Why Pharmacists Still Can’t Prescribe ARVs, Months After Court Gave the Green Light

By Catherine Tomlinson
A Supreme Court of Appeal ruling in October 2025 cleared the way for specially trained and permitted pharmacists to dispense antiretroviral medicines without a doctor’s script. Seven months later, no pharmacists are yet providing these services. Spotlight explores the reasons for the delay.
After a three-and a half year court battle between a group of private doctors and the South African Pharmacy Council (SAPC), the Supreme Court of Appeal (SCA) cleared the way for the SAPC to implement pharmacist-initiated management of antiretroviral treatment (PIMART) in October 2025.
The SAPC welcomed the ruling with a bullish press conference promising rapid implementation of PIMART. “The South African Pharmacy Council, together with stakeholders and the Department of Health, will work with speed to ensure that PIMART-trained pharmacists join other primary healthcare practitioners in providing primary care in relation to HIV and Aids,” said Mogologolo Phasha, president of the SAPC, at the time.
Vincent Tlala, CEO and Registrar of the SAPC, also in October 2025, said that the SAPC aimed to issue an e-note inviting pharmacists to apply for the PIMART permits in November. However, seven months later, this has still not happened and no pharmacists in the country are yet permitted to provide PIMART services.
What is PIMART?
PIMART stands for pharmacist-initiated management of antiretroviral treatment. It is a form of task-shifting that allows pharmacists to provide some limited HIV services that are currently only provided by doctors and nurses. The programme seeks to better utilise pharmacists in the country’s HIV response and relieve some of the burden on overcrowded and under resourced public clinics. It will also offer a route into treatment for people who are not willing or able to visit clinics.
It is intended that, under the PIMART programme, pharmacists that have completed a dedicated training programme and have received a special permit from the Director-General of Health will be authorised to provide first-line antiretroviral treatment to people with uncomplicated HIV without a doctor’s script. They will also be allowed to dispense HIV prevention medicines without a doctor’s script – this includes both pre-exposure prophylaxis (PrEP) and post-exposure prophylaxis (PEP). PrEP is taken prior to sex to prevent potential infection while PEP is taken shortly after a possible HIV exposure to prevent infection.
Why is PIMART needed?
PIMART was proposed by the SAPC in response to a request from the health department for the SAPC to design an intervention to enable pharmacists to take on a greater role in the country’s HIV response.
South Africa has adopted the UNAIDS 95-95-95 targets that aim to ensure that 95% of people living with HIV know their status, 95% of people diagnosed with HIV are on treatment, and 95% of people on treatment are virally suppressed (and therefore cannot transmit HIV onwards).
According to new estimates from Thembisa, the leading mathematical model of South Africa’s HIV epidemic, 7.9 million people are living with HIV in South Africa. Ninety six percent of people living with HIV know their status, yet only 82% of people who know they are HIV positive are on antiretroviral treatment.
While South Africa’s health system should be commended for the fact that around 6.2 million people are taking HIV treatment, it is concerning that 1.7 million people living with HIV are not yet on treatment. In recognition of this problem, the health department has launched the “Close the Gap” campaign.
The thinking behind PIMART is that pharmacies can help close the gap by providing an important third option to people who are disinclined or unable to access HIV treatment from public clinics or private sector doctors.
More urgent than ever following US funding cuts
While PIMART was always intended to help identify patients falling through the gaps between South Africa’s public and private health sectors and to link them to care, the need for this third option is now more urgent than ever. US funding cuts over the last 15 months or so have led to the closure of many NGO-run clinics that previously provided HIV treatment and prevention services to populations at high risk of HIV who often face stigma at traditional health facilities. These groups include sex workers, men who have sex with men, and people who inject drugs.
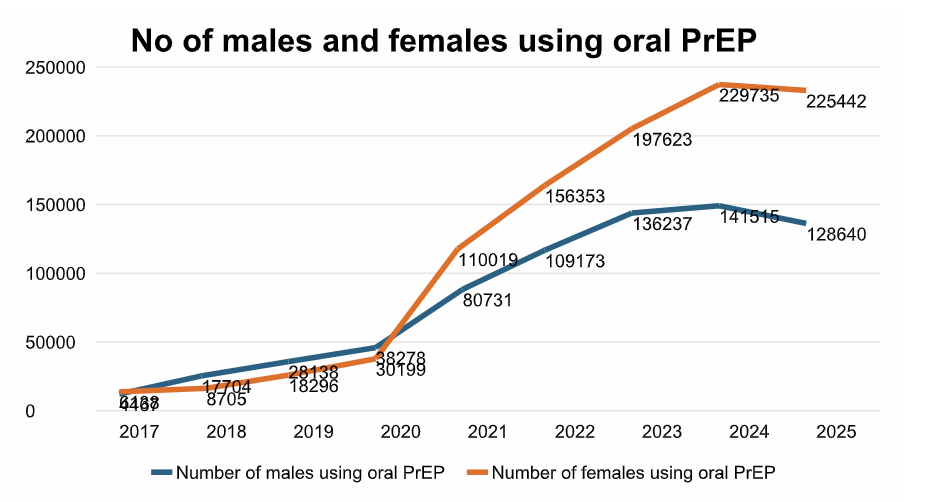
In addition to expanding access to HIV treatment, PIMART aims to increase access to PrEP and PEP to prevent new HIV infections. While the full impact of US funding cuts on these services remains unclear, the cuts likely contributed to the slight decline in PrEP use in South Africa seen in 2025, following seven years of steady growth in PrEP uptake.
Finger pointing and lack of accountability
Seven months after the Supreme Court of Appeal ruled that the SAPC could implement PIMART and the SAPC promised to move rapidly in implementing PIMART, pharmacists have still not been invited to apply for permits and no PIMART permits have yet been issued to pharmacists.
When asked why the programme remains unimplemented, the SAPC pointed to the Southern African HIV Clinicians Society’s (SAHCS) PIMART training course as the cause of the delay.
SAHCS is the only entity in the country providing PIMART training to pharmacists. In October 2025, Mokoena said several groups had expressed interest in becoming accredited to provide PIMART training. However, on 14 May 2026, Tlala told Spotlight: “While we have invited existing providers of pharmacy education in South Africa to offer (the course), the South African Pharmacy Council is yet to receive applications for the accreditation of the PIMART supplementary training course.”
He added: “Currently, the Southern African HIV Clinicians Society are the only approved provider for the PIMART short course.”
So, what’s going on with SAHCS’ PIMART training?
PIMART used to be on a very different timeline before it got tangled up in the court processes that led to the October 2025 SCA judgment. Back in July 2021, Spotlight reported that the launch of PIMART was imminent, and indeed, that was roughly the timeline the SAHCS training had been working toward.
In fact, the SAHCS has offered a PIMART training course for pharmacists that want to provide PIMART services since 2019. Professor Natalie Shellack, chairperson of the SAPC Education Committee, said in October 2025 that this course was developed jointly by SAHCS and SAPC.
Over a thousand pharmacists have completed SAHCS’s original PIMART training course as continuous professional development (CPD) training. But after the October 2025 SCA ruling, Lizeth Kruger, Dischem’s Clinical Executive, told Spotlight that due to the time lapse between the initial training and court ruling, Dischem pharmacists “will need to do a refresher course to ensure compliance and up-to-date knowledge”.
While SAHCS’s PIMART course has not yet been accredited by the SAPC as a PIMART course, it is accredited as a CPD course for pharmacists. Tlala told Spotlight in May that it has not been accredited as a PIMART course because of an identified “gap” in the course.
“The gap identified between the short course and the approved qualification standard meant that the approved provider of the short course, the Southern African HIV Clinicians Society, had to conduct a gap analysis and develop a bridging course to enable pharmacists trained in the short course to access the full PIMART scope of services,” said Tlala.
In response to questions about the “gap” in their training course identified by the SAPC, SAHCS’s CEO Dr Fiona Storie told Spotlight on 19 May: “SAHCS has completed a full review and update of the PIMART training course in line with the requirements for accreditation as a supplementary training course (i.e. not just a CPD accredited course).”
“As PIMART training was originally provided from 2019, there is a need for pharmacists to undergo refresher training since the field of HIV medicine is evolving and clinical recommendations change over time,” said Storie. She added: “SAHCS’ recommendation is that pharmacists undertake the newly updated PIMART training course as either a refresher/bridging course or, if not previously trained, as a new course.”
“SAHCS is engaging with SAPC to finalise the accreditation of the updated PIMART course as a refresher course and a new supplementary training course to make it available as soon as possible,” Storie said.
Limiting PIMART’s scope
Tlala told Spotlight that because of the “gap” in SAHCS’s training course, the SAPC has asked the Director-General of Health to grant limited scope PIMART permits.
“The Director-General: Health has been requested to issue a limited scope permit granting PIMART-trained pharmacists’ access to those services fully addressed in the short course previously delivered by the South African HIV Clinicians Society,” he said.
The health department confirmed to Spotlight that this request was received on 23 April 2026.
Neither the SAPC nor the Department of Health responded to Spotlight’s requests for clarification on which PIMART services the SAPC had proposed for inclusion in the limited-scope permits.
Angela Tembo, director of pharmacy health at the research centre Ezintsha, told Spotlight that she understands that the limited scope permits that the SAPC has requested the Director-General of Health to grant “will be limited to HIV prevention (PrEP and PEP) and not treatment”.
“Our understanding is that the delays [in implementing PIMART] relate to ongoing discussions around training requirements, accreditation processes, and the practical implementation pathway following the SCA ruling,” she added.
Tlala said as soon as the Director-General of Health approves the limited-scope permits, the SAPC will publicly communicate the launch of the PIMART programme and the services that may be accessed under such a permit.
“The full PIMART scope of services will only be available once the Southern African HIV Clinicians Society has finalised and submitted a bridging course following gap analysis or, alternatively, once another training provider is accredited to provide the PIMART Supplementary Training course,” he added.
Republished from Sptolight under a Creative Commons licence.
Read the original article.