Study finds the link between genetics and BMI has become stronger since the rise in obesity rates
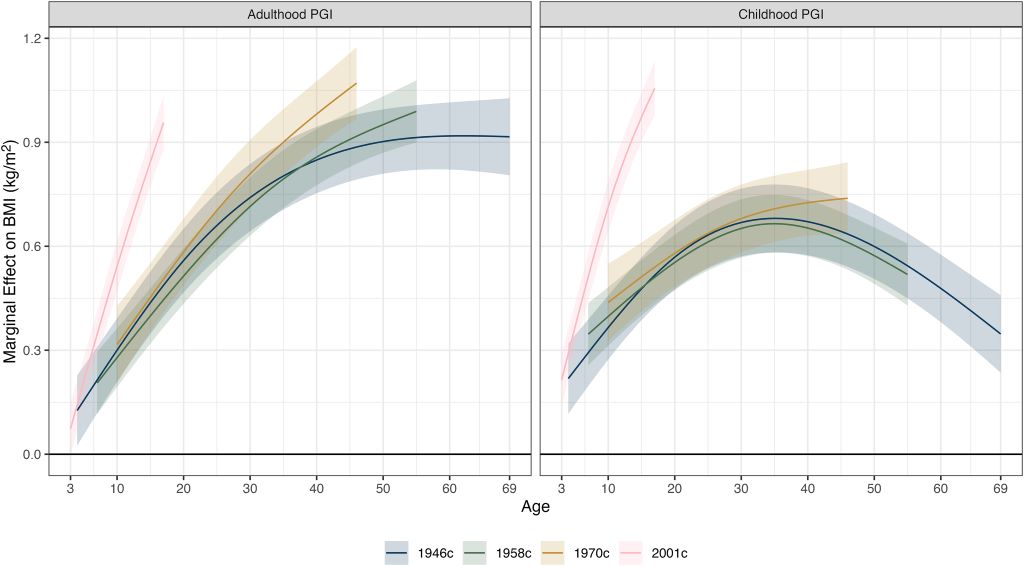
Association (+ 95% CIs) between PGI and BMI (kg/m2) by cohort, age, and PGI (adulthood or childhood). Derived from separate linear mixed effects models with the association between PGI and BMI allowed to vary by age (two natural splines). Adjustment was made for age (two natural splines), sex, first 10 genetic principal components, and a person-specific random intercept. Estimates were weighted using recruitment weights. Image Credit: Wright et al., 2026, PLOS Genetics, CC-BY 4.0
People who carry genetic variations linked to obesity are more likely to be heavier now than individuals with the same variants who were born before the recent obesity epidemic. Liam Wright of University College London, and colleagues, report these findings June 19 in the journal PLOS Genetics.
Over the past five decades, obesity rates have risen sharply for both children and adults. But strangely, rates of extreme obesity have increased faster than the overall increase in body mass index (BMI), an estimate of body fat based on a person’s height and weight. This trend suggests that some individuals are especially susceptible to environmental factors that encourage weight gain, such as the increasing availability of processed foods and decreasing amounts of physical activity. One cause of this susceptibility may be genetics.
To investigate this trend, researchers compared the BMIs and the presence or absence of multiple genetic variations previously linked to obesity in people from four British birth cohorts, born before or during the rise in obesity rates. The study included BMI data from early adolescence to adulthood for individuals born in 1946, 1958, 1970 and 2001 in Great Britain. Their analyses showed that these genetic variations were more strongly linked with having a high BMI in the two more recent cohorts, and were even more pronounced as people became older and among individuals with a higher BMI. These findings suggest that people with a genetic predisposition to having a higher BMI are likely more susceptible than others to changes in their environment that encourage obesity.
The researchers point out that the reason for the stronger association between genetics and BMI in the younger cohorts is unclear. However, they suspect that as the environment changed – with a rise in fast food restaurants and processed food – it may have enabled greater expression of genetic variants that encourage higher calorie consumption and, thus, higher BMI. They conclude that further work will be required to identify the specific environmental factors responsible for strengthening the link between genetics and BMI.
The authors add: “The obesity epidemic has increased BMI regardless of genotype, but it’s those most genetically predisposed to high BMI that have been most affected.”
Dihydropyridine calcium-channel blockers linked to poorer kidney outcomes in people with type 2 diabetes
Photo by Towfiqu Barbhuiya on Unsplash
Commonly prescribed blood pressure medications known as dihydropyridine calcium-channel blockers (DCCBs) may be associated with poorer kidney outcomes in people with Type 2 diabetes (T2D) and diabetic kidney disease (DKD), according to new research presented at the 63rd European Renal Association (ERA) Congress in Glasgow, Scotland.1
Kidney Outcomes Worse with DCCBs in T2D
The findings suggest that patients receiving DCCBs alongside current standard-of-care kidney-protective therapies face a significantly higher risk of major adverse kidney events compared with those treated with alternative antihypertensive medications.
DKD remains one of the leading causes of kidney failure worldwide and is driven by chronic damage to the kidney’s filtering system caused by prolonged hyperglycaemia.2 Effective blood pressure control is a cornerstone of management, particularly alongside renin-angiotensin system (RAS) inhibitors and sodium-glucose cotransporter-2 (SGLT2) inhibitors, which have transformed outcomes for patients by slowing kidney disease progression and reducing the risk of kidney failure.
Researchers analysed data from 31 031 adults with T2D treated between 2016 and 2021. All participants were receiving both RAS and SGLT2 inhibitors. Of these, 12 172 patients were also prescribed DCCBs, while 18 859 received alternative blood pressure therapies. Participants were followed for a median of approximately 3.5 years.
After adjusting for baseline demographic and clinical differences, DCCB use was associated with a 33% increased risk of major adverse kidney events compared with other antihypertensive treatments. The composite outcome included a decline of at least 40% in estimated glomerular filtration rate (eGFR) or progression to end-stage kidney disease requiring dialysis or kidney transplantation.
Lead author Dr Timna Agur noted that DCCBs are widely used as second-line blood pressure therapies in DKD, making the findings particularly relevant to current clinical practice. The researchers propose that the observed association may stem from the drugs’ effects on kidney haemodynamics. By preferentially dilating blood vessels entering the kidney’s filtering units, DCCBs may increase pressure within these structures, potentially contributing to ongoing damage despite concurrent kidney-protective therapies.
Blood Pressure Treatment Choice May Matter
Although the study was observational and cannot establish causality, the investigators emphasised that the results warrant further investigation. Prospective studies and randomised controlled trials will be needed to determine whether alternative blood pressure treatment strategies could offer greater kidney protection for patients with DKD.
References
Li J et al. Epidemiological status, development trends, and risk factors of disability-adjusted life years due to diabetic kidney disease: a systematic analysis of Global Burden of Disease Study 2021. Chin Med J. 2025;138(5):568-578.
Agur T et al. DCCB therapy and risk of CKD progression in type 2 diabetes on RASi and SGLT2i. Abstract 597. ERA Congress, 3-6 June 2026.
A new study published in JAMA Network Open found that removing olfactory groove meningioma, a type of brain tumour located near the base of the brain, may improve blood sugar control in patients with diabetes.
Researchers followed patients with an olfactory groove meningioma and diabetes over five years after surgery, tracking long-term changes in haemoglobin A1c (HbA1c), which is a standard measure of blood sugar control, and body weight after tumour removal surgery.
The research team found:
Blood sugar control improved after tumour removal in most patients.
Improvements often happened soon after surgery and lasted for years.
Many patients also lost weight after surgery.
Improvements occurred even when diabetes medications stayed the same.
“This type of brain tumour affects both frontal lobes simultaneously and is usually thought of as causing symptoms like vision problems, personality changes or loss of smell,” said Andrew Venteicher, MD, PhD, an associate professor at the University of Minnesota Medical School and neurosurgeon with M Health Fairview. “What surprised us was how much blood sugar control improved after surgery in many of these patients. The findings may help us better counsel patients before surgery and raise new questions about how the brain influences metabolism throughout the body.”
The findings suggest that some brain tumours may affect the body’s ability to regulate metabolism and blood sugar, and that removing certain brain tumours may improve blood sugar control and weight in some patients with diabetes, in addition to improving neurological symptoms.
Future studies will explore why these metabolic improvements occur and whether similar effects are seen in patients with other types of brain tumours. Researchers also hope to better understand how brain function, behaviour and metabolism are connected and whether these findings could help guide future treatment decisions.
New research presented at this year’s European Congress on Obesity in Istanbul, Turkey (12-15 May) shows the use of the new GLP-1 class of obesity drugs in people with asthma is associated with a 26% fall in the number of asthma exacerbations and a 14% drop in use of asthma inhaler reliever use. The study is by Simon Høj and Dr Kjell Erik Julius Håkansson Copenhagen University Hospital, Copenhagen Denmark and colleagues.
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are now widely used to treat overweight, obesity and type 2 diabetes (T2DM), with growing evidence of benefits that extend beyond blood sugar control.
In asthma, where overweight, obesity and metabolic dysfunction can lead to increased severity of symptoms and adverse events such as acute exacerbations, the authors suggest that GLP-1 RAs may improve asthma outcomes through weight loss, modulation of airway inflammation, and improvements in metabolic functions. Reductions in occurrence of asthma exacerbations are likely to reduce systemic corticosteroid exposure (a common treatment for acute asthma exacerbations orally or intravenously) and thus may reduce the risk of corticosteroid exposure-associated adverse events such as osteoporosis or new-onset T2DM. As such, as the clinical use of GLP-1 RAs expands, reliable estimates of their impact on asthma control are needed for individuals living with both asthma and overweight, obesity or T2DM.
The researchers conducted a nationwide self-controlled cohort study using linked Danish health registers. Adult individuals with a prior asthma diagnosis or ≥2 asthma inhaler prescriptions redeemed within 12 months) were included on the date of their first GLP-1 RA dispensing (index date). Eligible individuals had continuous registration data for at least 12 months before and after the index date.
Individuals with COPD or patients with severe asthma treated with new and relatively expensive biologic drugs within 12 months before or after the index date were excluded. Overweight or obesity was defined using ICD-10 codes for those conditions. Those who had no evidence of T2DM – with no diagnosis recorded or no evidence of other first line diabetes drugs prescribed – were also placed in the with obesity/overweight group. Those with a T2DM diagnosis or prescriptions recorded for first line diabetes drugs such as metformin were placed in the T2DM group.
The primary outcome was exacerbations, defined as an inpatient asthma hospital contact(s) and/or systemic oral or intravenous corticosteroid course(s). Secondary outcomes were the use of rescue medication (inhaled short-acting β2-agonists), inhaled corticosteroid exposure, and chest infection events defined as redemption of antibiotics commonly used for lower airway infections
The cohort comprised 27,523 individuals (mean age 54 years, 66% female) with asthma and comorbid overweight or obesity (49%) or T2DM (61%) and 26% recorded as having both conditions. Around 50% of the GLP-1 prescriptions were liraglutide, 48% semaglutide, and 2% others (exenatide, dulaglutide, lixisenatide).
Compared with the year before GLP-1 RA treatment, GLP-1 RA treatment was associated with a 26% lower exacerbation rate overall; and 28% lower in men compared with 23% lower in women. When stratified according to GLP1 RA treatment indication, the analysis showed individuals with asthma and comorbid overweight or obesity and individuals with asthma and comorbid T2DM had similar effect estimates – a 22% reduction in those with overweight or obesity and a 26% reduction in those with T2D.
Reliever medication use fell by 14% overall, suggesting fewer symptoms despite daily inhaled corticosteroid exposure also decreasing by 23% (inhaled corticosteroids are used to prevent exacerbations and treat symptoms in asthma). Furthermore, pneumonia events were reduced by 10%. People also living with allergic rhinitis saw similar decreases (23%) in exacerbations to those living without allergic rhinitis (28%). The authors are also working on updated analyses to show differences between men and women for these specific outcomes.
The authors conclude: “In this nationwide cohort of over 27,000 individuals with asthma and also overweight, obesity or type 2 diabetes, use of GLP-1 drugs was associated with significant reductions in exacerbation burden as well as reliever use, exposure to inhaled corticosteroids and pneumonia events, irrespective of whether the drugs were being used to treat obesity or type 2 diabetes.”
The authors explain that their study did not have access to clinical records (just if people had used GLP-1 and hospital admissions), so data on BMI and weight loss for participants were not available.
But Dr Håkansson says: “There’s a high chance that the weight loss is a major contributor to these results. A common symptom in both asthma and obesity is shortness of breath, and the presence of excess fatty tissue creates a pro-inflammatory state in the body in general. There’s also evidence from other studies suggesting that the inflammation caused by excess adipose tissue is distinct from the ‘classic’ asthma inflammation which often is driven by allergies or cells called eosinophils.”
And he adds: “As the use of GLP-1 therapies increase, researchers are finding an increasing number of effects outside of weight loss.”
New research presented at this year’s European Congress on Obesity (ECO 2026) in Istanbul, Turkey, shows that rapid weight loss (RWL) is much more effective than gradual weight loss (GWL) in both achieving higher weight loss and also sustained weight loss at one year.
There exist long‑standing beliefs suggesting that rapid weight loss (RWL) is unhealthy and that losing weight very quickly increases the likelihood of weight regain. However, these concerns are largely based on observational data, historical assumptions, or small, methodologically limited studies. Overall, the scientific evidence directly supporting these claims is limited and inconsistent, and high‑quality randomised controlled trial evidence is relatively sparse.
A recent large population-based cohort study, (Busetto et al., 2025), concluded that a body-mass index (BMI) of ≤ 27 kg/m² and a waist-to-height ratio (WHtR) of ≤ 0.53 after weight loss may represent clinically meaningful treatment targets for reducing the 10-year risk of obesity-related complications (type 2 diabetes, hypertension, atherosclerotic cardiovascular disease, and hip/knee osteoarthritis).
In this new study, the authors aimed to assess the comparative effectiveness of a rapid weight loss (RWL) program versus a gradual weight loss (GWL) program in achieving these treatment targets.
This 52-week investigator-initiated, randomised clinical trial randomised (1:1) a total of 284 adults with obesity (BMI ≥30) (257, 90% women) to either a 16-week food-based RWL-program (weeks 1–8: < 1000 kcal/day; weeks 9–12: < 1300kcal/day; weeks 13–16: < 1500kcal/day) or a 16-week food-based GWL-program (800–1000kcal/day below estimated total energy expenditure (with a mean self-reported intake in this group of approximately 1400kcal/day). Estimated energy expenditure was calculated by estimating the participants’ resting energy expenditure and adjusted based on if they had low, medium or high physical activity.
Following the initial weight loss phase, participants in both groups entered an identical 36-week weight-regain prevention programme. The interventions included weekly in-person weight-loss group sessions from week 1 to week 16, and thereafter, in-person group meetings every 14 days for the first 3 months followed by monthly meetings or individual contacts via webinars, video or telephone for the remaining 5 months of the study. In these sessions, participants were advised to increase their daily energy intake by 100–300 kcal during the first month, until weight stability was achieved. Thereafter, daily energy intake was adjusted as needed in response to any concomitant weight changes throughout the 8‑month weight‑maintenance phase. Participants were free to decide whether they wished to maintain their weight or pursue further weight loss. The majority opted for additional weight reduction following the initial 16‑week period.
The food composition in both programmes was based on current Norwegian dietary recommendations issued by the Norwegian Directorate of Health (https://www.helsedirektoratet.no/faglige-rad/kostradene-og-naeringsstoffer/kostrad-for-befolkningen). Core recommendations included consumption of healthy foods such as vegetables, fruits, whole grains, low‑fat dairy products, fish, eggs, lean meat, and other protein‑rich foods, while limiting the intake of saturated fats and added sugars.
The primary outcome was 1-year percent total body weight loss (%TBWL), and the proportions of participants achieving a BMI of ≤ 27kg/m² or a WHtR ≤ 0.53 after 1 year, were exploratory outcomes. Half of the participants were randomised to the RWL- and 142 to the GWL-programme. At baseline, in the RWL-group, the mean age was 48.5 years, body weight 102.4kg, height 169cm, BMI 35.8kg/m², waist circumference 112.5cm, and WHtR 0.67. Corresponding values in the GWL-group were 47.7 years, 103.0kg, 168cm, 36.5kg/m², 112.8cm, and 0.67.
During the initial 16 weeks, participants in the RWL-group lost significantly more body weight than those in the GWL-group, with mean %TBWL of -12.9% and -8.1%, respectively, corresponding to a between-group difference of -4.8%. At 1 year, the significant difference was maintained, with mean %TBWL of -14.4%in the RWL-group and-10.5 in the GWL-group, corresponding to a between-group difference of -3.9 percentage points. The proportion of participants achieving a BMI ≤ 27 kg/m² was significantly higher in the RWL-group than in the GWL-group at both 16 weeks (13.8% vs 0.8%) and 1 year (28.3% vs 9.7%). Similarly, a higher proportion achieved WHtR ≤ 0.53 in the RWL group at 16 weeks (24.2% vs 8.9%,) and at 1 year (33.0% vs 18.4%).
The authors conclude: “Among adults with obesity, participation in a structured rapid weight loss program resulted in significantly greater weight loss at 1 year, and higher rates of achieving clinically meaningful BMI- and WHtR targets compared with a gradual weight loss approach. These findings indicate that, when provided within a controlled and professionally supervised setting, rapid weight loss may represent a more effective method than gradual weight loss for reaching key body weight targets associated with reduced obesity-related health risks.”
The study is led by Dr Line Kristin Johnson, Department of Endocrinology, Obesity and Nutrition, Vestfold Hospital Trust, Tønsberg, Norway, and colleagues.
Dr Johnson adds: “Our results clearly challenge the prevailing belief that slow and steady gradual weight loss is necessary to prevent weight regain and reduce obesity-related complications. By contrast, we show that rapid weight loss is not associated with weight regain, and, more importantly, that a larger proportion of participants undergoing rapid weight loss – compared with gradual weight loss – achieved clinically meaningful treatment targets for reducing the 10-year risk of type 2 diabetes, hypertension, atherosclerotic cardiovascular disease, and hip/knee osteoarthritis.
“These findings are particularly relevant given the urgent need for effective weight-loss and weight‑maintenance strategies. As many individuals with obesity cannot access or afford medical or surgical treatments, our results support the potential of effective, commercially available weight‑reduction programs to help reduce the growing burden on public healthcare systems.”
Fluctuations – known as the ‘yo-yo’ effect – in body mass index (BMI) and blood pressure are associated with the progression of diabetic kidney disease in people with type 1 diabetes, new papers have revealed.
The findings, shown in two studies from Dr Murat Ozdede, Visiting Research Fellow, and Janaka Karalliedde, Professor of Diabetes, both from King’s College London, indicate that only having good average blood pressure and weight may not be enough to prevent progression of the disease. Instead, keeping fluctuations under control may be a better way to keep the kidneys healthy.
Variability – also known as ‘yo-yo-ing’ – in weight and blood pressure has been shown to be harmful in people with type 2 diabetes with regard risk heart and kidney disease. Our work is the first demonstration of this potential risk in people with type 1 diabetes, many of whom had normal weight, BMI and blood pressure. Future studies will need to explore if reducing variability with treatments can reduce the risk of kidney disease.”
Janaka Karalliedde, Professor of Diabetes, King’s College London
Diabetic Kidney Disease (DKD) affects up to 40% of people with diabetes and is one of the leading causes of kidney failure in the UK and many countries around the world. Individuals with kidney failure require kidney replacement therapy. Doctors already know that DKD is linked to higher blood glucose, higher blood pressure and protein in the urine. However, these biological functions change over time. Therefore, the researchers were interested in exploring whether variation of these risk factors may affect the body in ways that stress the kidneys and contribute to progression of kidney disease.
The first study looked at changes in systolic blood pressure (max pressure) and diastolic blood pressure (when the heart rests in between beats). The researchers measured variation in visit-to-visit changes, taken from test results of 3,079 adults with type 1 diabetes between 2004 and 2018.
They used estimated glomerular filtration rate (eGFR) test results to understand how well the kidneys were filtering the blood. A 50% fall of eGFR, or a final eGFR below 30 – indicating serious kidney damage – were the primary endpoints.
They found that both a higher systolic blood pressure and diastolic blood pressure variability was linked to substantially higher risk of kidney decline. This was independent of average blood pressure, meaning two people could have the same average systolic blood pressure, but the one who has higher variability may be at greater risk of kidney harm.
The second study explored whether BMI fluctuation – also known as metabolic cycling – could add additional stress to the kidneys and lead to the progression of the disease.
The researchers studied 3,270 adults over roughly 9.6 years, taking at least six BMI measurements during that time. They used four different ways of measuring variability to confirm their analyses.
They found that one of the key factors contributing to worsening of the disease was higher BMI variability, even after adjusting for other risk factors. After 12 years, cumulative incidence of the kidney endpoint was 11.9% in the highest variability group, compared with just 2.1% in the most stable group.
Baseline BMI itself was fairly similar between the different groups, suggesting that simply ‘being heavier’ was less of a risk factor than BMI that changed over time.
These findings are of particular importance considering recent trends in weight loss diets and medication, that can cause sudden weight loss caused by weight gain – a phenomenon known as the ‘yo-yo’ effect.
Rapid fluctuations in weight or blood pressure can cause damage to the blood vessels in the kidney. People with diabetes are more susceptible to blood vessel damage and it’s vital to prevent further aggravating factors. Avoiding fluctuations in weight, blood pressure, and blood sugar levels may help reduce to risk of kidney damage.”
Janaka Karalliedde, Professor of Diabetes, King’s College London
Join our podcast as we unpack a study exploring the potential of the asthma medication formoterol as a novel treatment for Metabolic Dysfunction-Associated Steatohepatitis (MASH), a severe liver condition often linked to diabetes.
The researchers used experiments involving high-fat diet mice and human liver cell cultures to show that this beta 2 adrenergic receptor agonist effectively reduces liver fat accumulation. It does so by stimulating mitochondrial biogenesis and enhancing metabolic efficiency. In addition, a massive retrospective analysis of nearly 60 000 patients revealed that those using long-acting versions of these drugs experienced significantly lower rates of liver complications and reduced mortality.
A team led by metabolism researcher Prof Timo D. Müller at Helmholtz Munich has developed a new approach for treating obesity and type 2 diabetes: a hybrid molecule uses the well-known GLP-1/GIP signalling pathway as a “door opener” and delivers an additional metabolic modulator specifically into the target cells. In laboratory experiments, mice subsequently ate less, lost more weight and showed improved blood glucose values compared with reference treatments. The researchers published their preclinical results in the journal Nature.
Modern incretin therapies – drugs that mimic the body’s own satiety and blood-glucose signals (GLP-1/GIP) – have markedly improved the treatment of obesity and type 2 diabetes. Yet a key challenge remains: physicians would like to use further metabolic “levers”, for example drugs that make cells more responsive to insulin, so that glucose moves more easily from the blood into tissues. However, such additional drugs often act system-wide rather than in a targeted manner, increasing the risk of side effects.
“Our guiding question was: how can we enhance incretin activity without creating a second, systemically active source of side effects?” says the study lead Timo D. Müller, Director of the Institute for Diabetes and Obesity (IDO) at Helmholtz Munich, Professor at the Ludwig Maximilian University of Munich (LMU) and researcher at the German Center for Diabetes Research (DZD).
Müller’s team therefore pursued the idea of an “address label with cargo”: the researchers chemically linked a well-established incretin active component to a second pharmacological component – the drug lanifibranor, a so-called pan-PPAR agonist. The incretin part binds to GLP-1 or GIP receptors on the cell surface and ensures that the hybrid molecule is taken up into the cell. Inside the cell, the second component binds to PPARs – “switches” in the cell nucleus that regulate genes involved in fat and sugar metabolism. The aim is for this additional metabolic effect to arise specifically in GLP-1R/GIPR- expressing cells, rather than throughout the body.
Low Dose via a “Trojan Horse”
Functionally, the hybrid molecule combines five drug targets in one: it activates two receptors on the cell surface (GLP-1R and GIPR) and additionally engages three PPAR “switches” inside the cell. Müller describes the principle as a “Trojan horse”: the incretin part opens the door; the “cargo” acts only once it is inside the target cell. “A major advantage is the amount,” says Müller. “Because the second component is not administered separately and systemically, but ‘travels along’ with the incretin part, it can be used at a dose that is orders of magnitude lower.” In this way, the drug gains efficacy without amplifying side effects through broad distribution across the body.
In laboratory mice with diet-induced obesity, the approach showed clear effects: “The animals ate less and lost more weight than under a GLP-1/GIP co-agonist without cargo,” says Dr Daniela Liskiewicz, group leader at IDO and co-first author together with Dr Aaron Novikoff. “In the head-to-head comparisons shown, the effect was in part even stronger than with a GLP-1-only drug.” The study therefore suggests that the coupling is not merely “more of the same”, but measurably strengthens incretin activity – at least in mice.
Additional Metabolic Readouts Improve
It was not only body weight that changed: in the experiments, blood-glucose values improved and there were indications of better insulin action in the body. Put simply, insulin was better able to “channel” glucose from the blood into tissues, and the liver released less glucose into the bloodstream. At the same time, the researchers report that typical gastrointestinal side effects were comparable in their assessment to those of existing incretin therapies – and that, in the parameters examined, they found no indications of two feared issues associated with the coupled component, namely fluid retention and anaemia.
Beyond glucose metabolism, the mouse data also provided indications of additional, potentially favourable effects on the heart and liver. It is important to note that this is a preclinical study: whether the results will translate to humans remains open – also because the GIP receptor differs between mice and humans. “We see a principle with strong effects in the animal model – now the task is to optimise the approach for humans and move it towards the clinic,” says Müller. For that development, strong industry partners will be needed, he adds.
Researchers at Karolinska Institutet and KTH Royal Institute of Technology have developed an improved method for creating insulin-producing cells from human stem cells. The results, published in Stem Cell Reports, demonstrate that these cells effectively regulate blood sugar levels in laboratory tests and can reverse diabetes in mice.
Type 1 diabetes occurs when the immune system destroys insulin-producing cells in the pancreas, meaning the body can no longer absorb glucose from the blood and regulate blood sugar levels. One possible treatment is to replace these cells with new ones. However, previous methods of producing such cells from stem cells have often yielded mixed results.
“We have developed a method that reliably produces high-quality insulin-producing cells from multiple human stem cell lines. This opens up opportunities for future patient-specific cell therapies, which could reduce immune rejection,” says Per-Olof Berggren, professor at the Department of Molecular Medicine and Surgery, Karolinska Institutet, and corresponding author alongside Siqin Wu, researcher at Spiber Technologies AB (formerly at Karolinska Institutet).
Optimised cell production
The optimised production process yields more mature and purer insulin-producing cells than previous methods. In a laboratory setting, the cells were able to secrete insulin and responded strongly to glucose. When the researchers transplanted these cells into diabetic mice, the animals gradually regained the ability to regulate their blood sugar. The transplantation was performed in the anterior chamber of the eye.
“This is a technique we use to monitor the development and function of the cells over time in a minimally invasive way,” explains Per-Olof Berggren. “We observed that the cells gradually matured after transplantation, retaining their ability to regulate blood sugar for several months, which demonstrates their potential for future treatments.”
Stem cell therapy for type 1 diabetes is already being tested in several clinical trials. However, a challenge with previous methods is that the stem cells often develop into a combination of the desired and undesired cell types, increasing the risk of complications. Another challenge is that the insulin-producing cells created are often not mature enough to respond well to glucose.
Solving previous problems
By adjusting the culture steps and allowing the cells to form three-dimensional clusters themselves, many unwanted cell types are eliminated and the cells gain a better ability to respond to glucose, according to the researchers.
“This could solve several of the problems that have previously hindered the development of stem cell-based treatments for type 1 diabetes. Building on this, we will work towards clinical translation aiming at treating type 1 diabetes,” says Fredrik Lanner, professor at the Department of Clinical Science, Intervention and Technology, Karolinska Institutet, and last author of the paper.
Older adults with type 2 diabetes face a difficult trade-off: they are among the most vulnerable to medication-related harms yet are often underrepresented in the clinical trials that guide treatment decisions. A new study led by Yuan Lu, ScD, helps address this gap by providing large-scale, real-world evidence about the safety of commonly used diabetes medications.
Published in Nature Communications, the study analysed data from more than 1.8 million people aged 65 and older across the United States and Europe. The researchers compared four major classes of second-line antihyperglycaemic medications – typically prescribed when first-line therapy such as metformin is not sufficient – across 18 safety outcomes.
“Evidence from clinical trials often does not fully capture older adults,” says Lu, assistant professor of medicine (cardiovascular medicine) at Yale School of Medicine. “They are more likely to experience side effects due to frailty, multiple chronic conditions, and the use of several medications at the same time.”
Newer diabetes drugs show overall safety advantages
The study found a consistent pattern: newer classes of medications, including GLP-1 receptor agonists and SGLT2 inhibitors, were generally associated with lower risks of several important adverse outcomes compared to older drugs such as sulfonylureas and DPP-4 inhibitors.
Newer agents were linked to lower risks of hypoglycaemia, hyperkalaemia, and peripheral oedema – complications that can be especially dangerous in older adults. However, the findings also highlight important trade-offs. For example, SGLT2 inhibitors were associated with a higher risk of diabetic ketoacidosis, while GLP-1 receptor agonists were more likely to cause gastrointestinal side effects such as nausea and vomiting.
Rather than identifying a single “best” medication, Lu emphasises that the results support more informed, individualised decision-making. “Some patients may have a higher risk of hypoglycaemia, while others may be more susceptible to diabetic ketoacidosis,” she says. “These risks need to be considered together as part of an individual patient profile.”
Real-world data at a global scale
A key strength of the study is its scale and approach. The analysis drew on nine large databases and was conducted through the Observational Health Data Sciences and Informatics (OHDSI), an international research network that enables standardized analyses across diverse health care systems.
By using harmonised real-world data and consistent analytic methods, the researchers were able to evaluate a broad range of safety outcomes in routine clinical practice – offering insights that complement and extend findings from randomised trials.
Supporting safer prescribing for an aging population
As the population ages and the use of newer diabetes medications continues to grow, understanding their safety profiles in older adults is increasingly important. The findings reinforce current guideline recommendations that often favour newer agents, while also underscoring the need to tailor treatment decisions to each patient’s risks and preferences.
Like all observational studies, the analysis cannot fully rule out unmeasured differences between patients. Still, the large, multinational design gives a more complete picture of medication safety in a population often underrepresented in clinical research.
Looking ahead, Lu and her colleagues hope to expand this work to examine the comparative safety of individual medications and to evaluate the safety of newer GLP-1 receptor agonists across a wider range of outcomes, including among people with obesity. “By providing more evidence in populations that clinicians see every day, our goal is to support safer, more informed care,” she says.