreuder say it needs to be made easier for people with TB to start and collect TB treatment. They suggest that private sector pharmacies could be a convenient alternative to public sector clinics. Bvudzijena adds that stable patients could also collect their medication from selected community pharmacies or other collection points closer to home, reducing unnecessary travel and long waiting times.
He also touched on the need for better, clearer information for people who have just been diagnosed with TB about where they need to go, what documents they might need and how to start treatment.
“When you’ve just been told you have TB, you’re already worried,” he says. “The last thing you need is to be sent from one place to another without knowing where to get help.” He adds that there needs to be better coordination between private healthcare providers and public clinics.
Both touched on the stigma associated with a TB diagnosis. Schreuder says she received support from family members but otherwise it felt like people were simply checking that she had been cleared to go back to work. Bvudzijena says overall the reaction to his diagnosis was mixed. Some people like his roommates and friends were supportive, but not everyone was so understanding. “It was tough,” he says.
Change in perspective
Bvudzijena says that getting sick with TB changed his perspective on the research he’s involved with.
“What I realise now, after having TB, is that this research is about so much more than science. My work is focused on improving TB diagnosis so people can be diagnosed earlier, while many of my colleagues are working on better treatments and vaccines. After going through TB myself, I know how much that work can mean to someone who’s sick. It’s really going to change people’s lives,” he says.
To Schreuder, the experience has also been eye-opening but in a different way. She recounts some of the stories she heard while waiting at the clinic, a woman who has arrived at 05:30 but hours later still hadn’t been helped because her file was missing. A man who is afraid he’ll lose his job if he waits any longer. Patients sent to wait outside on cold benches and concrete floors, some looking very ill. Data from community-led monitoring group Ritshidze suggests that long waiting times is a common problem.
“I can fight my own battles, but what about all those that are too afraid to say something?” Schreuder asks.
Every Mandela Day, South Africans answer the call to make a difference. Across the country, people dedicate 67 minutes to uplifting others by serving meals, painting schools, planting trees, mentoring young people, and supporting those in need.
But what if your 67 minutes could leave a legacy of hope? What if they could help save up to three lives? This Mandela Day, the South African National Blood Service (SANBS) is inviting South Africans to transform a simple act of generosity into a lifetime of impact by donating blood.
Unlike many acts of service, the impact of a blood donation doesn’t end when you leave the donor centre. It continues in emergency rooms, operating theatres, maternity wards and hospital beds across the country, where donated blood gives someone another chance to recover, celebrate another milestone, and experience another tomorrow.
Every lifesaving blood transfusion begins with one person making one simple decision: to show up.
That’s why SANBS is encouraging more South Africans, especially first-time donors to become part of a community of everyday heroes whose generosity gives strangers a second chance at life.
“Whether you have donated before or have always wondered if you should, Mandela Day is the perfect opportunity to take that first step,” says Monique Schreiner, Senior Manager: Donor Relations at SANBS. “The donation process is safe, simple and takes less than 67 minutes from start to finish. Yet those minutes could mean a lifetime for someone else.”
Nelson Mandela believed that each of us has the power to make a meaningful difference through service. Blood donors live that legacy every day – not for recognition or reward, but because they understand that, somewhere, someone is depending on the kindness of a stranger.
This Mandela Day, let your 67 minutes create a lifetime of impact.
Booking operating rooms with surgical precision starts with more accurate predictions of how surgeons spend their time
Photo by Piron Guillaume on Unsplash
Researchers at the University of Massachusetts Amherst have analysed nearly 86 500 surgeries at Baystate Medical Center to identify the top factors that influence inefficiencies in surgeon schedules. Having an efficiently organised surgical schedule has the potential to lower costs and reduce surgeon burnout, which would also improve patient outcomes.
As shortfalls in the availability of surgeons grow, the ability to meet surgical demands will only worsen, with implications for both healthcare delivery and costs.
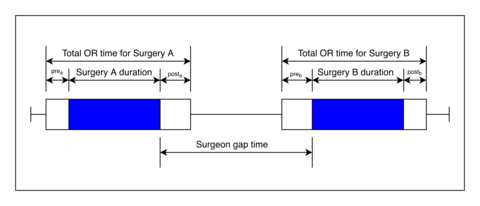
This illustrates the timeline of two surgeries performed by the same surgeon. The blue area represents the duration of the actual surgery itself, while the white blocks represent pre- and post-surgery activity. Surgeon gap time is the time interval between two operations where the surgeon is not actively working.
“The most expensive part in this process of getting a surgery is the surgeon,” says Muge Capan, assistant professor in the Riccio College of Engineering at UMass Amherst and an author of the new paper published in the Journal of the American Medical Informatics Association. “Surgeons are highly skilled and they perform high-risk tasks. When we think about utilising a resource, we don’t want them to sit idle – but we also don’t want to overutilise them because these are not machines, these are people. Finding that right balance is a challenging problem.”
However, to efficiently schedule, hospitals need to predict how long a procedure will take. This includes the surgery itself as well as many other factors that surround an operation – has the surgeon recovered from their previous operation? Is the room clean? Is the proper equipment in place? “There is a lot of uncertainty there at the system level,” says Capan.
Currently, surgeries are scheduled in blocks, which is not compatible with the unpredictable nature of a hospital. “If you’re scheduling tennis lessons, it works because a tennis lesson is exactly one hour,” says Capan. “You block the court for one hour, you play, you leave, next group. But blocks don’t make sense for surgeries, because they’re so uncertain.” As a result, operating rooms (ORs) can sit empty since any block of time less than two-and-a-half hours is unusable for most surgeries.
In the pursuit of engineering a better schedule, Capan and her team collaborated with surgeons to predict their schedule by focusing on the person, not the operating room.
Surgeons are highly skilled and they perform high-risk tasks… we don’t want them to sit idle – but we also don’t want to overutilise them because these are not machines, these are people. Finding that right balance is a challenging problem.
Muge Capan, assistant professor in the Riccio College of Engineering at UMass Amherst
“There’s so much research on the operating room itself – what happens between the time a patient leaves the OR to the time the next patient enters the OR,” says Jonathan Akhagbosu, first author on the paper and UMass Amherst industrial engineering Ph.D. candidate. “But we wanted to look at it from a surgeon’s point of view: What happens between when a surgeon finishes one case and proceeds to the next case?”
The researchers named this time between operations “gap time.” In their study, they used machine learning to analyse three years of medical records from Baystate Medical Center in Springfield to determine the characteristics of a surgery that can predict these gaps in a surgeon’s schedule.
A selection of the top factors associated with larger gap times are: if the surgeon’s previous or following case is an emergency, the preceding surgery is related to the chest (thorax), the following procedure is on the heart, or the surgery is highly demanding.
Also, the last factor on the list – the assessment of how taxing an operation is on the surgeon – the researchers used mathematical models to create a new measurement called surgical case demand. Cases fall into one of three tiers. Type 1 consists of short, scheduled procedures of low-severity illness and elective surgeries, such as the removal of fatty lumps from the skin (lipoma excision) or simple dental rehabilitation. Type 2 events are more demanding, such as a mastectomy or knee replacement. And type 3 surgeries are the most onerous: the condition is more severe and they happen during off-hour times. Examples include emergency brain or abdominal operations and spine procedures.
It’s also worth noting that eye (ophthalmology) and orthopedic surgeries were associated with shorter gap times.
Capan envisions that predicting schedules can help recapture some of this lost time. “If there’s going be a gap, let’s figure out if that gap is long enough that I could squeeze in something else,” says Capan. “This is called ‘collectible time’ in the literature. Collectible time means it’s a useful gap. So what we learned about gap time could potentially help us understand collectible time.”
Prevalence higher in rural areas in all regions, pooled data analysis of 44 countries reveals. Strong protective effects of education and delayed childbearing
Early menopause affects 1 in 14 women aged 30 to 49 living in low and middle income countries, finds a pooled data analysis of its prevalence in 44 nations published in the open access journal BMJ Global Health.
The incidence is consistently higher in rural areas than it is in urban areas across all regions and countries included in the analysis, but education and delayed childbearing strongly minimise the risk.
Women usually go through the menopause between the ages of 45 and 55, but it is considered to be early if it occurs before the age of 45, and premature if it occurs before the age of 40, note the researchers.
Early and premature menopause are major public health concerns, because they heighten the risks of cardiovascular disease, osteoporosis, metabolic disorders, cognitive decline, depression, and early death, as well as seriously affecting the quality of life, they add.
To date, research findings on the prevalence of early and premature menopause have been fragmented, focused on individual countries, and missing a detailed look at individual-level sociodemographic and reproductive factors, explain the researchers.
To close this important information gap, they drew on pooled data from the Demographic and Health Survey (DHS) for 716 648 women between the ages of 30 and 49 in 44 low and middle income countries, where menopause tends to occur earlier than it does in high income countries.
All regions of the world were included other than North and South America for which no data were available.
The researchers focused on the potentially explanatory variables of: health factors, such as age at first marriage and first birth; number of live births; terminations; community level factors, such as place of residence; and individual-level characteristics, such as age, education, occupation, wealth index and exposure to media.
The data revealed that most survey respondents were between 30 and 34 (29%),while both women and their husbands were most often educated up to secondary school level (34% and 17%, respectively). Most respondents lived in rural areas (62%).
More than a third (38%) of women married before the age of 18, and around 1 in 5 (21%) gave birth to their first child before this age. Over half the women (58%) had 3 or more children.
The overall prevalence of premature or early menopause was just over 7% (51,000 out of 716,648 women), which is much higher than previous global estimates, say the researchers, with the highest prevalence among 40-44 year olds (14%).
There was a six-fold difference between those countries with the highest and lowest prevalence, the analysis showed.
The highest prevalence was in Ethiopia, Indonesia, and Myanmar: 12%;11.5%; and just over 10%, respectively. The lowest prevalence was in Jordan, Gabon, and Armenia: just over 2%; nearly 3%; and nearly 3%, respectively.
Certain factors were associated with a high prevalence. These included giving birth before the age of 18 (11%); marriage before the age of 18 (just over 10%); no formal education (just over 9%); material disadvantage (just over 8%); no exposure to media (just over 8%); residence in rural areas (8%); and 3 or more children (7.5%).
The disparity in prevalence between rural and urban areas was consistent across all countries and regions, the analysis showed.
This “reflects fundamental inequalities in healthcare access, nutritional status, educational opportunities and occupational exposures,” highlight the researchers, adding that women in these areas are more likely to work as manual labourers and face workplace hazards, including exposure to agricultural chemicals.
Education was protective, with progressively lower odds the higher the level of education. Compared with women with no formal education, those with a college education were 58% less likely to experience an early or premature menopause. And women who were employed were 14% less likely to do so than women who weren’t working.
This is an observational study, and as such, no firm conclusions can be drawn about cause and effect. And the researchers acknowledge that their study relied on self-reported data and that they weren’t able to distinguish between natural and surgically induced menopause.
Several potentially important factors associated with menopause aren’t consistently included in the DHS survey data either, they note: smoking; alcohol intake; physical activity; diet; long term conditions; hormonal contraceptive use and breastfeeding duration; and environmental exposures.
But the health consequences of early and premature menopause will strain the health systems of low and middle income countries, particularly in South and East Asia and Pacific, and sub-Saharan Africa, point out the researchers.
“With populations in [these countries] ageing rapidly and women expected to spend an increasing proportion of their lives in the postmenopausal state, the prevalence represents a substantial and growing burden on health systems already constrained by competing priorities and limited resources,” they write.
The findings “underscore the urgent need to integrate menopause into reproductive health and non-communicable disease programmes, particularly targeting rural areas and addressing social determinants, including girls’ education and delayed marriage,” they conclude.
By Palesa Mokomele, Head of Community Engagement and Communication at DKMS Africa
For years, Black South African patients with blood cancer or blood disorders searching for a stem cell donor were told the odds were not in their favour. Their ancestry, the thinking went, carried too much genetic diversity for a donor search to reliably succeed. New research published in Blood Global Hematology says otherwise. The genetics, it turns out, are not the problem. What stands between many Black patients and a lifesaving transplant is the registry, and who is on it.
A study of nearly 57 000 South Africans mapped the HLA profiles of all four of the country’s population groups to calculate each community’s real odds of finding a match. HLA markers are what doctors use to determine whether a donor’s stem cells are compatible with a patient’s. In a same-community registry of a million donors, a Black South African patient’s probability of finding a full match is 80%. For a White patient, the figure is 81%.
The Registry Gap
The registry does not reflect the country it serves, and that gap is costing lives. South Africa is approximately 81% Black African and 7% White. In the study cohort, Black South Africans made up roughly 37% of donors and White South Africans 45%. Donor drives went where they were easiest to run, and the communities hardest to reach were left out.
The findings revealed large areas of the country where Black African donor representation is almost absent. Entire provinces contribute too few donors for researchers to meaningfully analyse matching patterns. Of the fifteen subpopulations large enough to analyse by language and province, seven were White communities.
The two least genetically diverse groups in the study were Afrikaans-speaking White people in Mpumalanga and isiXhosa-speaking Black Africans in the Western Cape. Because people in these communities are more genetically similar to one another, each new donor has a better chance of matching someone who needs them.
The registry is at least heading in the right direction. Fifty-six percent of new registrations come from people of colour. But it holds just 200,000 donors across all population groups, and the destination is a registry of a million Black African donors alone.
The Human Cost
Consider what that means for a patient like Sbahle, a six-year-old girl diagnosed with aplastic anaemia before she could pronounce the word. She has spent four years, most of her life, waiting for a donor. She is stable, back at school, and still without a match. Not long ago, a family in her position would have been told the odds were against them, and there was little to be done. We know better now.
For a patient still waiting, the donor who could save them may already be out there, alive, healthy, and simply not on the registry.
Not Everyone’s Odds Are the Same
The progress is not uniform. Coloured and Indian/Asian South Africans face a harder search: their greater genetic diversity means common profiles cover far less of the group, around 21% for Coloured patients, and full matches are rarer.
The outlook is not bleak. In a registry of 100,000 donors from their own group, a Coloured patient has roughly a 51% chance of a nine-out-of-ten match and 92% of an eight-out-of-ten. Advances in transplant medicine are also shifting what a near-match means in practice. Recent research has shown that post-transplantation cyclophosphamide, a drug used to prevent graft-versus-host disease, significantly reduces the impact of donor mismatches, to the point where a single mismatch may be clinically negligible. For Coloured and Indian/Asian patients who cannot find a full match, that development changes the calculation considerably.
From Research to Reality
This research also points to where investment should go. The biggest gains will not come from a new algorithm or a better search tool. They will come from signing up donors in the communities the registry has missed. That is slow, expensive, deeply unfashionable work, and it is the thing that actually gets a patient to a transplant.
Recruitment has to reach into Limpopo, KwaZulu-Natal, the Eastern Cape, the Northern Cape and the rural areas with no donor base at all, and it has to be permanent, not a run of once-off drives.
Science has now answered one of the biggest questions in stem cell transplantation: Black South Africans are not inherently harder to match. The challenge is building a registry that reflects the country itself. Every new donor brings that goal, and patients like Sbahle, closer.
For patients suffering from traumatic injuries that leave behind volumetric gaps – where significant bone and blood vessels are lost – the clock is always ticking. Without a nearby blood supply, cells in the centre of a large injury cannot survive, often leading to permanent tissue loss or failed grafts.
A team of eight scientists at The University of Texas at San Antonio has discovered a potential ‘perfect recipe’ to address this challenge. By blending two natural proteins found in the human body, the researchers created a specialised scaffold that allows bone and blood vessels to grow simultaneously at an accelerated rate.
The study, published in the journal Biomaterials Advances, identifies a 50:50 ratio of collagen and fibrin as the ideal environment for tissue repair.
The Lego blocks of healing
The technology relies on what scientists call interpenetrating polymer networks, or IPNs. In simpler terms, it is a microscopic support structure where different materials are entangled to create a stable foundation for new growth.
“An IPN network is two things that are entangled like a giant mess of Legos,” said Teja Guda, PhD, the Jacobson Distinguished Professor of Innovation and Entrepreneurship in the Department of Biomedical Engineering and Chemical Engineering at UT San Antonio and the study’s corresponding author. “We are leaving all the building blocks there and letting the cells build whatever Lego structure they like the most.”
In this biological ‘Lego’ set, one material is fibrin, the protein the body uses to form blood clots immediately after an injury. The other is collagen, the primary structural protein found in bones and other tissues.
Seeding the scaffold with MVFs and MSCs
To turn these protein gels into living tissue, the research team “seeded” the hydrogels with two critical types of biological starters: microvascular fragments (MVFs) and mesenchymal stem cells (MSCs). The MVFs have the capacity to grow into blood vessels, while the MSCs can, with the right environmental cues, grow into bone.
The researchers integrated these components by mixing the living MVFs and MSCs directly into the liquid protein solution before it underwent gelation. This 3D encapsulation ensured the cells were suspended throughout the entire depth of the scaffold rather than just sitting on the surface.
Balancing blood and bone
Standard medical treatments for severe bone loss typically involve autografts, where bone is harvested from another part of the patient’s body, or allografts, which use processed bone from a donor. These traditional grafts often fail to integrate because they lack an immediate blood supply to nourish the new tissue. Without rapid vascularisation, the transplanted bone can become necrotic, leading to a high rate of clinical failure in complex trauma cases.
The challenge for UT San Antonio researchers was finding the right balance between the two proteins to support both blood vessel and bone regeneration. Fibrin is excellent at recruiting the cells needed to form blood vessels, a process called angiogenesis. Collagen provides the mechanical strength needed to guide the development of bone, or osteogenesis.
“Whenever you have an injury where you are losing volume, you not only lose the tissue itself, but you’re also losing blood vasculature,” said Gennifer Chiou, a postdoctoral fellow at UT San Antonio and the study’s lead author. “We’re looking at how we can regenerate both the tissue and the vessel itself within specifically bone tissue.”
The team tested five different ratios of the two proteins. They found that while gels with more fibrin supported faster vessel sprouting, they lacked the stability needed for long-term bone growth. Conversely, high-collagen gels were too stiff for vessels to penetrate easily.
The 50:50 blend struck an ideal balance. The MVFs were able to sprout and branch out into a robust, interconnected network. Simultaneously, the MSCs developed in a stable environment, expressing the specific genetic markers needed to mature into bone-forming cells. This dual-growth approach ensures that as the new bone forms, it is continuously supplied with the blood and nutrients it needs to remain viable.
From the lab to the clinic
Because the materials used in the study – collagen, fibrin and the patient’s own blood vessels – are all naturally occurring in the body, the researchers believe the technology faces fewer regulatory hurdles than synthetic alternatives.
“There is almost nothing new in our material,” Guda said. “It’s your collagen, it’s your blood vessels, it’s your fibrin. The end goal is to provide evidence that will guide how clinicians think about healing wounds.”
The team hopes to proceed to preclinical trials in the near future, which will provide further support for the treatment to one day become standard practice.
The new dawn of managing occupational injuries as prescribed in the recently enacted Compensation for Occupational Injuries and Diseases (COID) Amendment Act 10 of 2022 puts at the forefront the need to rehabilitate injured workers. This ensures that their potential for reintegration into the world of work is maximised. Rand Mutual Assurance argues that rehabilitation must move from the margins to the centre of national workforce health strategies.
Speaking on the sidelines of the 25th Annual Board of Healthcare Funders (BHF) Conference, which took place in Cape Town from 4–8 July, Kyle Fredericks, Managing Executive: Social Insurance at RMA, emphasised that rehabilitation, reintegration and return to work were not simply clinical services, but strategic enablers of economic resilience, worker wellbeing and long-term productivity.
“Rehabilitation in the healthcare value chain has historically been treated as a downstream intervention – something that happens after an injury, after a claim, after a disruption. But the evidence is clear that rehabilitation is most effective when it is prioritised, integrated and supported from the very beginning of the occupational healthcare journey,” says Fredericks.
Rehabilitation as a driver of workforce resilience
South Africa’s labour market is undergoing rapid transformation, with new technologies, new models of employment and shifting workforce demographics reshaping how people work and the pressures they face. In this environment, the cost of prolonged recovery, delayed treatment and fragmented care pathways is becoming increasingly unsustainable.
“A resilient workforce can recover quickly, safely and sustainably from injury or illness. Rehabilitation is the engine of that resilience. It restores function, supports reintegration and protects workers from long‑term disability. When rehabilitation is integrated, the entire healthcare ecosystem strengthened,” notes Fredericks.
RMA’s position reflects a growing global consensus that rehabilitation is not an optional add‑on, but a core pillar of modern occupational healthcare. Countries that invest in structured rehabilitation programmes consistently report improved recovery outcomes, reduced compensation costs and higher return‑to‑work rates.
The consequences of fragmented rehabilitation pathways
Despite its importance, rehabilitation in South Africa remains unevenly prioritised across sectors. Workers often face delays in accessing appropriate care, limited coordination between healthcare providers and insufficient support for community or work reintegration. These gaps prolong recovery, increase the risk of complications and reduce the likelihood of successful return‑to‑work.
“Fragmentation is one of the biggest barriers to effective rehabilitation. When clinicians, therapists, employers, administrators and social insurers operate in isolation, workers fall through the cracks. Rehabilitation must be part of a connected ecosystem – one where every stakeholder understands their role in supporting recovery,” explains Fredericks.
Fredericks adds that strengthening rehabilitation requires more than clinical expertise; it requires collaboration, shared standards and a commitment to worker‑centred care. “Rehabilitation is a team effort. It succeeds when everyone is aligned around the same goal, which is restoring the worker to full participation in life and work.”
A call for stronger partnerships with healthcare professionals (and beyond)
RMA is using the BHF Conference as a platform to call for deeper collaboration with healthcare practitioners, rehabilitation specialists and allied health professionals. The organisation believes that building a robust rehabilitation ecosystem depends on strong clinical partnerships and shared ambition.
“We want healthcare professionals to understand our commitment to rehabilitation and reintegration. We are scaling our rehabilitation function significantly, and we are inviting clinicians, therapists and specialists to partner with us and recognise community-based mechanisms that make reintegration possible” says Fredericks.
“Together, we can build a rehabilitation ecosystem that is responsive, evidence‑based, and centred on the needs of workers.”
Fredericks points out that rehabilitation must be recognised as a specialised discipline that requires dedicated investment, continuous learning and integrated care pathways. “Rehabilitation is not a single event; it is a journey. And that journey must be supported by skilled professionals who understand the complexities of recovery”
Rehabilitation and the future of occupational healthcare
RMA’s advocacy for rehabilitation is part of a broader shift in the sector, which is seeing a move from reactive compensation models to proactive, integrated healthcare ecosystems. This evolution recognises that worker wellbeing cannot be achieved through compensation alone. It requires prevention, early intervention, coordinated care and structured rehabilitation.
“The future of occupational healthcare is holistic. It begins with prevention, continues through injury management and culminates in rehabilitation and return‑to‑work. Rehabilitation is the bridge between injury and recovery – without it, the system cannot deliver the outcomes workers deserve,” says Fredericks.
Fredericks adds that rehabilitation also plays a critical role in strengthening national productivity. “Healthy workers build healthy industries. When rehabilitation is strong, businesses benefit from reduced downtime, improved morale and greater long‑term stability.”