Stimulating a nerve in the ear may alleviate lung inflammation in mice
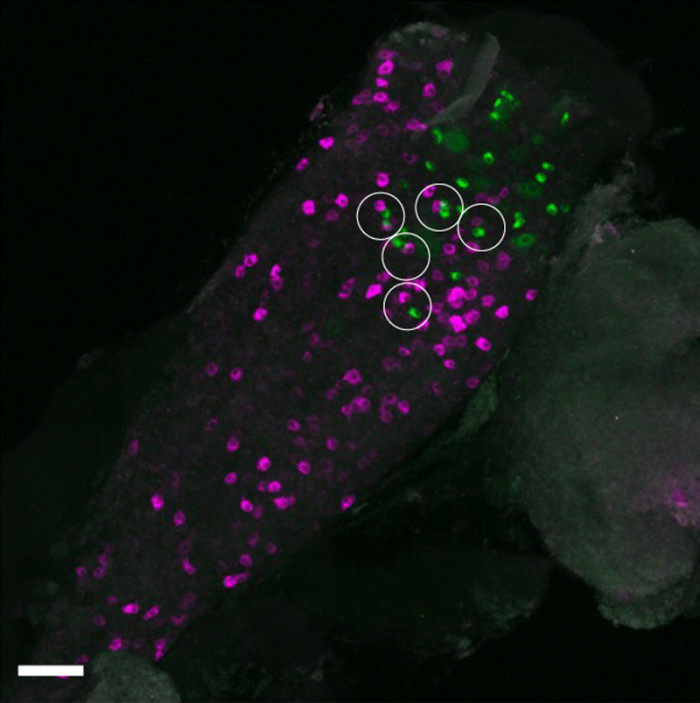
In the mouse vagal ganglion, sensory neurons labeled from the auricular skin (green) and the lung (magenta) are located in close proximity (white circles). These findings suggest a possible anatomical basis for how sensation from the auricular skin may influence airway immune responses via nerves that directly supply the lung. (Rintaro Shibuya, Kim Lab, Icahn School of Medicine at Mount Sinai.)
Neuroimmunology, the study of interactions between the nervous and immune systems, is a rapidly growing field enabling new approaches for monitoring and treating inflammatory diseases. In a recent study, scientists showed that in mice, stimulating a nerve in the external ear may help to ease inflammation in the lungs. Based on these findings, which are published in Immunity, the researchers are designing a clinical trial to test a novel device for treating asthma.
“We are always looking for new therapeutics and devices that can kickstart the body and get it back to doing what it needs to do,” says senior and corresponding author Brian S. Kim of the Icahn School of Medicine at Mount Sinai in New York. “This research suggests a new way to target the body’s inflammatory pathways.”
Neuroimmunology took off after research revealed how the vagus nerve – the ‘information superhighway’ that connects the brain to major organs and controls their functions – helps to regulate the immune system.
“The vagus nerve is hardwired to be a homeostatic organ,” says Kim. “You can think of it like a rheostat that integrates everything and keeps it in check.”
For this study, the authors leveraged the unique characteristics of the auricular vagus nerve, the only branch of the vagus nerve that reaches the surface of the skin. This nerve is found in the cymba conchae, the small, bowl-shaped depression in the upper part of the outer ear.
“Given the strong connection between the lungs and the vagus nerve, we sought to use the lungs as a test case to study these mechanisms and see whether manipulating the auricular branch could modulate inflammation,” says Kim.
The team studied these connections in mouse models using several approaches, including chemogenetics and optogenetics, to see what happened when the auricular vagus nerve was stimulated in the presence of an allergen. Their work showed that stimulation of the nerve increased levels of a neurotransmitter protein called CGRPβ in the airway. This, in turn, reduced inflammation in the lung. When the nerve fibres were instead inhibited, airway disease was exacerbated.
“Our findings reveal a previously unrecognised neuroimmune reflex linking the skin and the lung,” says first author Rintaro Shibuya of Kyoto University. “I hope this work inspires new ways of thinking about vagus nerve biology and future bioelectronic and neuroimmune therapies for inflammatory diseases.”
Although the research is in early stages, the team says this approach has many potential applications for treating diseases characterized by inflammation, including pulmonary fibrosis, inflammatory bowel disease, and rheumatoid arthritis.
“We still don’t know the extent to which the effects of stimulating the auricular vagus nerve go beyond the airway, but it’s something we will continue to study in the lab,” says Kim.
Increased brain ageing was associated with dementia, addiction and psychiatric disorders like schizophrenia
Generated with Gencraft AI
People with dementia, mild cognitive impairment, alcohol addiction, or psychiatric disorders such as schizophrenia show increased brain ageing, each in specific patterns within the brain, according to a study published July 21st in the open access journal PLOS Medicine by Shile Qi from the Nanjing University of Aeronautics and Astronautics, China, and colleagues.
Some conditions can make the brain age faster. Scientists calculate how old the brain is relative to the body using the predictive age difference (PAD), the difference between chronological age and the age predicted by brain imaging, where a positive PAD indicates that ageing is accentuated or increased. To better understand how brain disorders and divergences might affect brain ageing, the authors of this study collected structure magnetic resonance imaging (MRI) data from 45 900 controls across several brain imaging banks, and compared them with those of 2698 patients with different brain conditions and differences, including attention-deficit/hyperactivity disorder (ADHD), autism spectrum disorder (ASD), alcohol or tobacco addiction, Alzheimer’s disease (AD), mild cognitive impairment (MCI), schizophrenia, bipolar disorder or major depressive disorder.
The authors found that neurodegenerative disorders of AD and MCI had the largest association with a high PAD. Addiction and psychiatric disorders were also associated with increased PAD. In contrast, there were no differences in PAD between people with ADHD or ASD and controls.
The researchers also looked at PAD values in specific areas of the brain, and examined which genes showed increased expression in people with different brain conditions. The prefrontal cortex showed higher PAD across brain disorders. Higher PAD in the frontal and temporal lobes was associated with psychiatric disorders, while high PAD in the frontal and occipital cortex was associated with dementia. Addiction was connected with high PAD in the default mode network, and in the salience network and the putamen and thalamus. There were also differences in gene transcription that associated with specific conditions and divergences. While the results are correlational, and not causal, and while some conditions such as psychiatric disorders and addiction have high co-occurrence, the author suggest that understanding more about PAD could help provide biomarkers for commonly occurring brain disorders.
The authors add, “Different neurological disorders appear to leave different signatures on the brain ageing clock, which may help researchers better understand the neural and biological pathways involved in these conditions.”
Sometimes, doctors cannot find the cause of intracranial hypertension, a syndrome characterised by excess pressure inside the skull. Patients’ symptoms are effectively relieved by a procedure that dilates a vein in the brain… yet no one truly understands why. At the Paris Brain Institute, Stéphanie Lenck, Jean-Léon Thomas, and their colleagues have identified the mechanism behind this phenomenon. Their work, published in the journal Nature Neuroscience, sheds new light on the links between venous flow and the drainage of brain fluids, opening new therapeutic avenues.
Idiopathic intracranial hypertension (IIH) is a rare and poorly understood neurological disorder that affects 1 to 20 people per 100 000 – most often women of childbearing age. It is characterised by increased pressure inside the skull, in the absence of a tumour or any other identifiable cause. Patients typically present with a narrowing of the venous sinuses – large veins located in the dura mater, the fibrous membrane that envelops the brain and spinal cord – as well as poor circulation of brain fluids.
Patients live with chronic headaches, often accompanied by visual disturbances, tinnitus, dizziness, and severely disabling cognitive difficulties.
“When intracranial pressure is so high that it damages the optic nerve, patients receive emergency treatment to preserve their sight. However, other symptoms—sleep disorders, attention difficulties, and chronic fatigue—are often overlooked, even though they profoundly affect quality of life, sometimes for years. We still do not know why these symptoms vary so much from one patient to another and do not always match abnormalities seen on MRI,” explains Stéphanie Lenck (AP-HP), an interventional neuroradiologist at the Pitié-Salpêtrière Hospital and a researcher at the Paris Brain Institute.
Understanding the mechanisms of the disease is therefore essential for refining diagnosis and improving patient care in the short, medium, and long term.
A Closer Look at Meningeal Lymphatic Vessels
One effective treatment for IIH involves dilating narrowed venous sinuses using a stent, a small mesh tube that restores blood flow and venous pressure in the brain. In most cases, after a brief adjustment period, intracranial pressure drops and symptoms subside. Yet the mechanism behind this improvement has remained unclear: what is the relationship between veins and intracranial hypertension? Why is this intervention so effective?
To find out more, Stéphanie Lenck, Jean-Léon Thomas, and their colleagues followed 16 female patients with IIH and 20 healthy female volunteers, all of whom underwent thorough MRI examinations. In parallel, the researchers developed and studied a mouse model with altered cerebral venous flow.
Their findings are unequivocal: the circulation of brain fluids, including cerebrospinal fluid, is closely dependent on blood flow in the venous sinuses.
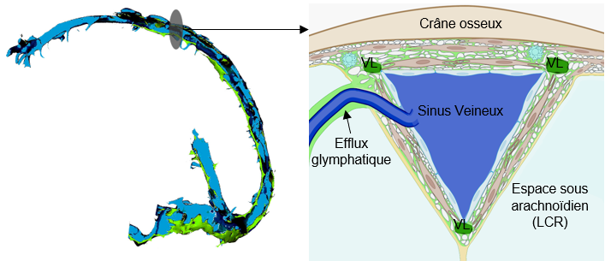
The brain’s drainage and immune surveillance rely on a network of specialized vessels: the meningeal lymphatics. They line the perisinus, an anatomical space between the outer layer of the dura mater, which is attached to the skull, and the inner layer, which runs alongside the venous sinuses. These delicate, highly environment-dependent vessels only function when blood flow in the large dural veins is normal.
Jean-Léon ThomasYale University, Inserm
When the venous sinuses are narrowed, venous pressure rises upstream, and fluid circulation in the perisinus is impaired. Brain fluids accumulate, causing the brain and skull of patients to swell under pressure. In mice, the lymphatic vessels can regress until they disappear entirely.
Because meningeal lymphatic vessels also regulate brain inflammation and immune surveillance, this regression is likely to have multiple consequences for the brain. These findings, therefore, open new avenues of research.
“Our findings could shed light on the mechanisms of sleep, a period during which the glymphatic system is activated. This waste-clearance system of the central nervous system is closely connected to the meningeal lymphatic vessels,” the researcher adds.
Draining the Brain: A Well-Oiled Machine
For the past decade, we have known that brain drainage and detoxification are partly driven by cerebrospinal fluid, which circulates through two complementary transport routes: the glymphatic system and the meningeal lymphatic vessels. This brain-cleansing system is activated during sleep, promoting a daily detoxification of the tissues.
Essential for immune surveillance and the removal of waste, including toxic proteins, these two pathways could influence the course of several neurological conditions, such as neurodegenerative diseases, multiple sclerosis, and glioblastomas. A better understanding of how cerebral clearance works could therefore lead to new therapeutic approaches.
Dural venous sinuses. Left: general side view. Right: frontal section at the level of the superior sagittal sinus. The blood leaving the brain flows through the venous sinuses (in blue). These sinuses are surrounded by the perisinus, a thin region of the dura mater where small lymphatic vessels (LV) run. In this region, glymphatic fluid – responsible for clearing waste from the brain – drains before reaching the cervical lymph nodes via the lymphatic vessels.
Science, Health, and Prejudice
Idiopathic intracranial hypertension occurs mainly in obese or overweight women, following rapid weight gain. It is still unknown why. This uncertainty contributes to the stigmatization of patients, who are sometimes unfairly blamed for being responsible for their own illness. Such prejudice can lead to inadequate care, an underestimation of the severity of symptoms and a downplaying of patients’ complaints, who may then withdraw and develop depressive symptoms.
The disease remains largely underdiagnosed, probably because it is poorly understood. Too often, only the objective symptoms are considered, such as a cerebrospinal fluid leak or papilledema—that is, a swelling of the optic nerve. Yet IIH should be regarded as a neurological condition in its own right, one that has a major impact on brain function… and not as a mere collection of isolated symptoms. Patients describe their illness very well. Let us listen to them! They are highly committed and have contributed enormously to our team’s advances, notably through the AFHTIC patient association.
Stéphanie LenckInterventional neuroradiologist at the Pitié-Salpêtrière Hospital and a researcher at the Paris Brain Institute
There is probably a genetic predisposition to the disease, to which hormonal factors contribute. Moreover, in women, the meningeal lymphatic network is less developed than in men, making them more vulnerable to damage to these vessels. This may explain their over-representation in IIH – but also in other diseases, such as meningiomas.
But what link could there be between weight gain and the onset of intracranial hypertension?
“Lymphatic vessels play a key role in the transport of fats. In cases of excess weight, their function may be disrupted. There is a lead worth exploring here,” the researcher concludes.
Reduced volume was found in areas of the brain connected to memory formation, indicating a potential link between TV watching and higher dementia risk
“Turn off that TV, it’ll rot your brain!” has been a household refrain for decades. While “rot” might be too strong a term, researchers are finding that the overall sentiment could have some merit.
A study published recently in Alzheimer’s and Dementia: Journal of the Alzheimer’s Association revealed that those who reported watching TV “very often” in midlife later exhibited reduced volume in areas of the brain associated with memory, smaller frontal and occipital lobes, and areas of damage in the brain’s white matter that are associated with aging, stroke risk, cognitive decline and dementia.
“For years we’ve focused on how much people sit. Our findings suggest we should also pay attention to what they’re doing while they’re sitting,” says David Raichlen, professor of biological sciences and anthropology at the USC Dornsife College of Letters, Arts and Sciences and a senior author of the study.
The findings weren’t just due to TV viewing’s sedentary nature. The study found that other types of sedentary activities did not have the same associations, indicating that what one does while sitting may matter much more than previously thought.
Watching changes
The researchers analyzed data from about 1,700 adults, average age 53, who enrolled in the Atherosclerosis Risk in Communities (ARIC) Study between 1987 and 1989. ARIC is a long-running study of the U.S. population designed to investigate cardiovascular and brain health.
Participants were asked how frequently, on a scale ranging from “never/seldom” to “very often,” they watched television during their leisure time and how much of their workday they spent sitting.
More than two decades later, participants underwent brain MRI. Compared with people who reported “never” or “seldom” watching TV, those who watched TV “very often” showed widespread structural differences across the brain.
The researchers found smaller volumes in areas associated with early signs of Alzheimer’s disease and more white matter hyperintensity volumes, an indicator of cerebral small blood vessel disease associated with cognitive decline and dementia. These participants also had smaller occipital and frontal lobes, regions associated with visual processing and executive functioning.
Differences persisted even when the researchers controlled for factors such as physical activity, diabetes, body mass index, smoking, and alcohol use.
Of note, the researchers relied on self-reported data for TV consumption, which can be less precise than timed tracking. Study participants also did not undergo a baseline MRI. Future research could begin with a baseline MRI to more concretely demonstrate changes over time.
Not all sitting is made the same
Strikingly, the sedentary element of TV watching didn’t appear to be the main driver for these changes.
Those who reported high amounts of sitting at work actually had larger frontal and occipital lobes, as well as reduced white matter hyperintensity volumes, indicating better brain health than among those who sit to watch TV. This could be due to the intellectually stimulating nature of many sit-down jobs, say the study authors.
Men appeared to be particularly vulnerable to these changes. When the MRI scans were separated by sex, researchers found that most of the changes to the brain, both from TV watching and occupational sitting, were seen in men.
Such findings indicate there is still more research to be done on this complex topic. However, we might eventually see a different approach to health guidance around sedentary activities. Rather than just directing their patients to move more, for example, physicians might recommend they reduce television time and add cognitively engaging activities for when they do sit.
“We frequently encourage the public not to spend too much time sitting down, but experts may want to expand that recommendation to encompass the activities done while sitting, since those seems to have distinct impacts on brain health,” says study corresponding author Natan Feter, postdoctoral scholar in the Human and Evolutionary Biology program at USC Dornsife.
Findings that neurons in mice are mostly generalists, instead of specialised for specific functions, has scientific community abuzz
A healthy neuron. Credit: NIH
What scientific findings proved so compelling that more than 11 000 preliminary copies of them have been downloaded before they finally appeared in the latest issue of Nature?
The new research focuses on a mystery as old as neuroscience. Is each neuron in the brain a specialist devoted to a limited task, like a hammer or a saw, or do they tend to be generalists, jacks-of-all-trades like Swiss Army Knives?
By combing through a trove of recordings from an international collaboration that analysed the brains of mice, researchers at Columbia’s Zuckerman Institute reveal that specialist neurons certainly do exist, but the majority appear to be generalists.
“We have to move away from this image of the brain as a machine made of gears, with every gear having an exact purpose that we can attach a label to,” said Stefano Fusi, PhD, a principal investigator at Columbia’s Zuckerman Institute, a member of the Kavli Institute for Brain Science and the paper’s co-senior author. “The brain doesn’t work like that. Instead, most neurons can display a huge diversity of responses, and this can help the brain solve a huge number of different tasks.”
These new findings shed light on how the brain may ultimately prove capable of performing complex tasks. In doing so, they may help reveal what happens when something goes wrong in the brain, and how those processes might be steered to go right again.
Whether neurons are specialists or generalists “is an old, important question, and one which researchers have really strong opinions on,” said Lorenzo Posani, PhD, the study’s co-lead author and a principal investigator at the Paris Brain Institute and France’s CNRS, who conducted this work while at Columbia’s Zuckerman Institute. Previous research found the brain is organised into modules devoted to vision and smell and other processes; so perhaps such specialisation might extend all the way down to the level of neurons. On the other hand, the brain is an incredibly powerful general-purpose computer that can respond in an extraordinary number of ways to a huge variety of situations, so maybe its neurons are similarly generalist in nature.
The problem with answering this question was that scientists often each tackled it with different approaches – for instance, they looked at different types of animals or brain regions or had the animals perform different tasks, Dr Posani said. This often led to conflicting results – in some studies, some neurons were clearly specialised, while others appeared not to be.
To help resolve the debate, in the new study, the researchers developed a strategy where they looked only at mice, across many brain areas at once as the rodents all performed the same type of activity. This involved analysing datasets much larger than typically studied, recordings of lots of neurons from the International Brain Laboratory consortium of activity in 43 regions across the mouse cortex on the level of single neurons.
In primary sensory areas, such as the brain region devoted to vision, neurons behaved in specialised ways. However, elsewhere, neurons generated far more diverse responses. In other words, when it comes to the question of whether neurons are typically specialists or generalists, these new findings suggest the latter holds true.
“We’re not saying that there are no specialised neurons,” said Dr Fusi, also a professor of neuroscience at Columbia’s Vagelos College of Physicians and Surgeons and a member of Columbia’s Center for Theoretical Neuroscience. “We’re saying they are the exceptions. They’re not the rule.”
The scientists did find that based on a neuron’s pattern of responses to a given task, they could pinpoint with surprising accuracy which specific module in the brain it belonged to. However, these neurons still generally display generalist behaviour.
“For example, compare this to maps of voter opinions,” Dr Posani said. “There are clear clusters where people generally vote the same way. But when you zoom in, you see mixes of opinions.”
In addition, not only are most neurons generalists, but they rarely duplicate the behavior of one another. “Each is versatile in its own way,” says study co-lead author Shuqi Wang, a doctoral student at École Polytechnique Fédérale de Lausanne in Switzerland. This helps enable the brain’s flexibility and computational power, she explained.
All in all, the researchers suggest the multi-purpose nature of most neurons lets each of them encode information about multiple variables, such as whether a shape is red or black, or a circle or square. In turn, neurons collectively encode “high-dimensional” representations, which combine several different variables at the same time, such as, say, a red circle or black square. Such high-dimensional representations let populations of neurons behave flexibly in terms of what input they receive and output they generate. “You can reuse these high-dimensional representations for lots of different tasks,” Dr Fusi said.
A key implication of these findings is that while each neuron generally encodes multiple variables, it is difficult to decode what any of these variables are from an individual neuron. It is only upon examining populations of neurons, like the brain does, that variables can be decoded. This is a major shift in thinking for the neuroscience community, “which for decades focused on one neuron at a time, discarding all neurons whose responses could not be understood,” Dr Fusi said.
The scientists are now working with Ueli Rutishauser‘s group at Caltech to investigate whether similar results are seen in humans, Dr. Fusi said. They also would like to see if neurons behaved more as generalists or specialists depending on what tasks a brain is asked to perform, he added. “There is still a lot to discover,” he said.
A night without sleep produced increased markers of connections between brain cells, showing that sleep in humans may be important for restoring cellular balance in the brain, according to a study published June 23rd in the open access journal PLOS Biology by David Elmenhorst from the Forschungszentrum Jülich Institute of Neuroscience and Medicine in North Rhine-Westphalia, Germany, and colleagues.
Scientists have long wondered why exactly humans and other animals need to sleep. One potential mechanism is that sleep is required to restore synaptic connections and homeostasis in the brain. Synapses – the connections between brain cells – become stronger during wakefulness. This increases the amount of energy the brain needs and leads to buildup of proteins in the brain. Sleep is thought to reset these levels, reducing synaptic connections and restoring homeostasis, but evidence has thus far been limited to animal models. To determine whether the synaptic homeostasis hypothesis is supported in humans, the authors of this study used positron emission tomography (PET) to look for markers of synaptic vesicle glycoprotein 2A (SV2A), a marker of brain synapses in 40 participants, half of whom had gone one night without sleep.
The authors found that after 28 hours of continuous wakefulness, the sleep deprivation group had higher measures of SV2A in several brain regions, including the hippocampus (an area important for memory), and the thalamus, an important information relay in the brain. When the sleep-deprived participants were allowed a two-hour nap, higher levels of SV2A were associated with more slow wave activity during sleep, a marker of deep sleep and sleep pressure. While SV2A is only a proxy for brain cell connections and the elevations were relatively small, the results support the synaptic homeostasis model of sleep, and suggest a biological connection between the need for sleep and the buildup of cell connections.
The authors add, “During sleep deprivation, the brain remains awake longer and continues to process stimuli and information. Our study shows that after approximately 28.5 hours of wakefulness, a marker for synaptic density increases in several brain regions. This suggests that sleep deprivation not only causes fatigue but is also accompanied by measurable changes in neural connections.”
Study demonstrates the potential of personalised assistive technologies for people with impaired hand function
Researchers at the Medical University of Vienna, in collaboration with ETH Zurich, the Technical University of Munich and Medical Faculty Belgrade, have developed a wearable neurorobotic system that combines electrical neurostimulation with hand exoskeletons. In a clinical trial involving 14 patients with hand impairments caused by neurological injury, the technology supported finger mobility, tactile perception and grip control. The results demonstrate the potential of personalised assistive systems for people living with the consequences of spinal cord or brain injury. The study has recently been published in the journal Science Advances.
Hand movements and the sense of touch are essential for everyday activities such as grasping, eating, dressing or personal hygiene. However, after damage to the central nervous system, motor and sensory impairments of the hand often persist. Conventional rehabilitation can achieve improvements, but does not always lead to sufficient restoration of hand function. There is therefore a great need for assistive technologies suitable for everyday use.
A research team led by study director Stanisa Raspopovic from the Center for Medical Physics and Biomedical Engineering at MedUni Vienna has developed the “SensoExo” system for assisting people with hand sensorimotor impairements. It combines a wearable hand exoskeleton with a custom-fitted neurostimulation sleeve. The sleeve stimulates specific nerves and muscles in the forearm through the skin. Sensors on the fingers detect touch and gripping forces and translate this information into electrical stimulation, providing users with tactile feedback. In addition, functional electrical stimulation can assist users open and close their fingers more easily.
“Our aim was not only to provide mechanical support for movement, but also to restore their sense of touch,” says Stanisa Raspopovic. “The interplay of strength, movement and the sense of touch is crucial, particularly when gripping. Without feedback on how firmly an object is being held, hand function remains significantly limited in everyday life.”
Individualised support depending on the impairment
The system was tested on 14 patients with neurological hand impairments. All study participants exhibited sensory deficits and therefore received tactile feedback via transcutaneous electrical nerve stimulation. In seven individuals with particularly severe motor impairments, functional electrical muscle stimulation was also used to support hand opening and grip strength.
The study compared three conditions: no support, support from an exoskeleton alone, and the combined use of an exoskeleton and neurostimulation. Eight of the 14 participants also completed functional grasping and releasing tasks with bulky and fragile objects. This investigation revealed that the combination of exoskeleton and neurostimulation provided additional benefits compared to an exoskeleton alone. In patients with severe motor impairment, SensoExo improved finger mobility to a greater extent than the exoskeleton alone. The artificially mediated tactile feedback also increased the areas of the hand where touch sensations could be perceived.
“The results show that motor assistance and sensory feedback must be considered together,” explains lead author Andrea Cimolato from the Center for Medical Physics and Biomedical Engineering at MedUni Vienna. “The system can be adapted depending on the individual’s impairment profile. People with more severe motor impairments benefited particularly from additional motor support, while those with pronounced sensory loss used the sensory feedback to grasp fragile objects more precisely.”
Improved grasping of everyday objects
In the functional tests, participants using SensoExo achieved the highest success rates when grasping and carrying objects. With bulky objects, muscle stimulation supported grip strength. With fragile objects, sensory feedback helped to avoid applying too much pressure.
“The technology is currently a prototype and not a fully developed medical device for everyday use,” emphasises Raspopovic. “However, the study provides early clinical evidence that non-invasive neurostimulation combined with wearable robotics can form a realistic basis for future personalised assistance systems.”
Primary CNS lymphomas in immunocompromised patients are among the rarest and at the same time most aggressive cancers – yet evidence-based recommendations for diagnosis and treatment have been lacking. An international research team led by Heidelberg Faculty of Medicine at Heidelberg University and the German Cancer Research Center has now identified characteristic imaging features of these tumours and developed a prognostic model to better assess disease outcomes. The researchers found that tumours positive for Epstein-Barr virus were associated with particularly poor prognosis. The findings, published in the journal Blood, may help guide future diagnostic and treatment strategies.
Primary CNS lymphoma is a rare cancer that arises from malignant white blood cells. Affected individuals develop tumours in the brain and, more rarely in the spinal cord, the eyes, or within the cerebrospinal fluid. These lymphomas can occur in people with weakened immune systems, for example after organ transplantation, in autoimmune diseases, or in association with HIV infection. This subtype, known as immunodeficiency-associated primary CNS lymphoma (ID-PCNSL) affects approximately 50 people per year in Germany. Researchers at the Heidelberg Faculty of Medicine at Heidelberg University had already shown in earlier work that ID-PCNSL is not simply a variant of classical CNS lymphoma, but a distinct disease entity characterised by specific genetic alterations.
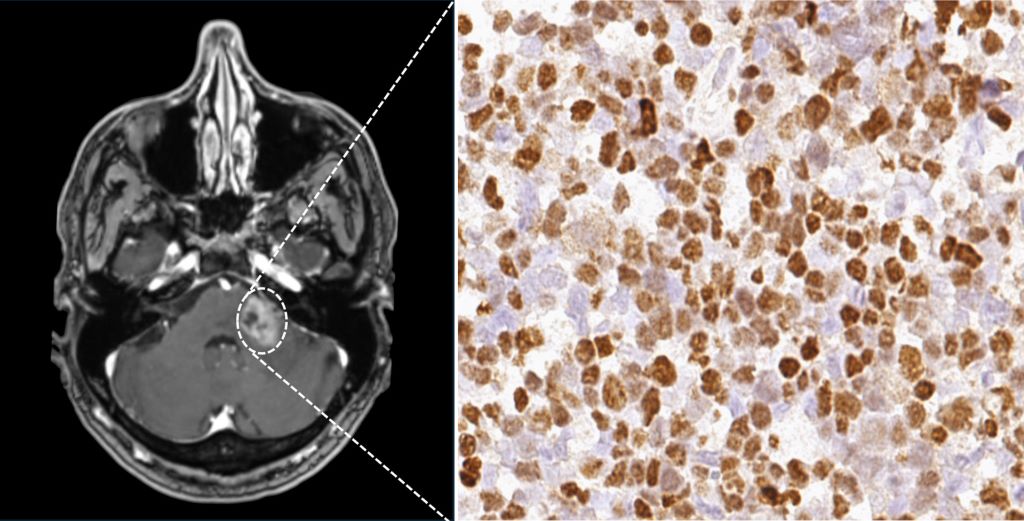
A recent study by the International Primary CNS Lymphoma Collaborative Group – an international network dedicated to the study of CNS lymphomas – has now provided further insights into the diagnosis and treatment of ID-PCNSL. Including data from 308 patients treated at 23 hospitals across seven countries, the study is the largest conducted to date on this rare cancer. The researchers analysed clinical findings, magnetic resonance imaging scans, and tumour tissue samples. Scientists from the Heidelberg Faculty of Medicine at Heidelberg University and the German Cancer Research Center (DKFZ) played a leading role in the study.
Epstein-Barr Virus influences imaging and prognosis
Epstein-Barr virus (EBV) is known to play a central role in this cancer and was detected in 79.2 percent of the tumours examined. “Our analyses show that EBV-positive tumours often follow a more aggressive course and are associated with an unfavourable prognosis,” says first author Dr Leon Kaulen. He conducts research at the Heidelberg Faculty of Medicine at Heidelberg University and at the DKFZ and is a physician at the Department of Neurology at Heidelberg University Hospital (UKHD). EBV-positive tumours also showed characteristic imaging features including different patterns of contrast enhancement compared with EBV-negative tumours.
The researchers developed a prognostic model based on three factors that can help to better predict the course of ID-PCNSL and patient survival more accurately. The three identified factors are the detection of EBV in tumour tissue, age, and the patient’s performance status. Depending on the combination of these three factors, disease courses differed markedly among the patients studied. If only one of the three risk factors was present, the median survival was 135 months. With two risk factors, it decreased to 29 months. If all three factors were present, median survival was reduced to three months. “The prognostic model, with its clear stratification, represents a major advance. It will enable us to assess patients much more precisely in the future and to tailor therapies more effectively to the individual clinical situation,” says senior author Professor Wolfgang Wick, Heidelberg Faculty of Medicine at Heidelberg University, Chair of the Department of Neurology at UKHD, and Head of the Clinical Cooperation Unit Neurooncology at DKFZ and UKHD.
Considering immunodeficiency and cancer together
So far, no standardised therapy has been established for patients with immunodeficiency-associated primary CNS lymphoma. “Our research provides important insights into which approaches may be associated with more favourable outcomes,” says Dr Leon Kaulen. Patients whose immune system could at least partially be reconstituted – for example through adjustment of immunosuppressive medication or effective treatment of HIV infection – and who additionally received combination chemotherapy with rituximab and methotrexate typically (85 percent) responded well to treatment. In a substantial proportion of patients, the disease also remained stable in the long term and became undetectable.“ Our data suggest that the interplay between the tumour and the weakened immune system plays a central role,” says Dr Kaulen. “Both aspects should therefore be addressed together in treatment.”
“With the current study, a robust evidence base for this rare disease is now available for the first time,” summarises Professor Wick. “This represents an important step toward precision medicine even in rare diseases. Relevant research in rare tumour entities can often only be carried out in large international consortia. International scientific collaboration therefore deserves particular attention.”
Brain showing areas related to ADHD. Credit: Scientific Animations CC4.0
A breakthrough study led by Monash University researchers has shed light on the factors shaping the intricate wiring of our brains. The research, published in the world-leading journal Cell, reveals that the brain’s complex wiring diagram, known as the cortical connectome, does not form at random. Instead, a new mathematical model shows that connections preferentially form between locations that support natural, shape-driven “resonant patterns”.
Lead author Francis Normand, from the Turner Institute for Brain and Mental Health at Monash University, likens the brain to a musical instrument, such as a bell or a drum.
“Just as the physical shape of a bell or a drum determines its vibrations and the music that it produces, the physical geometry of the brain constrains the patterns of neural activity it can support,” he said.
Mr Normand conducted the research, alongside Professor Alex Fornito and Dr James Pang, both from the Turner Institute for Brain and Mental Health at Monash University. By testing their mathematical formula against publicly available datasets, the research team showed that this geometric rule holds true across various species, from mice through to humans. This demonstrates that the physical shape of the brain has served as a blueprint in guiding its internal wiring for at least 90 million years of mammalian evolution.
Significantly, the researchers showed that the formula successfully predicts both how the brain is wired: its “topology”; and where the wires physically go: its “topography”, which are important properties that previous theories have failed to predict.
Mr Normand said that while the general idea of physical space constraining the brain has long been recognised, this study is the first to formalise and mathematically quantify the rule using a framework called neural field theory.
“Traditional models treat the brain as a collection of distinct regions sending signals through their connections. Our model suggests that the cortex can be treated like a continuous physical medium through which waves of activity propagate,” Mr Normand said.
“The model assumes that connections are strengthened between locations that show coordinated activity fluctuations when the brain expresses certain resonant patterns that it prefers due to its shape, much like the ripples formed by a raindrop will be influenced by the shape of a pond.
“Crucially, our model suggests the brain wires itself in an energy-efficient way to support these resonant patterns, strongly favouring low-frequency patterns, resembling a deep, low hum rather than a high-pitched chirp. These broad, brain-wide patterns require far less energy to sustain,” he said.
The research opens new doors for brain modelling in the future and could help understand how structural changes or malformations alter the brain’s wiring in psychiatric or neurological disorders.
“The fact that a single mathematical formula can accurately predict brain networks in both a tiny mouse and a human reveals just how powerful physical geometry is in shaping brain connectivity,” Mr Normand said.
Mayo Clinic researchers and collaborators have shown that an artificial intelligence (AI) tool can analyse routine pathology slides to help clinicians classify meningiomas, the most common primary brain tumour in adults, and better understand a patient’s risk of tumour recurrence.
The study, published in The Lancet Digital Health, demonstrates that deep learning models can support the extraction of molecular and prognostic information from standard haematoxylin and eosin, or H&E, slides – the same type of tissue images already used in routine clinical care. These insights are typically obtained through DNA methylation profiling, an advanced genetic test which provides valuable diagnostic and prognostic information but can be costly, time-consuming and is unavailable in many hospitals.
“This is one of the many studies where we can harness the strength of digital pathology by capturing the last two decades of genomic and molecular knowledge into AI algorithms,” says Gelareh Zadeh, MD, PhD, chair of the Department of Neurologic Surgery at Mayo Clinic in Rochester and Chief Medical Officer for Mayo Clinic Platform.
Making advanced tumor insights more accessible
Meningiomas can vary widely in behaviour. Some grow slowly and may never return after treatment, while others are more aggressive and more likely to recur. Understanding that risk is critical for patients and care teams deciding whether additional treatment, such as radiation therapy, may be needed after surgery.
Molecular testing can help identify which tumours are more likely to recur and which may respond differently to treatment. But these tests require specialized technology and expertise, limiting access for many patients.
Using tissue samples, pathology images and clinical data from 672 patients, researchers developed and tested AI models designed to help identify patterns linked to a tumour’s biology. Drawing on multiple de-identified datasets, including data resources from Mayo Clinic Platform, the models supported classification of meningioma subtypes and recurrence risk prediction using standard pathology slides that are already part of routine patient care.
The findings suggest that, with further validation, AI-based tools could one day help clinicians obtain more detailed tumour information to inform patient care, without requiring every patient to undergo advanced genetic testing.
Helping guide treatment decisions
For patients with meningiomas, recurrence risk can influence follow-up care, imaging frequency and whether radiation therapy should be considered. The study found that AI-based predictions remained useful even after accounting for traditional clinical factors such as tumour grade, the extent to which surgery was able to remove the tumour and patient age.
Researchers also found that the AI models could identify patterns of tumour heterogeneity – differences within the same tumour – that may help explain why some tumours behave more aggressively or respond differently to treatment.
The researchers note that additional prospective studies are needed before the AI models can be used routinely in clinical care. Still, they say the findings lay the groundwork for more accessible, personalised care for patients with meningiomas – and potentially for similar AI approaches in other cancers.
As with any clinical decision-support tool, the researchers emphasise that these models would require rigorous evaluation, validation and ongoing physician oversight before being considered for routine care. “The aim is to make these algorithms readily and simply accessible for use globally, improving patient care across many healthcare settings,” says Dr Zadeh.
For a complete list of authors, disclosures and funding, review the publication.