Epstein–Barr Virus Influences Rare Brain Lymphomas
Primary CNS lymphomas in immunocompromised patients are among the rarest and at the same time most aggressive cancers – yet evidence-based recommendations for diagnosis and treatment have been lacking. An international research team led by Heidelberg Faculty of Medicine at Heidelberg University and the German Cancer Research Center has now identified characteristic imaging features of these tumours and developed a prognostic model to better assess disease outcomes. The researchers found that tumours positive for Epstein-Barr virus were associated with particularly poor prognosis. The findings, published in the journal Blood, may help guide future diagnostic and treatment strategies.
Primary CNS lymphoma is a rare cancer that arises from malignant white blood cells. Affected individuals develop tumours in the brain and, more rarely in the spinal cord, the eyes, or within the cerebrospinal fluid. These lymphomas can occur in people with weakened immune systems, for example after organ transplantation, in autoimmune diseases, or in association with HIV infection. This subtype, known as immunodeficiency-associated primary CNS lymphoma (ID-PCNSL) affects approximately 50 people per year in Germany. Researchers at the Heidelberg Faculty of Medicine at Heidelberg University had already shown in earlier work that ID-PCNSL is not simply a variant of classical CNS lymphoma, but a distinct disease entity characterised by specific genetic alterations.
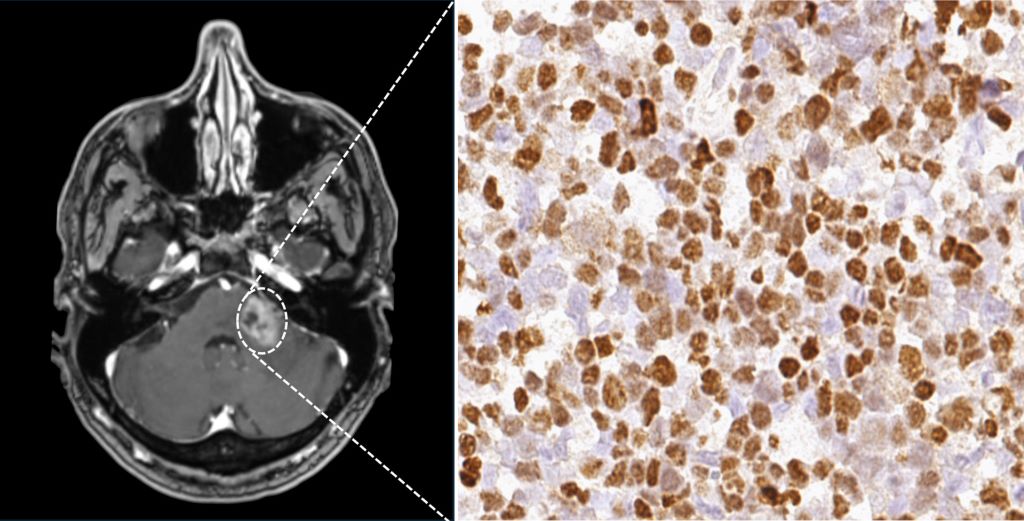
A recent study by the International Primary CNS Lymphoma Collaborative Group – an international network dedicated to the study of CNS lymphomas – has now provided further insights into the diagnosis and treatment of ID-PCNSL. Including data from 308 patients treated at 23 hospitals across seven countries, the study is the largest conducted to date on this rare cancer. The researchers analysed clinical findings, magnetic resonance imaging scans, and tumour tissue samples. Scientists from the Heidelberg Faculty of Medicine at Heidelberg University and the German Cancer Research Center (DKFZ) played a leading role in the study.
Epstein-Barr Virus influences imaging and prognosis
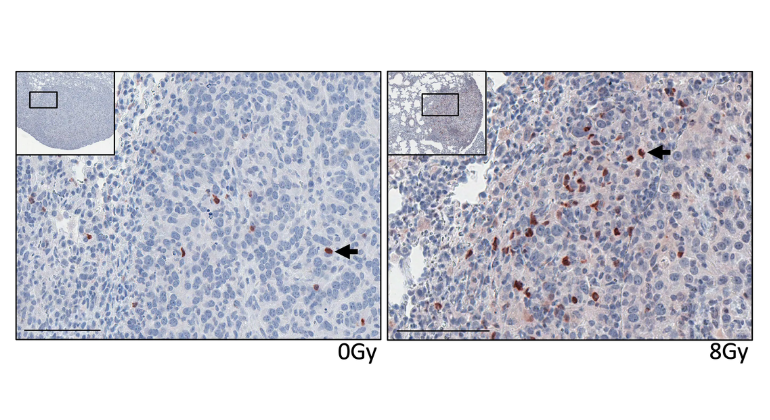
Epstein-Barr virus (EBV) is known to play a central role in this cancer and was detected in 79.2 percent of the tumours examined. “Our analyses show that EBV-positive tumours often follow a more aggressive course and are associated with an unfavourable prognosis,” says first author Dr Leon Kaulen. He conducts research at the Heidelberg Faculty of Medicine at Heidelberg University and at the DKFZ and is a physician at the Department of Neurology at Heidelberg University Hospital (UKHD). EBV-positive tumours also showed characteristic imaging features including different patterns of contrast enhancement compared with EBV-negative tumours.
The researchers developed a prognostic model based on three factors that can help to better predict the course of ID-PCNSL and patient survival more accurately. The three identified factors are the detection of EBV in tumour tissue, age, and the patient’s performance status. Depending on the combination of these three factors, disease courses differed markedly among the patients studied. If only one of the three risk factors was present, the median survival was 135 months. With two risk factors, it decreased to 29 months. If all three factors were present, median survival was reduced to three months. “The prognostic model, with its clear stratification, represents a major advance. It will enable us to assess patients much more precisely in the future and to tailor therapies more effectively to the individual clinical situation,” says senior author Professor Wolfgang Wick, Heidelberg Faculty of Medicine at Heidelberg University, Chair of the Department of Neurology at UKHD, and Head of the Clinical Cooperation Unit Neurooncology at DKFZ and UKHD.
Considering immunodeficiency and cancer together
So far, no standardised therapy has been established for patients with immunodeficiency-associated primary CNS lymphoma. “Our research provides important insights into which approaches may be associated with more favourable outcomes,” says Dr Leon Kaulen. Patients whose immune system could at least partially be reconstituted – for example through adjustment of immunosuppressive medication or effective treatment of HIV infection – and who additionally received combination chemotherapy with rituximab and methotrexate typically (85 percent) responded well to treatment. In a substantial proportion of patients, the disease also remained stable in the long term and became undetectable.“ Our data suggest that the interplay between the tumour and the weakened immune system plays a central role,” says Dr Kaulen. “Both aspects should therefore be addressed together in treatment.”
“With the current study, a robust evidence base for this rare disease is now available for the first time,” summarises Professor Wick. “This represents an important step toward precision medicine even in rare diseases. Relevant research in rare tumour entities can often only be carried out in large international consortia. International scientific collaboration therefore deserves particular attention.”
Source: Heidelberg University