
South African Scientists Make Breakthrough in Decoding Cancer’s Most Effective Survival Strategy
Kevin Naidoo, University of Cape Town
In the intricate biology of the human body, organs such as the breast, the colon and the lungs are lined with a defensive barrier known as the epithelium. At the heart of this barrier sits a remarkable protein called Mucin-1 (MUC1). In a healthy body, MUC1 is like a sentinel.
It stands on the cell wall, draped in a complex “armour” of long chains of sugar molecules (carbohydrates), where it serves as a physical shield against bacteria, viruses and toxins. Crucially, it communicates with the immune system, telling our natural defences when the body is under threat.
But in the case of cancer, this guardian exchanges its sugar coat armour for shorter sugar chains and so turns into a traitor. It stops sending danger signals to the immune system and instead binds to the immune cells, creating an anti-inflammatory microenvironment that promotes tumours.
The team I lead at the Scientific Computing Research Unit at the University of Cape Town is home to computer modelling experts and experimental chemical biology research scientists. The molecular details of this MUC1 alteration, which contributes to the transformation of normal cells into tumour cells, were recently published in Nature Communications, and provide a new look at exactly how this process happens.
By developing a novel “test-tube” synthetic biology approach, we modelled and decoded the molecular assembly line reorganisation that allows cancer to “redecorate” MUC1, turning it from a protective shield into a cloak of invisibility. We used our own computational chemistry algorithms to map the exact sugar coating positions that create a tumour-promoting environment.
Understanding the location and nature of the MUC1 sugars that prevent the immune system from detecting tumours provides the foundation for our laboratory and others in the field to develop cancer vaccines, biomarkers and therapeutics.
This South African-led discovery represents a major leap forward in our ability to decode one of cancer’s most effective survival strategies.
The problem: a malignant makeover
In a normal cell, the sugar molecules attached to MUC1 are long and complex. The process of attaching sugars is called glycosylation. In cancer cells, however, this process goes haywire. The sugar molecules are often cut short or altered, creating “aberrant” structures like the Tn and sialyl-Tn (sTn) antigens. These are specific types of sugar-protein combinations that are tags for tumour cells.
These altered sugars do two dangerous things: they allow the tumour to evade detection by the immune system, and they actively trigger the process of turning a normal cell into a cancerous one.
Because MUC1 is found in so many different types of cancer, the US National Cancer Institute has ranked it as the most accesible target.
To stop the cascading effect of the MUC1 changes from normal to tumour cells, scientists first had to understand exactly how the “assembly line” breaks down.
The discovery: relocating the factory
Our research team set out to do something ambitious: recreate the transition from a healthy sugar coating to a cancerous one in a laboratory setting.
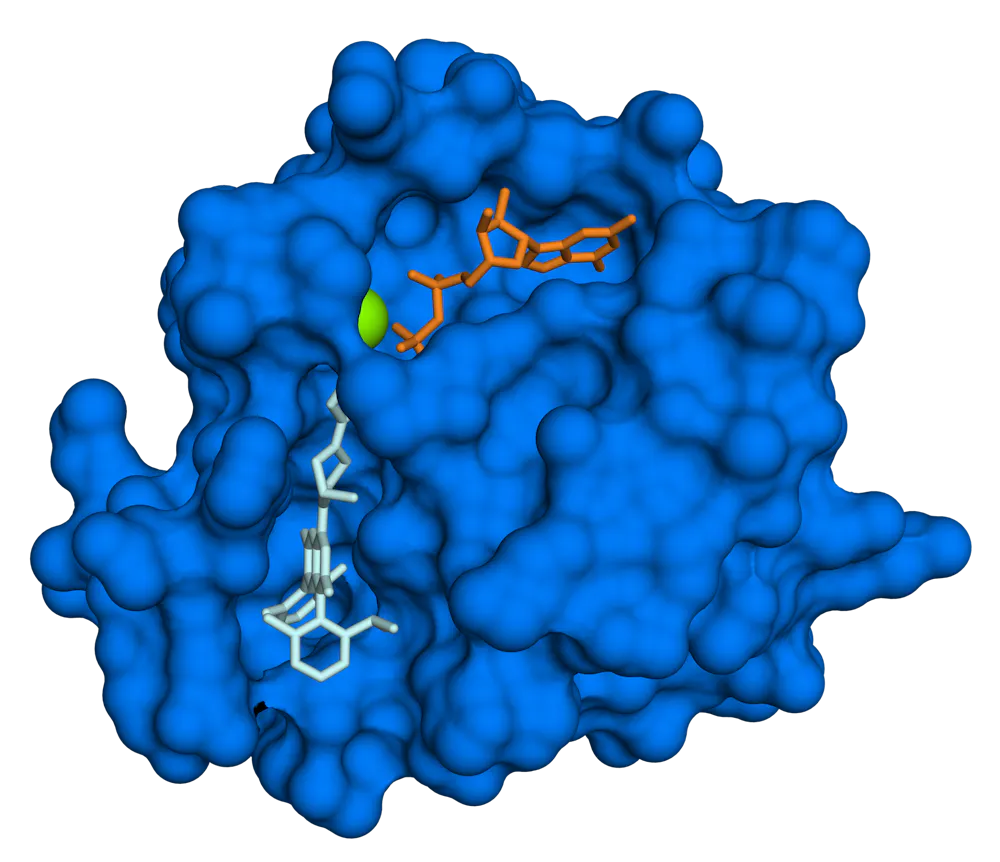
In normal cells, the enzymes that build these sugar chains (long molecules) live in a part of the cell called the Golgi apparatus, the cell’s “packaging and delivery centre”. We built an in vitro (test-tube) model to simulate what happens when these conditions change. We discovered that in tumour cells, the enzymes responsible for starting the sugar chains are relocated to another part of the cell, the endoplasmic reticulum, essentially the cell’s “factory floor”.
This relocation changes everything. Here, the enzymes are no longer inhibited by the usual cellular checks and balances. They take over the sugar sites on the MUC1 protein, creating the foundation for the cancerous Tn antigen.
To take the study even further, we used quantum chemistry. We simulated the behaviour of atoms and molecules at the most fundamental level to find out where these changes are most likely to happen. We identified a specific location on the MUC1 protein, known as the T13 site, which cancer enzymes prefer. This specific interaction is what drives the massive increase in the sTn antigen seen in malignant tumours.
Why this matters: from lab to patient
Understanding the “how” and the “where” of these sugar changes is the first step towards stopping them. The research didn’t stop at the test tube; the team is already looking at what this means for patients.
The next phase of the research, as detailed in a recent paper in Glycobiology, involves building a sophisticated “systems biology” computational model. A model can connect the changes in the MUC1 sugar coating to the behaviour of immune cells. For example, scientists found that when these cancerous sugars interact with macrophages (a type of white blood cell), they trigger the release of specific signals that tell the tumour to grow and spread.
We are refining these details for various types of cancer. We are comparing common forms of breast cancer with more aggressive, currently untreatable types to see if the “sugar code” differs between them.
By using this accurate, atomic-level data to build computer models of the entire biological system, we hope to identify new drugs that can block these signals. The goal is to move towards precision medicine: treatments that can strip away cancer’s sugar shield, allowing the patient’s own immune system to finally see and destroy the tumour.
Kevin Naidoo, Professor of Scientific Computing and Physical Chemistry, University of Cape Town
This article is republished from The Conversation under a Creative Commons license. Read the original article.








{kind=link}