
Bariatric Surgery Increases the Risk of Alcohol Problems

The body absorbs alcohol much more rapidly after bariatric surgery, researchers from Norway have found. Patients need to know this when they choose the kind of surgery they will have.
“Bariatric surgery can come with a price. Patients have a significantly higher risk of developing alcohol problems than if they did not undergo surgery,” said Magnus Strømmen, a researcher at the Centre for Obesity Research at St. Olavs Hospital and a PhD research fellow at the Norwegian University of Science and Technology (NTNU).
Between one and two per cent of the population in Norway has undergone bariatric surgery. The most commonly used surgical methods are gastric bypass and gastric sleeve.
Both methods make patients eat less and feel full faster. This is partly due to reduced volume on the stomach, and partly due to hormonal changes. But a person’s changed anatomy also has consequences for what happens when they drink alcohol.
“In a normal stomach, a significant part of the alcohol will be broken down and thus not pass into the bloodstream. This is due to an enzyme that is secreted in the lining of the stomach. It is this protective mechanism that we deprive the patient of when we operate on the stomach. In addition, what you drink passes much faster into the intestine,” says Strømmen.
The small intestine’s big job is absorption. Since the stomach’s ability to break down alcohol more or less stops, significantly more alcohol passes directly into the bloodstream. That’s true even if the patient drinks the same as before the operation.
You get drunk faster
In a new study, Strømmen and his colleagues have had 33 adult patients undergo stress tests with alcohol. The participants consumed measured amounts of vodka mixed with orange juice both before bariatric surgery, and 3, 12 and 36 months after the operation, after which they had their blood alcohol levels measured after they had consumed the alcohol.
“Our findings show that alcohol uptake almost doubles, both after gastric bypass and gastric sleeve. Perhaps an even more dangerous finding, from a substance-abuse perspective, is that patients reach the maximum blood concentration in only half the time. These effects are lasting, probably lifelong,” Strømmen said.
In other words: The patients were intoxicated faster, and to a much greater extent, by the same amount of alcohol, and it took longer to get sober.
“The effects were more pronounced for people who had gastric bypass surgery. But that does not mean that the sleeve operation is harmless in terms of subsequent alcohol abuse,” Strømmen said.
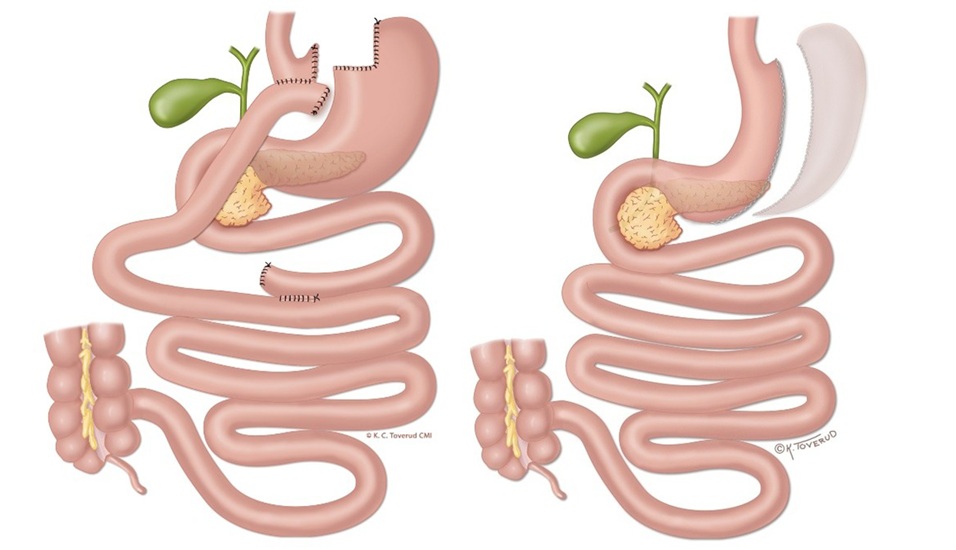
Gastric bypass (left) and gastric sleeve are the most common forms of bariatric surgery today. In gastric bypass, a corner of the stomach is connected directly to the small intestine, so that both the stomach and one meter of the small intestine are disconnected. In gastric sleeve surgery, part of the stomach is removed so that the volume is reduced, without reconnecting the intestines. Illustration: Kari C Toverud, CMI
Bypass had a 69 per cent higher risk than sleeve
In another study, the researchers compared the risk of getting an alcohol abuse diagnosis after the two bariatric surgeries. The researchers analysed data from the Norwegian Patient Registry linked to the Norwegian Prescription Database for 17,800 patients operated on in the period from 2008 to 2018.
They found that patients who had gastric bypass surgery had a 69 per cent higher risk of being diagnosed with an alcohol-related problem than patients with a gastric sleeve. Bariatric patients who were given an alcohol-related diagnosis also had a higher mortality rate and used specialist health services more than patients who underwent bariatric surgery and who did not receive an alcohol diagnosis.
“It is important that patients, their relatives and health personnel, especially in general medicine, substance abuse and gastro medicine, share this knowledge. These Norwegian studies, based on different data sources and different methodologies, indicate that some of our patients struggle with alcohol problems as a complication from the surgery. Alcohol problems can cost the patient, their relatives, and society a great deal,” Strømmen said.
He likes to tell patients that they need to practice saying no.
“They will suddenly be in social contexts where friends and surroundings expect you to drink as much as before the operation. But your physiology has changed. That means you need to be more careful than before,” he said.
Risk factors for bariatric surgery must be investigated
“We can’t just tell people what to do or not to do,” says Associate Professor Magnus Strømmen. “I believe more that patients need to be educated about the mechanisms behind it. Knowledge can motivate people to be more careful with alcohol. They need to know how altered alcohol absorption can affect their actions while under the influence and that all alcohol intake doubles the stress on their organs. Photo: Aleksander Mjøen
He himself has been involved in building up the obesity outpatient clinic at St. Olavs Hospital in Trondheim. Now he wants to be sure that clinics incorporate this new information into their daily practice. Patients must be assessed individually in relation to the risk of alcohol problems.
“We find that many patients have a clear idea of what type of surgery they want when they are referred. And for a long time, this was given very great importance in the decisionmaking. But obesity is not just a single phenotype. Despite having a large body, patients are very different, also in terms of health,” he said.
Some patients may have type 2 diabetes, others struggle with heartburn. Some may have more extensive obesity and thus desire greater weight loss.
“For a patient like this, gastric bypass may be best. Other conditions may make you want to recommend gastric sleeve. Now we know that the operations result in different risks of alcohol problems. This means we must also investigate the patient’s risk factors for substance abuse before we decide which operation the patient should have. Where patients have several risk factors, gastric sleeve may be a better alternative, but we must also ask whether high-risk patients should be operated on at all,” Strømmen said.
Patients need to know
He wants patients to receive more specific information before the operation.
“It is important that patients make their decision to undergo surgery on a genuinely informed basis. It is not enough to say that their alcohol uptake will change. Patients should be educated about the mechanisms behind increased risk after surgery, and not least how to react differently to alcohol intoxication after surgery as a result of the sudden increase. This information can at best prevent patients from developing alcohol-related problems,” he said.
The patient’s risk factors for substance abuse should be considered before the type of surgery is chosen.
“I think most obesity clinics can get much better at their alcohol history, ie, a thorough conversation about the patient’s alcohol habits and any risk factors. We need to get better at asking the right questions, and make a more precise assessment. But this also requires transparency from the patients. I believe that good patient education can make patients understand why it is important to be honest about these things,” says Strømmen.
Drugs can replace bariatric surgery
In recent years, more effective drugs have been developed against obesity. Strømmen believes these should be considered for everyone before surgery, but especially for those at increased risk of alcohol abuse.
“The current guidelines state that we should not operate on patients with an active substance abuse problem, and that high-risk patients should abstain from alcohol after surgery. However, the guidelines do not provide any guidelines for how patients should be screened. The lack of specification is a problem because this is information that many clinicians are reluctant to ask for, and which patients may be afraid to share,” he said.
By Ingebjørg Hestvik – Published 25.06.2026
References:
Strømmen, M., Dale, O., Klöckner, C. et al. Ethanol pharmacokinetics before and after sleeve gastrectomy and Roux-en-Y gastric bypass: a 3-year prospective study (the BAR-TRIAL). Int J Obes (2026).https://doi.org/10.1038/s41366-026-02113-3
Strømmen, M., Bakken, I.J., Sandvik, J. et al. Alcohol use disorders and related morbidity and mortality after sleeve gastrectomy and Roux-en-Y gastric bypass: a nation-wide registry study (the BAR-REGISTER). Int J Obes (2026). https://doi.org/10.1038/s41366-026-02123-1
Source: Norwegian SciTech News







{kind=link}
{kind=link}