Study shows that mechanical contraction by an app-controlled electrical device enhances wound healing
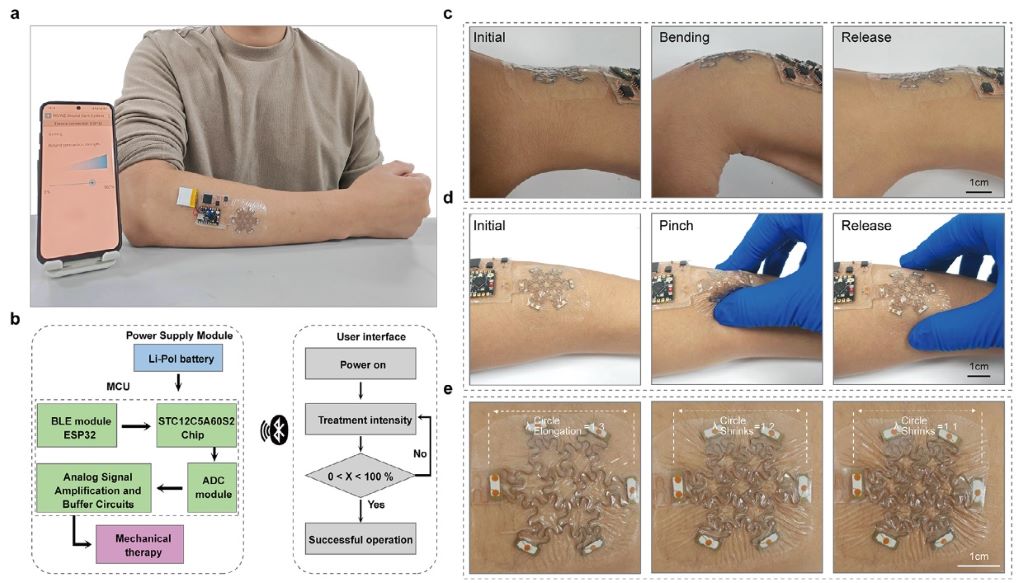
Application demonstration of MSWZ. (a) The flexible MCU of MSWZ integrates BLE communication and can be controlled by mobile terminal applications. (b) The core components of MSWZ and its manipulation logic. (c) MSWZ can work stably in high-strain areas such as wrist joints. (d) The MSWZ maintains a seamless fit to the skin. (e) The MSWZ achieves programmable mechanical contraction against human skin tension. Source: Cai et al., Advanced Science, 2026.
Skin is our protective barrier from the outside world, and it is highly susceptible to damage. To prevent infection, restore protective skin cells, and reduce scarring, it is essential to quickly and robustly close a wound. A new study, published by Wiley in Advanced Science, showed that a multi-axis stretchable wound zipper (MSWZ) is effective in closing complex wounds quickly, improving wound healing. The MSWZ uses programmable force that can be personalised via mobile application, enhancing patient comfort and compliance.
Current conventional approaches, such as sutures, cannot adapt to complex wound shapes and require healthcare professionals for their application. New alternatives, like temperature-responsive contractile dressings, are promising, yet can be unpredictable, compromised by environmental factors, and insufficient in their force to close a wound. Flexible bioelectronic systems enable precise control of mechanical contraction, though they have not yet been used in wound healing.
To utilise flexible bioelectronic systems for wound healing, researchers designed the MSWZ. The MSWZ is made up of a mechanical metamaterial in a lattice structure that shrinks and responds like human skin, a reliable conductive layer, and a breathable, flexible encapsulation material. Biocompatible and comfortable, the MSWZ stretches in six directions to accommodate complex wound morphologies, is wearable even on high-strain areas of the skin, and can be controlled through an app.
In rats, the pre-stretched MSWZ outperformed surgical suturing in the repair of linear wounds. For circular wounds, the pre-stretched MSWZ restored the epithelial barrier, decreased the wound width, and enhanced reconstruction of the collagen matrix. The MSWZ was effective in healing spindle- and oval-shaped wounds, which are most common in the clinic. Using immunohistochemistry, the researchers showed that pre-stretched MSWZ promotes blood flow to supply energy and nutrients for wound healing and supports matrix remodeling to reduce scar formation.
These findings suggest that the MSWZ enables rapid and robust wound healing at a molecular level. The MSWZ is easy to use, personalized, and programmable, adapting to complex wound types and the patient’s comfort level.
“Traditional wound closure methods, such as sutures or skin staples, not only contract in a single direction—making them unsuitable for complex wound shapes—but also fail to allow for quantification of the applied closure force. Our novel ‘multi-axis stretchable zipper’ addresses these limitations. Constructed from shape-memory alloy metamaterials, it can freely stretch in six directions to conform to any complex wound and enables precise, programmable mechanical contraction via a smartphone. We believe this technology offers an innovative solution for future wound care, ultimately alleviating patient suffering and significantly accelerating the healing process,” said senior author Yiming Zhang, PhD, of Xinqiao Hospital at Army Medical University in Chongqing, China.
Additional information NOTE: The information contained in this release is protected by copyright. Please include journal attribution in all coverage. For more information or to obtain a PDF of any study, please contact: Sara Henning-Stout, newsroom@wiley.com
Full Citation: “Multi-axis stretchable zippers for personalized wound healing.” Siyuan Cai, Guang Yao, Zijian Chen, Shiqi Zhou, Peisi Li, Liheng Lin, Huake Yang, Ziyi Zhou, Linbo Jin, Xingyi Gan, Chenzheng Zhou, Zhen Cai, Taisong Pan, Min Gao, Dongli Fan, Yuan Lin, and Yiming Zhang. Advanced Science; Published Online: June 11, 2026 (DOI: 10.1002/advs.75744). URL: http://doi.wiley.com/10.1002/advs.75744
Researchers at the Terasaki Institute for Biomedical Innovation and University of Arizona College of Medicine, have developed a topical gel formulation with 4-aminopyridine (4-AP) to treat burn wounds, achieving near-complete closure in 21 days. The findings are published in the journal Biomaterials.
Burn injuries rank among the most difficult wounds to heal. The current gold standard, transplanting skin from a donor site on the patient’s own body, is limited by donor site morbidity and the need for large amounts of healthy tissue. This research offers a non-invasive alternative: a laponite-gelatin gel that delivers 4-AP directly to the wound, concentrating the drug where it is needed rather than exposing the whole body to it. Prolonged systemic use of 4-AP can cause serious side effects, including seizures, making localised delivery a critical advance.
The drug is best known under the brand name Ampyra for treating multiple sclerosis. Earlier work showed it could influence keratinocytes and fibroblasts: the two cell types central to skin repair, but systemic administration carried unacceptable risks. Embedding it in a gel resolves that problem while preserving its therapeutic potential.
“By delivering 4-AP directly to the wound site, we harness its regenerative potential while avoiding the systemic risks that have limited its use. We believe this approach could meaningfully change how burn injuries are managed clinically,” said Dr. Johnson V. John, Assistant Professor at the Terasaki Institute for Biomedical Innovation
Laboratory tests confirmed that the gel releases 4-AP at a controlled rate, is compatible with living cells, and produces more than 90% wound closure within 48 hours. In animal studies, treated wounds closed faster than controls starting at day six, reaching near-complete closure by day 21, while control wounds remained partially open. Tissue analysis showed the gel reduced inflammation, promoted re-epithelialisation and angiogenesis, and drove fibroblast-to-myofibroblast transformation. Collagen deposition increased markedly by 438% for type I and 288 percent for type III versus controls (P < 0.05 to P < 0.0002), with an improved collagen ratio signalling better-quality tissue maturation.
Because 4-AP is already FDA-approved with a well-characterised safety profile, this repurposing strategy could accelerate the path to clinical trials compared with developing an entirely new compound from scratch.
“This research exemplifies our commitment to reimagining existing therapies to address medicine’s most persistent challenges. We look forward to seeing it advance toward clinical application,” stated Xiling Shen, Acting Director of the Terasaki Institute for Biomedical Innovation.
Giving whole blood or the component parts of blood are equally effective options for paramedics and emergency medical technicians to use in treating patients with severe, traumatic bleeding before arriving at the hospital, according to a large, nationwide trial directed by University of Pittsburgh and UPMC clinicians and scientists.
The results, published in the New England Journal of Medicine, provide flexibility to prehospital emergency care providers and could increase the odds that traumatically injured patients receive blood as soon as possible.
“Traumatic bleeding is the leading cause of trauma death and is the most time-sensitive injury a person could suffer æ more time sensitive than a stroke or heart attack,” said co-lead author Jason Sperry, professor of surgery in Pitt’s School of Medicine, and chief of trauma surgery at UPMC. “But it is preventable – and that starts with giving blood back to the injured person before they even arrive at the hospital.”
Donated blood is usually separated into parts – red cells, plasma and platelets – for storage and so the parts can be used individually as needed. When someone is bleeding, emergency clinicians will often give all or some of these parts to the patient at once. Giving either whole blood or its component parts had long been considered safe options.
But which is better for treating severe bleeding: Giving never-separated whole blood or giving the components? The answer matters for blood bank and emergency care logistics.
The multicentre trial, which ran from May 2022 to June 2025, enrolled and included 1020 severely bleeding patients who were transferred to a trauma centre by medical helicopter. The patients were randomised 2-to-1 to receive either whole blood or blood components.
The research team found no statistically significant difference between the two study arms. In both cases about a fifth to a quarter of the patients died within 30 days, compared to a third of traumatically bleeding patients who do not receive blood before arriving at the hospital.
“This is good news,” said co-lead author Guyette, who is also medical director of STAT MedEvac, which is directed by a consortium of UPMC hospitals and is the nation’s largest academic, nonprofit critical care transport group. “It means that emergency responders can use whatever form of blood is most accessible to them. In U.S. civilian emergencies that may be component blood because that is how most blood banks package it, but in military settings whole blood is often all that is available. We’ve shown that both are equally great options.”
In March, a European group announced the results of a similar, slightly smaller trial conducted in England, also published in the New England Journal of Medicine. Like the Pittsburgh team, they also found that giving whole blood or blood components was equally effective. The clinician-researchers believe that the combined findings will be reflected in guidelines set by various societies that oversee trauma care, surgery and blood handling.
Whole blood is good for 21 days after donation, so the clinician-scientists were also curious if patient outcomes were any different if they were given new blood or blood closer to the expiration date. They learned that it made no difference—outcomes were the same for patients receiving newer blood within 14 days of donation compared to those receiving older blood within seven days of expiration.
“Our thoughtful approach to the study design allowed us to not only answer the important question of the efficacy of whole blood compared to component therapy, but also to evaluate the health impact of an important public health question, the age of whole blood,” said senior author Wisniewski, who is also codirector of the Epidemiology Data Center at Pitt’s School of Public Health. “Our trial provides reassurance by verifying current standards that support the use of whole blood units throughout their entire shelf life.”
The team also noted that the findings wouldn’t have been possible without the generosity of blood donors, study participants agreeing to share their data and the hard work of emergency care providers.
“We’re very grateful to everyone involved, particularly the paramedics, emergency medical technicians and flight nurses,” Guyette said. “We are hopeful that this study and future research will give them better tools to save lives.”
Researchers at McGill University have developed a rapid way to engineer blood clots that stop severe bleeding and support tissue healing more effectively. Their technique, called “click clotting,” links red blood cell surface proteins through a chemical reaction, resulting in a biocompatible clot that is 13 times more resistant to fracturing and four times more adhesive than natural blood clots. The team said the method, described in Nature, could be used to develop life-saving biomaterials to help control severe bleeding, as well as benefit people with clotting disorders.
“Natural blood clots can be slow to form and mechanically fragile, which limits their ability to stop severe bleeding and can compromise healing,” said Jianyu Li, senior author and Professor of Mechanical Engineering and Canada Research Chair in Tissue Repair and Regeneration. “Our work shows that, when engineered appropriately, red blood cells can play a central structural role, enabling the design of stronger and more functional biomaterials.”
Shuaibing Jiang led the research during his PhD studies at McGill. He is now a Postdoctoral Associate at Mass General Brigham and Women’s Hospital, Harvard Medical School.
Researchers at the University of British Columbia, the Medical College of Wisconsin, the University of Colorado Boulder, the University of Toronto, and the Versiti Blood Research Institute also contributed.
Connected by chemical reaction
Previous efforts to crosslink red blood cells used chitosan, a polymer derived from crustacean shells, but these led to brittle clots, ruptured cells and inconsistent clotting. In “click clotting,” the clot structure is fundamentally strengthened through a fast, bio-safe chemical reaction that connects proteins on the red blood cell surface, forming a solid gel in just five seconds.
Because the “click” reaction doesn’t interfere with normal blood chemistry, it can work alongside the body’s natural clotting process. As a result, the artificial cell‑based gel, called a “cytogel,” can be added to whole blood, where it becomes embedded within the body’s own fibrin clot.
“The technology enables both autologous clots (using the patient’s own blood) and allogeneic clots (using type-matched donor blood). Autologous clots can be prepared in approximately 20 minutes, while allogeneic clots can be prepared within about 10 minutes. Given typical clinical time constraints, this approach has strong potential for in-patient emergency care, wound management and related settings,” Li said.
The results were confirmed through in vitro testing, as well as by testing on rodents. A highlight was the effective healing and regeneration observed in the injured liver, with performance exceeding that of the clinically used product tested in this study. Analysis showed minimal evidence of immune reactivity and no toxicity in major organs.
Further research required
The researchers say that while further study is required before the cytogel can be used in clinical settings, the research establishes a foundation for its design and application.
“Engineered blood clots have strong potential for broad clinical use and could improve outcomes across many medical situations,” Li said.
Icing a sprained ankle or sore muscle, long used to reduce pain and swelling, may in the longer run delay recovery and prolong pain, new research suggests.
In a preclinical study published in Anesthesiology, McGill University researchers found that even though cryotherapy (icing) eased pain in the short term, recovery time was more than doubled in some cases.
“These results highlight a paradox: treatments that reduce inflammation and relieve pain in the short term may, in some cases, interfere with the biological processes required for full recovery,” said lead author Lucas Lima, a research associate at the Alan Edwards Centre for Research on Pain.
The findings add to a growing body of research questioning the long-term benefits of common anti-inflammatory strategies, said Lima. Previous studies have shown that medications such as acetylsalicylic acid (Aspirin) can also extend the duration of pain, and animal research has suggested icing may delay tissue repair.
The new study provides, for the first time, direct evidence that icing can also affect the duration of pain itself, based on experiments with mice mimicking inflammatory and exercise-related injuries.
Icing is commonly used as part of the RICE protocol, a standard approach to managing injuries that includes rest, ice, compression and elevation. It is widely used by athletes, clinicians and in everyday injury care, but there is limited evidence for its long-term benefits, said the researchers.
“Our results suggest we need to better understand when anti-inflammatory strategies are helpful and when they are not,” said senior author Jeffrey Mogil, James McGill Distinguished Professor and E. P. Taylor Chair in Pain Studies.
He emphasized the results are not yet directly applicable to humans. A clinical trial is underway to test whether the same effect appears in patients recovering from procedures such as wisdom tooth removal.
About the study
“Cryotherapy and Duration of Inflammatory Pain in Mice” by Lucas Lima and Jeffrey Mogil et al. was published in Anesthesiology. The study was supported by the Canadian Institutes of Health Research Foundation and the Louise and Alan Edwards Foundation.
One of the study participants exerts force with their calf muscles while sensors measure electrical activity. (Photo: Ruoli Wang)
Even when people with incomplete spinal cord injuries can walk, everyday functions like standing, balancing or producing steady force may remain difficult. A new study shows why.
Using surface skin electrical sensors, a research team in Sweden identified previously unseen changes in motor coordination that result from incomplete spinal cord injuries (SCI). The study is the first to examine how individual motor units (nerve to muscle connections that create movement) work together in people with SCI.
“Our study reveals, at the cellular level, how the central nervous system adapts to the injury to control movement,” says Ruoli Wang, associate professor in biomechanics at Promobilia MoveAbility Lab, KTH Royal Institute of Technology. She says the researchers’ approach was completely non-invasive.
The study’s lead author, PhD student Zhihao Duan, says the researchers found the nervous system struggles to spread signals smoothly across muscles at low levels of exertion after the injury. And it appears to overcompensate at higher levels of exertion, sending “louder”, less refined signals.
Effect on motor units
Muscles move through hundreds or thousands of motor units, each turning on and off precisely to create smooth force. Composed of a single motor neuron and its connecting muscle fibres, these motor units respond to shared signals from the nervous system, much like different sections of musicians led by an orchestra conductor. That shared input is what allows them to act in coordinated patterns.
To explore how well these units coordinate under the control of the central nervous system, the team examined 25 people (including 10 control participants). They used high-density electromyography (HD-EMG) to measure electrical activity in the functionally similar calf muscles – soleus and gastrocnemius – while volunteers pushed lightly or moderately against a device.
Duan says that at 20% effort, fewer of the motor units in the two calf muscles were working in a shared, coordinated way compared with people without injury. As a result, their movements were shaky and unstable. “They were much less being driven by the same coordinated signal from the nervous system.” he says.
At a higher level of effort (50%) the SCI group showed stronger lowfrequency synchronization between the two muscles. The body loses flexibility and precision in control of the movement. “This could be a sign of the nervous system compensating by sending louder, less refined signals,” Duan says.
Unique insights
“One interesting finding is that after spinal cord injury the nervous system becomes more rigid and less able to change its approach as the muscles work harder. A healthy nervous system on the other hand is able to adapt its strategy as force demands, to adjust the shared neural drive level,” Wang says.
Although the study was limited by a small sample size and challenges in identifying enough motor units per muscle from the skin surface, Wang says the results offer unique insight into how SCI reshapes motor control.
“This finding may open the door to a new rehabilitation biomarker, helping clinicians and researchers design new neurorehabilitation strategies to re-tune the spinal cord control and to restore coordinated neural input,” she says.
An anterior cruciate ligament injury is a serious knee injury that often affects young, physically active people. On April 30, Dzan Rizvanovic will defend his thesis “Anterior cruciate ligament reconstruction: rationale for graft choice and treatment of associated injuries” in which he has investigated how treatment choice affects outcomes after ACL reconstruction.
“An anterior cruciate ligament injury (ACL injury) is a serious knee injury that primarily affects young and physically active individuals and can have long-term consequences for knee function, work capacity, and quality of life. Each year, a large number of patients in Sweden undergo surgical reconstruction of the injured ligament (ACL reconstruction), and this is the focus of my thesis”, says Dzan Rizvanovic, doctoral student at the Sports Medicine research group at the Department of Molecular Medicine and Surgery, Karolinska Institutet and specialist in orthopaedic surgery at Capio Artro Clinic.
“Using data from the Swedish Knee Ligament Registry, we studied tens of thousands of patients to investigate which factors are associated with different treatment strategies, and how these in turn relate to patients’ perceived knee function and the need for further surgery (revision). The thesis also has a particular focus on how the surgical volume of both the surgeon and the clinic is associated with treatment choices and outcomes”.
Which are the most important results?
“The main findings show that treatment strategies in ACL reconstruction are not solely related to the patient’s injury, but also to organizational factors. Surgeons and clinics with higher surgical volume are more likely to use different types of grafts (tendons used to replace the injured ligament), which may increase the opportunity for individualized treatment. They also repair meniscal injuries more frequently, a strategy that has been shown to be beneficial for long-term knee health. The management of cartilage injuries is also partly influenced by surgical volume”.
“Patients operated on by high-volume surgeons report better knee function two years after surgery and experience shorter waiting times from injury to surgery as well as shorter operative times. In contrast, the need for additional ACL reconstruction in the same knee is more related to patient- and injury-factors than to surgical volume”.
“The thesis also shows that graft choice influences subjective knee function at two years after surgery, particularly among females, which is an important finding”.
How can this new knowledge contribute to the improvement of people’s health?
“This knowledge can contribute to more equitable and individualised care. By clarifying how surgical experience and surgical volume are associated with treatment decisions and outcomes, healthcare systems can better organise resources and create conditions for strengthened competence and improved decision-making in ACL reconstruction”.
“The results can also be used in the dialogue between patient and surgeon to select the treatment that best matches the individual’s needs and circumstances, which in the long term may improve knee function and increase quality of life in this young and working-age population”.
“Furthermore, the results from this thesis highlight the need for discussion regarding clearer national guidelines for referral pathways, minimum surgical volume requirements, and follow-up of treatment outcomes. It is also important that reporting to national quality registers is complete and made mandatory in order to enable transparency and continuous quality improvement”.
What are your future ambitions?
“I hope to continue combining research with my clinical work to drive development forward and contribute to ensuring that patients with knee and sports-related injuries receive the best possible treatment. I also aim to contribute to a more equitable organization of healthcare, in which access to the right expertise at the right time does not depend on where in the country a patient lives”, says Dzan Rizvanovic.
Dissertation
The dissertation seminar will be held on Thursday, April 30th 2026 at 09:00, CIFU, Capio Artro Clinic, Valhallavägen 91, lecture hall house R. The doctoral thesis has been supervised by Anders Stålman.
Thesis
Rizvanovic, Dzan (2026). Anterior cruciate ligament reconstruction : rationale for graft choice and treatment of associated injuries. Karolinska Institutet. Thesis. https://doi.org/10.69622/31333828.v1
One in ten emergency patients with visible blood in their urine die within three months of presenting at A&E, new research has found. The WASHOUT study, presented Monday 16 March at the European Association of Urology Congress (EAU26) in London, found that a scan within 48 hours could reduce this risk.
Such a scan also ensured patients with cancer were diagnosed significantly faster. Around 1 in 4 people who presented at A&E with visible blood in their urine had an underlying cancer, with the most common being bladder cancer, the study found.
Around 25 000 people visit UK A&E departments each year because they have blood in their urine. Currently, patients receive different care depending on which hospital they visit or even which doctor they see. This is because there are no guidelines built on real-world evidence for doctors to follow. Based on global figures, only around half (53%) of patients receive a scan and a third (35%) receive surgery, with others discharged home or admitted to the ward to watch how their symptoms progress, says the WASHOUT study.
The WASHOUT study drew on global data to show that rapid action is critical for better patient outcomes. A CT scan or cystoscopy to look inside the bladder within 48 hours of arriving at A&E should determine the most appropriate next steps – such as whether the person should be treated for bladder cancer. Patients who didn’t receive investigative tests or appropriate treatment were 2.5% more likely to die within the next three months compared to those who did. They also spent more time in hospital and were more likely to be readmitted with the same problem within three months.
For patients with an underlying cancer, those who received investigative tests within the first 48 hours of admission were diagnosed within one day on average. In contrast, patients who were discharged without investigation faced a significantly longer wait, with diagnosis taking on average three weeks.
The research team is now taking steps to incorporate their findings into clinical guidelines, to help hospital staff provide the best treatment for these patients.
The study looked at data from more than 8500 people across 380 hospitals around the world and followed their journey for 90 days after arriving at A&E with blood in their urine. It also considered other factors that might have affected results, including age, frailty and other underlying conditions.
Nikita Bhatt, consultant urologist at St Vincent’s University Hospital, Dublin, led the research being presented at EAU26. She said: “This is the largest study exploring how we should treat people who present at A&E with blood in their urine. It’s a common problem affecting thousands of people around the world, and these patients are usually very unwell. But too often they fall through the gaps because it isn’t obviously tied to a specific disease. Our findings show how important it is that doctors take the necessary steps to identify the cause of the problem. For patients, the message is clear: if you have visible blood in your urine, don’t ignore it. See your doctor as soon as you can. If it doesn’t clear up, keep pushing until you find an answer. I hope our study gives patients the encouragement to do that.”
Jacqueline Emeks, a patient advocate on the WASHOUT study, who was diagnosed with a kidney infection and sepsis after arriving at A&E with visible blood in their urine, agrees: “These findings highlight that blood in the urine should trigger immediate action. It’s not something to watch and wait. For patients, this should mean quicker triage, earlier investigations and faster treatment, translating into safer care, fewer delays, and a better chance of avoiding severe illness or long-term harm. Patients know their bodies and deserve to be taken seriously. Blood in urine is a red flag until proven otherwise.”
Prof Dr Joost Boormans, a member of the EAU Scientific Congress Office and a urologist at the Erasmus University Medical Center, Rotterdam, said: “This is an important study highlighting the scale of the problem that emergency blood in the urine presents, both for patients and our already over-stretched healthcare systems. It’s difficult to draw strong conclusions about specific conditions because blood in the urine can be caused by many things, including cancer, and this group of patients is very diverse. But this study shows that timely investigative tests can accelerate diagnosis and reduce patients’ risk of readmission and long hospital stays, both being significantly high as shown in the WASHOUT study. As urologists in emergency care, we should be aware of these numbers and do more to get an immediate diagnosis for people with blood in urine, to reduce the burden on our healthcare systems and give our patients the best outcomes.”
Every day in South Africa, 30 people are shot dead. Another 43 are shot and survive. That is more than one person shot every 20 minutes, around the clock, every single day of the year.
Those numbers are staggering, but they don’t begin to convey the cascade of harm that extends beyond the bodies that take the bullets.
Consider this experience of Professor Sithombo Maqungo, head of orthopaedic trauma at Groote Schuur Hospital. A grandmother admitted with a fractured hip is scheduled for urgent surgery on Friday morning. As she is being prepped for theatre, a gunshot victim is rushed in, bleeding out. He dies, but the grandmother’s surgery is postponed as the weekend’s trauma cases overwhelm the unit. By Monday, her condition has deteriorated — blood clots, pressure sores, pneumonia. She dies. Her death certificate will not record “gunshot wound” as the cause. But she is, without question, a victim of gun violence.
This is the ripple effect of gun violence. One shooting does not claim one life. It consumes blood supplies, monopolises theatre time, depletes Intensive Care Unit beds, exhausts healthcare teams, and drives skilled professionals — paramedics, nurses, surgeons — out of a system that can no longer support them.
South Africa’s healthcare system is treating gun violence, it is not preventing it. And that distinction matters enormously.
Young men are the primary victims and perpetrators of gun violence, but women are increasingly killed with guns. After declining, following the Firearms Control Act of 2000, gun-related femicide has surged — rising 84% between 2017 and 2020/21. By 2020/21, firearms accounted for more than one-third of all femicides, the highest proportion recorded.
Failures in firearm oversight and the growth in licensed guns have contributed to this reversal.
South Africa’s own evidence shows that regulation works. When the Act was properly enforced between 2000 and 2010 — guided by a five-pillar strategy that tightened regulations and reduced the availability of firearms — gun deaths halved, from 34 people shot dead daily to 18, while a woman died at the hands of an intimate partner every eight hours rather than every six hours because fewer women were shot and killed.
As oversight weakened through under-resourcing, corruption and policy drift, deaths rose again.
Today, licence applications are 66% higher than in 2016, with a record 166,603 new applications in 2024/25 alone — expanding the pool of legally held guns that leak into criminal hands or are used to commit crimes.
Illegal guns don’t come from nowhere
A common misconception is that tightening firearm laws is pointless because most crime guns are unlicensed. But illegal guns do not appear from nowhere: virtually every firearm in criminal circulation was once legally manufactured and legally owned before it was lost, stolen, or sold into the illegal market. In South Africa, civilians are by far the biggest source of this leakage. Over the past 20 years, civilians have lost or had stolen an average of seven guns for every one lost or stolen by the police, according to South African Police Service annual reports. In 2024/25 alone, civilians reported the loss or theft of 7,895 firearms — 22 a day — and this is almost certainly an underestimate, since some owners do not report losses for fear of being charged with negligence (police reported the loss/ theft of 572 service guns in this time).
Legal guns are also used directly to commit crimes, particularly in domestic violence, where murder-suicides involving licensed firearms are well documented.
Controlling legal gun ownership is not separate from addressing gun crime — it is the primary mechanism for doing so.
The public health approach
A key question in response to South Africa’s gun violence crisis is why gun violence remains outside the core public health frameworks — and what would change if it were treated as the preventable health crisis it is.
A public health approach treats guns the way we treat other products that harm health — like alcohol and tobacco — moving the response upstream from treating wounds to preventing them by tightening controls over availability.
It would give healthcare workers, overwhelmed by the relentless flood of trauma, the ability to recognise that gunshot wounds are not inevitable but a preventable crisis dependent on political will and policy intervention.
It would create concrete opportunities for the health system to play a proactive role in prevention — screening for firearm access during domestic violence consultations to support gun removal from high-risk situations; linking young gunshot victims in surgical wards with gang exit programmes; using admission and forensic pathology data to identify violence hotspots and inform targeted policing.
It would make the true costs of gun violence visible to policymakers and the public — revealing how much is spent managing a preventable crisis on limited resources and overstretched facilities that could instead go towards primary healthcare, cancer treatment, or diabetes care. And crucially, it grounds the debate in evidence rather than ideology — vital in a post-truth world where beliefs, opinions, and hearsay are routinely presented as fact.
This approach would also recognise that firearms are a product sold for profit that harms people’s health. Just as taxes on alcohol and tobacco reflect their social costs and reduce consumption, firearms, ammunition and shooting activities should be subject to equivalent measures. This would generate revenue that could fund the very health services overwhelmed by the consequences of gun violence.
This sharpens the policy response too. South Africa’s Firearms Control Amendment Bill, currently at Nedlac, proposes strengthening limits on who can own firearms, the type and number of firearms and ammunition rounds that can be held, and for which purposes.
Treating gun violence as a public health crisis strengthens the case for these reforms: it positions the Bill not as a security measure but as a health measure, demanding the same urgent political commitment we would expect for any leading cause of preventable death and injury.
International framework
None of this can happen in isolation. South Africa needs international frameworks, evidence, and solidarity — and that is where the World Health Organisation (WHO) comes in.
On 10 February 2026, the Global Coalition for WHO Action on Gun Violence launched with more than 100 organisations across 40 countries, including a range of South African organisations spanning healthcare, child and women’s rights, legal advocacy, violence prevention, and research. The coalition’s formation was accompanied by a stark finding: not one of the World Health Assembly’s 3,200-plus adopted resolutions explicitly mentions firearms.
This is a profound gap. The WHO sets global standards that shape national health policy across 194 member states. When it fails to treat gun violence as a health priority, countries like South Africa are left without the international frameworks, evidence, and technical guidance they need to act.
The WHO has done this before, with other contested, politically sensitive issues — tobacco, HIV/AIDS, alcohol, violence against women — each time moving them from marginal concerns into mainstream public health priorities with measurable results. A resolution on road safety catalysed legislative reform in more than 100 countries. The Framework Convention on Tobacco Control contributed to lasting reductions in global tobacco use. The same is possible for gun violence.
The coalition is calling on the WHO to take ten key actions, including strengthening guidance on gun-related healthcare and supporting countries to use health systems as sites of gun violence prevention. South Africa — with some of the highest rates of gun violence in the world and a documented track record of evidence-based intervention — is uniquely placed not just to support this coalition, but to lead it by sponsoring a World Health Assembly resolution on firearm violence.
Our health professionals are close to breaking point. The surgeon who cannot cope with the relentless toll and resigns — leaving already stretched colleagues even more depleted. The paramedics who quit working in a war zone they never enlisted in. The medical students who leave the profession early, unable to bear the accumulated trauma of what they witness.
Gun violence is not inevitable. It is preventable. Treating it as a public health crisis is the only rational response to the evidence we already have.
Claire Taylor is from Gun Free South Africa, and Dean Peacock is from the Global Coalition for WHO Action. Views expressed are not necessarily those of GroundUp.
New oxygen-delivering technology can prevent amputations
Photo by Photomix Company on Pexels
As ageing populations and rising diabetes rates drive an increase in chronic wounds, more patients face the risk of amputations. UC Riverside researchers have developed an oxygen-delivering gel capable of healing injuries that might otherwise progress to limb loss.
Injuries that fail to heal for more than a month are considered chronic wounds. They affect an estimated 12 million people annually worldwide, and around 4.5 million in the U.S. Of these, about one in five patients will ultimately require a life-altering amputation.
The new gel, tested in animal models, targets what researchers believe is a root cause of many chronic wounds: a lack of oxygen in the deepest layers of the damaged tissue. Without sufficient oxygen, wounds languish in a prolonged state of inflammation, allowing bacteria to flourish and tissue to deteriorate rather than regenerate.
“Chronic wounds don’t heal by themselves,” said Iman Noshadi, UCR associate professor of bioengineering who led the research team. “There are four stages to healing chronic wounds: inflammation, vascularisation where tissue starts making blood vessels, remodelling, and regeneration or healing. In any of these stages, lack of a stable, consistent oxygen supply is a big problem,” he said.
When oxygen from the air or bloodstream cannot penetrate far enough into injured tissue the result is hypoxia, which derails normal healing. The researchers’ approach to preventing hypoxia with a gel is detailed in a paper published in Nature Communications Materials.
The soft, flexible gel contains water as well as a choline-based liquid that is antibacterial, nontoxic, and biocompatible. When paired with a small battery similar to those used in hearing aids, the gel becomes a tiny electrochemical machine splitting water molecules to generate a slow, steady stream of oxygen.
Unlike treatments that deliver oxygen only at the surface, the gel conforms to the unique shape of each wound, filling crevices where oxygen levels are often lowest and infection risk is highest. Before it sets, the material moulds precisely to the contours of the damaged tissue.
Equally important, the oxygen delivery is continuous. Vascularization can take weeks, so brief bursts of oxygen are not enough. The new system can provide sustained oxygen levels for up to a month, helping transform a nonhealing wound into one that behaves like a normal injury.
In tests on diabetic and older mice, chosen because their wounds closely resemble chronic wounds in older humans, untreated injuries failed to heal and were often fatal. With the oxygen-generating patch applied and replaced weekly, wounds closed in about 23 days, and the animals survived.
“We could make this patch as a product where the gel may need to be renewed periodically,” said Prince David Okoro, UCR bioengineering doctoral candidate in Noshadi’s lab and paper co-author.
The gel’s chemistry offers an added benefit. Choline, a key component, has properties that help modulate the immune system and calm excessive inflammation. Chronic wounds are often overwhelmed by reactive oxygen species, which are unstable molecules that damage cells and prolong inflammation. By increasing stable oxygen while helping rein in this immune overreaction, the gel restores balance rather than triggering further stress.
“There are bandages that absorb fluid, and some that release antimicrobial agents,” said Okoro. “But none of them really address hypoxia, which is the fundamental problem. We’re tackling that directly.”
The implications of this project extend beyond wound care. Oxygen and nutrient deprivations are major challenges in attempts to grow replacement tissues or organs, which is one of the primary goals of the Noshadi laboratory.
“When the thickness of a tissue increases, it’s hard to diffuse that tissue with what it needs, so cells start dying,” Noshadi said. “This project can be seen as a bridge to creating and sustaining larger organs for people in need of them.”
There are some factors causing the prevalence of chronic wounds that cannot be solved with a gel. In addition to climbing rates of diabetes and aging populations, UCR bioengineer and paper co-author Baishali Kanjilal notes other factors.
“Our sedentary lifestyles are causing our immune responses to decrease,” she said. “It’s hard to get to societal roots of our problems. But this innovation represents a chance to reduce amputations, improve quality of life, and give the body what it needs to heal itself.”