Supermarket Receipts Show Trends in Menstrual Pain Relief
An analysis of 211 million supermarket transactions found that more than a quarter of customers buying menstrual products bought pain relief at the same time.
More than a quarter of women buying menstrual products also purchase pain relief at the same time – and those in lower-income areas are significantly less likely to do so – according to a new study published this week in the open-access journal PLOS Digital Health by Dr. Victoria Sivill of the University of Bristol, UK, and colleagues, which used supermarket loyalty card data to map menstrual pain disparities across England.
Menstrual pain is a common concern affecting many individuals globally. Existing research highlights its negative impact on daily activities, including school and work attendance.
In the new study, researchers analysed anonymised loyalty card data from a major UK health and beauty retailer, encompassing 211 million transactions by 3.4 million individuals between 2006 and 2015. They analysed how often shoppers purchased menstrual products at the same time as pain relief, and how that compared to a customer’s baseline rate of buying pain relief.
The analysis found that 26.7% of customers who purchased menstrual products also bought pain relief in the same transaction. These customers were nearly four times more likely to buy pain relief while buying menstrual products compared to other shopping trips. As a validation of the approach, the most common interval between consecutive menstrual purchases across the dataset was exactly 28 days – consistent with the average menstrual cycle.
Regional income emerged as the strongest predictor of menstrual pain purchases: customers in the lowest-income areas were 32% less likely to purchase pain relief at the same time as menstrual products compared to those in the highest-income areas. The authors note that lower rates of pain relief purchases in deprived areas likely reflect an inability to afford over-the-counter medication rather than lower rates of menstrual pain itself
“The study highlights the need for greater awareness and policy interventions to address the high prevalence of menstrual pain as well as socioeconomic dimensions of menstrual pain,” the authors say. “Public health initiatives should incorporate menstrual pain relief as part of broader efforts to improve health equity.”
Co-author Dr James Goulding notes: “It is wonderful that smart data research in the UK is able to bring issues which may have once been overlooked in scientific settings – such as the sheer scale and impact of menstrual pain – to light. This is well overdue.”
Co-author Dr Anya Skatova adds: “Like many women, I was aware of how common menstrual pain is, but the scale of painkiller purchases alongside menstrual products was still striking. Using shopping data, we can see just how widespread the need for pain relief really is. This kind of evidence helps make menstrual pain visible at a population level and provides a strong foundation for systemic change in how it is recognised, treated, and prioritised in public health.”
Provided by PLOS
Press Preview: https://plos.io/42wSl1W
In your coverage please use this URL to provide access to the freely available article in PLOS Digital Health: https://plos.io/4wzrwbh
Contact: Anya Skatova, anya.skatova@bristol.ac.uk; James Goulding, james.goulding@nottingham.ac.uk
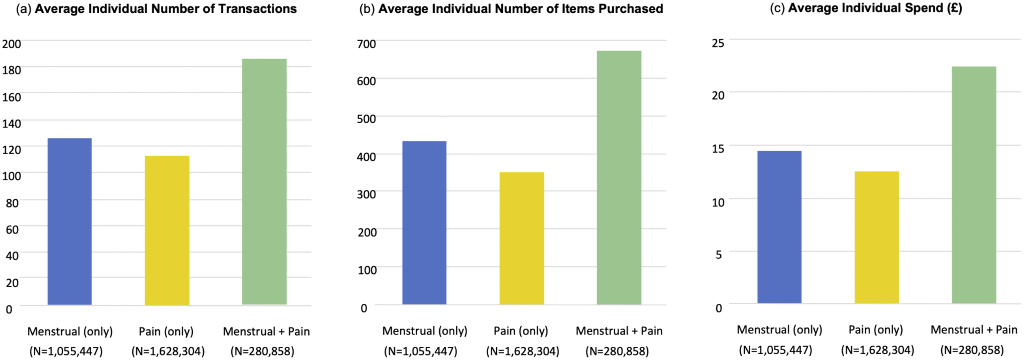
Image Caption: Fig 1. Average (mean) individual summary statistics for Menstrual, Pain and Menstrual Pain customer sets via analysis of transactional logs between 30th April 2006 to 16th April 2015.
Image Credit: Sivill et al, PLOS Digital Health, 2026
High-Resolution Image Link: https://plos.io/4ujYPxl
Citation: Sivill V, Ljevar V, Goulding J, Skatova A (2026) What can shopping transactional data reveal about relative prevalence of menstrual pain and period poverty in England? PLOS Digit Health 5(5): e0001308. https://doi.org/10.1371/journal.pdig.0001308