L-R – Dr Bilal Bobat, Professor Jerome Loveland, Dr Sharan Rambarran and Dr Dinen Parbhoo, the transplant team at Wits Donald Gordon Medical Centre alongside the liver perfusion machine, the first of its kind to be implemented on the African continent.
Johannesburg, 12 June 2026:For a patient waiting for a liver transplant in South Africa, the hardest part is not the surgery. It is the wait and the knowledge that an organ may never come. In a country facing severe organ shortages, every decision to accept or decline a donor liver carries immense weight and every viable organ that goes unused represents a lost opportunity to save a life.
At the centre of changing this reality is the Wits Donald Gordon Medical Centre (WDGMC), home to one of the leading liver transplant programmes in Africa and a unit internationally recognised for its contribution to specialised transplant care, research and surgical training. Having performed over 1 000 liver transplants, the programme represents decades of expertise, innovation and collaboration.
Now, WDGMC, in partnership with Surgeons for Little Lives and with support from key corporate sponsor Weelee, has introduced a state-of-the-art liver perfusion machine, becoming the first transplant centre on the African continent to implement this technology for liver transplantation.
This technology keeps donor livers viable outside the body while clinicians assess, monitor and actively improve the condition of the organ before transplantation. By allowing transplant teams to better maintain organ viability, the machine has the potential to increase organ utilisation, reduce complications and improve transplant outcomes for patients who may otherwise not survive the wait.
“As a transplant programme, our responsibility extends far beyond the operating theatre,” says Professor Jerome Loveland, Head of Solid Organ Transplantation at WDGMC. “This technology will help us better assess donor organs and increase the number of livers that can safely be transplanted, whilst simultaneously improving results. In a country where every donor organ matters, this will have a significant impact on organ utility and patient outcomes.”
South Africa’s transplant programmes continue to achieve strong outcomes despite operating within a severely resource-constrained environment and against the backdrop of ongoing organ shortages. As a result, transplant teams are often required to make difficult decisions under significant pressure.
“This technology changes the level of information we have available before transplantation. Traditionally, organs are preserved on ice and assessment is limited. Machine perfusion allows us to monitor how the liver is functioning outside the body. Beyond the valuable information it provides, the machine has the ability to resuscitate the liver by delivering oxygen to the liver cells, creating the best metabolic environment outside the body. This helps us make more informed clinical decisions and potentially increases the number of organs that can safely be transplanted,” says Dr Sharan Rambarran, Transplant Surgeon at WDGMC.
The introduction of the machine is also expected to contribute to reduced post-operative complications, shorter hospital stays and improved recovery outcomes.
“Too many patients in South Africa deteriorate while waiting for a transplant because there are simply not enough donor organs available,” says Dr Bilal Bobat, Transplant Hepatologist at WDGMC. “Anything that helps us safely expand organ utilisation has the potential to directly impact survival and quality of life for patients and families facing end-stage liver disease.”
“Weelee is always looking for opportunities to contribute to causes that create real and lasting impact,” says Errol Levin, CEO of Weelee. “Supporting advancements in liver perfusion technology aligns perfectly with our commitment to innovation that improves lives. This ground-breaking initiative has the potential to save countless lives and we are proud to be associated with a project of such significance.”
WDGMC plays a unique role within South Africa’s healthcare system. As a private academic hospital affiliated with the University of the Witwatersrand, the Centre combines highly specialised clinical care with academic medicine and collaboration across both the private and public healthcare sectors.
While the technology represents an important advancement in liver transplantation, clinicians stress that increasing organ donation awareness remains critical to improving access to life saving transplants in South Africa.
For the transplant teams, this marks not only a clinical advancement but the beginning of a broader effort to continue strengthening transplant medicine in South Africa.
A plant long used in traditional medicine is now at the centre of research that could shape future cancer treatment options in South Africa and beyond.
Researchers at the North-West University(NWU) are investigating the anti-cancer potential of Lessertia frutescens, commonly known as cancer bush, after laboratory studies showed activity against several forms of cancer, including drug-resistant small cell lung cancer and colorectal cancer.
According to Prof Chrisna Gouws, a research professor in the Centre of Excellence for Pharmaceutical Sciences in the Faculty of Health Sciences, the research team tested extracts from the indigenous plant on cultured human cancer cells and more advanced laboratory-grown “mini-tumours” known as spheroids.
“Lessertia frutescens has shown significant anticancer activity against several different cancer types in our research,” she says.
Targeting cancers considered incurable
She says the findings became more important when the team observed activity in cancers that no longer respond to conventional treatment.
“What is very interesting and exciting is the apparent activity in drug-resistant cancers such as resistant small cell lung cancer where known chemotherapies have limited to no activity,” Prof. Gouws says.
“This provides us with new avenues to investigate for treatment options to treat cancers currently considered incurable.”
The research team said another factor attracting attention is the plant’s longstanding use in traditional medicine and its safety profile.
“An important consideration is that this plant has a long history of use and is considered non-toxic and safe for use,” Prof. Gouws says.
“It’s anticancer activity comes without the significant side-effects known to occur with most standard chemotherapies.”
Other systems in the body may benefit
Researchers also found that the plant may support other systems in the body during treatment.
“Lessertia has known boosting effects for the digestive and immune systems, and it can have mood-enhancing activities as well,” she says.
“It may therefore not only target the cancer but positively impact the patient as a whole at the same time.”
The team is now studying the plant’s phytochemicals to identify the molecules responsible for the anticancer activity and understand how they work.
“Although many molecules have been identified and shown to contribute to the anticancer activity of the plant, the mechanism of action remains mostly unclear,” says Prof. Gouws.
“We are therefore delving deeper now to try and understand how and why this plant works.”
The next phase of the study will include animal model testing later this year to confirm safety and efficacy before future clinical trials can be considered.
At the same time, the researchers are developing a complementary medicine product that may be available in pharmacies by 2027.
Prof. Gouws says the project could also create economic opportunities.
“Chemotherapy can be very expensive and inaccessible in rural areas. A new plant-based treatment will be much more cost-effective and may be more accessible because it can be manufactured locally,” she says. “An increase in demand for the plant material will also create economic opportunities through farming.”
More about Prof Chrisna Gouws
Prof Gouws leads the strategic project for Human-Based New Approach Methodologies for Biomedical Research. She holds a PhD in biochemistry and has more than 15 years’ experience in utilising cell culture-based models for human health and disease research, including developing new complex in vitro models for applications in drug research, including traditional medicinal remedies and plant materials for cancer treatment.
She is the founder and executive committee chair for the Society for Advanced Cell Culture Modelling for Africa, a board member of International Microphysiological Systems Society, and co-editor of the NAM Journal.
From unregulated weight loss injections to unsafe pain tablets, substandard and falsified medical products pose a threat to the health of people. Spotlight reports on how regulators are fighting the problem in South Africa.
“I know that there is a risk, but at this point I feel that the benefits outweigh everything else,” says Anna*, who buys unregulated medicine on the black market.
She was prescribed GLP-1 RA medicines by a doctor after being tested for insulin resistance. She has lost around 30kg and says the positive impact on her body, life, and self-esteem has been massive. GLP1 RAs (Glucagon-Like Peptide-1 Receptor Agonists) medicines, sold under brand names like Ozempic and Mounjaro, are increasingly used for weight loss and to prevent and/or treat diabetes.
When global shortages affected GLP-1 RA stocks in local pharmacies, Anna started buying similar drugs directly from unregistered sellers. For around R1 650, a fancy-looking box with a three-month supply of injections is delivered to her in a small cooler box. “I knew then already that what I was buying was unregulated and potentially inferior or even dangerous,” she says, adding, “but I was finally starting to feel good about myself.”
Apart from being aware that the unregulated drugs could potentially harm her, Anna says she found that the regulated products were often out of stock, expensive, and came with stigma from pharmacists who quizzed her on whether she deserved the products. “If I could have kept doing it the proper way, I would have, but there were just too many obstacles,” she says.
Defining the problem
Weight-loss medicines are only one of several types of health products that are frequently purchased outside of formal channels, according to the South African Health Products Regulatory Authority (SAHPRA).
“Commonly affected products include painkillers, antibiotics, weight-loss and sexual enhancement products, skin-lightening products, and some chronic medicines,” Mokgadi Fafudi, SAHPRA’s manager of regulatory compliance, tells Spotlight.
“Combating the threat of substandard and falsified medical products is one of the urgent global challenges of this decade,” says Faridun Nazriev, the external relations and communications officer at the World Health Organization (WHO) Country Office in South Africa.
“Substandard products are those that do not meet quality standards and specifications, often due to poor manufacturing practices or inadequate quality control. Falsified medical products deliberately misrepresent their identity, composition or source”, according to the WHO. These products, it adds, are often created and distributed with the intent to deceive consumers for financial gain.
Two other definitions should not be confused with these, cautions Dr Andy Gray, a senior lecturer in Pharmacology at UKZN and co-director of the WHO Collaborating Centre for Pharmaceutical Policy and Evidence-Based Practice.
Compounded medicines are custom formulations that may be specific to a patient, but are generally not registered by SAHPRA.
Generic medicines are those that have been tested and found to be as safe and effective as originator medicines, but are generally cheaper. Generic medicines on the market have been approved by SAHPRA and are not in any way substandard.
Gray says the term counterfeit is no longer used by the WHO, because it refers specifically to breaches of intellectual property, like trademarks.
Lack of data
While the WHO estimates that 1 in 10 medicines in low-and middle-income countries are substandard or falsified, all regions are affected and have been seeing an increase, according to a 2024 report from the WHO’s Global Surveillance and Monitoring System.
South Africa also appears to have rising rates. SAHPRA’s 2021/2022 annual report notes that 101 health product quality complaint reports were filed. In 2022/23, that figure nearly tripled to 297.
Fafudi says that the organisation received 588 reports of possible non-compliance in the 2024/2025 year. She says that for the 2025/26 year, this number exceeds 570 cases, though this has not yet been published by SAHPRA.
But such reports are likely only the tip of the iceberg. Gray laments that we don’t have the full picture of how big the problem of substandard and falsified medical products really is.
This is partly because, by its very nature, the sale of substandard and falsified medicines is usually hidden. Fafudi says that these medicines are often sold through informal markets, unregulated outlets, online platforms, and cross-border smuggling networks.
Gray adds that these medications aren’t necessarily always sold through informal means. “They may be infiltrated into wholesalers or state medicine depots, and then distributed,” he says, “Or they may be sold directly to pharmacies or prescribers and then sold to patients.”
A threat to patients
As in Anna’s experience with GLP-1 RAs, there is often a demand for unregulated products because the properly regulated products can’t meet the public demand.
Fentse Maseko, who works in the Department of Pharmacology and Pharmacy at Wits University, researched this issue in her Master’s thesis and advocates in the space. She notes that in many low- and middle-income countries, particularly in remote and underserved areas, limited access to medicines may force patients to seek treatment from informal markets. She adds that in South Africa, porous borders and rising costs also play a role.
Whatever the reasons behind their proliferation, the risks to the healthcare system and individuals are multi-faceted.
“Substandard and falsified medicines are a serious threat to patient safety and public trust,” says Refiloe Mogale, the executive director for the Pharmaceutical Society of South Africa (PSSA). “These products can lead to treatment failure, harm, or even death.”
Maseko warns that it can also add to the growing problem of antibiotic resistance if antibiotics are substandard. It can also strain the healthcare system when second or third-line treatments are needed for issues initially addressed with unregulated products, or caused by them.
The role of the regulator
The main body in South Africa responsible for regulating substandard and falsified medicines is SAHPRA. Fafudi explains that they conduct post-market surveillance and inspections, run a whistleblower reporting system, manage product recalls, and monitor illegal advertising and online sales.
SAHPRA also works with specialised units in the South African Police Service as well as other stakeholders such as customs to enforce joint operations. Fafudi says such joint operations have been conducted on at least a monthly basis.
There are also legal actions, including issuing warnings, seizing or destroying products and criminal prosecution. According to the Medicines and Related Substances Act 101 of 1965, fines or prison sentences not exceeding 10 years may be prescribed.
The PSSA however charges that not enough is being done. “Key gaps are visible in insufficient regulatory capacity, weak border control, limited enforcement scale and the under-resourced National Action Plan,” Mogale says. “The system is overwhelmed by the speed and sophistication of the problem.”
Reporting unregulated products
The public can help address the problem of substandard and falsified medicines. SAHPRA advises buying only from licensed and authorised pharmacies and healthcare providers.
“Be cautious of unusually low prices, miracle cure claims, and poor packaging,” Fafudi warns. “Always check packaging, expiry dates, and consult healthcare professionals before use.”
Suspicious products or sellers can be reported on the SAHPRA website.
Jas Bhana, Chief Executive Officer of the Innovative Pharmaceutical Association of South Africa, adds that the public can also report suspicious products to the National Department of Health or their nearest pharmacy. “Combating this threat requires collective vigilance to safeguard every patient’s right to safe, quality, and effective medicines,” she says.
This goes hand-in-hand with the need for consumers to know the dangers, Maseko explains. “While public education plays an important role in mitigating this risk, effective risk communication remains a challenge, particularly in communities with limited health literacy,” says Maseko.
On a bigger scale, Nazriev explains that the WHO prioritises prevention, detection, and response as the main pillars of action. This includes local regulation as well as collaboration between countries.
“Given the transnational nature of globalised medical product supply chains as well as criminal networks, collaborating across borders and sectors is essential to national, regional and global responses,” he says.
Better regulation
Gray acknowledges that there is a challenge in budgets and laboratory capacity, but even so he calls for more to be done. “SAHPRA needs to move from a largely reactive stance to a more proactive one, sampling medicines from the distribution chain and submitting them for checking, and then report to the public on their findings,” he suggests.
The PSSA recommends implementing a national medicine registry with a track-and-trace system and stricter control of online medicine sales, including mandatory certification and monitoring.
SAHPRA is already planning along some of these lines. “Future plans include strengthening supply chain traceability, enhancing detection systems, regulating online medicine sales, and increasing public awareness campaigns,” says Fafudi.
Part of this direction comes from a National Action Plan (NAP), launched late last year by SAHPRA, with support from the National Department of Health and the WHO.
“All actors within the supply chain, particularly at key pinch points in both the public and private sectors, must be equipped with the knowledge, skills, and equipment to identify and report suspicious products to SAHPRA,” Health Minister Dr Aaron Motsoaledi is reported to have said at the launch of the NAP. “All activities should mitigate the risk of substandard and falsified medical products. This includes increased vigilance at ports of entry, through to post-market surveillance of high-risk products, inspection of manufacturers, distributors and wholesalers.”
Whether all this will be done, and what it will mean for people like Anna who knowingly choose to use unregulated medicines, remains to be seen.
New post-portem study reveals over 80% of infection-related neonatal deaths in South Africa are preventable.
Photo by William Fortunato on Pexels
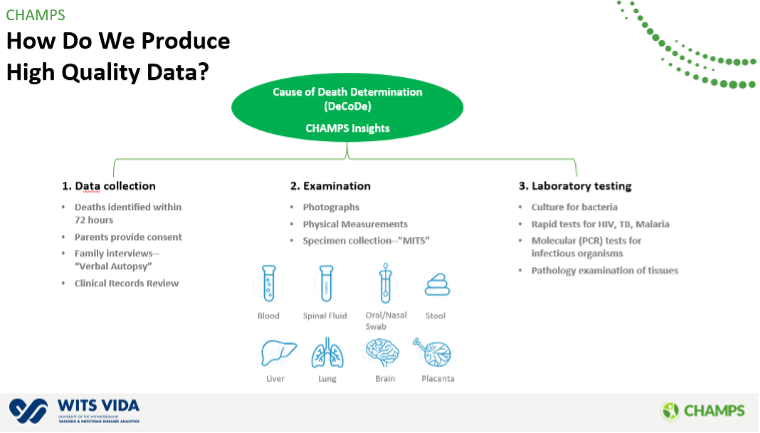
A groundbreaking study published in The Lancet Infectious Diseases Journal has identified that the vast majority of neonatal (newborn infant in the first 28 days of life) deaths caused by infections in South Africa and other low-and-middle-income countries could be prevented through improved clinical care and targeted medical interventions. The research, conducted by the Child Health and Mortality Prevention Surveillance (CHAMPS) network, utilised innovative post-mortem techniques that enables accurate identification of causes of death in low-resource settings. To provide the most granular look to date at what is killing newborns in these regions, more than 2600 neonatal deaths were analysed using minimally invasive tissue sampling (MITS).
Dominant Hospital Pathogens: In South Africa, Acinetobacter baumannii was the overwhelming driver of hospital-acquired infections, contributing to 74.3% of presumed hospital-acquired neonatal deaths.
Community-Acquired Threats: Group B Streptococcus (GBS) was identified as the leading cause of community-acquired neonatal deaths in South Africa, accounting for 30.6% of such cases, followed by Escherichia coli at 24.7%.
Emerging Fungal Risks: South Africa was the only site to report specific life-threatening fungal infections, including Candidozyma auris and Nakaseomyces glabratus, in the causal pathway to death.
Preventability: The modifiable factors identified to reduce these deaths include improvements in infection prevention and control (50.8%), clinical care (50.7%), and antenatal and obstetric care (42.2%).
The findings reveal that current empirical antibiotic treatments may be insufficient, particularly in high-burden settings where antimicrobial resistance is rising. The study also shows that infections often occur alongside other conditions such as prematurity and birth complications, indicating that neonatal deaths are driven by multiple, interconnected factors.
“These findings indicate an urgent need to review empirical antibiotic treatment for neonatal infections,” said Prof Shabir A. Madhi, Director of the South African Medical Research Council Vaccines and Infectious Diseases Analytics Research (Wits VIDA) Unit and lead author of the study. “The high prevalence of multidrug-resistant pathogens like K. pneumoniae and A. baumannii suggests our current standard protocols may no longer be sufficient. Alarmingly, some of these bacteria are resistant to all classes of antibiotics currently available.”
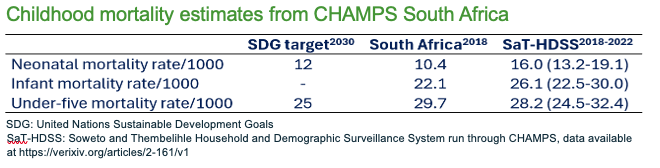
Nearly half of all deaths in children under five occur in the neonatal period, with the highest burden in Africa and South Asia. Importantly, local data further underscores the urgency of action. Within the Soweto and Thembelihle surveillance population, the neonatal mortality rate is estimated at 16.0 deaths per 1000 live births, significantly higher than both South Africa’s national estimate of 10 per 1000 and the Sustainable Development Goal (SDG) 2030 target of 12 per 1000 live births.
These findings highlight persistent inequalities in maternal and child health outcomes, even within urban settings, and reinforce the need for targeted, evidence-based interventions.
The MITS technique used at Wits VIDA uses needle biopsies rather than full autopsies to collect biological specimens. This method proved far more effective than traditional antemortem diagnostics, which failed to identify a pathogen in up to 73% of suspected sepsis cases in South Africa.
The study provides one of the most comprehensive, pathogen-specific analyses of neonatal deaths to date and ultimately, the study highlights a powerful opportunity. That most infection-related neonatal deaths are preventable.The CHAMPS consortium concludes that prioritising new maternal vaccines and strengthening hospital infection control are essential steps to reducing the high burden of neonatal mortality.
CHAMPS South Africa consistently shares its granular research findings with the National Department of Health (NDoH) through various channels to ensure this detailed evidence assists in developing targeted strategies to prevent neonatal infections. These data, which provide a precise look at the pathogens responsible for mortality, are intended to help the NDoH refine empirical antibiotic protocols and strengthen hospital infection control measures. Beyond policy-level engagement, CHAMPS collaborates with local communities to raise awareness regarding prevention strategies, specifically emphasizing the importance of early antenatal care booking and consistent attendance. By focusing on these modifiable factors, the initiative seeks to improve obstetric care and reduce the number of babies born “too soon or too small,” addressing the preterm birth complications that frequently underlie neonatal deaths.
About CHAMPS: The Child Health and Mortality Prevention Surveillance (CHAMPS) network is a global collaboration funded by The Gates Foundation. It aims to provide accurate data on the causes of childhood death to inform policy and save lives in high-mortality regions.
Cipla has been awarded a public sector vaccine tender, reaffirming the company’s commitment to strengthening South Africa’s immunisation program through the equitable supply of high‑quality, affordable vaccines.
Cipla submitted bids across several critical paediatric and childhood immunisation categories, including Pneumococcal Conjugate Vaccine (PCV‑10), Rotavirus vaccine, Hepatitis B (Paediatric formulation). These vaccines play a vital role in preventing life‑threatening childhood illnesses and reducing the burden on healthcare systems.
CEO of Cipla Africa, Paul Miller, said: “This tender award marks an important milestone for Cipla as we continue to expand our vaccine footprint in support of national immunisation priorities. We can meaningfully contribute to comprehensive immunisation programmes and long‑term disease prevention efforts.
“Our participation across multiple vaccine categories demonstrates our commitment to addressing critical public health needs and strengthening health outcomes for children and communities.”
Cipla’s vaccine portfolio is underpinned by stringent quality standards and a focus on ensuring continuity of supply reliability. Cipla has a long history of partnering with the Department of Health to support equitable access to quality healthcare, including the supply of antiretrovirals and various vaccines.
Cipla South Africa focus will be ensuring reliability of supply, consistency, and responsible partnership with the public health sector, particularly in communities where access to healthcare remains uneven. CEO of Cipla Africa, Paul Miller, said: “This tender reaffirms our ongoing partnership with the state, as part of Cipla’s mission of ensuring access to quality, affordable healthcare.”
As part of our ethos of “Caring for Life”, we strongly believe in the importance of robust routine immunisation programmes that save lives, reduces inequality and delivery lasting benefits for society as a whole. In public health, progress often comes down to getting the basics right – ensuring vaccines are available, delivered on time, and reach every child who needs them.”
Participation in the Expanded Programme on Immunisation (EPI) aligns with Cipla’s broader mandate to support preventative healthcare and long‑term public health sustainability, said Miller.
Cipla South Africa continues to work closely with healthcare partners and has invested in initiatives to strengthen vaccines knowledge and reduce vaccine hesitancy. For more information about vaccines, visit https://medinformer.co.za/?s=vaccines
South Africa is facing an alarming increase in non-communicable diseases and related mortality. According to Statistics South Africa, deaths due to non-communicable diseases such as type 2 diabetes and hypertension increased by over 58% between 1997 and 2018.
The crisis of overweight and obesity in the country adds to the risk of these diseases. Nearly 40% of the adult population is overweight. Although physical activity can help prevent and manage many non-communicable diseases, 47% of adults do not engage in any physical activity. Most people struggle to meet the World Health Organization’s recommended 150-300 minutes of moderate-intensity aerobic physical activity per week.
A significant part of the challenge is that people have adopted an “all or nothing” approach to physical activity. The perception is that one has to participate in structured workouts, such as gym sessions, running, or cycling.
Instead, research has shown that even brief, low-intensity movements can yield measurable physical and mental health benefits. Even everyday tasks count. New evidence shows that short movement bouts of less than five minutes can have positive health implications.
As researchers in exercise science and sports medicine we have observed that physical activity is particularly low in South Africa. Only 19.8% of adults meet the WHO’s guideline, against the global average of 73%.
Our study of 62 office-based workers at the University of the Witwatersrand also showed the short-term health impact of height-adjustable, sit-to-stand desks. Our intervention reduced prolonged sitting and slightly improved indicators such as body mass index and blood pressure. Given South Africa’s high burden of obesity and sedentary lifestyles among office workers, these improvements are encouraging and support global health messaging that even modest increases in daily movement can positively influence health.
These findings were the springboard for the “Mzansi, what’s your move?” campaign at the university. We want to encourage staff and students to move more by showing how simple actions add up to physical activity. The campaign is supported by a series of comics and murals on campuses.
Here, we highlight some of the actions that we used in our campaign to encourage everyone to get moving. These are daily tasks that may seem mundane but count as physical activity, while reflecting people’s realities.
Housework
Many people do not consider housework a form of physical activity. But tasks like sweeping, mopping or vacuuming require sustained movement and engage multiple muscle groups.
Scrubbing floors, washing windows and cleaning bathrooms involve movements such as squatting and stretching. Working in the garden can strengthen muscles too.
As part of our campaign, we’ve developed comic strips that highlight movements that can be done at home and in the community. We emphasise how all family members can move in ways that fit their lifestyles and physical abilities.
Active commuting
Walking or cycling to work or school contribute significantly to daily physical activity. Studies have shown that active commuting is associated with lower body fat, reduced blood pressure, and improved mental well-being.
Including movement into daily travel routines is a practical way to accumulate physical activity without setting time aside. Walking briskly to a train station, cycling a few kilometres to work, or taking a longer walking route to drop off children at school accumulates over time. Even seemingly small changes, such as getting off the bus one stop early or taking the stairs instead of the elevator, produce measurable health benefits over weeks and months.
However, achieving the full benefits of active commuting is complex and it relies on cities building and maintaining road infrastructure. In South Africa, safety is a legitimate concern for all road users. A 2024 Statistics South Africa report shows that more pedestrians than car occupants died in road crashes in 2007, 2013, and 2019. Another safety concern relates to the country’s high crime rates. People may be reluctant to walk, even in their own neighbourhoods.
These challenges are not insurmountable. For starters, people should consider people moving in groups, joining walking and running clubs.
Beyond what individuals can do, municipalities can do something about green spaces. This includes ensuring that parks are safe to walk in and are clean. Broken pavements and bicycle lanes need to be maintained in all neighbourhoods.
Incidental movements
Incidental movements refer to small bouts of activity that occur throughout the day. Integrating these movements into everyday life can yield significant health benefits, especially in office contexts, where many people sit for extended periods. Employers can try nudging staff, for example to use the stairs instead of elevators, with simple posters or painted footprints. Another way to encourage physical activity is to centralise shared equipment (printers, bins, water stations) so that staff walk short distances.
Micro-breaks also provide opportunities for informal movements. Stretching during meetings or after long sitting periods, standing discussions instead of seated ones, and walking meetings for small groups all contribute to the physical activity of employees.
In 2024, we investigated the short-term impact of physical activity interventions such as high-intensity interval training and moderate-intensity continuous training on 43 labourers at the University of the Witwatersrand. The number of participants in this study was small, but the findings show that our intervention reduced indicators such as waist circumference, body mass index, blood glucose and blood pressure, and improved physical fitness.
Way forward
People don’t need a gym membership or a strict workout schedule to get moving. Simple, everyday activities all add up to meaningful physical activity. Small movements help to reduce the risks of chronic diseases, strengthen muscles, boost mental wellbeing, and counteract the harmful effects of prolonged sitting.
These “movement snacks” make exercise accessible, manageable and sustainable, particularly for people who find structured workouts intimidating or time-consuming.
Around 3.8 million people in South Africa developed depression in 2024, researchers estimate in a major modelling study. Photo from Pixabay CC0
By Gauta Mashego
Substance abuse is both a symptom and a consequence of untreated mental illness, and government needs to urgently step in to confront this dangerous overlap, argues Gauta Mashego of SECTION27.
Mental health globally has been in crisis for years. The strain on mental health was especially visible when the world stood still during the COVID-19 pandemic. The prevalence of anxiety and depression increased by 25% in the first year of the global outbreak of the SARS-CoV-2 virus, according to the World Health Organization. However, as the pandemic eased and life returned to the usual, open conversations around mental health also tapered off.
In South Africa, as in many low-and-middle income countries, people struggle with mental health disorders such as anxiety and depression. Around 3.8 million people in South Africa developed depression in 2024, estimate researchers in a major modelling study published as a preprint in March on medRxiv.
Mental health is shaped by many factors
Several studies worldwide report a high prevalence of substance use among people with mental illness compared to the general population.
Researchers have found that patients who suffer from psychotic disorders, such as schizophrenia and bipolar mood disorder, were more likely to abuse alcohol and illegal substances. Indeed, findings from a community survey highlighted a substantial burden of co-occurring mental disorders and alcohol use among men in three provinces in South Africa.
What also makes our society vulnerable to both mental health conditions and increased use of drugs and the development of substance use disorders, is our historical context of apartheid as well as socio-economic factors such as poverty, unemployment, and violence. Researchers have argued that mental health problems are related directly to poverty, while others also make the case that the poor are at greater risk than the rich to suffer from mental illness. At the same time, those living with mental illness are more likely to remain trapped in poverty due to high treatment costs, reduced productivity, and stigma around mental illness.
The kids are not alright
Underage drinking further complicates an already complex problem.
Up-to-date statistics of underage drinking in South Africa are limited, however the matter was thrust into the spotlight on Christmas day in 2025 when a disturbing video circulated on social media showing children between the ages of 6 and 12 consuming alcohol in the presence of adults.
Providing insights into the drinking behaviours of adolescents aged between 11 and 18, a 2019 Human Sciences Research Council study in townships across three provinces found that most had their first drink at the age of 13 or 14 years.
Highlighting the extent of underage drinking among Grade 8–11 learners from public schools in all nine provinces, the 2011 South African Youth Risk Behaviour Survey recorded that around 17% of 13-year-olds and 18% of 14-year-olds had engaged in drinking five or more drinks within a few hours on one or more days in the preceding month.
Mental disorders that commonly co-occur with alcohol use disorders in adolescents include antisocial disorders, mood disorders, and anxiety disorders.
Young people’s drinking habits are often linked to factors such as social norms, and the accessibility and affordability of alcohol. Added to this, since young people are often prolific consumers of media, they are frequently exposed to alcohol advertising and marketing, which encourages the consumption of alcohol.
But there is some hope.
The Liquor Amendment Bill aims to amend the Liquor Act of 2003 to prohibit the advertising, promotion or product placement of liquor in all forms of media. The Amendment Bill is at a very early stage in the legislative process, and it is likely to take time before we see any changes to the law (and longer before we see its implementation).
Other legislative changes debated include raising the legal drinking age from 18 to 21 and keeping schools alcohol-free, and more generally to place a moratorium on new liquor licences and stronger enforcement against Liquor Act violations.
South Africa also has a National Drug Master Plan 2019-2024. It was released by the Department of Social Development, and importantly, it recognises addiction as a chronic disease affecting the brain and behaviour.
However, experts say that while it is a great document, the Central Drug Authority which is tasked with implementing the plan, needs more power and resources to implement the plan’s recommendations.
South Africa also has a National Mental Health Policy Framework and Strategic Plan (2023-2030), that was introduced by the Department of Health. Similarly to its previous iteration, the latest plan envisions the integration of mental healthcare into primary healthcare. A key objective of the new plan is to ensure that mental healthcare users have access to care near their places of work. Another aim is to strengthen collaboration between government departments like education and social development to ensure that mental health is incorporated in planning and service development.
However, as it stands, many public healthcare facilities lack mental health professionals, with rural and underserved communities having little to no access to care. Only about 50% of public hospitals offering mental health services have a psychiatrist, while the country has less than one psychologist for every 100 000 people.
Shortages of mental health professionals mean patients often wait months for appointments. For an adolescent or a child who experiences anxiety, depression or suicidal thoughts, these delays can feel unbearable and it is quite possible that they may give up before receiving help. Currently, only one in ten children diagnosed with treatable mental conditions will have access to care.
While South Africa developed extensive legislative and policy frameworks to give effect to the constitutional right to healthcare, including mental healthcare, constitutional promises must make a difference in the lives of people. Unfortunately, millions of people in the country face barriers to mental healthcare, exposing the persistent gap between constitutional promises and lived reality.
When families lack access to counselling, community-based mental health services and early intervention programmes, harmful coping mechanisms continue to be passed down rather than prevented. To achieve the objectives of the Mental Health Policy Framework by 2030 and to catch up with the National Drug Master Plan that lapsed in 2024, stronger political will and meaningful action are urgently required. This is a crisis South Africa can’t evade.
*Mashego is a candidate attorney with SECTION27.
Note: Spotlight is published by SECTION27, but is editorially independent – an independence that the editors guard jealously. Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.
While South Africa was among the first countries to introduce mandatory salt reduction targets in processed foods, health experts warn that hypertension remains a major public health concern. The reason is increasingly clear, the problem is no longer only what is manufactured, but how people eat every day.
As World Salt and Hypertension Awareness Week (4–29 May) approaches, the focus should shift from reformulated products to daily behaviour change. High salt intake causes the body to retain excess fluid, which increases the volume of blood in the system and places greater pressure on the artery walls, directly leading to the development of hypertension.
“While the policy has successfully reduced hidden salt in many staple foods, it has not yet shifted South African taste preferences.,” says Lizeth Kruger, Clinic Executive at Dis-Chem. “We are still reaching for the shaker out of habit, and that’s where the real danger lies.”
Hypertension remains one of South Africa’s leading risk factors for heart disease and stroke, often progressing silently until complications arise. According to the Heart and Stroke Foundation South Africa, more than one in three adults lives with high blood pressure, a ‘silent killer’ that accounts for roughly half of all strokes and 40% of heart attacks in the country.
Kruger says a shift in everyday eating habits could reduce excess salt intake
1. Automatic salt shake
Many people add salt before tasting their food, even when meals have already been seasoned during cooking or processing.
2. Hidden salt in everyday staples
Stock cubes, processed meats, margarine and sauces remain significant sodium sources, especially when used frequently in daily cooking.
3. Convenience meals and takeaways
Ultra-processed foods and fast meals are often high in sodium, with a single serving sometimes approaching or exceeding the recommended daily limit.
4. A conditioned taste for salt
Long-term high-salt diets have shaped taste preferences, making fresh, whole foods seem bland and reinforcing reliance on added seasoning.
5. Unnoticed snack intake
Savoury snacks, biltong and crackers contribute meaningful sodium but are often not counted in daily intake.
Small changes, meaningful impact
Kruger says reducing salt intake is less about strict diets and more about changing repeat behaviours.
“Small, consistent adjustments can make a real difference over time,” she explains.
Tasting food before adding salt is a simple first step, as many meals are already seasoned. Rinsing canned foods such as beans or corn can also reduce sodium content.
Flavour can be enhanced using alternatives such as garlic, lemon juice, herbs and black pepper, while checking labels for lower-sodium options helps guide better choices.
A shared responsibility
“Regulation has laid the foundation, but the final step is ours,” Kruger advises. “By becoming more aware of everyday habits, we can reduce the risk of hypertension, stroke and heart disease in our homes.”
By Gale Shabangu, Chairperson, Hospital Association of South Africa (HASA)
Recently, President Cyril Ramaphosa made an important decision: to pause the promulgation of the National Health Insurance (NHI) Act until the Constitutional Court has ruled on the pending challenges to Parliament’s role in passing the Act. In doing so, he affirmed that due process must guide reform.
It is a reminder that healthcare reform is not a race to the finish line, but a journey that requires careful pacing, broad consultation and respect for the voices of South Africans. Reform at this scale is like tending a vast garden: every seed must be planted with foresight, every path cleared with care, so that the harvest nourishes all.
Families already feel the strain of rising costs – electricity, food, borrowing – and medical contributions that climb steadily. Yet even in this pressure, there is resilience. South Africans have always found ways to adapt, to share, to build together. Healthcare reform must honour that spirit, ensuring affordability is not a privilege but a shared foundation.
The private healthcare system is a necessary and valuable part of the scaffolding of our healthcare system, sustaining capacity that millions rely on. Unfinished reforms, such as risk equalisation, mandatory membership, and base benefit packages, remain like bridges half‑built. Completing them would stabilise participation and strengthen the entire ecosystem.
If private participation declines, demand does not vanish – it shifts. Public hospitals, already carrying immense responsibility, would feel the weight. Yet here lies the opportunity: to recognise that public and private healthcare are not adversaries but allies. The public sector anchors universal access; the private sector provides funded capacity that absorbs demand and sustains innovation. Together, they form a single ecosystem, each part vital to the whole.
Healthcare reform is about weaving our systems together into a fabric strong enough to carry us all.
As the President recently noted, readiness is central to bringing legislation into effect. Readiness is not bureaucracy – it is the heartbeat of reform. It signals that change must be feasible, not forced; sustainable, not symbolic. That is a hopeful message, because it means reform will be paced by practicality, not politics.
The path forward is clear and promising: complete outstanding reforms in medical schemes, strengthen risk pooling, invest in primary care and prevention, and sequence structural changes responsibly. These steps are not obstacles – they are stepping stones toward a healthier, more equitable South Africa.
Healthcare reform is a national undertaking and a shared responsibility. Government, funders, providers, employers and civil society are all custodians of this commitment. What matters now is how we act, with realism, collaboration and a clear focus on strengthening what already works.
Equitable access to quality healthcare is our shared goal. Achieving it requires evidence, readiness, and respect for complementarity. With stability, sustainability and collaboration as our compass, South Africa can build a healthcare system that is workable and inspiring – a system that reflects the resilience, dignity and hope of its people.
Healthcare requires stewardship. With stability, sustainability, and collaboration guiding reform, South Africa can build a system that works for everyone. And with optimism guiding reform, I believe we can build a system that works for everyone – today, tomorrow and for generations to come.
More than 33 000 healthcare workers helped patients more than 20 million times in the Western Cape in the last financial year. (Photo: QuickNews)
21st April 2026
By Christina Pitt
The Western Cape health department is ramping up its workforce with 800 new frontline posts. After years of austerity and with long lists of vacancies, questions now turn to how soon the new posts will translate into staff on the ground.
The Western Cape health department is adding more than 800 staff to frontline and support services in a bid to strengthen a health system in which hiring has been stifled by years of austerity.
Health MEC Mireille Wenger announced a recruitment drive, which includes 316 nurses, 124 doctors and 80 emergency medical personnel. For medical workers to have more time at their patients’ bedsides, she said this plan also targets 38 allied health professionals, such as physiotherapists and dieticians, alongside 278 administrative and management staff.
As it stands, more than 33 000 staff in the province helped patients more than 20 million times in the last year, according to Wenger. For public hospitals and clinics, the news of the new jobs offers some hope that the constant pressure on staff capacity will be relieved.
One example of where the new jobs may make a difference is with surgical backlogs in the province. Of the nearly 100 000 people waiting for surgery in 2025, 87 975 have been waiting for more than a year, while 20 027 have been on the list for more than 60 months. Some of these people entered the system during the height of the Covid-19 pandemic and have been left in limbo through years of budget cycles and hiring freezes.
The budget paradox
While governance has been poor in most of South Africa’s nine provincial health departments, with corruption and looting in Gauteng being a particular concern, the Western Cape health department has received seven consecutive clean audits, maintained stable leadership and largely avoided controversy.
As part of a total R106.8 billion package over three years, the Western Cape health department’s 2026/27 budget is R34.47 billion, which is a 6.25% increase from last year.
When adjusted for inflation, provincial health budgets have been falling for most of the last decade. This has contributed to constrained hiring budgets and exacerbated staff shortages. The tide finally turned with above-inflation increases in the 2025 and 2026 budgets – although belts remain very tight.
Professor Alex van den Heever, Chair of Social Security Systems Administration and Management Studies at the University of the Witwatersrand, said that the Western Cape’s health department is a relatively well-run machine yet is dogged by underfunding.
Understanding this requires a look at how provincial health departments are funded.
While provincial health departments get some funds via sources such as provincial revenue and conditional grants, most of their funding flows from the province’s slice of the national budget. For the 2026/27 financial year, the country’s nine provinces was allocated R810.5 billion.
How much each province gets is determined by the provincial equitable share formula, which has been under review since 2015. The provincial equitable share formula considers factors, such as the size of the school-aged population and the number of people living in poverty. Its health component considers factors like the population without medical aid, adjusted for health risk, medical aid membership, and clinic and hospital visits.
Provinces decide how they divide their share of the budget between their provincial departments.
There are however some issues with the provincial equitable share formula. Firstly, it makes use of certain data from the South African census, which means that the information does not reflect current demographic and service realities, said Van den Heever (the census is conducted only every 10 years). Secondly, the usefulness of the results from the latest census of 2022 is in question because certain data sets, such as income, mortality, fertility, and employment figures, were missing.
As a result, National Treasury has been unable to fully update its calculations to factor in the census 2022 data, contributing to a lag in how population changes are reflected in budget formulas. As far as we can tell, National Treasury has relied on datasets updated at different times in the year, such as Stats SA’s mid-year population estimates, allowing it to phase in changes gradually rather than introduce sudden adjustments.
Broadly, Van den Heever said the result is a system forced to pick up the tab for a population the national budget hasn’t yet acknowledged. Citing an example linked to health, he says the formula ignores patients who travel from other provinces to access specialist care at tertiary hubs like Groote Schuur Hospital in Cape Town.
The claw-back
Some of the vacancies in the Western Cape health department reflect periods when the government cut funding due to broader economic challenges, Doctor Saadiq Kariem, the department’s Chief Operating Officer, told Spotlight.
Indeed, between 2021 and 2024, the province absorbed an R8.4 billion reduction in its budget allocation.
This has forced leadership to make some tough calls, including vacancies for frontline services like health. Kariem explained: “It was a process of consciously delaying the filling of those posts so that we could make up for the loss in funding. Sometimes we, along with local managers, decided to shift posts from a vacancy to another part of the service platform based on service needs and pressures.”
“You know, these are heart wrenching choices because all of those posts are absolutely essential and I know that not filling them will have an impact on the service provision and result in poorer health outcomes. So yes, the austerity measures had a significant impact on the post filling rate,” he added.
According to the health department’s annual report, 3 737 people left the department’s employment in the 2024/2025 financial year. By the end of March 2025, 2 772 funded posts remained vacant.
Nationally, vacancies among nursing staff are particularly acute. As of 2023, across enrolled, auxiliary, community service, professional, primary healthcare and specialist nurses, there were about 14 000 vacant posts across the country.
Sabelo Ntshanga, Western Cape provincial secretary of the Democratic Nursing Organisation of South Africa, said burnout caused by workload is the main driver of attrition.
“The reality is that it’s not being filled quickly. It takes up to a year sometimes while the demand in the communities remains high,” he said. “Burnout is underreported and when the nurses get sick from burnout, that’s another burden on top of the shortage of staff.”
Overall, while the 800 new posts represent a step in the right direction, it appears to be more about holding the line than an actual growth spurt. As Kariem says, it represents an effort to “claw back” towards a stable staffing baseline while attempting to invest in future service capacity.
The red tape
Things won’t change overnight though. Wenger noted in her speech that “it will take time to fill these posts”.
Kariem explained that recruitment follows a multi-stage process as vacancies are advertised, followed by shortlisting and interviews. Final appointments then require approval at different levels of the system, depending on the seniority and specialty of the role. “We see delays throughout the process,” he said. “Once there is the ability to advertise a post, we have to give sufficient time for an advert to run… then for interviews and for permissions to follow.”
This means that even funded posts can remain unfilled for extended periods as they move through administrative and approval processes.
Adding further delays to an already complex process, the National Treasury and the Department of Public Service and Administration (DPSA) advised cost-containment measures in October 2023, which was extended until March 2025. It required additional approvals before recruitment could proceed.
Wenger bemoaned these regulations when it was rolled out. “The DPSA’s recent regulations, intended to slow down recruitment, are doing real harm to large service delivery departments like Health. Staff retire or move on, and yet our system lacks the agility to replace them fast enough. This leaves remaining healthcare workers overburdened, and services strained,” she said.
At the same time, not all vacancies can be filled due to shortages of suitably qualified candidates, particularly specialist nurses. Kariem explained that this in part reflects longer-term gaps in investment in postgraduate training. He said the department is using recent budget increases to strengthen human resources information systems to better identify skills gaps and fill vacancies.
These staffing pressures also affect training and retention. Ntshanga said they limit the system’s ability to release nurses for professional development, constraining career progression and contributing to low morale.
At Groote Schuur Hospital, the department noted that nursing staff shortages have affected multiple units across the hospital in 2024/25, contributing to reduced service capacity.
For Ntshanga, the new posts are a small drop in a very large bucket. “As much as it is a good deed from the department, it doesn’t come close to what we need on the shop floor,” he said.