Endocrine Society guideline addresses different subgroups of central precocious puberty
Photo by Ben Wicks on Unsplash
Some subgroups of children with precocious puberty – such as older girls with slowly progressing puberty – may not need the same level of testing or treatment, according to a new Endocrine Society Clinical Practice Guideline.
“Children who start puberty earlier than usual should be carefully evaluated so they receive the right care at the right time – without unnecessary tests or treatment,” said the guideline’s writing group chair, Ana Claudia Latronico, MD, PhD, of the University of São Paulo. “The Endocrine Society’s guideline gives clinicians evidence-based suggestions to identify central precocious puberty, understand its causes and decide when and what treatment is appropriate.”
Central precocious puberty happens when a child’s brain activates puberty-related hormones too early – before age 8 years in girls and before age 9 years in boys. This early hormone signalling triggers physical changes such as breast development in girls, testicular enlargement in boys, rapid growth, and, in some cases, early menstruation.
Early puberty can affect a child’s adult height and is associated with long-term physical and emotional health risks, including psychosocial stress, heart disease, and some cancers later in life.
According to the guideline authors, puberty-pausing medication, which temporarily pauses the brain signals that start puberty, can be an effective treatment and has the potential to increase adult height as well as improve psychosocial and long-term health outcomes among children with early puberty.
“Some subgroups of children may not need the same level of testing or treatment. For example, older girls with slowly progressing precocious puberty often have normal adult height without intervention,” said the guideline’s writing group co-chair Stephanie Roberts, MD, of Boston Children’s Hospital in Boston, Mass. “We give clinicians suggestions that avoid unnecessary or invasive testing and treatment, such as sometimes initially using a period of observation by their health care provider, using simpler testing methods and individualising treatment when indicated.”
Suggestions from the guideline include:
Monitoring girls with early breast development with physical exams every 4-6 months before initiating diagnostic testing
Observing girls under 7 years old for 4-6 months to distinguish slowly vs. rapidly progressing puberty, since slow progression often results in normal adult height without treatment.
Using simple first-line testing with a basal luteinising hormone (LH) blood test rather than GnRH agonist stimulation testing.
Avoiding routine brain MRIs in older children (> 6 years in girls and > 7 years in boys) without neurological symptoms.
Not routinely doing genetic testing, especially for cases without a family history of early puberty.
Starting treatment with longer-acting puberty-delaying medications (rather than shorter-acting medications) whenever it is expected that longer-acting medications will be used for long-term therapy.
Not routinely using growth hormone therapy.
Not routinely doing frequent lab monitoring during treatment unless treatment failure is suspected.
Discontinuing therapy by early adolescence (about 10-11 years in girls, 11-12 years in boys).
Blood protein levels change markedly already during childhood and adolescence, and differences between girls and boys become increasingly pronounced with age. This is shown by a new study in Nature Communications from Karolinska Institutet in collaboration with colleagues from SciLifeLab and KTH Royal Institute of Technology. The results suggest that blood protein levels change over the course of a lifetime, rendering adult reference values inadequate for children and adolescents.
In the study, the researchers analysed blood samples from 100 participants in the population-based BAMSE cohort at ages 4, 8, 16 and 24 years. Using advanced protein technology, over 5000 proteins were measured, of which just over 3500 could be tracked over time. More than half of these proteins changed with age even during childhood.
The greatest changes were observed between the ages of 8 and 16, a period that coincides with puberty. Many proteins increased sharply during this time, only to decrease again in early adulthood, whilst others showed more gradual increases or decreases from childhood to adulthood.
”Our study shows that reference values from adults cannot be used when interpreting protein levels in children and adolescents. Protein levels are strongly age-dependent even early in life, says one of the lead authors”, Sophia Björkander, assistant professor and docent at the Department of Clinical Science and Education, Södersjukhuset, Karolinska Institutet.
The researchers also identified clear gender differences. In early childhood, the differences were few, but from adolescence onwards they increased markedly. By the age of 24, around 30 per cent of proteins differed between women and men, including those linked to growth, metabolism, the immune system and reproductive processes.
”Gender differences become very clear from adolescence and early adulthood. This shows that both age and gender are fundamental biological factors that must be taken into account when proteins are used as biomarkers”, says Sophia Björkander.
Blood proteins are used as biomarkers
Today, blood proteins are widely used as biomarkers to detect, for example, inflammation, hormonal imbalance, cardiovascular disease and metabolic disorders. An important finding from the study is that different levels of proteins in children may reflect normal development rather than disease.
”By mapping protein development, we are creating a reference that can be used to identify early deviations. This opens up possibilities for risk assessment of chronic diseases and more personalised medicine”, says senior/last author Erik Melén, project leader at BAMSE and professor at the Department of Clinical Science and Education, Södersjukhuset, Karolinska Institutet.
The researchers point out that the number of participants is limited and that the results primarily apply to a relatively homogeneous population.
The study is part of the Human Disease Blood Atlas, which is a resource within the Human Protein Atlas and is based on the Swedish BAMSE cohort. The BAMSE project is jointly run by the Department of Clinical Science and Education, Södersjukhuset and the Institute of Environmental Medicine, both at Karolinska Institutet, as well as the Centre for Occupational and Environmental Medicine, Region Stockholm.
The research has been funded by, among others, the Swedish Research Council, Region Stockholm, the Swedish Heart-Lung Foundation and the Knut and Alice Wallenberg Foundation. The researchers state that there are no conflicts of interest.
Fluoride is a naturally occurring mineral that has been shown to strengthen teeth and reduce cavities. Many municipalities add fluoride to their drinking water – called community water fluoridation – as a public health measure to support dental health. In recent years, however, some have claimed that ingesting fluoride can harm children’s IQ.
Researchers at the University of Minnesota led a team that investigated the connection between fluoride in drinking water and children’s IQ to see if these claims had merit. The study, published in PNAS, examined Wisconsin state testing records, archival information about when Wisconsin cities began to fluoridate their water, and data from the Wisconsin Longitudinal Study, which has followed a random sample of 10,317 high school seniors from 1957 through 2026. Key findings include:
There is no evidence supporting a connection between community water fluoridation and children’s IQ.
There is also no evidence supporting a connection between community water fluoridation and cognitive functioning at various points later in life.
Findings confirm evidence published in previous research which also used a national sample, but considered school achievement test scores instead of actual IQ scores.
“Utah, Florida and many municipalities have chosen to remove fluoride from drinking water based on flawed studies that considered the IQ effects of exposure to massive doses of fluoride,” said lead researcher John Robert Warren, a professor in the College of Liberal Arts. “Because levels of fluoride added to municipal drinking water in the U.S. are so much lower, almost all prior evidence from those international studies is not relevant to U.S. public policy debates.”
Future research will continue examining the benefits and harms of adding fluoride to community drinking water.
Study co-author Gina Rumore, co-director of the Demography and Economics of Aging Coordinating Center at the University of Minnesota, noted that these findings “provide no support for the claim that community water fluoridation has any harmful effect on children’s IQ or on adult cognition.”
Strong evidence ties early language difficulties to later adjustment challenges. Can environmental factors make these problems worse? In a new study, FAU researchers, in collaboration with Aarhus University in Denmark, find that unsupervised or “solo” screen time worsens the behavioural and emotional challenges confronting young children with limited language skills. A total of 546 4- to 5-year-old children from 24 childcare centres in Denmark were followed for six months. Investigators assessed their language abilities, behavioural adjustment and the amount of time the children spent watching screens alone.
The study findings, published in the journal Research on Child and Adolescent Psychopathology, found that solitary screen time acts as an amplifier, exacerbating conduct problems in children with poor communication skills and low productive vocabulary. The results highlight the critical role of the home learning environment in early childhood development. For children who struggle with language skills, time spent alone with a screen is time not spent mitigating risks through healthy social engagement with parents or friends.
Early problems with language can have a lasting negative impact on social and emotional development. Building on this foundation, a new groundbreaking study from Florida Atlantic University and Aarhus University in Denmark tests the hypothesis that unsupervised, solitary screen time during early childhood increases the likelihood that language difficulties will lead to socioemotional difficulties.
The study, published in Research on Child and Adolescent Psychopathology , found that pathways from poor communication skills and low productive vocabulary to later adjustment problems were particularly strong among preschool- and kindergarten-aged children who averaged at least 10 to 30 minutes of solitary screen time per day across the course of a week.
Study participants were 546 4- and 5-year-olds (264 girls, 282 boys) attending 24 population-based childcare centers across 13 municipalities in Denmark. Teachers completed assessments twice of child adjustment difficulties, such as conduct and emotional problems, over the course of about six months during a single school year. At the outset, teachers administered standardized tests of child language abilities, including communication skills and productive vocabulary. Parents reported on solitary screen time, which was defined as the average number of hours per week that children spent alone viewing handheld devices or television, excluding screen time supervised by or consumed with an adult.
Consistent with several previous studies, there were longitudinal associations from oral language problems to later adjustment difficulties. Across the six-month period, poor communication skills and high levels of solitary screen time separately predicted escalating emotional difficulties.
Unique to this study was the finding that solo screen time magnified problems arising from language difficulties. Associations from low productive vocabulary and poor communication skills to increases in conduct problems were strongest among children whose parents reported that their children were well above average in solitary screen time exposure.
“Unsupervised screen time forecloses opportunities for social engagement that might mitigate the behavioral risks that follow from language problems,” said Brett Laursen, Ph.D., senior author and a professor of psychology in FAU’s Charles E. Schmidt College of Science.
Laursen uses an economics model to explain the results. Economists define opportunity costs as losses attached to a choice. If an adult stays up late with a book, the opportunity cost of reading is a good night’s sleep.
“The opportunity costs of solitary screen time can be particularly steep for vulnerable youth. Children have a finite number of free time hours in a day,” said Laursen. “Every hour a child spends alone with a device is an hour they aren’t engaged in social interactions that boost language skills. It is an hour not spent practicing the social and emotional skills required to build friendships. Screens don’t demand compromise, sharing or dialogue – the exact skills that children with communication difficulties need to practice.”
Young children learn language from in-person interactions – very little is acquired from video screens. Further, electronic media cannot replace the rich social experiences children gain from play and engagement with peers.
“Young children with limited language skills are already at risk for social and emotional challenges,” said Molly Selover, lead author and an FAU doctoral student in psychology. “There is little reason to expect that screens help children overcome the adaptive challenges posed by oral language problems and many reasons to suspect that they make matters worse.”
Excessive screen use by young children is widespread: the World Health Organization recommends no more than one hour per day for children ages 2 to 5, yet a global review found that two-thirds of households exceed this limit. In the United States, about half of young children spend more than two hours a day on screens during the week, with even higher use on weekends. Of course, both content and supervision matter.
For children ages 2 to 5, the American Psychological Association encourages parents to limit screen time to no more than one hour per day and to co-view and interact with their children during this time rather than using the screen as a babysitter. They also note that the quality of the content on screens is extremely important, perhaps more important than the total amount of time spent viewing.
The authors say that high caliber content has documented benefits for children, especially as children get older. Unfortunately, when left to their own devices, many young children prefer fast-paced, brief and highly stimulating content, some of which may be age-inappropriate.
“Electronic media is as an integral component of the home learning environment; many children spend more time with tablets and phones than with toys, books and friends,” said Selover. “Like other home environment risks, solitary screen time poses a unique peril to young children with heightened vulnerabilities. Adults tend to think of screens as pleasant distractions and may use them as convenient babysitters. But for preschool children with language vulnerabilities, unsupervised screen time is not benign – it can be an active barrier to well-being.”
The authors acknowledge that their findings may not be popular. Screens are a ubiquitous part of everyday life. Nevertheless, they encourage parents to carefully scrutinize how young children engage screens.
“The findings matter because they show that an all-too-common environmental risk – elevated solitary screen time – can worsen behavioural and conduct challenges for children who face an already difficult developmental path,” Selover said.
Trial provides new evidence to guide early treatment decisions for families and clinicians
An infant participating in the Baby CHAMP study raises both hands while seated in a stroller. The NIH-funded trial led by the Fralin Biomedical Research Institute at VTC examines early therapies designed to improve arm and hand function in young children with cerebral palsy affecting one side of the body. Credit: Jennifer Murray
Infants and toddlers with unilateral cerebral palsy, which affects the brain’s control of muscles on one side of the body, show lasting improvements in hand and arm function when they receive early, high-dose therapy, according to a new multisite clinical trial led by Virginia Tech researchers at the Fralin Biomedical Research Institute at VTC.
The Baby CHAMP (Children with Hemiparesis Arm-and-Hand Movement Project) study directly compared three therapist-delivered interventions: two forms of constraint-induced movement therapy, which limit the stronger arm to encourage use of the weaker one when combined with therapy, and bimanual therapy, which promotes coordinated use of both hands.
The researchers found that children ages 6 to 24 months showed similar gains whether therapy involved full-time casting, a splint worn during sessions, or bimanual training without constraining the stronger arm.
Published in Pediatrics Open Science, the study addresses a long-standing gap in clinical evidence.
“The brain in the first two years of life is remarkably plastic,” said Stephanie DeLuca, associate professor at the Fralin Biomedical Research Institute at VTC and co-principal investigator of the trial. “By delivering high-dose, play-based therapy early, we’re capitalizing on a window of opportunity when the nervous system is especially responsive to experience.”
While both constraint-induced movement therapy and bimanual therapy are widely recommended for children older than 2 years with unilateral cerebral palsy, limited data have been available to guide treatment decisions for infants and toddlers.
“This gives families and clinicians evidence-based options,” said Sharon Landesman Ramey, a Virginia Tech Distinguished Scholar, professor at the Fralin Biomedical Research Institute at VTC, and co-principal investigator of the Baby CHAMP trial. “The encouraging message is that early, intensive therapy works — and multiple approaches can help children build critical motor skills. Caregivers and families now have actionable evidence that can shape care during one of the most important periods of brain development.”
Unilateral cerebral palsy affects movement on one side of the body and can result in lifelong impairment of upper extremity function. Early intervention is considered critical because the brain is especially adaptable during the first two years of life.
DeLuca is director of the Fralin Biomedical Research Institute at VTC Neuromotor Research Clinic, which investigates novel treatments for children with a range of biomedical conditions and provides worldwide training for therapists to become certified in new evidence-based therapies.
All children received three hours of therapy per day, five days a week, for four consecutive weeks, totaling 60 hours of structured intervention. Parents also supported additional guided home practice.
Fifty-eight children were enrolled in the randomized controlled trial, funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health. Fifty-three completed treatment and end-of-therapy assessments, and 41 returned for evaluation six months later.
Across all three groups, children demonstrated significant improvements in the ability to use both hands, individually and together. Improvements were measured using standardized developmental assessments administered by evaluators who were unaware of each child’s treatment assignment.
Children also showed gains in fine motor skills in their less-affected arm. Improvements were most pronounced at the six-month follow-up, suggesting that benefits continued to build after formal therapy ended.
Researchers had hypothesized that bimanual therapy might lead to greater improvements in two-handed skills and that full-time casting might yield stronger gains in the affected arm. The data did not support those predictions. Instead, outcomes were broadly comparable across approaches.
The study also addressed concerns that constraining the stronger arm could impair its development. No evidence of harm was observed. In fact, children in the full-time cast group showed slightly greater gains in fine motor skills in their non-affected arm at six months compared with the bimanual group.
“This is important to the field because many people have worried that the use of a constraint might slow the developmental process of the less-affected arm,” DeLuca said. “Our findings confirm that this did not occur and this therapy may even help promote improvements in skills on the less-affected arm and hand.”
Some parents reported their child showed short-term frustration wearing a cast or splint, and minor skin irritation occurred in a small number of children using casts, but no were caused by the therapy itself.
The trial was conducted in collaboration with researchers at Virginia Tech, The Ohio State University, and Nationwide Children’s Hospital. Therapists were centrally trained to deliver structured, play-based interventions grounded in motor learning principles, including repetition, reinforcement, and progressively challenging activities.
Longer-term studies will be needed to better understand how early therapy influences development across many dimensions of a child’s life.
Even when controlling for age and family background, COVID’s impact was evident
Photo by Kelly Sikkema on Unsplash
The COVID pandemic disrupted children’s ability to self-regulate, according to research from three UK universities just published in the journal Child Development.
The study by Lancaster University, East Anglia and Durham reveals that the pandemic hampered children’s ability to regulate their behaviour, stay focused and adapt to new situations – skills known collectively as executive functions.
The greatest impact was seen among pupils who were in reception when the first lockdowns began – a crucial stage at four or five when youngsters normally learn to socialise, follow routines and navigate the busy world of the classroom. Primary school in the UK then begins at Grade 1, starting at age five or six.
These children showed less growth in their self-regulatory and cognitive flexibility scores over time compared to a second group of children who were in preschool when the pandemic started.
The research team say these children may still be feeling the effects years later.
How the research happened
Scientists were already running a long-term study tracking youngsters from toddlerhood to early school years when the COVID pandemic hit.
They followed 139 children aged between two-and-a-half and six-and-a-half years old over several years, including 94 families who joined the study before Covid struck.
This meant that they had a rare baseline of children’s abilities before the pandemic began, which allowed them to track exactly how development changed during and after the lockdowns.
Using a standardised assessment called the Minnesota Executive Function Scale, they were able to measure the same cognitive skills at regular intervals.
Dr Eleanor Johns from Lancaster University’s Department of Psychology said: “We began this study to understand how children’s executive function develops across early childhood, and we saw clear, steady growth between 2.5 and 6.5 years of age. However, because our longitudinal study spanned the COVID-19 pandemic, we also had a unique opportunity to examine how this unprecedented disruption affected the children we were already following.
“We found that children who had just started school when the first lockdown began showed a slower rate of growth in executive function compared to those who were preschool age. Starting school is a major developmental transition, as children learn new routines, adapt to classroom rules, and develop self-regulation alongside their peers. When schools closed almost overnight, those opportunities were suddenly removed.”
The research revealed that:
Individual differences in executive function abilities were remarkably stable. Children who had stronger skills at two-and-a-half years old tended to remain ahead at six-and-a-half years.
Children from lower socio-economic households consistently scored lower, echoing long-standing research on the impact of maternal education and home environment.
Even when controlling for age and family background, COVID’s impact was evident. Children who were in reception at the start of the pandemic made more modest improvements in executive function compared to those still in preschool.
Dr Johns said: “Our findings suggest that the structured school environment and regular interaction with peers play a crucial role in supporting the development of executive function. When those experiences were disrupted, children’s executive function developed more slowly than that of younger children who were still in preschool.”
The researchers say their work highlights a generation of children who may need more support from teachers, schools and health services in coming years.
Vegetarian and vegan diets can support healthy growth when carefully planned with appropriate supplementation, finds a major new meta-analysis – the most comprehensive study to-date of plant-based diets in children.
A team of researchers, from Italy, USA and Australia, analysed data from over 48 000 children and adolescents worldwide who followed different dietary patterns, examining health outcomes, growth and nutritional adequacy. They found that vegan and vegetarian diets can be nutrient-rich and support healthy growth, but also carry a risk of deficiencies if key nutrients are not obtained through fortified foods or supplements.
The peer-reviewed study, published in Critical Reviews in Food Science and Nutrition, also suggests that plant-based diets may offer additional health benefits for children – including improved cardiovascular risk profiles – compared with omnivorous diets that include meat, fish and other animal-derived foods.
This large meta-analysis is the most comprehensive study to date of plant-based diets in children under 18 years of age, examining data from 59 studies across 18 countries. It compared lacto-ovo-vegetarian (which include dairy products and eggs, but exclude meat, fish and poultry) and vegan diets (which exclude all animal-derived foods) with omnivorous diets across a wide range of nutritional and health outcomes in 7280 lacto-ovo-vegetarians, 1289 vegans and 40 059 omnivores.
The study found that vegetarian children consumed more fibre, iron, folate, vitamin C and magnesium than omnivores, but they had lower intakes of energy, protein, fat, vitamin B12 and zinc. While evidence on vegan diets was more limited, similar patterns emerged.
“Notably, vitamin B12 didn’t reach adequate levels without supplementation or fortified foods, and calcium, iodine and zinc intakes were often at the lower end of recommended ranges, making them important nutrients to consider for children on plant-based diets,” explains the study co-author Dr Jeannette Beasley, an Associate Professor in the Departments of Nutrition and Food Studies and Medicine at New York University.
“Vegan children, in particular, had especially low calcium intake.”
Health benefits
Despite these risks, both vegan and vegetarian children displayed more favourable cardiovascular health profiles than omnivores, with lower total and low-density lipoprotein (LDL) cholesterol – the “unhealthy” form of cholesterol.
Growth and body composition measures indicated that children on plant-based diets tended to be leaner than omnivores: vegetarian children were slightly shorter and lighter, with lower body mass index (BMI), fat mass and bone mineral content. Vegan children also had shorter stature and lower BMI scores.
“Our analysis of current evidence suggests that well-planned and appropriately supplemented vegetarian and vegan diets can meet nutritional requirements and support healthy growth in children,” states lead-author Dr Monica Dinu, who focuses on exploring how nutrition shapes health and well-being at the Department of Experimental and Clinical Medicine, at the University of Florence, in Italy.
Parents: take an informed approach
Plant based diets remain entirely achievable for children and can offer environmental advantages as well as health benefits. The authors stress that families should not be discouraged from choosing vegetarian or vegan diets for ethical, environmental or health reasons. Instead, they recommend that parents approach these diets with informed planning and, where possible, seek support from clinicians such as dietitians and paediatric health professionals. With attention to a few key nutrients, these diets can fully meet children’s needs during periods of rapid growth while reducing nutritional risks.
“We hope these findings offer clearer guidance on both the benefits and potential risks of plant-based diets, helping the growing number of parents choosing these diets for health, ethical or environmental reasons,” Dr Dinu adds.
More research needed, but balance is key
The authors also emphasise the need for clear, evidence-based guidance to support families with planning healthy plant-based diets for children, who may have higher nutritional needs during periods of rapid growth and development.
However, the researchers caution that these results are limited by the cross-sectional design of most included studies, variability in methods and populations, and challenges in accurately assessing children’s dietary intake.
“In conclusion,” says fellow co-author Dr Wolfgang Marx, from the Food & Mood Centre, at Deakin University, Australia, “while well-planned vegetarian and vegan diets are nutritionally adequate and beneficial for adults, there is far less clarity about their suitability for children – leading to inconsistent or even conflicting advice for parents.
“Our findings suggest that a balanced approach is essential, with families paying close attention to certain nutrients – particularly vitamin B12, calcium, iodine, iron and zinc – to ensure their children get everything they need to thrive.”
A study conducted by University of Louvain (UCLouvain), published in Nature Communications, shows that part of the brain of babies born blind is permanently altered, while another part remains surprisingly intact. Babies’ brains are much more adaptable than previously thought: even if they cannot see at the very beginning of life, they can later learn to recognise the world around them.
Some babies are born with early blindness due to dense bilateral congenital cataracts, requiring surgery to restore their sight. This period of several months without vision can leave a lasting mark on how the brain processes visual details, but surprisingly little on the recognition of faces, objects, or words.
Using brain imaging, the researchers compared adults who had undergone surgery for congenital cataracts as babies with people born with normal vision. The results are striking: in people born with cataracts, the area of the brain that analyses small visual details (contours, contrasts, etc.) retains a lasting alteration from this early blindness. On the other hand, the more advanced regions of the visual brain, responsible for recognising faces, objects, and words, function almost normally. These “biological” results have been validated by computer models involving artificial neural networks. This distinction between altered and preserved areas of the brain paves the way for new treatments. In the future, clinicians may be able to offer visual therapies that are better tailored to each patient.
“Babies’ brains are much more adaptable than we thought,” explains Olivier Collignon, Professor at University of Louvain (UCLouvain). “Even if vision is lacking at the very beginning of life, the brain can adapt and learn to recognise the world around it even on the basis of degraded information.”
These findings also challenge the idea of a single “critical period” for visual development. Some areas of the brain are more vulnerable to early vision loss, while others retain a surprising capacity for recovery. “The brain is both fragile and resilient,” adds Olivier Collignon. “Early experiences matter, but they don’t determine everything.”
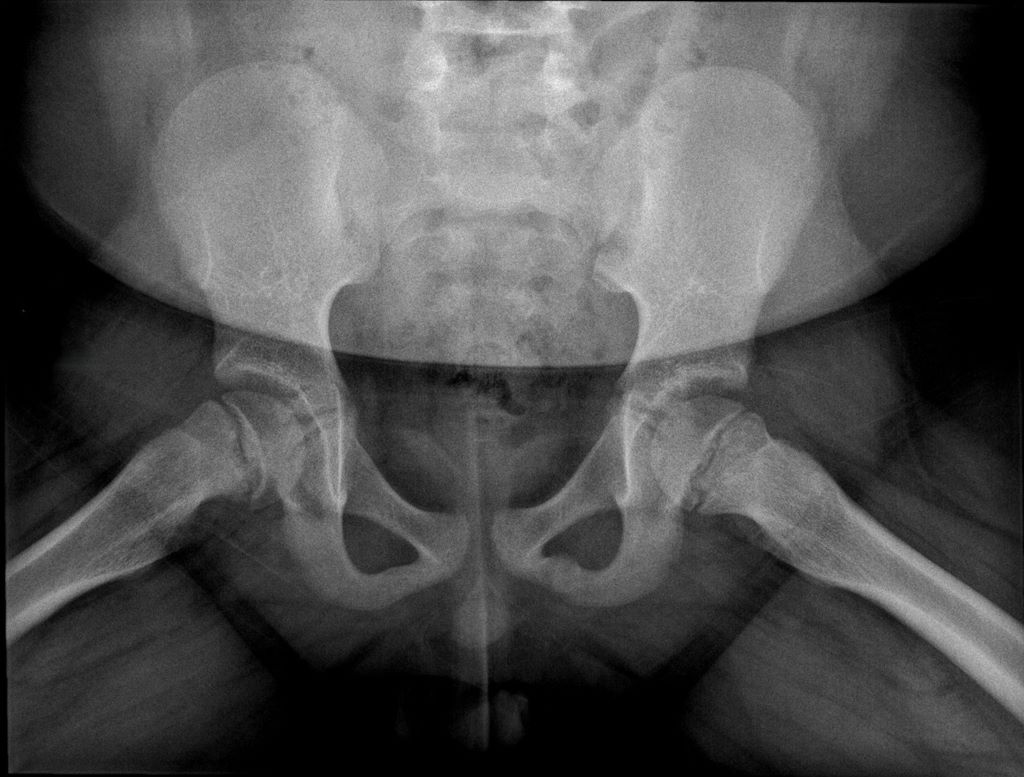
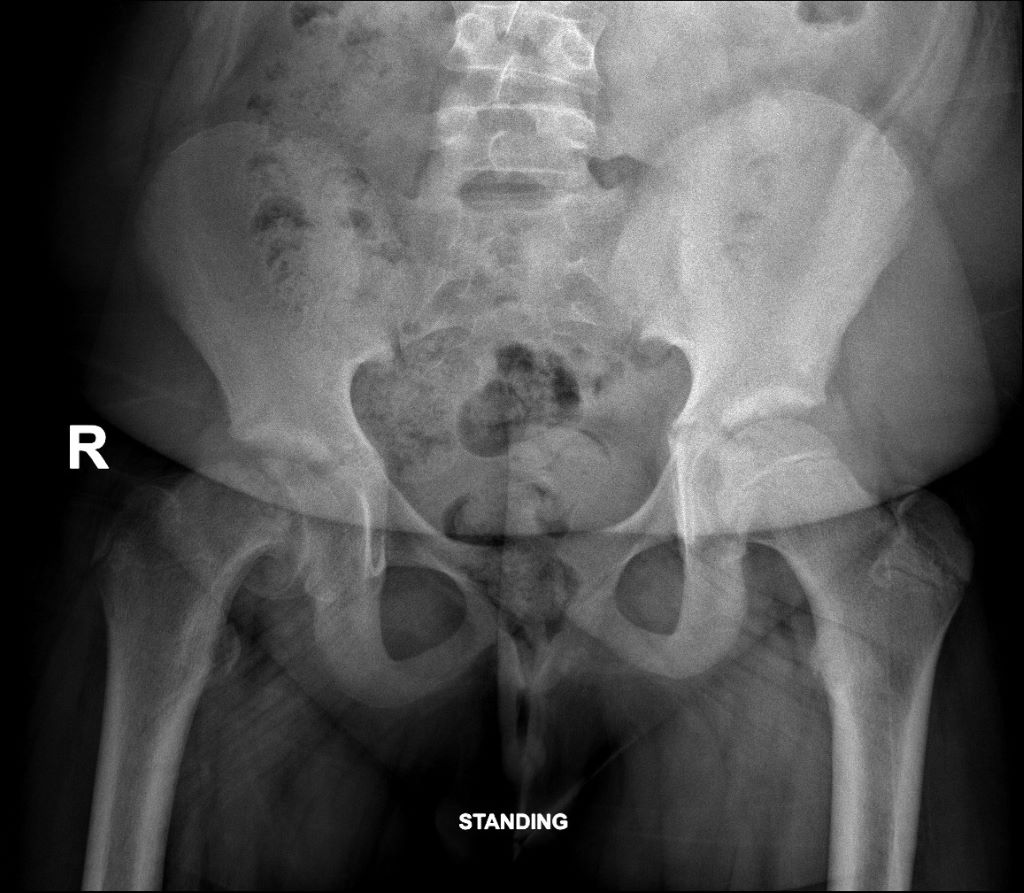
Frog leg lateral view of the hips. Widening of the growth plate (physis) with blurring and irregularity of the femoral neck (metaphysis). Inferior offset of the head in relation to the neck (early slip).
Slipped Capital Femoral Epiphysis (SCFE) is the most common adolescent hip disorder. It occurs when the ball at the top of the thigh bone (femoral head) slips off the neck of the bone through the growth plate (physis). A bit like an ice cream sliding off a cone… Dr Ryno du Plessis, a renowned orthopaedic and joint replacement surgeon in the Western Cape, talks about what it is and why it is often misdiagnosed.
SCFE usually happens during growth spurts in children aged 9 to 16 years and is more common in boys and in children with obesity, endocrine disorders, or other risk factors.
Why is this problem often missed?
AP view of the hips. ‘Melting ice cream sign’: Femoral head (epiphysis) slipping off the femoral neck (metaphysis) though the growth plate (physis) like an ice cream melting from the cone.
Despite its frequency, SCFE is routinely misdiagnosed or diagnosed late – unfortunately, sometimes months after symptoms start. Studies show that over 50% of SCFE cases are not diagnosed at the first medical visit.
Here’s why:
Pain felt in the knee or thigh: Physicians often focus on the wrong joint and the hip is never X-rayed
Labeled as a groin strain: Adolescents in sports may be diagnosed with muscle strains or ‘growing pains’
Symptoms develop gradually: Children may limp without severe pain, leading to delayed concern
Physiotherapy prescribed early: Instead of imaging – patients are referred to physio – delaying diagnosis
Lack of hip-specific X-rays: It requires a frog-leg lateral X-ray.
Why does delay matter?
The longer the slip is left untreated, the more serious the outcome. Every week or month of delay increases the severity of the deformity, often silently.
Late diagnosis risks:
More severe deformity
Loss of bloody supply to the femoral head. This is known as avascular necrosis and can lead to pain, limited movement and eventually, hip collapse and osteoarthritis
Early-onset hip arthritis
Complex surgery
Children diagnosed early often need just one screw to stabilise the hip. Those who are diagnosed late may face major reconstructive surgery, longer recovery, and reduced hip function for life.
Red flags for parents, teachers and coaches
If you notice any of the following signs in a child or teen – especially those who are overweight – take it seriously and ask for a hip X-ray:
Limping for more than a week
Complaints of pain in the knee, thigh, groin, or buttock
Walking with the foot turned outwards
Stiffness or loss of motion in the hip
Sudden inability to walk or stand after a minor stumble (may indicate an unstable SCFE)
Radiology – diagnostic challenges
Dr Jaco Greyling, a radiologist from SCP Radiology, says SCFE diagnoses can be delayed due to several factors, including
Hip X-rays not ordered by the initial healthcare provider (eg, GP or physiotherapist)
Only a single anterior-posterior pelvis projection is performed, whereas a frog-leg lateral view must also be specifically requested by the referring physician. Radiologists should ensure the child returns for this view if it was not initially ordered
Findings in the pre-slip phase are subtle and may be missed, even by experienced radiologists
He says, ’the recommended imaging is an anterior-posterior pelvic view which shows malalignment and widening of the growth plate and a frog-leg lateral view, the most sensitive for detecting early or subtle slips.’
‘Key radiological signs,’ says Dr Greyling are:
Widening of the growth plate
Loss of height of the femoral head
Loss of alignment of the anatomical lines that intersect with the femoral head
‘Melting ice cream sign’ slipping off the femoral neck at the growth plate (epiphysis).
Follow-up recommendations:
Dr Greyling suggests repeat imaging within two weeks if symptoms persist, and an early referral to a paediatric orthopaedic surgeon and an MRI for patients with risk factors and ongoing pain.
Early SCFE is usually treated with in-situ fixation using one or two screws. The goal is to stabilise the rounded end of a long bone to prevent further slippage.
In cases where both hips are at risk (especially in young or overweight patients), pinning of the opposite hip as well is sometimes recommended to prevent it from occurring.
Severe or late cases have a high risk of AVN, which is the death of bone tissue caused by a disruption in its blood supply, leading to pain, stiffness, and potential bone collapse or joint destruction over time and permanent disability.
The take-home message
SCFE is treatable and preventable if recognised early.
If a child has an unexplained limp, especially with thigh or knee pain, don’t assume it’s just a strain. Ask the doctor directly: “Could this be SCFE? Should we get hip X-rays done?”
One simple question. One X-ray. It could save a child’s hip.
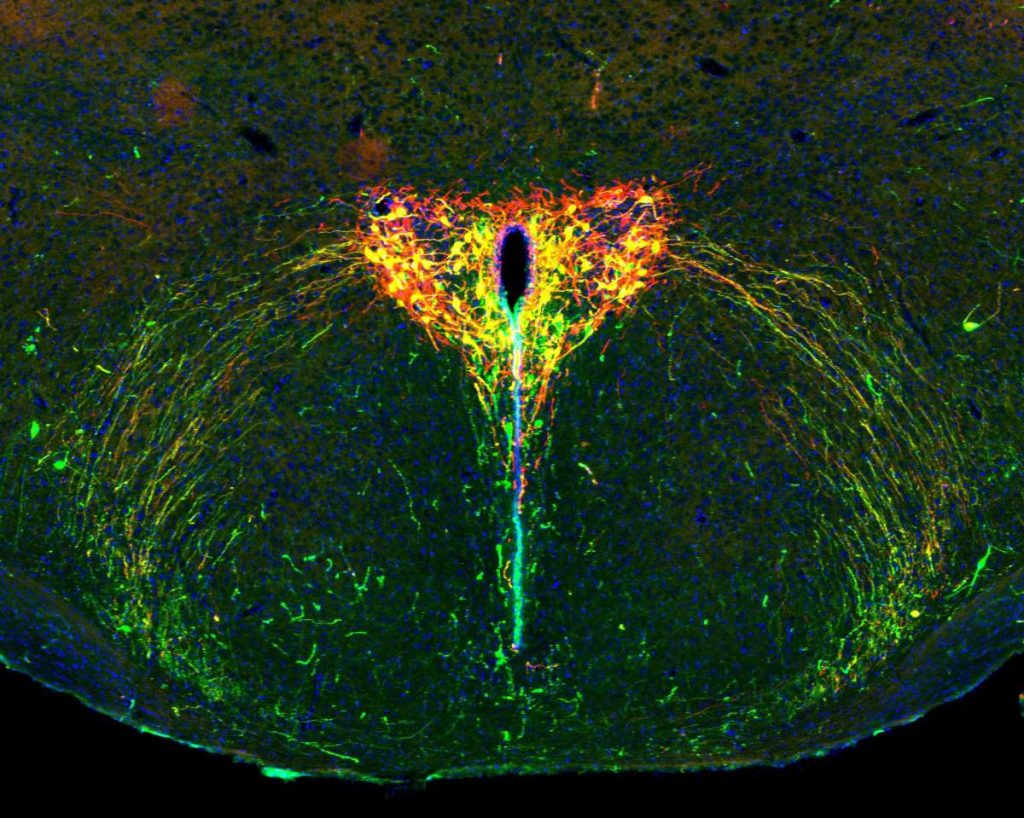
The developing brain of a two-week-old mouse pup under the microscope. The oxytocin system appears in green, the light-sensitive protein in red and cells that carry both show up in yellow. Cell nuclei are in blue. Credit: Weizmann Institute of Science
According to attachment theory, the attachment between an infant and a primary caregiver shapes the baby’s future social ties. Yet little is known about the biological mechanisms underlying childhood attachment, mainly because it is so difficult to study the young brain in natural conditions.
Now, scientists in Prof Ofer Yizhar’s laboratory at the Weizmann Institute of Science have developed a new, noninvasive research method that makes it possible to silence selected nerve cells deep within the brains of mouse pups without disrupting their natural behaviour. Using this method, the researchers investigated the role of oxytocin, a short protein released from nerve cells in the brain. While most oxytocin research has focused on adults, the new findings, published in Science, show that oxytocin also shapes the social behaviour of pups and may underlie emotional differences between males and females that emerge early in life.
Oxytocin, sometimes referred to as the “love hormone,” was once thought to simply promote sociability in adults. Over time, however, it became clear that its role is far more complex: In some circumstances, it intensifies behaviors and emotions far removed from love, such as anxiety or aggression. Recent research has also shown that young mammalian brains – including those of human children – are especially sensitive to oxytocin. In brain regions responsible for sensory processing, emotional regulation and social behavior, the number of oxytocin receptors peaks during early childhood: around ages two to three in humans, and two to three weeks in mice. Some studies have even linked oxytocin deficiency to childhood autism. Still, without sufficiently precise tools to examine neural activity deep within the developing brain, many aspects of the role of oxytocin in early life have remained a mystery.
“The findings may offer a clue as to why males and females diverge in their social behaviors and emotional worlds long before puberty”
To shed light on the subject, a team led by Dr Daniel Zelmanoff, a physician-scientist in Yizhar’s lab, developed a noninvasive technique to probe specific nerve cells in the young brain. The group, pioneers in the field of optogenetics – a technology that uses light to switch individual cells on or off – devised a method in which the targeted brain cells of mouse pups are infected with an engineered virus. This otherwise harmless virus introduces a foreign gene of mosquito origin that encodes a light-sensitive protein; when exposed to light, the protein “turns off” the nerve cell. In fact, the protein is so light-sensitive that the researchers could silence selected nerve cells deep inside the brain simply by shining red light on the pups’ heads.
“This new method allows us to peek inside the brain without disturbing the pups’ everyday lives, making it a powerful tool for studying nervous system development,” Yizhar explains. “It is especially useful for studying oxytocin because this hormone’s effects depend on social context – and our method lets us switch off the oxytocin system on demand, only during the exact situation we want to study.”
The researchers focused on oxytocin’s role during the temporary separation of a mouse pup from its mother and their reunion a few hours later – a situation familiar to every parent of a young child. The scientists observed increased oxytocin activity in the pup’s brain during separation, which returned to normal after reunion with the mother. Pups with an active oxytocin system during the separation gradually adapted to being alone in an unfamiliar environment, producing fewer ultrasonic vocalizations – the mouse equivalent of a baby’s cry. In contrast, pups whose oxytocin system was silenced did not adapt; they continued emitting distress calls at the same rate until reunited with their mothers. These findings show that the so-called “love hormone” also plays a critical role in coping with loneliness.
Attachment theory holds that children who are securely attached to their parents show distress when separated from them but are able to calm down over time, feeling free to explore their surroundings. “We discovered that mouse pups need an active oxytocin system in order to adapt to separation from their mothers,” says Yizhar. “This suggests that the oxytocin system plays a role not only in the brain of the parent, which was already known, but also in that of the infant. In addition, since oxytocin receptors are present in the sensory processing centers of the young brain, we hypothesize that this hormone also helps sharpen a pup’s senses when it is alone.”
Children do not quickly forget the experience of being separated from their parents, and this separation shapes how they behave when reunited. For example, a securely attached child separated from a parent for a few hours will seek contact upon reunion, and is quickly calmed. The researchers found that activation of the oxytocin system in mouse pups during separation not only strengthened them in the moment but also determined how they behaved when their mothers returned. These pups emitted more ultrasonic calls than usual, and the frequency of the calls grew as they got closer to their mothers. Using artificial intelligence, the team identified a distinct vocal pattern: Before attaching to the mother’s nipple, the pups made high-pitched, frequent calls; afterwards, their calls dropped in pitch and slowed in tempo.
“Activating the oxytocin system during separation increases the pup’s motivation to regain closeness to the mother when reunited,” Yizhar explains. “This is reflected in the heightened rate and unique pattern of their calls. We now understand that these ultrasonic vocalizations are much more than just crying: The high-pitched, rapid calls appear to signal a request for closeness, while the lower-pitched, slower-paced calls likely express a quick return to calm and a wish to remain attached. Of course, more research is needed to pin down the exact meaning of each vocalization type.”
In the next stage, the researchers explored whether oxytocin’s role in pups differs between the sexes, as it does in older animals. They found that female pups with an active oxytocin system emitted many more ultrasonic calls when reunited with their mothers than females with silenced oxytocin systems, whereas the calls of male pups were unaffected by the status of their oxytocin systems. “This is the first sex difference observed in oxytocin system activity at such an early stage of development,” Yizhar notes. “It may offer a clue as to why males and females diverge in their social behaviours and emotional worlds long before puberty.”
“Most known functions of oxytocin are shared by all mammals,” Yizhar concludes. “Still, future studies must check whether the hormone affects the development of social behaviour, emotional maturity and maternal attachment in the brains of children. If so, this could help us better understand what can go wrong in emotional and social development – as in autism spectrum disorder, for example – and how to intervene at an early stage.”