Photo by Miguel Á. Padriñán: https://www.pexels.com/photo/syringe-and-pills-on-blue-background-3936368/
For oral medications that prevent new HIV infection to be effective, the patient must take certain actions, including attending doctor’s visits every three months and – most importantly – consistency.
These daily oral antiretrovirals, more commonly referred to as PrEP (pre-exposure prophylaxis), such as Truvada®, are extremely effective at HIV prevention, but only if they are taken daily as directed. Truvada’s efficacy is greatly compromised when taken inconsistently.
However, results from a recent Gilead-funded clinical trial (Purpose-2) led by physicians at Emory University and Grady Health System indicate that a twice-yearly injection of Lenacapavir offers a 96% reduced risk of infection overall, making the injection significantly more effective than the daily oral PrEP. The findings were recently published in the New England Journal of Medicine.
“Seeing these high levels of efficacy – at almost 100% – in an injectable that people only have to take every six months is incredible,” says Colleen Kelley, MD, lead author of the study and professor in the School of Medicine at Emory University. “This is a considerable and profound advancement in medicine, especially for people whose circumstances don’t allow them to take a daily oral medication, and for those among populations disproportionately impacted by HIV.”
In the randomised, double-blind, Phase III clinical trial comparing the efficacy of the two medications, 99% of the participants in the Lenacapavir group did not acquire an HIV infection. During the trial, only two participants in the Lenacapavir group, comprised of 2,179 people, acquired HIV. This compares to nine new HIV infections in the Truvada®group, which had 1,086 people. The trial showed that adherence to the injectable was higher than of the daily oral pill.
Kelley adds that while PrEP is incredibly effective at preventing infection, part of what made the injection more effective in the clinical trial was the challenges associated with adherence to a daily oral pill.
“What we see over time is that about half of people who start taking daily oral PrEP stop within a year due to various factors,” says Kelley, referencing healthcare disparities in general. “Having an effective injectable that is only needed twice annually is very significant for people who have trouble accessing healthcare or staying adherent to daily, oral pills.”
The inclusion of racially, ethnically, and gender-diverse participants in the clinical trial was notable because it was representative of populations disproportionately impacted by HIV in real time. For example, the trial groups were comprised of cisgender men and gender-diverse people at 88 sites in Peru, Brazil, Argentina, Mexico, South Africa, Thailand, and the US.
According to the study, the same populations that are disproportionately impacted by HIV are the same populations that have limited access to PrEP – or may have difficulty consistently taking the oral antiretroviral medication – ultimately highlighting the need for more options. The study also indicates that more than half of the new HIV infections nationwide in 2022 were among cisgender gay men, and 70% of those were among Black or Hispanic individuals.
Valeria Cantos, MD, associate professor in the School of Medicine at Emory University, physician at Grady Memorial Hospital, and the principal investigator for the clinical trial at the Grady research site, emphasized the importance of having trials that include populations truly representative of the patients that Grady serves.
“At Grady, our focus is on increased representation of underserved and vulnerable populations, acknowledging and addressing the distrust towards research held by some community members due to prior abuses or neglect of these populations by research institutions in the past,” Cantos says. “Grady is an established, trusted research site because of its commitment to equity.”
At the Grady clinical trial site, medical materials were available in Spanish, and bilingual staff members recruited and enrolled trial participants who only spoke Spanish. Cantos also indicated that the site enrolled participants who are representative of the populations that would benefit the most from Lenacapavir. In addition to Grady, the Hope Clinic and Emory Midtown Hospital were among the 88 sites supporting the clinical trial.
“We are not reaching everyone we need to reach with our current HIV prevention interventions, such as those who are disproportionately impacted by HIV and health care disparities,” says Kelley. “For people that are unable to take the daily oral pills, the injectable agents can really give incredible efficacy and be a game changer in helping them stay HIV negative.”
Since the Phase III clinical trial has been completed and submitted by the FDA for consideration, Kelley is hopeful that Lenacapavir may be approved by 2025 for commercial use.
A University of Minnesota Medical School research team has found that giving iron supplements to children living with human immunodeficiency virus (HIV) in sub-Saharan Africa could be an important first step in optimising brain development.
The study, published in Lancet HIV, demonstrates that iron, while often withheld from children with HIV due to fear of increasing infection risk, is in fact beneficial. This finding paves the way for future research examining iron’s role in neurodevelopmental outcomes in children with HIV.
“With the success and widespread availability of antiretroviral therapy (ART), children with HIV in sub-Saharan Africa are living longer, and optimising their brain development is a new public health imperative,” said Sarah Cusick, PhD, associate professor at the U of M Medical School and a member of the Masonic Institute for the Developing Brain.
Between May 2018 and November 2019, researchers enrolled 200 children with HIV and anaemia who had received ART for at least six months. The study participants were randomly chosen to receive either iron supplements or a placebo for three months. Children who received iron had higher haemoglobin concentrations and better markers of iron nutrition than those who received the placebo. There also was no evidence of increased risk of infection.
According to Dr Cusick, further research is needed to assess brain development and infection risk over a longer period of time.
Rates of HIV and Hepatitis C are “extremely high” among people who inject illicit drugs, according to new research by TB HIV Care. The organisation tested over 1200 injecting drug users in Tshwane, eThekwini, Mashishing and Mbombela (formerly Nelspruit).
In Tshwane 72% tested positive for HIV and nearly 90% had antibodies for hepatitis C virus (HCV), which could indicate past or present infection.
HCV is a blood-borne virus which damages the liver. When left undiagnosed it can be fatal, though it’s usually curable if treated.
Less than half of those who tested positive for HIV in Tshwane were aware of their HIV status. As such they would not have been on treatment and could have been spreading the virus without knowing.
Survey Site
HIV Prevalence among people who inject drugs
Antibodies for Hepatitis C among people who inject drugs
Share of HIV positive people who knew their status
eThekwini
49%
75%
76%
Mashishing
45%
41%
77%
Mbombela
30%
91%
64%
Tshwane
72%
89%
48%
Results of the TB HIV Care survey of four cities.
People who inject drugs (such as heroin) are at a higher risk of contracting HIV and HCV when needles are shared – something which happens because drug users don’t have easy access to new ones.
This has long been a problem in South Africa and appears to be getting worse. Research conducted in eThekwini in 2013 found that 17% of injecting drug users were HIV-positive. According to the new research, a decade later the figure has nearly tripled to 49%.
Professor Harry Hausler, CEO of TB HIV Care and a former technical advisor to the National Department of Health on TB/HIV, believes the main reason for this “massive” uptick in blood-borne diseases among drug users is “the limited access to needle and syringe programs” in the country.
Government ignored its own solution
Research shows overwhelmingly that providing clean needles to drug users reduces the spread of HIV, not only by removing the need to share injecting equipment but often because needle programs offer other services such as health education and condoms.
A large review published in 2017 identified 133 academic studies on needle and syringe programs (commonly known as NSP). The results were “supportive of the effectiveness of NSP in reducing HIV transmission among [people who inject drugs], as well as in reducing HCV infection, although the latter to a lesser extent”.
Yet despite these formal policy commitments, there is virtually no public funding for such interventions.
A person discards used needles in a specialised bin provided by TB HIV Care at a mobile clinic in Wynberg, Cape Town.
One exception is the Pretoria-based Community Oriented Substance Use Program, sponsored by the Tshwane Municipality. It has been left to non-profit groups, such as TB HIV Care, to provide these services. According to Hausler, the organisation currently provides clean needles to nearly 10 000 injecting drug users in Cape Town, Nelson Mandela Bay, eThekwini, Tshwane and Mbombela.
Users access needles from drop-in centres as well as mobile clinics – usually vans that get driven on set days to areas where injecting users congregate. Users discard their old needles in specialised bins provided by TB HIV Care. They will then receive a pack, which includes clean needles, alcohol swabs and sterile water.
Nurses are present at the mobile clinics so users can also get tested for HIV and HCV. They also offer ordinary medical services, such as cleaning and bandaging wounds.
Mobile clinics are also manned by psychosocial and human rights workers, and peer educators (people who were beneficiaries but now work for TB HIV Care) from whom users can get counselling or report abuses.
“We’re not just a needle provision organisation”, says Loraine Moses, who oversees quality standards for the program. “We’re a health services organisation”. Users have to register with peers and get health counselling and education before getting their needles, she says.
Beneficiaries have access to various amenities at TB HIV Care’s drop-in centres, including showers, lounging areas and washing machines.
Anthony (surname withheld), previously a heroin user for 15 years, who now volunteers for TB HIV Care, spoke to GroundUp at a drop-in centre in Cape Town.
“In the beginning, I started experimenting with friends in school [but] after my mother passed away, I found that there are those properties in [heroin] that calm you and numb pain, so that’s when I started to delve [into the drug] more.”
After ending up on the street and becoming “a slave to that drug”, he increasingly wanted to get sober. Fetching needles from a TB HIV Care site, he began speaking with one of the peers. The person told him about TB HIV Care’s opioid agonist program, which helps users to quit or reduce their heroin intake.
Opioid agonists are drugs which block heroin withdrawal. Methadone is the most widely known. Numerous clinical trials show that initiatives which offer methadone to heroin users over an extended period are more effective than rehab programs that force users to quit cold turkey.
Hausler says that TB HIV Care currently provides methadone to over 1100 people. Along with the medicine, they receive counselling and are assisted with finding shelter, and in some cases to reintegrate with their families.
Anthony says he’s been taking methadone since June last year. The program also helped him link up with a shelter and get an ID document so that he could find work.
“Being a client at TB HIV Care has helped me a lot to reintegrate back into society,” he says. “Being on the street, you lose a lot of yourself”.
A notice board at the TB HIV Care drop-in centre in central Cape Town.
Law enforcement continues to confiscate needles
Local governments have assisted TB HIV Care with some of its services. The City of Cape Town provides the HIV tests for use at mobile clinics, according to Hausler.
And yet, not only has the government failed to directly fund the sterile needle programs but in some cases it appears to work against them.
Research carried out by TB HIV Care shows that users frequently have their injecting equipment confiscated by law enforcement officers.
In Tshwane and eThekwini more than half of all people surveyed said that the authorities had seized or destroyed their needles at least once in the previous six months.
Outcome
Mashishing
Mbombela
eThekwini
Tshwane
No
57%
76%
31%
36%
Yes, In the last 6 months
18%
20%
64%
54%
Yes, but not in the last 6 months
25%
4%
5%
10%
Results of survey question: Have you ever had your needles and syringes confiscated or destroyed by a police officer/law enforcement? Source: TB HIV Care
“What’s very frustrating is that there are two arms of government,” says Hausler. “There’s health and then there’s police. And police are confiscating needles and syringes that we’ve been providing to clients – [even though what we’re doing] is a clearly endorsed health intervention.”
Hausler notes that in some cases the organisation has “really good alliances with local police”, but in other cases it is a constant battle.
“There needs to be better mainstreaming of education of officials across all government departments on the … HIV and TB response [plans],” says Hausler. “If people were really sensitised, we would not run up against as many obstacles.”
Asked for comment, Gauteng SAPS spokesperson Lieutenant Colonel Mavela Masondo told GroundUp that “possession of needles is not a criminal offence. Therefore, we cannot arrest a person [for] possession of needles, and neither can we confiscate needles”.
Note: The full report by TB HIV Care, which received assistance from the United States CDC, is not yet publicly available. A 16 page summary of some of the findings can be found here.
Professor Harry Hausler, CEO of TB HIV Care, at his office in Cape Town.
In June, we heard what could be this year’s biggest HIV breakthrough: a twice-yearly injection can prevent HIV infection. Findings from a second large study of the jab has now confirmed that it works. Elri Voigt goes over the new findings and unpacks the licenses that are expected to facilitate the availability of generic versions of the jab in over a hundred countries, including South Africa.
The second of two pivotal studies of a six-monthly HIV prevention injection containing the antiretroviral drug lenacapavir has confirmed that the jab works remarkably well.
The first study, called PURPOSE 1, found that the jab is safe and highly effective at preventing HIV infection in women. The second, called PURPOSE 2, found the same for cisgender men, transgender men, transgender women and non-binary people who have sex with men assigned male at birth.
Interim findings from PURPOSE 2 were presented last week at the HIV Research for Prevention (HIVR4P) conference in Lima, Peru.
The researchers compared the safety and efficacy of lenacapavir injections every six months to a daily HIV prevention pill – a combination of emtricitabine and tenofovir disoproxil fumarate, called F/TDF. The results have not yet been published in a peer reviewed journal, but is expected to be soon, according to Principal Investigator for PURPOSE 2 Dr Colleen Kelley, a professor of medicine at Emory University’s School of Medicine.
In the PURPOSE 1 study, none of the 2 134 people receiving the lenacapavir injection got HIV during the study. In PURPOSE 2, there were two HIV infections among the 2 179 people receiving the injection. These numbers are dramatically better than those for HIV prevention pills and for people in the communities where the study was done who were not receiving prevention injections or pills.
These findings mean the evidence is now in place for the manufacturer, Gilead Sciences, to file with regulatory authorities to register lenacapavir injections for HIV prevention. Such registration is required before the jab can be marketed for prevention. Lenacapavir injections are already registered in some countries as a last resort treatment for HIV, but not yet in South Africa.
“Now that we have a comprehensive dataset across multiple study populations, Gilead will work urgently with regulatory, government, public health and community partners to ensure that, if approved, we can deliver twice-yearly lenacapavir for PrEP worldwide, for all those who want or need PrEP,” Daniel O’Day, the chairperson and Chief Executive Officer of Gilead said in a press release. (PrEP, or pre-exposure prophylaxis, refers to taking antiretrovirals to prevent HIV infection.)
Top line findings
The interim results presented at HIVR4P by Kelley, showed that when compared to the background HIV incidence calculated in the study, lenacapavir reduced HIV infections by 96%. And when compared to the F/TDF prevention pill, the injection reduced HIV infections by 89%.
Among the 3 265 participants enrolled in the study, 11 people acquired HIV- two of the 2 179 people who were assigned to the lenacapavir arm and nine of the 1 086 participants assigned to the prevention pill arm. This translated to HIV incidence of 0.93 per 100 person years in the prevention pill arm compared to only 0.1 per 100 person years in the lenacapavir arm.
This was compared to the background incidence, which was determined when screening eligible participants for HIV. Out of 4 634 people screened for the study, 378 or 8.2% were diagnosed with HIV. Based on further laboratory testing, it was estimated that of those 378 people, 45 or 11.9% recently acquired HIV (classified as being within the last 120 days or so). This latter group provided the background HIV incidence, which was estimated to be 2.37 per 100 person years.
This is a novel study design, Kelley told Spotlight, because this calculation was used to estimate the HIV incidence that would have occurred in a placebo group without actually enrolling a placebo group.
“It’s no longer ethical to have a placebo group in HIV PrEP trials because we know that we have effective PrEP agents,” she said. “Yet, it’s almost essential to have a placebo group when you design a clinical trial so that you can really say how effective your medication, your new agent is [compared] to having nothing.”
When asked at a press conference about the two breakthrough infections in the lenacapavir arm, Kelley said the analysis for this is ongoing and will hopefully be available at a future conference and in a journal soon. She said that the two breakthrough infections in the lenacapavir arm were detected by routine testing during the study.
Principal Investigator for PURPOSE 2 Professor Colleen Kelley at the 5th HIV Research for Prevention Conference in Lima, Peru. (Photo: Nicole Bergman/IAS)
Kelley added that around 90% of participants in the two study arms were able to receive their injection on time. “So, we at least know that the injections were delivered in a timely fashion for almost all participants,” she said.
Whether or not the two infections occurred in people who had received the jabs on time and according to the study protocol will be closely watched as more study details is shared in the coming months.
To be enrolled in the study, participants had to meet several criteria. They had to be older than 16, never received HIV prevention injections before, weigh more than 35kg, have good kidney function, not have been tested for HIV in the last 12 weeks, and had to have been sexually active in the last 12 months.
All study participants were given a pill a day and an injection, those in the lenacapavir arm received two 1.5 ml lenacapavir injections every six months and a daily placebo pill, while those in the prevention pill arm received the daily F/TDF pill and a placebo injection every six months.
The study was conducted across seven countries, with 6 sites located in South Africa and others in Argentina, Brazil, Mexico, Peru, Thailand, and the United States, according to study data on Gilead’s website.
Safety data
Overall, Kelley said lenacapavir was safe and well-tolerated despite some side effects, mainly related to the injections. A total of 43 people dropped out of the study due to side effects.
The most common adverse event in the study was injection site reactions. There were more injection site reactions in the lenacapavir arm compared to the prevention pill arm. 29 people dropped out of the study because of these, 26 in the lenacapavir arm and 3 in the prevention pill arm (people in this study arm received placebo jabs).
The most common injection site reaction were subcutaneous nodules – these are harmless, usually invisible, small lumps under the skin. Nodules occur because lenacapavir is injected under the skin where it forms a drug depot. Injection site reactions and nodule size decreased with subsequent injections. This side effect and trend of decreasing reactions was also noted in the PURPOSE 1 study. Other injection site reactions were pain and erythema which is a type of skin rash.
According to Kelley, there were no serious adverse events related to injection site reactions.
When injection site reactions are excluded, according to Kelley, the other adverse events were similar across both arms, with 74% of participants in each arm experiencing an adverse event. The majority were mild or moderate.
Seven participants in each study arm dropped out due to side effects that weren’t related to injection site reactions. Those who discontinued from the lenacapavir arm will be given prevention pills for a year. This is done to protect these participants, Kelley explained, from potentially acquiring HIV when lenacapavir levels wane, as well as to reduce the risk of potential drug resistance developing.
There were a few serious adverse events, although Kelley told Spotlight she does not currently have any additional information on what these were. She explained that a serious adverse event is generally classified as something like hospitalisation, a life-threatening condition, an important medical event or adverse pregnancy outcome.
“Usually when we look at something like this, we look at the rates compared in the two arms of the study and it was 3% in the LEN [lenacapavir] arm and 4% in the F/TDF arm, so they were equal, essentially the same in both study arms,” Kelly said.
There were six deaths during the study, but none were related to the study drugs.
Next steps for lenacapavir
Now that the interim results have been announced, both studies have been unblinded and entered an open-label phase where participants have the choice of switching to or continuing with the injection.
Professor Linda-Gail Bekker, the Chief Executive Officer at the Desmond Tutu Health Foundation, recently said on a webinar hosted by the South African Health Technologies Advocacy Coalition, that study participants are now able to use the PrEP option they’d prefer – either oral PrEP or the injection. This means all participants will be able to access lenacapavir through the studies if they wanted to use it.
But it will likely be a while before anyone outside of these studies can access lenacapavir as HIV prevention.
“This is an incredible intervention. Now we have to make sure everyone can get it and that’s going to be the most important next step, ensuring that everyone who needs this drug has access,” Kelley told Spotlight.
Gilead’s generic licensing agreement and pricing
What we do know so far about the next steps for lenacapavir is that the process to allow for generic manufacturing has started. This month, Gilead released its voluntary licensing agreements with six generic companies for manufacturing cheaper versions of lenacapavir.
Dr Andrew Gray, a senior lecturer in Pharmacology at the University of KwaZulu-Natal, told Spotlight that no South African firms have been included in the voluntary licenses – four of the generic licensees are in India, one is in Pakistan, and one is in Egypt.
“In essence, they [the generic companies] are allowed to sell their generic versions in a number of identified countries, specified by Gilead,” Gray said. The agreement lists 120 countries, including South Africa.
Gilead itself will also be prioritising the registration of lenacapavir in 18 countries, which it said represent about 70% of the HIV burden in the countries named in the license. The list includes South Africa, Uganda, and Botswana. Gilead says it will start filing for registration with regulatory authorities by the end of the year.
It will be important to see how quickly Gilead seeks regulatory approval for lenacapavir with the South African Health Products Regulatory Authority (SAHPRA), Gray said. Registration with SAHPRA will be required before the injection can be rolled out in South Africa.
In putting together this timeline, we’ve spoken to several well-placed experts, but we stress that this is very much a back-of-the-envelope exercise and far from set in stone. (Infograph: Spotlight)
Some countries won’t be able to procure generics
Gilead received criticism for several omissions from the list of countries that the generic manufacturers can sell to. The US-based HIV advocacy group AIDS Vaccine Advocacy Coalition, among others, pointed out the exclusion of several countries which have high HIV incidence. Some of those countries participated in PURPOSE 2- namely Brazil, Argentina, Mexico and Peru.
A spokesperson from Gilead told Spotlight the manufacturer’s access policy included tailored approaches to ensure rapid and broad access of lenacapavir and it objectively considered the countries where a voluntary licence would provide the most benefit.
“Gilead’s voluntary licence primarily covers countries based on economic need and HIV burden, which are primarily low- and lower-middle income countries. The voluntary licence also covers certain middle-income countries with limited access to healthcare,” the spokesperson said.
Acknowledging that some middle-income countries do have a high HIV burden, Gilead is “exploring several innovative strategies to support access to LEN for PrEP (if approved), including tiered pricing, and are working with payors to establish fast, efficient pathways to help reach people who need or want PrEP”, said the spokesperson.
“Ensuring access in middle-income and upper-middle income countries, including those in Latin America, is a priority for Gilead. Planning for these countries, incorporating input from advocates and global health organizations, is ongoing and updates will be shared as discussions progress,” the spokesperson added. “Additionally, Gilead is committed to ensuring that individuals who participated in the PURPOSE studies have been offered and will be able to stay on open label lenacapavir until it is available in their country.”
The company’s decision to license generic manufacturers directly is at odds with earlier calls from several activist groups and UNAIDS to license via the UN-backed Medicines Patent Pool.
Pricing
It will also be important to see if Gilead will disclose a single exit price for the South African market, according to Gray.
In its press release announcing the voluntary licensing agreement, Gilead stated it will “support low-cost access to the drug in high-incidence, resource-limited countries through a two-part strategy: establishing a robust voluntary licensing program and planning to provide Gilead-supplied product at no profit to Gilead until generic manufacturers are able to fully support demand”.
It is too early in the process to reveal a price for lenacapavir yet, the spokesperson from Gilead told Spotlight.
“While Gilead prepares for global regulatory filings, it is too early to disclose the price of lenacapavir for HIV prevention. Our pledge is to price our medicines to reflect the value they deliver to people, patients, healthcare systems and society. For Gilead-branded lenacapavir, we do plan to price it at no profit to Gilead in 18 select high-incidence, resource-limited countries until generic manufacturers are able to fully support demand,” the spokesperson said.
Spotlight previously reported on research that estimated that if produced at sufficient volumes, the price of lenacapavir could be drastically reduced to levels likely considered affordable by the South African government. For instance, if enough volume was produced to supply 10 million people with PrEP, the price for the injection could be as low as $40 (under R800) per person per year. At the moment, Gilead supplies lenacapavir for HIV treatment in wealthy countries for about $40 000 per person per year.
Gilead’s lenacapavir product will be the first to register in South Africa and will almost certainly be the only lenacapavir product available here for several years – that is because it is expected to take generic manufacturers a few years before they can start producing generic lenacapavir. Based on calculations made for other PrEP products, it seems unlikely that the Department of Health would be willing to procure lenacapavir at a price significantly above R1 000 per person per year. The HIV prevention pill currently costs government around R800 per person per year.
A therapy showing promise to help control tuberculosis (TB) does not interfere with combined antiretroviral therapy (cART), according to research by Texas Biomedical Research Institute (Texas Biomed) which was recently published in JCI Insight.
“This is an important hurdle that this host-directed therapy had to clear in order to help patients battling both HIV and TB,” said study leader Professor Smriti Mehra, PhD of Texas Biomed.
TB is responsible for more than 1.3 million deaths worldwide every year. Dr. Mehra and her team have been investigating a therapy currently used in cancer as a potential treatment for patients with drug-resistant TB and/or comorbid HIV. While many cases of TB can be controlled with months of antibiotics, the infection can return in people who are immunocompromised as a result of HIV. Now that cART is so effective at controlling HIV, a resurging TB infection can often be deadly to those individuals.
Dr Mehra is studying a host-directed therapy that blocks or inhibits an immune system protein naturally found in the body. The protein, called IDO (short for Indoleamine-2,3-dioxygenase), normally suppresses the immune system, preventing it from causing excessive inflammation and organ damage. Inhibiting IDO for short intervals of time has led to more successful cancer treatments. Dr. Mehra’s team has previously shown the same approach improves control of TB in conjunction with antibiotics.
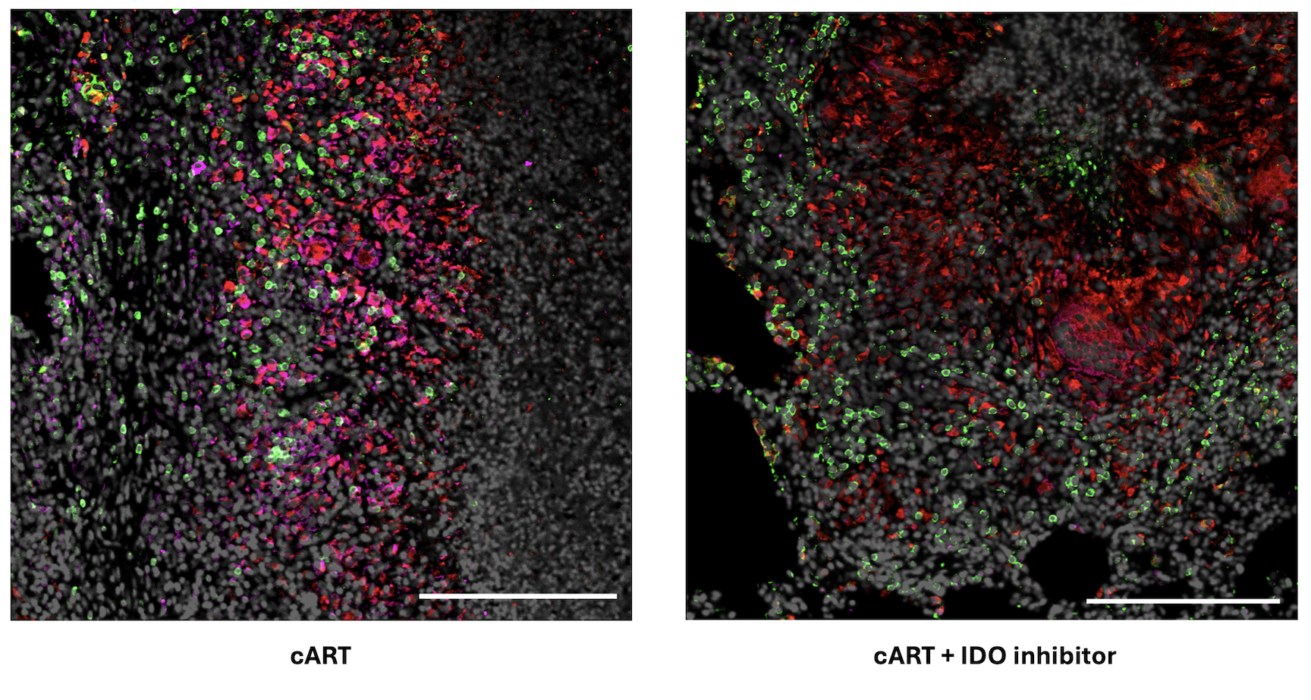
This current study in nonhuman primates with both TB and simian immunodeficiency virus, the nonhuman primate version of HIV, showed the IDO inhibitor does not interfere with cART.
Researchers compare the impacts of cART by itself versus cART plus the IDO inhibitor in lung tissue of nonhuman primates with both TB and SIV. Left: Following just cART, significantly more IDO is detected in pink. Right: With the IDO inhibitor and cART, immune cells recruited to fight bacteria are observed inside the granuloma, a hallmark structure of TB. Specifically, CD4+ T cells are in green and CD68 proteins expressed by macrophages are in red.
“There was no increase in viral load in animals given cART and the IDO inhibitor, compared with animals only given cART, proving the inhibitor is safe to give to patients with HIV,” Dr. Mehra said.
Now that the researchers have shown the inhibitor works well in conjunction with TB antibiotics and with cART separately, they plan to study how it performs when given in conjunction with both antibiotics and cART together. This treatment regimen is standard for patients with both HIV and active TB. Dr. Mehra said that longer-term studies are also needed to confirm there are no unintended side effects.
The IDO inhibitor is already FDA-approved for use in patients with cancer, which shortens the path to potential approval for patients with TB/HIV when compared with developing a brand-new drug.
The African Centre for Disease Control and World Health Organization have raised the alarm following a drastic uptick in mpox cases. This surge is being driven by a new strain of the virus. Elri Voigt reports about what we know so far and potential implications for South Africa.
Mpox, a viral illness first identified in Africa in 1970, made headlines in 2022 when it spread across the globe for the first time. Since then, the outbreak has evolved, with multiple strains of the virus circulating in different countries. A new strain, known as clade Ib, first discovered in the Democratic of the Republic of Congo (DRC), is responsible for much of the most recent surge in mpox cases.
These recent developments are complex, and the situation is likely to change. This was the common theme of a special session on the mpox outbreak during the World Health Organization (WHO) Regional Committee for Africa meeting at the end of August. This session took place two weeks after the WHO declared the outbreak to be a Public Health Emergency of International Concern.
“We don’t have one outbreak. We have multiple outbreaks in one,” Dr Jean Kaseya, the Director General of the African Centre for Disease Control (CDC) remarked.
These outbreaks are caused by different clades of the mpox virus. Clades are a classification system based on the genetic similarities between different strains of a virus, explained Professor Tulio de Oliveira, Director of the Centre for Epidemic Response and Innovation (CERI) at Stellenbosch University (SU). “So, what it means is that when we see a genetic change [in a virus] that’s really visible and that may have impacted it, normally we call it a different clade or genotype or variant,” he said.
This is similar to classifying different strains of SARS-CoV-2 as variants, Dr Duduzile Ndwandwe, a molecular biologist working for Cochrane South Africa, an intramural research unit within the South African Medical Research Council, told Spotlight.
She explained that the different mpox clades and sub-clades have mutated so they have genetic differences but still fall under the umbrella of mpox.
“In a nutshell…it’s just talking about the differences in the genome sequence of the virus, how many mutations [it has] or how big the mutations are in that virus’s strain of mpox,” she said.
‘Jump in evolution’
Dr Aida Sivro, senior scientist at the Centre for the AIDS programme of Research in South Africa (CAPRISA), in 2022 told Spotlight that there are two clades of the mpox virus, which were then referred to as the Central African Clade (clade I) and the West African Clade (clade II).
Since then, clade I went through a big jump in evolution and a sub-clade emerged in the DRC, now called clade Ib, De Oliveira told Spotlight. The previous outbreak in 2022 was mostly driven by another sub-clade called clade IIb.
To further complicate matters, there’s a third strain of the virus also circulating – clade Ia.
At the moment, the DRC accounts for about 90% of mpox cases in the African Region, according to Dr Fiona Braka, the Emergency Response Manager for WHO’s AFRO region. She explained that right now the situation is not fully understood because a lack of diagnostics and testing capabilities is limiting understanding of the true burden of disease.
What we do know, she said, is that there are two distinct outbreaks in the DRC. Based on the information currently available, clade Ia is circulating in regions in the country where mpox is considered endemic and affecting mostly children. While clade Ib is spreading mostly among adults in the eastern provinces of South Kivu and North Kivu.
The clade Ib strain has since spread from the DRC to neighbouring countries Burundi, Rwanda, Uganda and Kenya, according to Braka. Sweden and Thailand have also identified one case each.
As of 1 September, the WHO reported that there have been 3 751 confirmed cases of mpox and 32 deaths across 14 countries in African in 2024 alone. But there are many more suspected cases of mpox that have not been tested.
Implications for South Africa
De Oliveira said at this point, South Africa shouldn’t be overly concerned about mpox, but it should be alert. The best way to do this is to make sure the public know what the symptoms are so they can present for diagnosis and treatment if they suspect they have the virus.
In a similar vein, Ndwandwe said the public shouldn’t panic, but we as a country need to remain vigilant. She added that because clade Ib is spreading on the African continent, there is a risk of it spreading to South Africa through cross-border travel, making it a public health concern.
This year, 24 cases of mpox have been reported in South Africa. Three people have died, while 19 have recovered. Two people are still considered to have active disease, with the most recent case identified in early August.
But this doesn’t necessarily mean there aren’t more cases of mpox in the country. “What we do suspect is that we may have milder cases that are actually not reported,” Nevashan Govender, the operation manager of the Emergency Operations Center at the National Institute for Communicable Diseases (NICD) told Spotlight.
He said so far, all the cases in the country have been caused by clade IIb and no cases of clade Ib have been identified.
A polymerase-chain-reaction (PCR) test is the gold standard test used to determine whether someone has mpox. But genome sequencing would need to be done to identify what clade they have.
Lots of unknowns around new strain
At the moment, there are a lot of unknowns around clade Ib.
What is of concern, according to Braka is the severity of disease seen especially in people who are immunocompromised and in pregnant women and children. Ndwandwe added to this and said there is a concern that clade Ib has higher fatality rates than clade IIb.
De Oliveira cautioned against jumping to conclusions about the severity of this new clade without sufficient data. He said we don’t know for sure yet if clade Ib is causing more severe disease than IIb. What we do know from mpox in general, he said, is that when someone is immunocompromised in some way, they tend to develop more severe symptoms.
Govender echoed De Oliveira’s caution that we don’t yet know enough about clade Ib to say definitively if it is for example more transmissible than other clades
“It’s not to say that it isn’t [more transmissible], but there is just not a lot of evidence stating that it is absolutely true…There’s a lot of knowledge and information gaps,” he said.
The NICD in a recent update also stressed that there are a lot of unknowns about this new strain. It added: “South Africa continues to prioritise enhanced surveillance and raising awareness for mpox.”
The state of vaccines and treatment for mpox
Spotlight reported previously that the smallpox vaccine, which hasn’t been routinely administered in South Africa since the 1980s when smallpox was eradicated, is thought to offer some degree of protection against mpox. However, it’s difficult to predict just how much protection the smallpox vaccine would provide, Sirvo told Spotlight for that previous article.
There are currently three vaccines against mpox that have been approved in some countries, a spokesperson from the vaccine alliance Gavi told Spotlight. These are LC16m8, JYNNEOS and ACAM2000.
LC16m8 is a third-generation small pox vaccine manufactured by KM Biologics. According to WHO, from 2022 it had mainly been used in Japan.
The JYNNEOS vaccine is a third-generation smallpox vaccine, manufactured by Bavarian Nordic, Ndwandwe said, and it was used during the outbreak in 2022. She added that this vaccine is considered the preferred option due to its safety profile and targeted protection against mpox.
ACAM2000 is a second-generation vaccine for smallpox and manufactured by Emergent BioSolutions. But it was only approved by the FDA for use in those at high risk for mpox at the end of August this year. It was not widely used during the 2022 outbreak but was available in some places under a compassionate use protocol (a means of providing medicines or vaccines that have not yet been registered).
In 2022, the Centre for Disease Control (CDC) recommended that JYNNEOS be used as the primary vaccine against mpox because it was associated with fewer side effects than ACAM2000.
While these vaccines exist, it doesn’t mean everyone can access them easily. Countries on the African continent have so far relied on vaccine donations facilitated by the WHO, with an initial 10 000 doses expected to arrive in Africa sometime this month.
Vaccine manufacturers KM Biologics and Bavarian Nordic have submitted proposals to the WHO for emergency use listing (EUL), according to WHO Director-General Dr Tedros Adhanom Ghebreyesus. He added this will allow UNICEF and the vaccine alliance GAVI to buy the vaccines to supply to countries that haven’t issued their own national regulatory approval yet.
The treatment options for mpox are also limited. According to this WHO factsheet on mpox, some antivirals have received emergency use authorisation in some countries and are being evaluated in clinical trials. However, so far there is no proven effective antiviral treatment for mpox.
Tecovirimat, which was approved to treat smallpox, is one of these antivirals being evaluated. According to the CDC, studies in animals have shown the antiviral might help treat mpox but it is still considered an investigational drug for mpox. The drug has been used in some cases of severe mpox.
When asked about this, Ndwandwe agreed more research needs to be conducted to fully understand the evidence around using Tecovirimat. “But what we know now is that the fact that it was authorised for compassionate use, there is some benefit to using that treatment, given that there isn’t any other [treatment,” she said.
Mpox vaccine and treatment availability in South Africa
According to De Oliveira, a small batch of vaccines against mpox and an antiviral drug were made available to South Africa through donations during the outbreak earlier this year.
But the country would need more vaccines if cases increase to protect those at risk for severe disease.
At the moment, South Africa does not have access to any mpox vaccines and has asked for a donation of 40 000 vaccine doses, Foster Mohale, spokesperson for the health department told Spotlight. The country has requested the JYNNEOS vaccine, based on the recommendation by the National Advisory Group on Immunisation.
He added that South Africa’s request to its international partners and the WHO is ongoing support with access to tecovirimat should the need increase. He also requested the WHO’s assistance in procuring the 40 000 vaccine doses to vaccinate high-risk groups if mpox cases increase.
When asked if the department will be entirely reliant on donations of mpox vaccines or would seek to procure its own if cases increase, Mohale said it depends. “South Africa has been in communication with the vaccine manufacturer, Bavarian Nordic, and will consider procurement if needed,” he added.
Because there is a shortage of mpox vaccines and treatment and uncertainty about the sustainability of donated supplies, Ndwandwe said: “Our best defence at this point in time is to prevent [the spread of mpox cases] as much as possible and detect the cases as they start, early on.”
Symptoms of mpox
Govender said the NICD is urging people not to panic but to stay informed on the signs and symptoms of mpox using some of the accurate information available from either the National Department of Health or the NICD.
“The first line of defence for any public health emergency and outbreak comes from when people take initiative to protect themselves,” he said.
Mpox, which is spread by close contact, either household or sexual contact, with someone who has the virus, could initially manifest in flu-like symptoms or the characteristic mpox rash. These include a fever, sore throat, muscle aches, headaches and swollen lymph nodes, according to the WHO factsheet on mpox. The rash starts flat and then becomes a blister filled with fluid, which eventually dries and falls off. The rash can occur on someone’s palms or soles of their feet, face, mouth and throat and sometimes the genital areas.
Children, pregnant women and those who are immunocompromised are most at risk for developing severe disease or dying, the factsheet stated. This includes people living with HIV whose viral load is not well controlled.
Mpox is a virus and as with all viral infections it’s the immune system that fights it off, Ndwandwe explained. However, if someone is immunocompromised, so has a weakened immune system, there is a greater chance that the mpox virus will overtake their immune system and cause severe disease.
This is one of the reasons why we would be concerned about the disease in South Africa, Professor Helen Rees, the Co-Chair of the Incident Management Team (IMT) on mpox, previously told eNCA.
“We have many people living with HIV in the country, many of whom are on antiretroviral therapy, their immune system is good. But we have many others, who don’t know what their status is and might be vulnerable to severe mpox,” she said.
Finalised data published in the New England Journal of Medicine, has confirmed the stunning results of a trial in which a twice-yearly dose of lenacapavir completely prevented HIV infection in a group of adolescent girls and women in South Africa and Uganda.
A major challenge with HIV prophylaxis with cisgender women is adherence and persistence with daily oral regimens. The twice-yearly subcutaneous injection of lenacapavir helps to circumvent these problems by offering extended protection.
Based on the initial results announced by Gilead Sciences on the 20th of June, the PURPOSE 1 phase 3 clinical trial met its key efficacy endpoints of superiority of twice-yearly lenacapavir to once-daily oral (emtricitabine 200mg and tenofovir disoproxil fumarate 300mg; F/TDF) and background HIV incidence. Given the strength of these results, the blinded phase of the trial was halted and open-label lenacapavir was offered to all participants.
The double-blind, randomised, controlled trial recruited 5338 participants who were initially HIV-negative. They were randomised 2:2:1 ratio to receive subcutaneous lenacapavir every 26 weeks, daily oral emtricitabine–tenofovir alafenamide (F/TAF), or daily oral F/TDF (active control); all participants also received the alternate subcutaneous or oral placebo. They compared the efficacy of lenacapavir and F/TAF with F/TDF against the estimated background incidence of HIV infection.
Among the 2134 participants in the lenacapavir group, there were 0 infections (0 per 100 person-years). Meanwhile in the F/TAF group, there were 39 infections among 2136 participants (2.02 per 100 person-years) and 16 infections among the F/TDF group’s 1068 participants (1.69 per 100 person-years).
HIV incidence with lenacapavir was significantly lower than background HIV incidence and than HIV incidence with F/TDF. HIV incidence with F/TAF did not differ significantly from background HIV incidence, and no evidence of a meaningful difference in HIV incidence was observed between F/TAF and F/TDF.
The researchers did note that adherence to F/TAF and F/TDF was low. While no safety concerns were found, injection-site reactions were more common in the lenacapavir group (68.8%) than in the placebo injection group (F/TAF and F/TDF combined) (34.9%); 4 participants in the lenacapavir group (0.2%) discontinued the trial regimen owing to injection-site reactions.
Although South Africa has the largest number of people living with HIV worldwide, strides have been made in controlling the epidemic, especially in the reduction of HIV incidence, testing, and treatment. Researchers from the South African Medical Research Council (SAMRC) and University of KwaZulu-Natal (UKZN) are inching closer to finding the answer to the natural control of HIV infection, leading to improved health outcomes and quality of life amongst South Africans.
According to the latest survey by the Human Sciences Research Council, in 2022, there were approximately 7.8 million people afflicted with HIV in South Africa, the highest absolute number of people living with HIV globally. Yet despite having the largest genetic diversity in the world, African human genome sequences represent the lowest of all the human genomes that have been sequenced worldwide. There is a dire need to leverage genomics to back up and scale targeted intervention programs to put more people living with HIV on effective treatment.
Of particular interest in the global investigations into HIV is “elite controllers” (ECs), a rare group of HIV‐1‐positive individuals whose immune systems can seemingly suppress the infection from developing without taking antiretrovirals (ARVs). For every 200 people living with HIV, around one may be an elite controller (0.5%). In South Africa, with its high rate of HIV infection, the prevalence of ECs also appears to be higher. By “unmasking” the secrets of ECs through research, clues can be revealed, and new therapies potentially developed to benefit broader groups of people living with the disease.
In order to identify the polymorphism and mutations within individuals of African descent, and understand how they are associated with HIV disease progression, Dr Veron Ramsuran, Associate Professor at UKZN, and Prof Thumbi Ndung’u, Director for Basic & Translational Science at the Africa Health Research Institute, joined hands with SAMRC, MGI and local South African clinics in 2019 to take their 20+ years of work in EC research to the next level using whole genome sequencing (WGS).
“The HIV Host Genome project was started at the same time as we launched SAMRC’s African Genomics Centre in Cape Town with the support from MGI,” said project co-investigator Rizwana Mia, also co-founder of the SAMRC Genomics Centre and Senior Program Manager in Precision Medicine at SAMRC. “The partnership saw MGI putting down a high-throughput sequencing workflow and assisted us with the specialised scaled infrastructure design in our lab. This was at a time when there was no real infrastructure for large-scale next generation sequencing in Africa.”
“More importantly, by moving our laboratory workflow to scale, we are hoping to develop genomic research to address this quadruple burden of disease that South Africa faces,” explained Mia. “Our project looks at a unique cohort of patients that have the ability to control the HIV virus to ascertain how disease progresses and the host-directed mechanisms for innate immune control. In addition, we included family sets to help us better understand the relationship between pediatric non-progressors and their parents who are also HIV positive, to uncover and genetic differences that may contribute to host immune control of HIV.”
“We’ve identified new genes and polymorphism that are playing a role with HIV disease through new data generated from Whole Genome Sequencing,” said Dr Veron Ramsuran, principal investigator of the HIV Host Genome project. “Traditionally, there is a list of mutations or genes that are known to associate with HIV, yet they are largely based on studies on Caucasian populations. Our HIV research is adding to the general pool of knowledge pertaining to individuals of African descendent, which will thereby inform new treatment and new vaccine opportunities.”
“What’s important is also understanding how drugs interact with the individual,” added Ramsuran. “We’ve found in the past that certain polymorphism is associated with drug metabolism in genes. Building on this understanding of drugs in combination with the genetics of the individual, we can develop prediction tools to inform clinicians on drug type or dosage depending on the presence of the polymorphism to facilitate a more rapid metabolism of the drug.”
Encouragingly, investigations into Africa’s diseases will continue beyond this point. The HIV Host Genome project has laid the groundwork for the ambitious National 110K Human Genome Project. This large-scale population study will involve 110 000 participants from the South African population, aiming to understand more about of their genomic diversity, address various health challenges, and pave the way for personalized medicine in the country. Furthermore, the data collected will be incorporated into a national population database, enhancing research outcomes and deepening disease understanding for Africa.
Given South Africa’s diverse population, limited human genomics data and significant healthcare burden from diseases such as HIV, understanding pathogenesis and inherent mutations is important for implementing targeted treatments and public health programs. With its lower sequencing cost, high quality data, and efficient all-in-one workflows, MGI’s equipment play an instrumental role , will continue to drive progress in studying rare HIV phenotypes, which holds great promise in advancing the development of targeted interventions and cures– not only for HIV – but many other diseases.
“Looking at the genetic variation and its impact on HIV is a gamechanger, because it will shed light on some of the best immune responses that can be generated against the HIV virus,” stated Prof Thumbi Ndung’u, principal investigator of several of the project’s cohort studies. “And actually, this knowledge will be widely applicable and could have an impact on other diseases – infectious and non-infectious – as well as their drug interventions. It will make sure that Africans, just like everybody else, are at the centre of drug and vaccine development.”
Photo by Miguel Á. Padriñán: https://www.pexels.com/photo/syringe-and-pills-on-blue-background-3936368/
By Nthusang Lefafa
Despite some improvement over the past three years, the North West province continues to experience medicine shortages, according to a survey by a community clinic monitoring initiative. We unpack the latest findings and ask why shortages persist in the province.
Some people in need of HIV or tuberculosis (TB) medicines were sent home empty handed after visiting clinics in the North West. This is according to the latest survey of public healthcare services in the province published by community-led clinic monitoring group Ritshidze. The survey data was collected in April and May this year.
Of the roughly 490 000 people living with HIV in North West, around 380 000 (77%) are on antiretroviral treatment, according to figures from Thembisa, the leading mathematical model of HIV in South Africa. Antiretroviral treatment is recommended for everyone living with the virus.
According to Ritshidze, besides HIV and TB medicines, other commonly reported stockouts at clinic-level include pain medicines (such as Paracetamol and Ibuprofen), cardiac medicines (such as Aspirin), contraceptives, dry stock (gauze, bandages, needles), maternal health medicines, psychiatric medicines, and different vaccines.
Out of the 72 facilities surveyed in the province, medicine stockouts lasting one to three months were reported at 20 and stockouts lasting three to six months were reported at six.
‘Failed to comply’
The North West health department, according to Ritshidze, has failed to comply with national guidelines recommending that people living with HIV should be provided with a three or more month supply of antiretrovirals at a time. They found that 71% of people surveyed in 2024 received antiretroviral refills of three to six months – in each of the previous three years this number was below 30%. There was large differences between districts, with 97% of people surveyed in Bojanala district reporting getting a 3 month supply of ARVs — compared to 37% in Dr Kenneth Kaunda.
Giving people longer antiretroviral refills like this means people do not have to visit health facilities as often to collect their medicines.
Various factors influence giving more people longer antiretroviral refills, Tebogo Lekgethwane, Director of Media and Communications in the province’s health department, told Spotlight.
A crucial factor, he said, is that patients must have a good track record of collecting their medication as well as a history of a documented undetectable viral load. “There’s therefore a criteria for multi-month supply which includes the fact that patients should have been on treatment for six months, they are compliant and clinically stable,” said Lekgethwane.
No “crisis” of medicine shortages
While the year-on-year comparisons should not be overinterpreted – Ritshidze themselves advise caution – the numbers nevertheless provide some indication that when it comes to medicines stockouts things are trending in the right direction. The total number of stockouts in the province reported to Ritshidze plunged from 895 in 2021 to 148 in 2024 – over the same period stockouts of HIV medicines went from 115 to 19 and stockouts of TB medicines from 28 to 7.
Lekgethwane was at pains to point out that Ritshidze’s findings do not necessarily represent the actual picture of the entire province. He said that the department believes that the Ritshidze report is subjective and relies on isolated incidents. These incidents, Lekgethwane said, are often quickly addressed.
“The current provincial medicine availability report shows that medicine availability has stabilised above 80%. As at the end of June 2024, ARV stock was at 89.5%, Expanded Programme on Immunisation and Contraceptives remained above 90%, TB treatment at 79%, Oncology treatment at 81.7% and Diabetes Mellitus at 85.8%. Therefore the province does not have a crisis of medicine shortages,” he said.
Asked what exactly these percentages mean, Lekgethwane said that it indicates the actual medicines stock available in the province in relation to what is required.
A pharmacy expert consulted by Spotlight further explained that the percentage indicates the percentage of medicines on a list or in a class that is available in the province.
The way these numbers are tracked is somewhat tricky. Firstly, if a clinic is supposed to have 10 different HIV medicines in stock, but they only have 8 in stock, then its HIV medicines availability would be at 80% (having a single pack of a medicine counts as having it in stock). When many facilities are considered together, as with an entire province like North West, the key indicator looks at what percentage of those facilities have medicines availability above 90%. We thus understand the figures shared by Lekgethwane to mean that 89.5% of facilities, depots and so on in the province have HIV medicines availability above 90%.
Catching up with payments
Past medicine shortages in the province were partly attributed to companies ceasing delivery of medicine due to non-payment of invoices. While the North West health department was under National Department of Health administration in 2020, the offices at the Mmabatho Medical Depot was raided. The search uncovered a number of unpaid invoices worth millions, some dating back to 2014. One unpaid invoice was for more than R16 million.
Bolstered by a Pharmaceutical Intervention Team to address medicine shortages, Lekgethwane said the department’s payments system is now in top shape.
“Payment of suppliers has remained a priority and the finance unit has assisted the team by making good progress on payments of supplier accounts. The unit continues to investigate and intervene when suppliers indicate their account status to the pharmacies.
“This has led to an increased number of deliveries from suppliers to the depot and increased direct deliveries to pharmacies from contracted companies as well as deliveries of main orders, allocation of orders and emergency orders from the depot to the pharmacies,” he said.
“The Department can confidently confirm that the financial management of pharmaceuticals has been improved resulting in 97% of 2024/2025 accruals being paid and remaining with only two accounts that are on hold. The two accounts that are on hold will only be paid once their compliance requirements are sorted,” said Lekgethwane.
He said that the intervention team has the capacity to assess and intervene, in among others, pharmaceutical supply chain issues, system effectiveness, distribution and delivery processes, storage capacity, human resource capacity and safety issues.
Lekgethwane said the team’s first priority was to assess the Mmabatho Medical Depot before moving onto pharmacies in hospitals and clinics across the province.
Getting medicines to rural areas
While Ritshidze also raised concern around transportation for the delivery of medicines, the department said transportation has never been a challenge.
“There are contracted service providers who deliver to the Mmabatho Medical Depot and the depot delivers to hospitals. Clinics receive their medicine from their referral hospital,” said Lekgethwane.
“However, the department is currently implementing the bulk pharmacies for districts to bring medicines closer to facilities”, he added. A bulk pharmacy is a medicine storage facility which serves as a medical depot. It is situated in the districts and helps with bringing medicines closer to rural areas so that medicines do not have to be transported from major towns.
In this regard, Lekgethwane said the Dr Kenneth District Bulk Pharmacy was recently opened and soon the General De la Rey Bulk Pharmacy will open.
He said the department is confident that the use of these bulk pharmacies will improve medicine storage and distribution capacity.
Shortage of pharmacists and pharmacy assistants
The Ritshidze report found that only 9% of surveyed facilities had a pharmacist and only 18% had a pharmacist assistant. Government regulations state that either pharmacists or pharmacy assistants should be responsible for stock receiving orders and updating the stock visibility system. However, Ritshidze found that enrolled nurses, enrolled nurse assistants, facility managers, and even cleaners acted in that capacity at some clinics.
The province has a 6% vacancy rate for pharmacists while 342 are currently employed, according to the 2024/2025 health department annual performance plan tabled in the North West Provincial Legislature earlier this month. The plan states that the department’s organisational structure makes provision for 10 pharmacists to be appointed in the province for every 100 000 uninsured individuals.
The DA’s Hendriette van Huyssteen says there is a challenge of pharmacists and pharmacy assistants where there are clusters of less than 10 000 uninsured individuals (where one pharmacist would be allocated for 10 000 uninsured individuals) and the clinics servicing them are far removed from one another.
“With the NHI [National Health Insurance] being signed into law, the number of pharmacists will become only a greater challenge. The cost per pharmacist employee stands at R765 000.00 per annum. It is unclear as to where the funding would come from for the remuneration of the additional pharmacists needed under the NHI, as even the NHI Act is unclear in this regard,” she said.
Notwithstanding the issue of budget constraints, the training of more pharmaceutical staff is integral to having fully functional health systems, said Professor Andrew Robinson. He is a deputy dean in the Faculty of Health Sciences at North West University (NWU). He was previously a deputy director general in the North West health department.
“To improve the pharmaceutical skills in the province, the NWU must ensure it aligns its pharmacy training to address the skill needs of the provincial health department to ensure equitable health service delivery to all, which is necessary for successful implementation of the NHI,” he said.
Colourised scanning electron micrograph of HIV (yellow) infecting a human T9 cell (blue). Credit: NIH
An experimental drug originally developed to treat cancer may help clear HIV from infected cells in the brain, according to a new study published in the journal Brain. For the first time, researchers at Tulane University found that a cancer drug significantly reduced levels of SIV, the nonhuman primate equivalent of HIV, in the brain by targeting and depleting certain immune cells that harbour the virus.
This discovery marks a significant step toward eliminating HIV from hard-to-reach reservoirs where the virus evades otherwise effective treatment.
“This research is an important step in tackling brain-related issues caused by HIV, which still affect people even when they are on effective HIV medication,” said lead study author Woong-Ki Kim, PhD, associate director for research at Tulane National Primate Research Center. “By specifically targeting the infected cells in the brain, we may be able to clear the virus from these hidden areas, which has been a major challenge in HIV treatment.”
Antiretroviral therapy (ART) is an essential component of successful HIV treatment, but the virus persists in “viral reservoirs” in the brain, liver, and lymph nodes, where it remains out of reach of ART.
The brain has been a particularly challenging area for treatment due to the blood-brain barrier preventing treatments from reaching the virus. In addition, macrophages are extremely long-lived, making them difficult to eradicate once they become infected.
Infection of macrophages is thought to contribute to neurocognitive dysfunction, experienced by nearly half of those living with HIV. Eradicating the virus from the brain is critical for comprehensive HIV treatment and could significantly improve the quality of life for those with HIV-related neurocognitive problems.
Researchers focused on macrophages, a type of white blood cell that harbours HIV in the brain. By using a small molecule inhibitor to block a receptor that increases in HIV-infected macrophages, the team successfully reduced the viral load in the brain. This approach essentially cleared the virus from brain tissue, providing a potential new treatment avenue for HIV.
The small molecule inhibitor used, BLZ945, has previously been studied for therapeutic use in amyotrophic lateral sclerosis (ALS) and brain cancer, but never before in the context of clearing HIV from the brain.
The study, which took place at the Tulane National Primate Research Center, utilised three groups to model human HIV infection and treatment: an untreated control group, and two groups treated with either a low or high dose of the small molecule inhibitor for 30 days. The high-dose treatment lead to a notable reduction in cells expressing HIV receptor sites, as well as a 95-99% decrease in viral DNA loads in the brain .
In addition to reducing viral loads, the treatment did not significantly impact microglia, the brain’s resident immune cells, which are essential for maintaining a healthy neuroimmune environment. It also did not show signs of liver toxicity at the doses tested.
The next step for the research team is to test this therapy in conjunction with ART to assess its efficacy in a combined treatment approach. This could pave the way for more comprehensive strategies to eradicate HIV from the body entirely.