Does Iron Accumulation in the Brain Contribute to Neurodegeneration?
Salk Institute scientists discover chronoferroptosis, a chronic stress pathway in cells that causes neurons to become less resilient over time and more vulnerable to neurodegeneration
Click here for a high-resolution image.
Credit: Salk Institute
Neurodegenerative diseases affect tens of millions of people worldwide. Among these, Alzheimer’s and Parkinson’s diseases are the most common; in the United States alone, the Alzheimer’s Disease Association and Parkinson’s Foundation report roughly 7 million people with Alzheimer’s and another million with Parkinson’s. An intriguing clue lies in the tangled mystery of neurodegeneration that scientists are working to solve: iron accumulation.
Scientists have noticed that iron can slowly build up inside neurons. Early in life, this iron accumulation appears to have little effect on neuronal function. However, later in life, it can contribute to a slow neuronal demise. Salk Institute researchers studied nerve cells to figure out if and how this iron accumulation relates to neurodegenerative diseases. They found that the excess iron stuck in neurons lowers the cells’ defences, making them more vulnerable to stressors and other cellular insults through a process they named chronoferroptosis.
The study, published in Cell Death Discovery on June 18, 2026, points to iron accumulation as a key target in the effort to predict, prevent, and treat neurodegenerative diseases.
“Resilience has become a huge topic of discussion when it comes to Alzheimer’s disease and other neurodegenerative disorders, trying to make the brain more resilient in the face of stressors that contribute to neurodegeneration,” says senior and co-corresponding author Pam Maher, PhD, a research professor at Salk. “Our study reveals that cells lose resilience when iron hits a certain level, making neurons more susceptible to stressors that damage or even kill them.”
What do we already know about how the body uses iron, and is it linked to neurodegeneration?
Iron is an essential mineral for a healthy body. Found in dark leafy greens, starchy cereals, lean meats, seafood, and other common foods, iron helps red blood cells develop, carries oxygen around the body, makes hormones, and so much more, with a hand in everything from the immune system to energy production.
“It’s one of the most important minerals in the body,” says co-corresponding author Nawab John Dar, PhD, a postdoctoral researcher in Maher’s lab. “So, it isn’t the iron itself that is a problem with age. It is this accumulation of iron over time that is the problem.”
While the jury is still out on the exact mechanisms that initiate iron accumulation in neurons, the Salk team suspects the buildup is caused by a failure in the cells’ iron export machinery – iron enters neurons as usual but fails to get removed after use. But this failure doesn’t impact neurons for quite some time. The question is, why?
“People have been doing these experiments looking at iron exposure’s influence on cells over short 24- to 48-hour spans,” explains Dar. “But if neurodegenerative disorders are progressive, shouldn’t we have a cellular model that is progressive, too?”
Is iron accumulation making neurons less resilient?
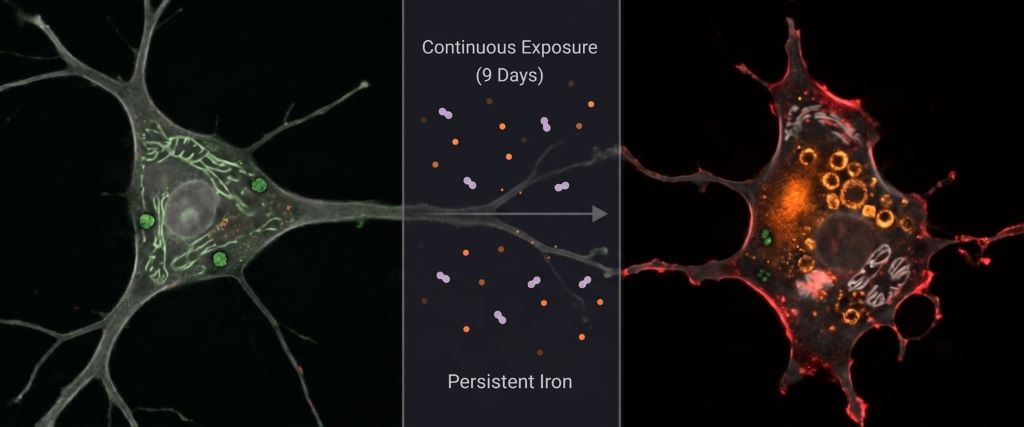
Using a human-derived nerve cell line, the Salk team created the first progressive model of iron accumulation in neuronal cells. They compared the effects of both acute (between six and eight hours) and chronic (nine days) exposure to iron. What they discovered was an entirely new pathway, which they dubbed chronoferroptosis.
Maher has been studying ferroptosis for decades. Until now, ferroptosis was considered an iron-dependent cell death pathway, with cell death dependent on a process called lipid peroxidation. “It is like the cellular equivalent of when a cooking oil or nut goes bad. The fats in that oil or nut have undergone peroxidation,” explains Maher.
Chronoferroptosis adds the dimension of time to ferroptosis. To the researchers’ surprise, the pathway does not necessarily end in cell death. Instead, the findings reveal that ferroptosis can act as a cellular stress pathway.
In acutely exposed neurons, there was very little biochemical difference pre- and post-exposure to iron. However, in chronically exposed neurons, there were lots of changes: upregulation of some processes and downregulation of others; accumulation of harmful chemicals and depletion of helpful ones; and elevated lipid peroxidation. And when each exposure group was exposed to further stress, acutely exposed neurons could handle the stress, while chronically exposed neurons could not.
“We think these coordinated alterations in iron-handling and antioxidant defence proteins make chronically exposed neurons vulnerable to neurodegenerative pathology,” says Dar. “Entering this state of chronoferroptosis may set neurons up for age-related failure.”
How might chronoferroptosis inform neurodegeneration care?
By creating the first progressive model of iron accumulation in neuronal cells, the researchers were able to reveal surprising new clues in the case to crack neurodegeneration. “It’s not the amount of iron that seals the fate of these cells,” says Dar, “it’s the amount of time they spend under stress.”
Perhaps scientists will one day be able to detect when the brain begins entering this vulnerable state, when iron accumulation starts stressing neurons. They could then develop new interventions to address iron imbalances and keep neurons more resilient for longer.
“It’s not something we worked on in this paper, but our lab has developed several compounds to inhibit this pathway,” says Maher. “This could really be a promising therapeutic route for boosting neuron resilience and staving off neurodegeneration as we grow older.”
Source: Salk Institute