If you’re a black, 34-year-old South African woman living with HIV, antiretroviral (ARV) treatment options have likely been limited to tenofovir disoproxil fumarate (TDF), lamivudine (3TC) and the ‘gold standard’ dolutegravir (DTG).
Now, another once-a-day, three-drug regimen has been found to be as effective as DTG in supressing HIV viral load.
Not only is the once daily regimen of tenofovir disoproxil fumarate (TDF), lamivudine (3TC) and doravirine non-inferior to DTG, it is associated with significantly less weight gain and has a better lipid profile than the combination favoured and recommended as first-line in many countries, and increasingly in low-and-middle income countries.
These were the end point findings of the South African Opti-DOR study presented at the 2026 International AIDS Society Conference on HIV Science on 31 July and published in the Journal of the American Medical Association (JAMA).
Dr Joana Woods, Senior Research Clinician at Ezintsha at the University of the Witwatersrand (Wits) and lead author, says:“The findings are important because although second-generation ARVs such as dolutegravir and bictegravir are highly effective HIV medicines, they have been consistently associated with substantial weight gain and new onset obesity, particularly among women and black populations and especially when combined with TAF. This has raised concern about long-term cardiometabolic risk, including diabetes and cardiovascular disease.”
In primary healthcare, prevention is better than having to deal with long term consequences. This is why in a country like South Africa with widespread HIV and NCDs, managing weight gain in people living with HIV is critical to their health.
“So if you can start an ARV that’s not going to cause as much weight gain, or not cause weight gain at all, or have an alternative, that would be first prize. And that’s the premise of this study,” says Woods.
About the OPTI-DOR Study
The Africa Health Research Institute (AHRI) ran the rural arm of the Opti-DOR study at the AHRI-Somkhele site in rural northern KwaZulu-Natal province.
“By including participants from both rural KwaZulu-Natal and urban Gauteng, we can be confident that these findings are relevant to people living with HIV in different communities across South Africa,” says Professor Limakatso Lebina, Principal Investigator at the rural AHRI-Somkhele study and Director of Science at AHRI.
The AHRI site enrolled 178 participants between December 2023 and March 2025, with the Johannesburg site enrolling the rest, for a total of 600.
Participants were randomised in a 1:1 ratio to receive either oral daily doravirine (TDF/3TC/DOR) or dolutegravir (TAF/FTC/DTG).
Weight gain differed significantly between the two study groups. Median weight gain at week 48 was 3.0 kg with doravirine (TDF/3TC/DOR) compared with 5.0 kg with dolutegravir (TAF/FTC/DTG).
Increases in total body fat percentage were also significantly lower with doravirine (TDF/3TC/DOR) at 1.5%, versus 2.2%.
“These results add some clarity to a challenge that has frustrated both doctors and patients for years: how to treat HIV effectively without causing significant weight gain,” says Lebina. “For many patients, especially black women who are disproportionately affected by treatment-associated weight gain, this could be a game changer. It offers an important new treatment option that supports long-term health while maintaining excellent HIV control.”
Non-inferior yet drug resistance potential
Woods emphasises that the efficacy of doravirine is dependent on patients’ absolute adherence to taking it. If doravirine is taken properly, HIV viral load will be suppressed. However, failure to adhere can cause drug resistance.
“Doravirine is non-inferior to dolutegravir in the sense that if you take the drug properly, you will suppress it [HIV viral load]. If you don’t take it properly, you will likely become resistant. That unfortunately is one of the downsides of using doravirine.”
In the Opti-DOR clinical trial, seven patients developed resistance to the drug. These participants were then switched over to dolutegravir and successfully suppressed again.
Woods emphasises that doravirine is unlikely to be a replacement for DTG: “It is not a replacement. It has to be targeted to patients who are at risk of gaining more weight – and complications thereof.”
Despite drug resistance, the data prove that doravirine is not inferior to dolutegravir and that it causes less weight gain.
Research into action
Doravarine is already an available and registered drug.
The researchers have alerted the South African National Department of Health and the South African Health Products Regulatory Authority.
“Imagine you’re a diabetic and you only have access to one drug? It’s the same thing with HIV. Yes, the drug they have at the moment is really top of the tops, but it doesn’t suit everybody. You have to have options. Until we can cure HIV, you’ve got to make it as easy as possible for people to take their treatment. That’s what it comes down to.”
Key findings of the Opti-DOR study at week 48
Doravirine [TDF/3TC/DOR] was non-inferior to dolutegravir [TAF/FTC/DTG] for viral suppression.
Viral suppression was achieved by 89.0% of participants on doravirine [TDF/3TC/DOR] and 90.7% on dolutegravir [TAF/ FTC/DTG].
Median weight gain was significantly lower with doravirine [TDF/3TC/DOR]: 3.0 kg versus 5.0 kg.
Total body fat percentage increased less with doravirine [TDF/3TC/DOR]: 1.5% versus 2.2%.
Lipid changes favoured doravirine [TDF/3TC/DOR].
Glycaemic measures and blood pressure were similar between arms.
No emergent integrase inhibitor resistance was observed.
Bone mineral density declined more with doravirine [TDF/3TC/DOR].
Serious adverse events and major laboratory abnormalities were infrequent across and similar between both groups, and not considered treatment related.
Through Cipla’s voluntary licensing agreement with Merck (MSD), Cipla may support potential future access to generic alimatravir, an investigational medicine being studied for HIV-1 pre-exposure prophylaxis (PrEP).
The announcement underscores Cipla’s role in supporting responsible partnerships at a critical moment for the global HIV response, as global leaders, researchers and healthcare professionals convene in Brazil this week for the world’s largest HIV and AIDS conference.
Through the agreement, Cipla may produce generic alimatravir following completion of development, applicable regulatory approvals, technology-transfer requirements and any other country-specific requirements. The voluntary licensing agreement builds on Cipla’s vertically integrated capabilities across the pharmaceutical value chain, enabling the company to support the development and manufacturing activities, under the terms of the agreement.
As one of Africa’s leading pharmaceutical companies, Cipla has contributed to improving access to critical HIV medicines and prevention-related public-health programmes across the continent. In the early 2000s, Cipla made quality, affordable antiretrovirals available at less than $1 per day, contributing to wider access to HIV treatment during a critical period in the global HIV response.
Building on this legacy, Cipla continues to strengthen its contribution to public health through the development, manufacture and distribution of high-quality, affordable medicines that support national and regional HIV priorities, where such medicines are appropriately authorised and supplied in accordance with local requirements.
Paul Miller, CEO of Cipla Africa, said: “Cipla’s vision has always been to make quality healthcare more accessible for patients who need it most. This licensing agreement reflects our long-standing commitment to supporting responsible innovation in HIV prevention for the patients and communities we serve. We believe that expanding future access, where permitted by applicable regulatory requirements, requires extensive manufacturing expertise, reliable supply chains and strategic partnerships that can translate scientific innovations into real-world impact.”
Investment in Local Manufacturing, Sustainable Access
Cipla’s manufacturing network and established presence across African markets position the company to support widespread, sustainable access to HIV medicines. Through decades of experience in producing and supplying medicines at scale, Cipla has helped strengthen healthcare systems and HIV treatment programmes.
The company also remains committed to supporting local healthcare priorities by investing in local manufacturing capabilities and working collaboratively with governments and healthcare professionals to improve access to life-saving medicines. Cipla has been supplying the South African government with equitable access to HIV medication for a number of years. These efforts align with broader ambitions to strengthen pharmaceutical manufacturing capacity on the continent, reinforcing Cipla’s commitment to secure and ensure reliable ARV supply.
Most recently for example, Cipla made significant investments in its local manufacturing facility, upgrading the capacity of the ARV production line with the installation of a new Countec bottle line and increased its tablet filing capacity by 190%. The company is able to locally produce 475 million ARV tablets annually and has upscaled its manufacturing capabilities to ensure sufficient capacity to meet current demand and support near‑term growth, ensuring continuity of supply. Cipla’s overall manufacturing capacity is 1,625 billion tablets annually.
“With a long history of leadership in HIV treatment and prevention, Cipla remains dedicated to helping shape a future where innovative healthcare solutions are accessible, affordable and available to communities across Africa. We want people to live a long and healthy life as part of our ethos of caring for life,” said Paul Miller, CEO of Cipla Africa.
*According to Statistics South Africa, the number of people living with HIV in the country is estimated to be approximately 8 million (12,7% of the population)[1].
Important regulatory notice: Alimatravir is an investigational medicine. It is not registered by the South African Health Products Regulatory Authority (SAHPRA), has not been approved for sale or supply in South Africa, and is not currently available in South Africa. Its safety, quality and efficacy have not been evaluated or approved by SAHPRA. This communication is a corporate announcement about a voluntary licensing agreement and is not intended to promote, recommend or encourage the use of any medicine.
Alimatravir remains investigational and no claims are made regarding its safety, efficacy or suitability. No availability in South Africa is implied by this announcement. Any future availability remains subject to successful completion of development, regulatory approval and applicable local authorization requirements.
Taking antiretroviral therapy as recommended has expanded the lifespan of people with HIV. (Photo: Unsplash)
By Elna Schütz for Spotlight
South Africa’s first set of clinical guidelines focused on older people living with HIV has been released. They offer practical steps in a resource-strained health system to take care of an ageing patient population.
The guidelines are particularly important in South Africa since the country has an ageing population of people living with HIV. Many of these people would only have started treatment relatively long after they contracted the virus, largely because of the government’s reluctance to make antiretroviral treatment available in the early 2000s. The sooner people start treatment after infection, the better their long-term prognosis tends to be.
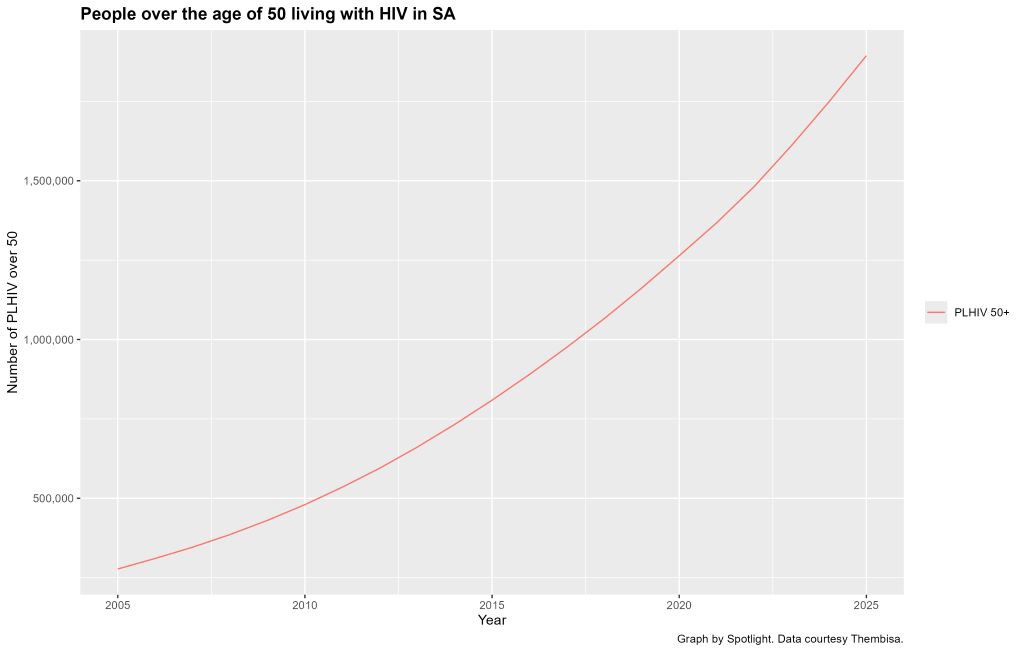
In 2025, there were around 1.9 million people over the age of 50 living with HIV in South Africa, according to Thembisa, the leading mathematical model of HIV in the country. This is 24% of the estimated 7.9 million HIV positive people in the country. The 1.9 million figure is more than double the 800 000 people over 50 who were living with HIV in 2015. This number is projected to rise to over 3.6 million by 2035.
Most people over the age of 50 who are living with HIV contracted the virus before they turned 50. The increase depicted in this graph is thus mainly a function of people who are already living with HIV ageing into the over 50 age group. Some people over 50 do become newly infected with HIV, but those numbers are comparatively small.
The changing make-up of the population of people living with HIV, coupled with the fact that antiretroviral therapy has been crucial for clearing and suppressing HIV in the body was a core driver for developing the new guidelines, Dr Camilla Wattrus, the Clinical Director at the Southern African HIV Clinicians Society, tells Spotlight. She is one of the guidelines’ authors.
“Antiretroviral therapy has expanded the lifespan of people with HIV, but we must now also consider how to preserve the ‘health span’ in this group,” says Wattrus.
She explains that this means increasing the years that are spent in good health with a good quality of life.
Another co-author of the guidelines, Nomathemba Chandiwana, Chief Scientific Officer at the Desmond Tutu Health Foundation, points out that after antiretroviral treatment was introduced in South Africa, the life expectancy of people living with HIV increased dramatically. “We didn’t think people would live as long as they have now, so that’s been a big success,” she says. “But now we have new problems.”
Chandiwana says that older people living with HIV have around 16 fewer years in good health than people without HIV. The 16-year figure (technically 15.3) seems to originate in a study published in 2020 in the JAMA medical journal that compared the health and lifespans of insured people with and without HIV in the United States. For people with HIV who started antiretroviral treatment when they were still healthy (CD4 countes above 500), the difference in healthy years was 9.5 years.
Another broad concern is that clinicians may be focused on HIV-related issues like viral suppression for these patients and not be sufficiently aware of other ageing-related developments. People with HIV get the same ageing related diseases as other people, but there is evidence that they tend to get them earlier.
We know from Thembisa model outputs that on average, people living with HIV today are slightly more likely to die of non-HIV-related causes than AIDS. According to the model, there were 53 000 HIV-related deaths in the year from mid-2024 to mid-2025. This is a thousand fewer than the 54 000 people with HIV who died of non-HIV-related causes over the same period.
What is in the new guidelines
The new guidance states that it is designed to:
Raise healthcare workers’ awareness of the needs and concerns of the population of people living with HIV who are 50 years and older.
Inform healthcare workers about an ageing-related approach to older people with HIV.
Highlight good practices to help healthcare workers provide optimal care for this population.
Provide resources about ageing with HIV for healthcare workers, their patients and their patients’ carers.
Guide clinical settings in implementing geriatric care into HIV clinical practice.
The clinical advice in the guidelines follow the World Health Organisation’s (WHO) principles for Integrated Care for Older People (ICOPE), which emphasises prevention prior to frailty, person-centred assessment, and the involvement of healthcare workers other than doctors.
The guidelines cover a thorough list of challenges faced by older people with HIV that need to be monitored and addressed. For instance, physiologically, there is a risk of comorbid conditions like hypertension and cancer, and an increased risk of complications from polypharmacy, when more than five medicines are used concurrently. Social and behavioural challenges include that older people are perceived to be less likely to get infected with HIV and therefore have lower rates of HIV testing and use of HIV prevention tools.
This population is also at risk of being disregarded or not fully cared for in the healthcare system. The guidelines give examples such as restricted mobility access to health facilities and healthcare workers being unaware of the HIV-related risks in older people. “The health system needs to be equipped to manage their needs in a holistic and integrated way, and that is what this guideline aims to support,” says Wattrus.
The guidelines include a comprehensive schedule of what need to be assessed and screened and at what regularity. There is a particular focus on geriatric syndromes like frailty, cognitive impairment, and managing comorbid non-communicable diseases.
“The idea is that every visit with an older patient involves more than just routine HIV care and that it becomes a conversation about how that person is functioning and living,” says Wattrus.
The guidelines also emphasise how care can be offered by a variety of healthcare providers, depending on the resources available. “Recommendations enable task-shifting, which is a practical necessity in a country where specialists such as geriatricians are scarce, and the bulk of HIV routine care is delivered by healthcare workers at primary care level,” says Wattrus.
Even though the guidelines focus on overall health in older people living with HIV, managing HIV is, of course, a part of this. It cautions that “CD4 recovery may be slower and blunter compared to younger individuals,” but viral suppression is still the primary treatment goal.
The crucial factor here is to choose the correct antiretroviral treatment regimen for the patient. For instance, popular tenofovir disoproxil fumarate (TDF) combinations should be avoided in people at risk of or with osteoporosis, bone fractures, or renal impairment. Regimens with tenofovir-alafenamide or abacavir may be better, though the latter is contraindicated if there is high cardiovascular risk.
The new local guidelines hit largely the same notes as a major commission on HIV and ageing that was published by the journal Lancet HIV to coincide with the AIDS 2026 conference taking place in Rio de Janeiro, Brazil.
“Supporting healthy ageing requires more than sustained viral suppression; it requires care that is informed by what matters most to the individual, with attention to maintaining physical and mental function, minimising healthcare complexity, and addressing multimorbidity, polypharmacy, stigma, and social determinants of health,” the commission found.
Simple systems, big change
Apart from giving healthcare workers a framework for giving better care to older people living with HIV, the guidelines advise how this larger change in the health system can happen for this growing older population. “What is great is that most of the recommendations are not complicated or expensive,” says Wattrus.
She explains that the sensitisation and training of healthcare workers, especially in primary care, is a crucial first step. If they know how to, they can easily incorporate brief screenings, such as those for frailty, into normal appointments. For example, as Chandiwana points out, several geriatric tests need only a chair for the patient to sit down on and get up from. She says it is easier to do these things for people with HIV during their existing appointments, compared to people without HIV who may not be visiting health facilities for regular screenings.
Another relatively easy adaptation is to simply make healthcare services easier to access. “This can be done by having appointments aligned across conditions, fewer unnecessary referrals and genuine attention to broader aspects of their health such as poverty, isolation and limited mobility,” she says.
Chandiwana also suggests that one could consider rolling out geriatric care health cards to track screening, as is often done with children. She would also like to see more community buy-in, in a similar way as there was during the earlier part of the HIV treatment roll-out. For instance, she suggests community health clubs and increased health literacy efforts around ageing.
Avoiding problematic polypharmacy, says Wattrus, is another low-cost, high-yield strategy that does not require specialist input. “Routinely reviewing medication lists, identifying unnecessary drugs, and checking for interactions is straightforward and can make a significant difference,” she says.
More specialists would of course help. Chandiwana says there are fewer than 50 geriatric specialists in the country. She says there is also a much wider need for geriatric-specific training across the healthcare system, including for primary care nurses and community healthcare workers.
Lastly, Chandiwana says the guidelines offer a much-needed look into the unique challenges and needs of older people with HIV as an opportunity for the government to act to prevent a future problem. “So that investment in having scalable, simple systems for people who are ageing, both with HIV and without, I think, would be fantastic, but that needs money,” she says.
If an HIV prevention pill that provides a month of protection at a time performs well in two ongoing clinical trials, it could become the next big thing in HIV prevention after the lenacapavir injection. A new licensing agreement is paving the way for South Africa’s Aspen Pharmacare to produce the pill should the study findings be positive and the drug be registered.
In June, South Africa’s health department started rolling out the six-monthly lenacapavir HIV prevention injection to around 10% of public sector clinics. While the rollout of this jab still has a long way to go, the next generation of HIV prevention products is already on the horizon.
Two of those new products stand out. One is a new formulation of lenacapavir that looks as if it can provide 12 months of protection at a time. While results so far are promising, the pivotal data on this once-yearly HIV prevention jab is only expected in a year or two.
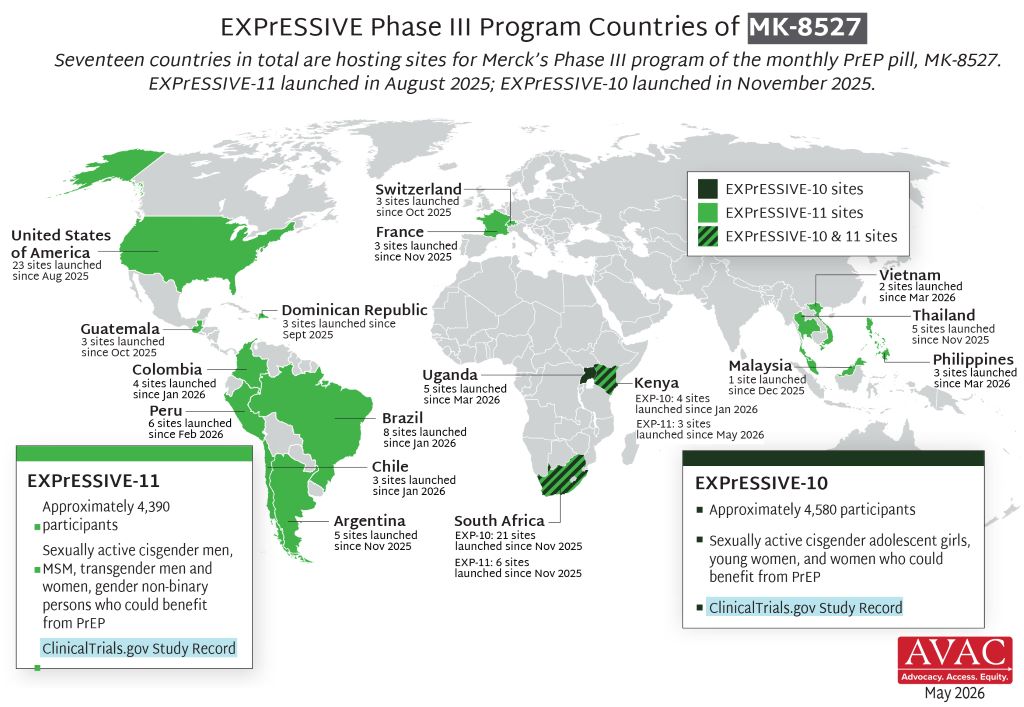
The other product that has many people in the HIV world excited is a monthly HIV prevention pill that contains a highly potent antiretroviral medicine called alimatravir (it was previously called MK-8527). It starts working within around an hour after someone takes it and appears to provide a month of protection at a time. One benefit of the pill, compared to the lenacapavir injection, is that it would be easier to distribute at scale, given that there is no need for a nurse to administer an injection.
As Spotlight reported in some depth last year, alimatravir looked very promising in a phase 2 study, although for now the jury is still out on the drug’s safety and efficacy. It is currently being evaluated in two pivotal phase 3 clinical trials called EXPRESSIVE-10 and EXPRESSIVE-11. Both these studies started last year and are expected to be completed by around mid-to-late 2027. Medicines are typically only registered for use after positive results in such phase 3 studies.
“The monthly pill offers an alternative for people who would like a long acting, less frequently dosed PrEP but not needle friendly … so it really is about giving more options especially on the pill side,” Professor Linda-Gail Bekker, primary investigator in South Africa on the EXPRESSIVE-10 study, told Spotlight. “You could imagine that just having to remember to take a small easy to swallow pill on the day you pay your bills monthly could be very easy for people. We understand that the packaging is also going to be very user friendly- looking more like a gum packet than a bottle of antiretroviral pills which may also reduce stigma.” (PrEP refers to pre-exposure prophylaxis like HIV prevention pills or injections.)
Licence to make generics
The prospects for future access to alimatravir got a major boost last week when the pharmaceutical company Merck (known as MSD outside of the United States and Canada) announced that it granted licences to seven different companies to produce generic versions of the monthly pill. One of the seven companies is South Africa’s Aspen Pharmacare. The others are Uganda’s Quality Chemical Industries Limited, Kenya’s Universal Corporation Ltd, and Aurobindo, Cipla, Emcure and Viatris in India.
Early responses to the licences have mostly been positive.
Having a generic company with a licence in South Africa is excellent news, said Bekker.
“It is particularly exciting to see manufacturers in Kenya, South Africa and Uganda included in these licenses,” Mitchell Warren, Executive Director of AVAC (a global HIV advocacy group), told Spotlight by e-mail. “These are the first generic PrEP licenses in East and Southern Africa, meaning manufacturing can happen where trials are happening, where need is greatest and where we have the largest PrEP markets.”
“Through our agreement with MSD (Merck), we have the opportunity to support the future supply of an innovative HIV prevention option while strengthening local pharmaceutical manufacturing and healthcare resilience across the continent,” Stephen Saad, Aspen Group Chief Executive, said in a media statement. Under the agreement, the company says it will receive a technical package from Merck, together with licensing rights covering 129 countries, including all African countries.
Speaking to Spotlight, Stavros Nicolaou, Aspen’s Head of Strategic Trade, described alimatravir as “ground-breaking and a potential game-changer”. He commended Merk for starting the licensing process so early. He framed the licence as an important step forward for both South Africa’s HIV response and for local production of antiretrovirals, although he also raised concerns about the procurement of locally manufactured antiretrovirals – the percentage of South Africa’s antiretroviral tenders awarded to local manufacturers has been trending downward.
According to earlier reporting by Business Day, Nicolaou has declined to give any indication as to a potential price for the pill, but he did tell the publication that they could potentially supply it for both South Africa’s public and private sectors.
There are indications that a relatively low price is on the cards. Research being presented at AIDS 2026 this week found that alimatravir could be mass produced and sold at a profit for as little as $15 (around R250 to R300) per person per year. This is less than half the $40 per person per year that South Africa is expected to pay for generic lenacapavir injections in a year or two from now.
“Merck expects to provide initial supply and continue supplying product as needed while licensed generic manufacturers complete development, obtain the necessary regulatory approvals and prepare to provide supply in the licensed territories. The goal is to help avoid delays in access by providing an initial supply pathway until generic manufacturing capacity is established and brought online,” the company said in a media statement.
Earlier licensing
The timing of the licensing announcement is somewhat unusual – such announcements are typically only made after phase 3 trials have been concluded and it is confirmed that the drug is safe and effective.
“Granting licensing agreements to generic manufacturers while clinical trials are still enrolling, before it is known if the product is effective, should significantly reduce the time to market for the product,” Warren said in an earlier AVAC media statement. “The timeline announced today gives us ample opportunity to work with ministries of health, donors, communities, and Merck to plan for broad access to the monthly PrEP pill.”
Warren told Spotlight that the small amount of active drug in alimatravir and the fact that it is an oral dose should make the technology transfer from Merck to generics quite quick. “The hope would be that genetic alimatravir reaches the market within months of the approval of the originator, compared to more than a year for lenacapavir,” he said.
Nicolaou was also upbeat about how quickly things are unfolding. He said that Merck’s decision to execute licences while the phase 3 clinical trials are ongoing allows for an earlier registration pathway (if phase 3 findings are positive, alimatravir will have to be filed for registration with regulators like the South African Health Products Regulatory Authority). He also pointed out that it is a small tablet and that it should be easier to manufacture than HIV prevention injections.
Nicolaou told Spotlight that the plan is for Aspen to do formulation of alimatravir in South Africa, but that they are not currently planning to produce the active pharmaceutical ingredient – this will likely be sourced from Chinese or Indian suppliers.
Some activist criticism
But while the timing has generally been welcomed, there has also been some criticism over the licenses.
A statement from activist group HealthGap points out that Latin American countries like Brazil, Argentina, and Colombia are not included in the list of 129 countries covered by the license, even though some of the phase 3 trial sites for alimatravir are in these countries. The HealthGap statement calls for compulsory licenses to be issued.
In an earlier statement, Merck said that, in recognition of the significant unmet need in Latin America, “Merck is in active discussions with organizations, including Fiocruz (a key player in medicines production and procurement in Brazil), with a goal to enable rapid availability and broad supply of alimatravir in the region”.
Disclosure: The Gates Foundation has provided financial support for clinical trials of alimatravir. Spotlight receives funding from the Gates Foundation, but is editorially independent – an independence the editors guard jealously. Spotlight is a member of the South African Press Council.
Researchers have found that a new once-weekly antiretroviral formulation appears to be as effective as the daily pills. Photo by Danilo Alvesd on Unsplash
By Marcus Low and Elri Voigt
A new antiretroviral combination pill that is taken only once a week appears to work as well as daily pills at treating HIV. This is according to interim study findings to be presented next week at the AIDS 2026 conference in Rio de Janeiro, Brazil.
Almost all of the over six million people in South Africa who are currently taking HIV treatment are taking it in the form of one tablet taken once a day. These tablets contain a combination of three different antiretrovirals, most commonly dolutegravir, lamivudine or emtricitabine, and tenofovir.
Now researchers have found that a new once-weekly antiretroviral formulation appears to be as effective as the daily pills. The new pill contains only two antiretrovirals, islatravir and lenacapavir. A different formulation of lenacapavir is used in the six-monthly HIV prevention injections being rolled out at around 10% of public sector clinics in South Africa.
“I think this is the next treatment blockbuster,” Professor Francois Venter told Spotlight this week when asked about the new once-weekly pill. Venter is the Executive Director of the Ezintsha Research Centre at the University of the Witwatersrand. He was not involved in the studies of the once-weekly pill.
“Patients are crying out for less frequent dosing, and it does not have the fiddliness and complexity, the supply line, healthcare worker training, or resistance issues of the current or immediate next generation of injectables. Imagine dispensing the same number of tablets for 6 months as previously for a month. It looks cheap to make. Low- and middle-income countries really should be taking note,” he said.
Two studies
The findings to be presented in Rio are from the first 48 weeks of two relatively large, multi-country, phase 3 studies called ISLEND-1 and ISLEND-2. Both studies will continue for another 48 weeks. The final study findings will only be reported after the full 96 weeks are completed.
The two studies have similar designs. Both started out with people who were already on antiretroviral therapy and doing well on treatment (607 people in ISLEND-1 and 624 in ISLEND-2). The researchers then switched roughly half of the people in each study over to the weekly islatravir/lenacapavir pill. The outcomes of those who switched to the weekly pill were then compared to those who didn’t switch and simply kept taking the treatment they had been taking before.
A key difference between the studies is in the control groups. In ISLEND-1, the researchers specifically recruited just people who were taking the antiretroviral combination of bictegravir, emtricitabine, and tenofovir alafenamide. In ISLEND-2, they recruited people who were taking whatever the local standard of care was (which often differs between countries). Some of the many ISLEND-2 clinical trial sites are in South Africa where the standard of care is dolutegravir, lamivudine or emtricitabine, and tenofovir.
Another notable difference between the studies is that ISLEND-1 is double-blinded, whereas ISLEND-2 is an open label study. This means that in ISLEND-1 neither study participants or their doctors know which study arm they are on – this is achieved by also giving people on the weekly arm daily placebo pills and people on the daily arm pills that look like the weekly placebo. In ISLEND-2, people know what study arm they are on and there is no need for placebos.
Both studies have a non-inferiority design, which is to say their main aim is to establish whether the weekly pill is roughly as safe and effective as existing treatments. Such designs are commonly used in HIV treatment trials given that existing treatments are already very safe and effective. The potential step forward in this research is the weekly dosing, not improved safety or efficacy against HIV.
“Developing new antiviral HIV medications remains important in order to address pill fatigue, adherence challenges, broaden treatment, with the goal of ending the HIV epidemic,” Professor Jürgen Rockstroh, lead author of the presentation of the ISLEND-1 results at AIDS 2026, told Spotlight by e-mail.
What the researchers found
The short version, as described in a conference media release, is that in both studies the weekly pill was found to be “efficacious and well tolerated and statistically non-inferior” to the controls it was measured against. In other words, based on the 48-week data, the weekly pill is passing the test so far. The findings have also been summarised in a media statement by pharmaceutical company Gilead Sciences.
The key indicator that the researchers looked at was the proportion of people whose HIV viral load was not suppressed at 48 weeks (they used a cut-off of 50 copies per millilitre of blood). If antiretroviral treatment is working well in someone’s body, one’s viral load is typically suppressed below this level.
In ISLEND-1, zero of the people on the weekly pill had a viral load above the cut-off, while one person on the bictegravir, emtricitabine, and tenofovir alafenamide study arm was above the cut-off. In ISLEND-2, one person taking the weekly pill had a viral load above the cut-off, while four people on the standard of care arm were above the threshold. Given that outcomes on the weekly pill were technically better than for the controls, it should come as no surprise that the non-inferiority thresholds were met.
Though the once-weekly pill was well-tolerated, there are some interesting nuances in the safety data. In ISLEND-1, treatment-related adverse events were very similar between the two study arms. In ISLEND-2, however, treatment-related adverse events were reported in 18% of participants treated with the once-weekly pill compared to less than 1% receiving standard of care antiretroviral regimens. Among those receiving the weekly pill in ISLEND-2, the most common treatment-related adverse events reported were headache (5%), nausea (3%) and diarrhoea (3%). There were no red flags regarding more serious treatment-related adverse events.
“It is not uncommon to see a higher rate of treatment related adverse events in the experimental arm of an open label switch study due to reporting bias. That is, when someone knows they are on a new drug, they may be more apt to believe that any new symptoms are caused by the new drug,” Dr Amy Colson, a principal investigator for both ISLEND studies at a study site in Boston in the United States, explained to Spotlight. “Of note, all treatment related adverse events in ISLEND-2 were grade 1 or grade 2. And importantly, the rate of treatment related adverse events in the ISLEND 1 study – which was a double-blind study – was nearly identical in the islatravir/lenacapavir and bictegravir/emtricitabine/tenofovir alafenamide arms which further supports that the discrepancy in ISLEND 2 may indeed be due in part to reporting bias in the open label study.” (Adverse events are graded from 1 to 4, with 1 being the least severe. Only grade 3 and 4 adverse events are considered severe.)
“It is too early to comment on how any safety signals from the ISLEND 1 and ISLEND 2 trials will impact eligibility for future studies or eligibility for treatment outside of clinical trials. However, safety data at week 48 from both trials was reassuring. The overall rates of adverse events, grade 3 adverse events, serious adverse events and discontinuations due to adverse events was highly comparable between islatravir/lenacapavir and comparator groups in both trials,” Colson said.
The early data from ISLEND-2 suggests that people who switched to the once-weekly pill prefer it to the daily treatments they were taking before. According to Colson, 78% reported that they were more or much more satisfied with the weekly pill relative to their prior daily treatment and 64% reported that their prior daily treatment was more of a burden than the weekly pill. More extensive data on people’s self-reported experience of the treatment will be reported on at a future conference.
The new weekly pill is not the first long-acting form of HIV treatment, although it is the first long-acting HIV treatment in pill form. HIV treatment injections administered every two months have been available in the United States for around four years. Spotlight has previously explored in depth why we do not have these HIV treatment injections in South Africa.
Next steps
In a media statement released early in June, pharmaceutical companies Gilead Sciences and Merck (called MSD outside of the United States and Canada) indicated that they plan to file the once-weekly pill with medicines regulators “globally”. Spotlight asked both companies whether this will include filing with the South African Health Products Regulatory Authority, but neither company answered this question. Gilead has the patent on lenacapavir and Merck on islatravir. ISLEND-1 and ISLEND-2 were sponsored by Gilead. Gilead has already filed a weekly lenacapavir pill, used for HIV prevention rather than treatment, for registration with the United States Food and Drug Administration.
The companies didn’t provide details in response to Spotlight’s questions on their pricing plans and whether they would license other companies, directly or through the Geneva-based Medicines Patent Pool, to produce generic versions of the pill.
“Merck and Gilead are committed to supporting global efforts to reduce the incidence and burden of HIV by bringing forward new treatments. This includes our joint investigational long-acting oral treatment option, ISL/LEN. The single-tablet regimen represents a potential step-change in HIV treatment by offering a once-weekly oral regimen that may broaden choice for people living with HIV,” a Merck spokesperson told Spotlight by e-mail. “We remain focused on advancing the development program. If approved, our decades of experience collaborating with a range of stakeholders will help us explore pathways with the goal of facilitating rapid uptake and broad access around the world.”
Vaccine approach yields high numbers of HIV-neutralising antibodies in non-human primates
Colourised scanning electron micrograph of HIV (yellow) infecting a human T9 cell (blue). Credit: NIH
A new HIV vaccine developed by La Jolla Institute for Immunology (LJI), Scripps Research scientists, and IAVI has the potential to protect humans from developing HIV infection and AIDS. This HIV vaccine is the first to generate a high number of ‘broadly neutralising’, virus-fighting antibodies in primates.
“This feels like a huge success,” says LJI Professor and Chief Scientific Officer Shane Crotty, PhD, who co-led the research with Scripps Research Professor William Schief, PhD. “We constructed a successful vaccine from the ground up, which required a deep understanding of the immune system.”
This groundbreaking research, published inNature, is the result of 14 years of collaboration between La Jolla Institute for Immunology and Scripps Research, as part of the Scripps Consortium for HIV/AIDS Vaccine Development (CHAVD). “This has been one of those Apollo moon mission-type projects, where there is an exceptional goal and the team has to accomplish a myriad of discoveries and inventions along the way,” says Crotty.
Outsmarting HIV
The new vaccine works by intervening in a process called B cell maturation. B cells make antibodies. Like many immune cells, B cells have an early ‘naïve’ stage before they are ready to make antibodies. B cells start to mature once they get the signal that a pathogen, such as a virus, is trying to attack. B cells see pieces of that pathogen’s molecular structure and start producing antibodies that can bind to that structure and halt infection.
It can take a little while for B cells to find the right “bullseye” on a pathogen. But B cells keep trying. As they mature, B cells tweak their antibody production, refining antibody structures to bind to a pathogen in just the right, vulnerable spots.
Scientists describe B cell development as a training process or bootcamp. In most cases, the body is left with a well-honed B cell army.
HIV is hard to beat because it doesn’t give B cells a chance to develop effective antibodies. The first problem is that HIV disguises itself from the immune system. The virus is wrapped in an ever-shifting cloak of sugar molecules, called glycans. This lets HIV sneak undetected past human cells, which are also covered in glycans.
The second big problem is that HIV mutates very quickly. “The worldwide diversity of HIV mutations is extraordinary. Even the diversity within one individual person living with HIV is dramatic,” says LJI Instructor Patrick Madden, Ph.D., who served as study co-first author with Jon Steichen, Ph.D., an institute investigator at Scripps Research.
The third problem is that HIV changes its shape when it infects human cells. Even if B cells get a glimpse of its viral structure – snap! – the structure changes.
Taken together, these problems rarely give B cells a chance to hone their antibody responses against HIV. Even if a B cell manages to make neutralising antibodies, the virus can mutate or change its shape, rendering those antibodies useless.
The LJI and Scripps Research teams spent years hunting for ‘broadly neutralising’ antibodies that can actually bind to HIV and recognise key viral structures, even if the rest of the virus mutates. These antibodies are very, very rare, but they can be found in blood samples from a small number of people living with HIV.
An effective HIV vaccine would need to prompt the immune system to make these same broadly neutralising antibodies. “How could we flip the whole immune response on its head so the rare responses become the common responses? That was a critical challenge we faced,” says Crotty.
Testing the new vaccine
It was time to go back to B cell bootcamp. The scientists studied what made the HIV-fighting B cells special. Then they reversed the process to see exactly how those B cells matured. By looking back at the maturation process, the researchers could track how the B cells changed when they saw specific pieces of the HIV structure.
The team discovered that B cells matured to make broadly neutralising antibodies after they got an early look at parts of HIV’s outer “envelope” protein. Because these viral sites sparked an immune response, scientists would call them “antigens.”
An effective HIV vaccine would likely need to include models of these antigens. The antigens would work like mugshots of America’s most wanted. If B cells saw those antigens early and often, they would get really good at recognising and even neutralising HIV. “We were trying to mimic the progression of those neutralising antibodies,” says Madden.
In a feat of molecular engineering, the Schief Lab developed vaccine molecules that resembled the real HIV antigens. The scientists then worked with Emory National Primate Research Center, to test this potential HIV vaccine in a non-human primate species called rhesus macaques.
The researchers first administered a “priming” vaccine meant to activate each animal’s naïve B cells. The animals then received a series of “shepherding” booster shots to help their B cells develop along the right path.
“This series of vaccinations will guide, or ‘walk’, a B cell from its naïve state to its broadly neutralising state,” says Madden.
This new type of vaccine approach is called “germline targeting” because it targets naïve B cells in their ‘germline’ or naïve form, before they begin their training process.
The scientists found that around 44 percent of the animals went on to produce broadly neutralising antibodies against HIV in their blood. These antibodies were impressively abundant.
“We succeeded in taking ultra-rare antibody responses and turning them into common responses by the end of the vaccination process,” adds Crotty. In other research recently published, they reported a new strategy to accelerate related vaccine antibody responses [See Nature Immunology paper].
The team didn’t test whether these antibodies could prevent infection, but it’s significant that these antibodies could be found in the blood, where they could encounter and potentially block HIV.
Bringing the HIV vaccine to humans
The Crotty Lab plans to investigate how they might change the booster shot regimen to make the HIV vaccine even more effective. “It was incredible to get those results, but of course we’d like to see a response in 100 percent of the animals,” says Madden.
Importantly, the antibodies found in the animal subjects resembled the exact kinds of broadly neutralising antibodies seen in those rare humans who made their own neutralising antibodies. It’s clear that our immune systems can make these powerful antibodies, given the right training.
“We believe this vaccine approach is even more likely to succeed in humans, because of the immunogenetics,” Crotty says.
The priming immunogen used in this study was evaluated in humans in the HVTN 144 trial and is currently being tested in the Phase 1 trial IAVI G004. IAVI, Scripps Research, the HIV Vaccine Trials Network, and partners are now advancing plans to further evaluate the full immunisation regimen in a future human clinical study.
Lenacapavir is injected just under the skin, typically in the stomach area, where it forms a small depot that very slowly releases the drug over time. Photo by Elen Sher on Unsplash
By Amy Green
With a new six-monthly injection, South Africa last week launched the most promising new HIV prevention tool in years, but much of the infrastructure that made HIV prevention services accessible to high-risk groups has been dismantled over the last year. Spotlight asks whether we can successfully deliver this breakthrough technology without the trusted pathways decimated by cuts to aid from the United States.
When 29-year-old Keegan Daniels* visited a public hospital outside Cape Town earlier this year to be placed on medication to prevent HIV infection, he says he wasn’t sure what to expect, but it definitely wasn’t to be reprimanded, lectured and told that anal sex “is abnormal”.
Oral pre-exposure prophylaxis (oral PrEP) refers to antiretroviral tablets taken to prevent HIV infection. When used as prescribed, oral PrEP has been shown to reduce the risk of HIV infection from sex, including in men who have sex with men (MSM), by approximately 99%, according to a 2022 meta-analysis.
During the short consultation, Keegan claims the doctor, who appeared unfamiliar with prescribing PrEP, chastised him for addressing him as “sir” rather than “doctor”, and made assumptions about his sexual orientation.
“I am gay, but when he told me I was ‘homosexual’ instead of asking me, I felt as if I was there to be shamed instead of helped,” says Keegan, who identifies as a gay man.
Keegan tells Spotlight that he sought out oral PrEP after an experience that left him worried about his HIV risk. As a man who has sex with other men, he is also part of a population disproportionately affected by HIV. According to the World Health Organisation (WHO), men who have sex with one another are up to 26 times more likely to acquire HIV than the general population. This is largely driven by biological risk factors associated with anal sex combined with other social and structural vulnerabilities faced by this group.
The consultation became increasingly uncomfortable, Keegan says, when the doctor began discussing the importance of marriage as a method to prevent HIV and the risks associated with anal sex.
“He may not have meant it that way, but it felt like a judgement,” Keegan says.
His experience highlights long-standing concerns from activists, researchers and healthcare providers about discrimination experienced by members of marginal groups at public sector clinics. One solution to such discrimination has been to create special clinics for groups like men who have sex with men where they could access HIV treatment, prevention, and other services without judgment. But this alternative was dealt a major blow last year with the closure of many such specialised programmes funded through the United States President’s Emergency Plan for AIDS Relief (PEPFAR).
There are now concerns that the destruction of such specialised services could limit the reach and impact of the latest addition to South Africa’s HIV prevention toolkit. Last Friday, South Africa officially launched its public sector rollout of an injection that provides six months of protection against HIV infection at a time. The jab, a form of injectable PrEP, contains the antiretroviral drug lenacapavir. (See Spotlight’s special briefing on lenacapavir for more detail.)
PrEP in South Africa
The recent history is worth revisiting. South Africa became the first country in Africa to start rolling out oral PrEP back in 2016. Initially, the strategic focus of the programme was on “key populations”, groups that bear a disproportionate burden of HIV infection and who are at the highest risk of new infections. Key populations include sex workers, men who have sex with men, transgender persons, people who inject drugs and people in prisons or other similarly closed settings.
UNAIDS estimates that in Sub-Saharan Africa, key populations and their sexual partners accounted for roughly 39% of new HIV infections in 2020, despite representing a much smaller proportion of the population.
“PrEP is central to South Africa’s HIV response because treatment alone will not end the epidemic,” says National Department of Health spokesperson Foster Mohale.
“South Africa still has a very large HIV burden, with millions living with HIV and substantial ongoing new infections, especially among adolescent girls and young women, key populations, and pregnant and postpartum women,” he adds.
“After a decade, South Africa is home to the largest and most successful PrEP programme in the world, even though it has not delivered the impact we wanted,” says Mitchell Warren. He is the executive director of AVAC, a US-based advocacy organisation, largely focussed on HIV prevention, that does extensive work in South Africa. Warren’s point about the impact not being what we wanted, refers to the fact that, comparatively large as our PrEP programme is, uptake has been much lower than what was hoped.
He says that the oral PrEP programme started to gain more traction around the time of the COVID-19 pandemic. “A lot of that was thanks to PEPFAR, through the support around programmatic delivery of PrEP and most notably the initiatives designed for key populations,” Warren says.
Making sense of the numbers
The most recent figures show that over 2.1 million individuals have been initiated on oral PrEP in South Africa, Mohale tells Spotlight.
However, most of these are considered to be people restarting PrEP and not new users, according to Professor Francois Venter, Executive Director of Ezintsha at Wits. He says that the real figure for overall PrEP users is closer to 500 000.
This view is roughly in line with estimates from Thembisa, the leading mathematical model of HIV in South Africa. The two types of indicators here are important to distinguish. Since many people start and then stop taking PrEP, looking just at PrEP initiations provides a very limited view. This is why Thembisa also includes estimates of the total number of people taking PrEP at specific points in time (technically the middle of each calendar year).
According to Thembisa, just over 350 000 people were taking PrEP as of mid-2025 – a slight decline compared to the 2024 number. Prior to this decline, the programme had been showing solid year-on-year growth.
Aid setback
When trying to understand why PrEP numbers stopped growing, and instead declined slightly in 2025, one very likely culprit stands out – aid cuts.
Venter argues that the relative success of South Africa’s PrEP programme was underpinned by an ecosystem of specialised key population services, most of which were funded by the United States Agency for International Development (USAID) under PEPFAR.
“Most of these 500 000 estimated PrEP users in South Africa started in these key populations programmes,” says Venter.
“But one sudden decision by the Trump administration essentially destroyed PrEP in South Africa, and because South Africa is so significant in terms of HIV incidence and prevalence, it also threw the global PrEP response into chaos.”
In February 2025, the Trump administration terminated large numbers of USAID-funded health projects and massively reduced funding for many HIV programmes. While a limited waiver allowed some treatment services to continue, HIV prevention activities were largely excluded. Programmes focussed on helping people avoid HIV infection, including many PrEP services, were among the hardest hit.
The cuts all but decimated specialised clinics and services for key populations in the country, according to Venter.
“The dismantling of the key population programme is an absolute disaster for PrEP. Clinics gone, just shut down. About 80% of the specialised key population services were funded by USAID,” says Venter.
Despite the health department’s assurances that these PrEP users from key populations will be integrated into the normal existing services in our healthcare system, he says “there is absolutely no evidence that this has happened”. Venter adds: “I suspect the vast majority stopped taking PrEP.”
Over 8 000 PEPFAR-funded staff involved in HIV programmes lost their jobs, important HIV prevention research projects were halted, civil society organisations were forced to retrench staff and attenuate their outreach programmes and, most alarmingly, thousands of PrEP users were lost in the system, according to Eugene van Rooyen, who is the Legal and Policy Advisor for the Sex Workers Education and Advocacy Taskforce (SWEAT).
“It is impossible to know exactly how many of these clients stopped taking PrEP. We did a survey late last year [2025] that showed that less than half of the former users of key populations services in Cape Town were still on treatment,” he says.
The SWEAT survey aimed to find out what happened to these individuals after the services stopped but did not disaggregate PrEP users from people on antiretroviral treatment.
“Regardless, the results are a tragedy. All those years of gaining trust in these communities, and all the millions invested in the PrEP programme, all down the drain,” Van Rooyen says.
The concerns raised by activists are echoed in findings from Ritshidze, South Africa’s largest community-led monitoring programme. Ritshidze, which surveys thousands of public healthcare users annually and monitors more than 400 healthcare facilities across the country, was established to track the quality of HIV and TB services from the perspective of people using them.
Its most recent report found early signs that the PEPFAR funding cuts may already be affecting access to HIV services. Approximately, 56% (189 out of 340) of facility staff surveyed reported reduced capacity after the PEPFAR withdrawal while reports of stigma and discrimination remained common.
Vertical services vs integration
While Keegan says he experienced stigma and challenges accessing PrEP through the general public sector, his older cousin Jason* describes an entirely different experience when he first started PrEP.
“I started PrEP three years ago at the Wits RHI Transgender Clinic in Bellville [Cape Town], it was easy, comfortable, safe. I felt empowered and had zero problems getting onto PrEP there,” says Jason, who is also a part of the MSM community. Although he doesn’t identify as a transgender person, he says the clinic staff welcomed him and his peers. It was a space that removed many of the barriers key populations face when accessing healthcare. But it was also one of the many clinics that ceased to exist after the funding cuts.
The National Department of Health maintains that “the PrEP programme has not collapsed, because it is anchored in the public health system”. Their argument has broadly been that people who went to specialist clinics should be redirected to public sector clinics. To address discrimination, provincial health departments have run several programmes aimed at sensitising clinic staff to the needs of key populations. This has included staff involved in administering the lenacapavir injection.
As for PrEP, Mohale says South Africa made “a deliberate decision to move PrEP out of the early pilots that commenced in 2016 into the broader public health system at scale”. Today, he says, “approximately 99% of public primary healthcare facilities offer oral PrEP”.
“The key success factor is that PrEP is not a vertical programme, it is integrated into primary healthcare and combination prevention,” says Mohale.
What all this means for lenacapavir
“This is not merely a medical advance. It is a practical intervention that can transform lives. It reduces barriers to adherence. It expands choice. It strengthens dignity. And it empowers people to take control of their health and their future,” President Cyril Ramaphosa said in a prepared speech at the launch of South Africa’s lenacapavir rollout last Friday.
The first phase of the rollout will see lenacapavir available in 360 health facilities across the country. This is roughly 10% of the country’s public sector clinics. While it remains to be seen how high demand will be, there are clearly limits to what level of demand can be accommodated. Initially, South Africa will only have enough lenacapavir for around half-a-million people. This is partly why specific groups like young women and girls, MSM, and sex workers are being prioritised.
Thus, in the fact that there is some prioritisation of specific groups the lenacapavir rollout partially mirrors the rollout of oral PrEP a decade ago. But unlike the initial oral PrEP rollout, specialised key population clinics will play little part.
Mohale explains that the integration of services is the philosophy underlining the rollout of the lenacapavir programme, a philosophy he says is fundamental to the success of PrEP in South Africa.
Venter disagrees: “Key population programmes exist for a reason – they work. People need verticalised services.”
Meanwhile, a statement released by a coalition of several civil society groups criticised the rollout plan of being “unambitious, low-scale, and in danger of being more about pomp than public health impact”.
“A programme that does not adequately prioritise key and vulnerable populations such as sex workers, outside of clinics, will leave those most in need of HIV prevention services, even more vulnerable,” Katlego Rasebitse, from SISONKE Movement, says in the statement.
A rollout beyond clinics?
The introduction of lenacapavir has mostly been received with resounding optimism. But some have also raised concerns and have cautioned that the rollout won’t be without obstacles.
“Getting hundreds of thousands of otherwise healthy individuals to come to public health facilities to get lenacapavir is not a likely pathway to scale. We have got to be very clear, dropping lenacapavir into clinics is not a pathway to success,” says Warren, who has also praised South Africa and the National Department of Health for launching the national injectable PrEP programme.
“There are many innovative ways to deliver PrEP outside of facilities, like mobile clinics, outreach services, among others. There is a lot of work around implementation science being done in South Africa that can be used to make this programme ambitious enough to be a global PrEP success story,” he says.
There are several implementation science research projects underway looking at innovative ways of delivering PrEP, including lenacapavir, outside of traditional settings.
Unitaid has launched a project, valued at US$22.5 million, that “will support South Africa to expand access to lenacapavir through innovative, community-based delivery and demand-generation approaches that complement national rollout through public health facilities”.
Largely focussed on reaching key populations, the project aims to generate real-word evidence on these innovative delivery models, evidence that “will help inform national scale-up”. It is exploring a range of delivery settings including pharmacies, mobile clinics and even hair salons.
‘I was trying to do the right thing’
When Keegan walked out of the doctor’s consultation room that day in April, he says that he felt angry, self-conscious and deeply uncomfortable. Instead of continuing the process to get onto PrEP, he left the hospital.
“I have been through a lot of trauma in my life, a lot of stigma because of my orientation. It took a lot for me to start healing. This experience brought me back to that space of self-doubt. I left there feeling like I’m nothing. I’m a piece of dirt,” he says.
His cousin, Jason, had an appointment the next day, at the same place for the same reason. Since the closure of the clinic in Belville, Jason had chosen to pay for his monthly PrEP pills himself, instead of facing the challenges anticipated in a regular public health facility, but he says this route had stopped being financially feasible.
“By that time, I had cooled down and Jason convinced me to go back to the hospital with him,” says Keegan.
After the mandatory blood draws and HIV testing, he filled his prescription at the hospital pharmacy.
As Keegan sat down, he says he showed Jason the box.
“That isn’t PrEP Keegan, those are pills for HIV positive people,” said Jason. He had experience with oral PrEP and recognised the ARVs by the packaging. His partner, living with HIV, uses the same medication.
After a protracted process, several conversations with nurses and the doctor. Keegan says he eventually received the correct medication. He told Spotlight that, even though he is educated and informed, he only started PrEP “through luck”. There are many other people from marginalised groups “who probably won’t have my luck”.
“What will they do?” he asked.
“I was trying to do the right thing. The responsible thing for my health. In the end, I didn’t feel like I was doing the right thing. I felt like I was being punished.”
Despite this experience, both Keegan and Jason are excited at the prospect of the twice-yearly injectable PrEP.
“You won’t catch me coming back to this hospital, but I would find a clinic that treats people well. Even if I have to drive for hours, I would, just to have this injection every six months, instead of drinking pills every day,” Keegan says.
* Names have been changed to protect the identity of sources
Republished from Spotlight under a Creative Commons licence.
Study strongly suggests that most persistent cases of viral detection, despite ideal HIV drug therapy, are not due to virus transmission or a rebound of active disease
Colourised transmission electron micrograph of an HIV-1 virus particle (yellow/gold) budding from the plasma membrane of an infected H9 T cell (purple/green).
Antiretroviral drugs for HIV infection have enabled most people living with the virus to live long and healthy lives. However, a small portion of people experience detectable – and worrisome – traces of the virus that causes AIDS despite strict adherence to long-term treatment regimens and the absence of symptoms. New findings published in Nature Communications suggest that most cases of this phenomenon, which is called non-suppressible viraemia, are explained by defective and noninfectious copies of the virus. The research was partially supported by grants from the National Institutes of Health (NIH).
The study, which involved more than 50 people, found that while traces of HIV-1 RNA can persist in blood after optimal therapy, cases of non-suppressible viraemia are driven by HIV-1 RNA with defects in a piece of the RNA known as 5’-leader.
“From a clinical perspective, this is important because people with HIV are taught that the absolute goal of their medication is to achieve undetectable viral load and they worry,” says Francesco R. Simonetti, MBChBD, PhD, the senior study author and an assistant professor of medicine in the Division of Infectious Diseases at Johns Hopkins University School of Medicine. The new findings, says Simonetti and his team, should provide relief to many people living with HIV who fear a viral rebound or who are concerned about transmitting the virus to partners despite taking effective treatment.
For the study, the investigators examined blood samples from 52 people living with HIV who had detectable loads of the virus despite taking long-term antiretroviral drug therapy.
These samples, which were assessed from 32 people and compared to an additional 20 samples, were collected between 2021 and 2025. The majority of participants were white men, between ages 58 and 68, and received care in the U.S., Canada and Denmark. The researchers found that most detectable forms of the virus, around 95%, were due to defective copies, and most defects were due to mutations or deletions in the 5’-leader region of HIV-1 RNA. This region is known to orchestrate the production of copies of the virus, but in this case the defects prevented the generation of infectious virus.
Modern antiretroviral therapies, which date back to 1996, prevent HIV from infecting new populations of immune system cells, but aren’t able to retroactively prevent previously infected cells from releasing HIV viral particles. Since those cells usually represent a small portion of infected cells after a person is on stable therapy, most people who take antiretroviral therapies are able to bring their viral loads to clinically undetectable levels in their blood.
However, in some cases, which are estimated to occur less than 1% of the time, people may experience clinically detectable levels after taking long-term antiretroviral drug therapy. This could happen years later, or, in less frequent cases, they may have never achieved undetectable levels.
This new study offers evidence that clinicians can now study the virus in blood plasma and confirm if clinically detectable levels are due to defective copies released from one or a few T-cell clones, says Simonetti. If so, he adds, this could eliminate the need for extra medications and could prevent related complications. It could also help people living with HIV have access to surgeries or other procedures, such as hip or knee replacements or organ transplants, and participate in clinical studies if they know they have HIV under control.
The assay taht the researchers created and used to confirm the defective copies of the virus for this study is cost-effective and can be broadly used in HIV clinics and research settings. Similar to using a liquid biopsy to detect cancer mutations in DNA, the assay, which is called CLAWS (Capturing 5′ Leader Anomalies Without Sequencing), uses advanced technology to identify detectable viral loads that are due to defective copies.
“We know that these defective proviruses cannot infect new cells, but they are still clinically relevant,” says Simonetti. “Think of how many extra visits, extra drugs, extra costs and tests they’ve been causing.”
“It’s also clear from the new study that, over time on treatment, intact proviruses that make virus are pruned away, while defective ones escape the immune system,” he says. “Now we want to understand these differences in immune recognition to uncover HIV’s vulnerabilities.”
The long-acting HIV prevention injection, lenacapavir, will become available to around half a million people in South Africa. Photo by Anna Shvets
By Marcus Low and Elri Voigt
On June 5, 2026, an HIV prevention injection will for the first time become available at some of South Africa’s public sector clinics. In this Spotlight special briefing, we pull together all you need to know about this “breakthrough” jab.
We’ve come a long way from the worst days of South Africa’s HIV epidemic, but the virus still claims over 50 000 lives per year and, even in 2026, annual new infections remain stubbornly high at over 140 000.
Reducing the rate of new infections is not an easy task. The most effective measure is to make as many as possible of the roughly eight million people who are living with the disease non-infectious. The good news is that most people with HIV become non-infectious once they are stable on antiretroviral treatment. The bad news is that the growth of South Africa’s HIV treatment programme has slowed. The pool of infectious people thus seems set to remain relatively large.
For people who are not living with HIV, the most effective form of protection over the years have been the correct use of condoms. Condoms also have the benefit that they protect against other sexually transmitted infections.
But condoms aren’t the only game in town. Voluntary medical male circumcision substantially decreases men’s risk of contracting HIV, something that also provides indirect protection for women.
And then there are antiretrovirals (ARVs) taken to prevent HIV infection. Landmark studies published in the 2010s showed that taking a tablet that contains the antiretroviral medicines tenofovir and emtricitabine could reduce someone’s risk of contracting HIV to near zero. Such tablets are commonly referred to as oral pre-exposure prophylaxis, or oral PrEP. For several years now, these HIV prevention tablets have been widely available in South Africa’s public healthcare system, although uptake has been somewhat muted. Modelling work from Thembisa, the country’s leading mathematical model on HIV and TB, suggests that only a few hundred thousand people are taking the tablets.
The long-acting revolution
One challenge with HIV prevention pills is that not everyone can, or wants to, take them every day. For some, taking ARVs, or being seen to take ARVs, still comes with an accompanying dose of stigma. For others, remembering to take a pill every day can be tricky. Ultimately, the incentives for healthy people without HIV to take prevention medicines simply aren’t as compelling and immediate as they are for people who already have the virus in their bodies.
As in some other areas of medicine, one solution to this treatment adherence challenge is simply to make it more convenient to take the treatment. Many women, for example, prefer three-monthly contraceptive injections or three-yearly implants to a regular pill. There is some evidence that similar preferences apply to HIV prevention medicines.
So-called long-acting therapies does what the name suggests – act over longer than standard periods. They could take many forms, from slow-release tablets to injections that leave a depot under the skin that slowly releases drugs into the blood stream, to small implantable devices that are typically left in the arm for several years.
The first long-acting HIV prevention option to take the world by storm was an injection. It made headlines in 2020 when a pivotal study found it to be more effective than the daily prevention pills – the difference being largely due to better adherence, rather than differences in the ARVs used. This jab, containing the antiretroviral drug cabotegravir, provides two months of protection against HIV infection at a time.
Two years later, the World Health Organization recommended the jab, called CAB-LA, for HIV prevention, and it was registered for use in South Africa. Rollout beyond an implementation science setting stalled however when the prices the drug’s manufacturer ViiV Healthcare was willing to sell it for were deemed unaffordable by the South African government.
Fortunately, a new prevention jab that provides protection for three times as long as CAB-LA was on the way. In 2024, two large studies, found an injection of the antiretroviral drug lenacapavir given every six months was almost 100% effective in preventing HIV infection. These findings would later be hailed as the journal Science’s 2024 scientific breakthrough of the year. It is this “breakthrough” that is being rolled out in South Africa from June 2026.
Two often-neglected groups in HIV research, adolescents (aged 16 and 17), and women who become pregnant while in a study, were included in clinical trials of lenacapavir. The jab was found to be safe in both populations, which means it can now be offered to adolescents and pregnant women in the South African rollout.
Lenacapavir is injected just under the skin, typically in the stomach area, where it forms a small depot that very slowly releases the drug over time. These depots can form small lumps under the skin. Though harmless and usually not visible, it will be important that people getting the jab know to expect these “subcutaneous nodules”. The other most common side effects seen in the two pivotal studies were pain at the injection site and a skin rash. These reactions and the size of the nodules appear to decrease with subsequent injections.
Prior to their first injection, people will first have to get an HIV test to ensure they aren’t already living with HIV. This is important since treating someone with HIV with just lenacapavir could result in the development of drug resistance. Together with the injection, people starting lenacapavir will also have to take some lenacapavir tablets for two days. Since the depot releases the injected drug very slowly, these tablets are needed to get the drug levels in the body up more quickly so that it can provide full protection as soon as possible. (The Department of Health has published a guideline document setting out how it should all work at the clinic.)
In addition to the lenacapavir and CAB-LA jabs, there is also a long-acting vaginal ring that contains the ARV dapivirine. The ring provides one-month of protection at a time, with a three-month version also under development. The available evidence however suggests that the dapivirine vaginal ring is not as effective at preventing HIV infection as oral PrEP or the two injectable options.
The long road to jabs at clinics
Having the scientific evidence that an injection works is of course only one step in that jab’s long journey to the point where people can get it at clinics. An essential next step was regulatory approval, which lenacapavir received from the South African Health Products Regulatory Authority in October 2025. After regulatory approval was secured, the next question became whether a sufficient supply of the product can be procured in South Africa on acceptable terms.
Lenacapavir is currently only being produced and marketed by the pharmaceutical company Gilead Sciences, who holds the critical patents on the product. In the US, lenacapavir is sold for around $28 000 per person per year. The Global Fund (the world’s largest multilateral funder of health in low- and middle-income countries) and PEPFAR (the United States President’s Emergency Plan for AIDS Relief) are however procuring limited stocks of lenacapavir at a lower price for use in some low- and middle-income countries. It is some of these Global Fund-procured jabs that will be used in the first phases of the lenacapavir rollout in South Africa.
For now, largely due to the limited stocks, the local rollout will target only around half a million people at 360 clinics in areas with high HIV rates, but the plan is to scale-up considerably in the next few years.
The South African government will likely start buying lenacapavir from generic manufacturers in 2027 or 2028. Gilead has so far issued licenses that will allow six different companies to produce lenacapavir and to sell it in 120 different countries, including South Africa.
The Gates Foundation and a partnership including UNITAID, the Clinton Health Access Initiative, and Wits RHI, have concluded separate deals with generic manufacturers that should see these generics sold for a price of no more than $40 (under R800) per person per year. This is lower than what government currently pays for oral PrEP and modelling work suggests it would be affordable for the South African government. Barring any unforeseen hiccups, the pieces are thus in place to facilitate widespread access to lenacapavir in South Africa in the coming years.
For now, none of the generic versions of lenacapavir will be produced in South Africa. Negotiations are however under way that may eventually see a local company licensed to produce the jab. Such local production is seen as important for ensuring security of supply, although it is not clear that local companies will be able to compete with Indian generic drug-makers on price.
At the time of writing, neither the lenacapavir or CAB-LA injections can be purchased at private sector pharmacies in South Africa. Oral PrEP can be purchased for around R300 for a month’s supply. The monthly dapivirine vaginal ring should cost in the region of R500 per ring. (These prices are based on the 30 April 2026 Single Exit Price database published by the health department.)
How many people will want the jabs?
One of the big unanswered questions about lenacapavir is how many people will come forward to get the jabs. We are hopeful that the Department of Health will routinely provide detailed numbers on uptake in the coming months and years.
The initial rollout is largely clinic-based, but researchers will also be assessing how well distribution works through mobile clinics. We need not stop there of course. At the height of the COVID-19 pandemic, public sector users could access SARS-CoV-2 vaccines from nurses at private sector pharmacies. With sufficient political will, the same could be done with lenacapavir. No doubt some young people will rather get their jab at the mall than at the clinic.
Those in control of the rollout will have to think carefully about how they promote and provide the jab. At its core, it is an empowering tool that can help people stay HIV-free, but as often is the case with HIV-linked products, there is a risk of stigma. In addition, even though lenacapavir is not a vaccine, some vaccine scepticism might well transfer over to lenacapavir since it is administered as an injection. As with any large healthcare intervention, one will not have to look far to find lenacapavir-related misinformation on social media.
Either way, just having the jab at clinics and hoping people will come get it might not be good enough if we’re hoping to see good uptake. Fortunately, we have several research groups and NGOs in South Africa who have world-class expertise on just this type of issue. Hopefully government will draw on this unique reservoir as they adjust and shape the lenacapavir rollout.
So what’s next
The rollout of the lenacapavir jab in South Africa will not be the end of our HIV prevention story. Two promising products in the pipeline are a new formulation of lenacapavir that looks like it could provide a full year of protection per shot and a pill containing another antiretroviral that could provide a month of protection at a time. We are keeping a close eye on the ongoing development of these products. There are also still hopes that an effective HIV cure or vaccine might one day be developed, although this is a much longer shot than better long-acting antiretroviral formulations.
In the meantime, though, twice-yearly lenacapavir is rightly dominating the headlines.
Modelling suggests that over the next 20 years, an ambitious lenacapavir rollout could reduce new HIV infections by around 20% to 30%. There can be little doubt that, like condoms and antiretroviral treatment for people living with HIV, providing lenacapavir at scale makes public health sense.
But thinking of lenacapavir mainly in terms of cost-effectiveness and public health benefits risks obscuring its more immediate and transformative human potential. For many people, especially young women, a discreet and convenient form of HIV prevention that they can control may well make the difference between contracting HIV or not.
As experts often point out, when it comes to products that can prevent HIV, choice – as in the world of contraception – is key. Some products will work for one person, but not for others. As circumstances change, a product that might have once worked may no longer be the best option. Having more than one product in the “toolkit of prevention” makes it easier to find what actually works in people’s lives.
For years, the HIV world has been flush with rhetoric about empowering young women – a group that is profoundly affected by HIV. An ambitious lenacapavir rollout might be the most concrete realisation of those ideals yet. We simply have to get it right.
Disclosure: The Gates Foundation is mentioned in this article. Spotlight receives funding from the Gates Foundation, but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council.
Colourised transmission electron micrograph of an HIV-1 virus particle (yellow/gold) budding from the plasma membrane of an infected H9 T cell (purple/green).
Researchers at Karolinska Institutet, in collaboration with colleagues at The Scripps Research Institute and Emory University, have developed a new vaccine strategy that has generated antibodies capable of neutralising highly divergent HIV variants. The study, published in the journal Nature, provides new insights into how the immune system can be guided towards a particularly protected part of the virus.
HIV mutates rapidly, making it difficult to develop an effective vaccine. One major challenge has been to stimulate the immune system to produce so‑called broadly neutralising antibodies that recognise parts of the virus shared by many HIV variants.
In the study, the researchers focused on a small structure located at the very top of the virus’s surface protein, known as the apex, which is important for the protein’s three-dimensional structure. The apex is similar across many HIV variants but is shielded by dense layers of sugar molecules, making such binding difficult to achieve.
“We developed a strategy in which specially designed HIV proteins were attached to tiny fat particles, known as liposomes. This enabled multiple copies of the virus’s surface protein to be presented to the immune system simultaneously, thereby strengthening the immune response”, says Mónika Ádori, researcher at Department of Microbiology, Tumor and Cell Biology, Karolinska Institutet.
The vaccine strategy was tested in an animal model in which macaques were immunised with liposomes linked to a selected HIV protein and then given booster doses in which the protein was gradually altered. The aim was to train the immune system to recognise features that are shared across different HIV variants.
Resembles antibodies that develop in humans
With this strategy, all vaccinated animals developed antibodies that neutralised a wide range of HIV variants. When the researchers analysed the antibodies in more detail, they found that they bind to the virus’s apex in a way similar to antibodies that sometimes develop in humans after long‑term HIV infection.
“The study shows that it is possible, through vaccination, to steer the immune system towards this specific part of the HIV surface protein,” says Gunilla Karlsson Hedestam, professor at the Department of Microbiology, Tumour and Cell Biology at Karolinska Institutet and a shared senior author of the study.
“This is an important step towards understanding how an HIV vaccine could be designed. Discussions are now underway about how the strategy could be taken forward into clinical studies,” she continues.
The study was funded by the US National Institutes of Health (NIH). The researchers report no conflicts of interest.
Publication
”Vaccine generates broadly cross-neautralizing antibodies to the HIV Env apex“, Javier Guenaga, Monika Adori, Shridhar Bale, Swastik Phulera, Ioannis Zygouras, Fabian-Alexander Schleich, Xaquin Castro Dopico, Sashank Agrawal, Miyo Ota, Richard Wilson, Jocelyn Cluff, Tamar Dzvelaia, Marco Mandolesi, Wen-Hsin Lee, Agnes A. Walsh, Mariane B. Melo, Laurent Verkoczy, Darrell J. Irvine, Martin Corcoran, Ian A. Wilson, Diane Carnathan, Guido Silvestri, Andrew B. Ward, Gabriel Ozorowski, Gunilla B. Karlsson Hedestam, Richard T. Wyatt, Nature, online 29 April, doi: 10.1038/s41586-026-10429-3