A more effective vaccine against shingles – an often painful and debilitating condition caused by the same virus that causes chickenpox – will soon be available in South Africa’s private sector. Photo by Mufid Majnun on Unsplash
By Marcus Low and Catherine Tomlinson
Ten years after its launch in the United States, a new, more effective shingles vaccine is finally set to hit the market in South Africa. While the vaccine, called Shingrix, should soon be available at private sector pharmacies, it seems unlikely that it will be provided in the country’s public healthcare system any time soon.
A more effective shingles vaccine is finally set to hit the market in South Africa. Shingles is a common and painful condition that mostly affects the elderly and people with weakened immune systems. It generally appears with a telltale red rash and cluster of red blisters on one side of one’s body, often in a band-like pattern.
“Shingles is pretty awful to get – it’s extremely painful, and some people can get strokes, vision loss, deafness and other horrible manifestations as complications,” infectious disease specialist Professor Jeremy Nel previously told Spotlight. “Shingles really is something to avoid, if at all possible.”
One way to prevent the viral infection, is to get vaccinated against it. Unfortunately, getting hold of shingles vaccines have been a challenge in South Africa.
A vaccine called Zostavax, from the pharmaceutical company MSD, was approved by South Africa’s medicines regulator in 2011, but taken off the market here in 2024. It was only around 50% effective at preventing shingles.
A more effective vaccine, called Shingrix, was introduced by GlaxoSmithKline (GSK) in the United States in 2016. Shingrix is estimated to be around 90% effective in preventing shingles.
But, as Spotlight reported last year, access to Shingrix in South Africa has been severely constrained. That was partly because the vaccine had not been registered by the South African Health Products Regulatory Authority (SAHPRA). Because of this, the only way to get the vaccine in the country was via a Section 21 application – a mechanism in the Medicines Act that allows for the limited importation of unregistered medicines.
That situation changed earlier this month when Shingrix was registered by SAHPRA, thus opening the door for the jab to be imported at scale and sold at pharmacies.
“GSK’s vaccine against shingles (herpes zoster) is expected to be available in South Africa by the end of June 2026,” a GSK spokesperson told Spotlight this week.
It will be launched at a price of R2 783 per dose, including VAT. The total price charged by pharmacies will be slightly higher due to extras like the cost of administration.
Shingrix vaccination requires two doses administered two to six months apart. Since Shingrix is a schedule 4 product, you will need a prescription from a doctor to get it. (You can see more technical details about the vaccine as released by SAHPRA here.)
What about public sector access?
After a vaccine is registered by SAHPRA, the next step on the road to potential public sector access is typically for that vaccine to be considered by the National Advisory Group on Immunisation (NAGI). NAGI then makes a recommendation to the National Department of Health on whether or not the vaccine should be procured for the public sector.
“The decision for the public health sector to offer any vaccine, including Shingrix, is based on the recommendations by NAGI, which considers a number of factors, including availability of [the] registered health product, effectiveness and safety, operational feasibility, alignment with public health priorities, and whether sufficient funding is available,” Foster Mohale, spokesperson for the National Department of Health, told Spotlight.
He said the department has not yet received NAGI’s assessment outcomes and recommendations regarding Shingrix.
It seems likely that an asking price of over R2 000 per dose will be considered unaffordable for the public sector. That said, the price will have to be weighed up against the savings that will result from fewer people developing shingles and requiring treatment.
Spotlight asked GSK whether the company has engaged with the health department regarding the potential supply of Shingrix to the public sector and what price they might offer the government (the department of health often procures medicines at lower prices than what is asked in the private sector).
A GSK spokesperson responded: “As Shingrix is expected to become available in South Africa by the end of June 2026, we anticipate its initial introduction within the private sector. GSK is open to relevant discussions regarding the availability of this vaccine in the public sector.”
What about medical scheme coverage?
For now, it is unclear to what extent medical schemes in South Africa will cover the jab.
“For a vaccine to be considered for funding by the medical scheme, it must be registered with SAHPRA, have a valid NAPPI code, and be commercially available in South Africa,” Dr Noluthando Nematswerani, Chief Clinical Officer at Discovery Health, told Spotlight.
Nematswerani pointed out that Shingrix is not yet commercially available in the country. Spotlight received her comments on 25 June 2026.
When Shingrix does become commercially available, that is to say when it’s available in pharmacies, it seems likely that at least some medical scheme members will be able to access it using their medical savings accounts.
“Discovery Health Medical Scheme funds vaccines that are registered with SAHPRA from the member’s available Medical Savings Account (MSA) on plans that include an MSA benefit,” said Nematswerani.
“Until Shingrix becomes commercially available locally, Discovery Health Medical Scheme members can only access Shingrix via a Section 21 authorisation process. Medicines accessed under Section 21 are treated as a general scheme exclusion and are therefore not funded from scheme benefits,” she said.
Who should get the vaccine?
As we previously reported, South Africa does not have guidelines regarding who should receive the shingles vaccine and when they should receive it. The US Centers for Disease Control and Prevention recommends that all adults over 50 receive the two-dose Shingrix vaccine. They also recommend that people whose immune systems can’t defend their body as effectively as it should, like those living with HIV, should get the vaccine starting from age 19.
In March 2025, the World Health Organization (WHO) recommended that countries where shingles is an important public health problem consider the two-dose shingles vaccine for older adults and people with chronic conditions.
“The vaccine is highly effective and licensed for adults aged 50 years and older, even if they’ve had shingles before,” according to the WHO. It advised countries to look at how much the vaccine costs compared to the benefits before deciding to use it.
The South African Health Products Regulatory Authority, with the South African Pharmacy Council, recently announced what was described as a crackdown on a compounding pharmacy. They allege “critical regulatory non-compliance” in relation to the compounding of unregistered medicines. In his latest Inside The Box column, Dr Andy Gray provides some background to the issues at stake, while recognising that some key elements remain contested.
Until the 20th century, medicines dispensed by pharmacists were all compounded (mixed) from raw ingredients, most of which were inorganic chemicals and herbal products. The gilded majolica jars displayed in pharmacies and museums depict the names of those common ingredients, often in Latin. Hence, a jar labelled as “Paraf mol alb” would contain “paraffinum molle album”, or white soft paraffin (white petroleum jelly), more commonly known as Vaseline.
The market for finished pharmaceutical products, in the form of modern tablets, capsules and the like, has grown dramatically over the last century. Even so, the need for the preparation of medicines in a pharmacy, from either raw ingredients or existing products, has not entirely disappeared.
#InsideTheBox is a column by Dr Andy Gray, a pharmaceutical sciences expert at the University of KwaZulu-Natal and Co-Director of the WHO Collaborating Centre on Pharmaceutical Policy and Evidence Based Practice. (Photo: Supplied)
There has always been a need for the preparation of particular products for individual patients in cases where a commercial product does not exist or is not suitable. For example, a pharmacist may be asked to produce an eye drop when no commercial products exist, using an injection as the starting material. Similarly, where a patient is unable to swallow tablets or capsules, an oral liquid preparation may be compounded. In many cases, the preparation is done extemporaneously, meaning that it is done specifically for that patient at a point in time. Such medicines are compounded by pharmacists as part of their usual professional practice in community and hospital pharmacies.
Exceptions, limitations and contestation
Modern medicines regulatory practice is based on the concept of registration or marketing authorisation. This is where a manufacturer is required to provide evidence to the national medicines regulatory authority of the quality, safety and efficacy of a medicine, before it can be sold. However, an exception has been created, allowing for compounding of medicines. In the South African medicines legislation, this is provided by section 14(4) of the Medicines and Related Substances Act (Act 101 of 1965).
The usual approach is described in section 14(1) of the Act, which states that “no person shall sell any medicine … which is subject to registration by virtue of a declaration published in terms of subsection (2) unless it is registered”. The declaration in this regard refers to the call-up notices issued for different pharmacological classifications of medicines since 1967, when the Act came into operation. All pharmacological classifications have now been made subject to registration.
The exception is provided by section 14(4), which states that subsection 14(1) will not apply when a medicine is “compounded in the course of carrying on his or her professional activities by a pharmacist”. A similar exception applies to licensed dispensing and compounding practitioners and veterinarians. Two scenarios are envisaged: compounding a preparation in accordance with a prescription for a particular patient, or compounding by a pharmacist for the retail trade.
However, there are three critical additional restrictions: a compounded medicines shall “not contain any component the sale of which is prohibited by this Act or any component in respect of which an application for registration has been rejected”, the compounded medicine “is not or has not been advertised”, and the “the active components of such medicine appear in another medicine which has been registered”. Thus, unless declared undesirable or never before registered, an active ingredient may be compounded and sold without being registered. A compounded medicine may also not be advertised to the public or to health professionals.
Further details were provided by the General Regulations to the Medicines and Related Substances Act, which were published in 2017. The initial version of those regulations added some additional restrictions, for example restricting the quantity to be compounded to the “quantity that is intended to be used by a patient for not more than 30 consecutive days from the date of compounding”. More importantly, sub-regulation 3(3)(a) prohibited compounding that was intended “to circumvent the provisions of section 14 of the Act”, the requirement for registration.
Legal challenge
In December 2021, the North Gauteng High Court in Pretoria ruled in a case brought by The Association of Compounding Pharmacists of South Africa, challenging the regulations. While noting that “[w]hat constitutes pharmacy compounding is not well defined”, Judge Norman Manoim ordered that the regulations be redrafted and that a draft guideline on good compounding practice be published. In particular, the judgment recognised the need to clarify what was needed for “anticipatory compounding”, where medicines were compounded in anticipation of a prescription or for sale by a pharmacist.
In accordance with the court judgment, amended regulations were published for comment and finalised in 2022, deleting sub-regulation 3(3)(a), and recognising that a pharmacist could “based on the amount of medicine compounded previously for a particular period, compound such medicine in anticipation of supply thereof within such particular period”. Lastly, the regulations required that draft guidelines on good compounding practice be published within 6 months, for public comment. These draft guidelines were published for comment in June 2023, but have not been issued in final form. The draft guidelines are no longer accessible on the South African Health Products Regulatory Authority (SAHPRA) website.
Compounding pharmacies
While the extemporaneous compounding of medicines for individual patients is routinely performed in most community and hospital pharmacies, “anticipatory compounding” has emerged as a speciality practice.
Compounding pharmacies are not recognised as a specific category of pharmacies licensed by the Department of Health and recorded as such by the South African Pharmacy Council (SAPC). The current regulations to the Pharmacy Act only recognise community, institutional (hospital), wholesale, manufacturing and consultant pharmacies. The services that each category of pharmacy can deliver are regulated, with both community and institutional pharmacies enabled to perform “compounding, manipulation or preparation of any medicine or scheduled substance”. Specialist compounding pharmacies are thus licensed as community pharmacies.
SAHPRA licenses manufacturers and wholesalers of medicines, not community pharmacies. Section 22C(1)(b) of the Medicines and Related Substances Act states that the Authority “may … issue to a … manufacturer, wholesaler or distributor of a medicine … a licence to manufacture, import, export, act as a wholesaler of or distribute, as the case may be, such medicine … upon such conditions as to the application of such acceptable quality assurance principles and good manufacturing and distribution practices as the Authority may determine”.
Whether a compounding pharmacy, licensed as a community pharmacy, can import active pharmaceutical ingredients (APIs) for the purposes of compounding, is contested. It is the API which is responsible for the desired medicinal effect but can also be the cause of adverse events. Inactive excipients are added to produce the final dosage form administered to patients.
The question of quality
As was outlined in a previous column in this series, patients are assured of the quality of medicines on the South African market by virtue of their registration by SAHPRA and compliance with Good Manufacturing Practice (GMP) standards by licensed manufacturers. Compounded medicines are an exception to the rule – they are unregistered, and their preparation is not subject to GMP.
In the case of medicines compounded for individual patients, the risk is more manageable. Where larger quantities are prepared in anticipation of demand, and in particular where sterile preparations such as injections are made, the risks may be greater.
Equally, there is a need to ensure that APIs used for manufacturing or compounding medicines are of acceptable quality. A draft guideline on post-importation testing, published by SAHPRA for comment in May 2026, applies to all imported APIs.
Following a major incident in the United States, where contaminated compounded corticosteroid injections resulted in a number of serious fungal infections, US law was amended in 2013 to create a new category of outsourcing facilities regulated by the Food and Drug Administration (FDA), not by state pharmacy boards. State pharmacy boards were not considered to have the capacity to effectively regulate large scale compounding, especially for higher risk sterile preparations.
In South Africa, while the Good Pharmacy Practice standards issued by the SAPC cover the usual services delivered by community and hospital pharmacies, they are insufficient to cover larger scale anticipatory compounding or outsourcing services.
Ongoing contestation
Existing South African law may well be deficient in the way in which it regulates compounding pharmacies. How the current legal provisions are applied and interpreted is contested and will be the subject of a number of court challenges.
Patient safety must remain the key animating feature of any future regulatory process that is fit for purpose and effective.
*Dr Gray is a Senior Lecturer at the University of KwaZulu-Natal and Co-Director of the WHO Collaborating Centre on Pharmaceutical Policy and Evidence Based Practice. This is part of a series of columns he is writing for Spotlight.
Disclosure: Gray serves on three technical advisory committees at the South African Health Products Regulatory Authority.
Note: Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.
Lenacapavir is injected just under the skin, typically in the stomach area, where it forms a small depot that very slowly releases the drug over time. Photo by Elen Sher on Unsplash
By Amy Green
With a new six-monthly injection, South Africa last week launched the most promising new HIV prevention tool in years, but much of the infrastructure that made HIV prevention services accessible to high-risk groups has been dismantled over the last year. Spotlight asks whether we can successfully deliver this breakthrough technology without the trusted pathways decimated by cuts to aid from the United States.
When 29-year-old Keegan Daniels* visited a public hospital outside Cape Town earlier this year to be placed on medication to prevent HIV infection, he says he wasn’t sure what to expect, but it definitely wasn’t to be reprimanded, lectured and told that anal sex “is abnormal”.
Oral pre-exposure prophylaxis (oral PrEP) refers to antiretroviral tablets taken to prevent HIV infection. When used as prescribed, oral PrEP has been shown to reduce the risk of HIV infection from sex, including in men who have sex with men (MSM), by approximately 99%, according to a 2022 meta-analysis.
During the short consultation, Keegan claims the doctor, who appeared unfamiliar with prescribing PrEP, chastised him for addressing him as “sir” rather than “doctor”, and made assumptions about his sexual orientation.
“I am gay, but when he told me I was ‘homosexual’ instead of asking me, I felt as if I was there to be shamed instead of helped,” says Keegan, who identifies as a gay man.
Keegan tells Spotlight that he sought out oral PrEP after an experience that left him worried about his HIV risk. As a man who has sex with other men, he is also part of a population disproportionately affected by HIV. According to the World Health Organisation (WHO), men who have sex with one another are up to 26 times more likely to acquire HIV than the general population. This is largely driven by biological risk factors associated with anal sex combined with other social and structural vulnerabilities faced by this group.
The consultation became increasingly uncomfortable, Keegan says, when the doctor began discussing the importance of marriage as a method to prevent HIV and the risks associated with anal sex.
“He may not have meant it that way, but it felt like a judgement,” Keegan says.
His experience highlights long-standing concerns from activists, researchers and healthcare providers about discrimination experienced by members of marginal groups at public sector clinics. One solution to such discrimination has been to create special clinics for groups like men who have sex with men where they could access HIV treatment, prevention, and other services without judgment. But this alternative was dealt a major blow last year with the closure of many such specialised programmes funded through the United States President’s Emergency Plan for AIDS Relief (PEPFAR).
There are now concerns that the destruction of such specialised services could limit the reach and impact of the latest addition to South Africa’s HIV prevention toolkit. Last Friday, South Africa officially launched its public sector rollout of an injection that provides six months of protection against HIV infection at a time. The jab, a form of injectable PrEP, contains the antiretroviral drug lenacapavir. (See Spotlight’s special briefing on lenacapavir for more detail.)
PrEP in South Africa
The recent history is worth revisiting. South Africa became the first country in Africa to start rolling out oral PrEP back in 2016. Initially, the strategic focus of the programme was on “key populations”, groups that bear a disproportionate burden of HIV infection and who are at the highest risk of new infections. Key populations include sex workers, men who have sex with men, transgender persons, people who inject drugs and people in prisons or other similarly closed settings.
UNAIDS estimates that in Sub-Saharan Africa, key populations and their sexual partners accounted for roughly 39% of new HIV infections in 2020, despite representing a much smaller proportion of the population.
“PrEP is central to South Africa’s HIV response because treatment alone will not end the epidemic,” says National Department of Health spokesperson Foster Mohale.
“South Africa still has a very large HIV burden, with millions living with HIV and substantial ongoing new infections, especially among adolescent girls and young women, key populations, and pregnant and postpartum women,” he adds.
“After a decade, South Africa is home to the largest and most successful PrEP programme in the world, even though it has not delivered the impact we wanted,” says Mitchell Warren. He is the executive director of AVAC, a US-based advocacy organisation, largely focussed on HIV prevention, that does extensive work in South Africa. Warren’s point about the impact not being what we wanted, refers to the fact that, comparatively large as our PrEP programme is, uptake has been much lower than what was hoped.
He says that the oral PrEP programme started to gain more traction around the time of the COVID-19 pandemic. “A lot of that was thanks to PEPFAR, through the support around programmatic delivery of PrEP and most notably the initiatives designed for key populations,” Warren says.
Making sense of the numbers
The most recent figures show that over 2.1 million individuals have been initiated on oral PrEP in South Africa, Mohale tells Spotlight.
However, most of these are considered to be people restarting PrEP and not new users, according to Professor Francois Venter, Executive Director of Ezintsha at Wits. He says that the real figure for overall PrEP users is closer to 500 000.
This view is roughly in line with estimates from Thembisa, the leading mathematical model of HIV in South Africa. The two types of indicators here are important to distinguish. Since many people start and then stop taking PrEP, looking just at PrEP initiations provides a very limited view. This is why Thembisa also includes estimates of the total number of people taking PrEP at specific points in time (technically the middle of each calendar year).
According to Thembisa, just over 350 000 people were taking PrEP as of mid-2025 – a slight decline compared to the 2024 number. Prior to this decline, the programme had been showing solid year-on-year growth.
Aid setback
When trying to understand why PrEP numbers stopped growing, and instead declined slightly in 2025, one very likely culprit stands out – aid cuts.
Venter argues that the relative success of South Africa’s PrEP programme was underpinned by an ecosystem of specialised key population services, most of which were funded by the United States Agency for International Development (USAID) under PEPFAR.
“Most of these 500 000 estimated PrEP users in South Africa started in these key populations programmes,” says Venter.
“But one sudden decision by the Trump administration essentially destroyed PrEP in South Africa, and because South Africa is so significant in terms of HIV incidence and prevalence, it also threw the global PrEP response into chaos.”
In February 2025, the Trump administration terminated large numbers of USAID-funded health projects and massively reduced funding for many HIV programmes. While a limited waiver allowed some treatment services to continue, HIV prevention activities were largely excluded. Programmes focussed on helping people avoid HIV infection, including many PrEP services, were among the hardest hit.
The cuts all but decimated specialised clinics and services for key populations in the country, according to Venter.
“The dismantling of the key population programme is an absolute disaster for PrEP. Clinics gone, just shut down. About 80% of the specialised key population services were funded by USAID,” says Venter.
Despite the health department’s assurances that these PrEP users from key populations will be integrated into the normal existing services in our healthcare system, he says “there is absolutely no evidence that this has happened”. Venter adds: “I suspect the vast majority stopped taking PrEP.”
Over 8 000 PEPFAR-funded staff involved in HIV programmes lost their jobs, important HIV prevention research projects were halted, civil society organisations were forced to retrench staff and attenuate their outreach programmes and, most alarmingly, thousands of PrEP users were lost in the system, according to Eugene van Rooyen, who is the Legal and Policy Advisor for the Sex Workers Education and Advocacy Taskforce (SWEAT).
“It is impossible to know exactly how many of these clients stopped taking PrEP. We did a survey late last year [2025] that showed that less than half of the former users of key populations services in Cape Town were still on treatment,” he says.
The SWEAT survey aimed to find out what happened to these individuals after the services stopped but did not disaggregate PrEP users from people on antiretroviral treatment.
“Regardless, the results are a tragedy. All those years of gaining trust in these communities, and all the millions invested in the PrEP programme, all down the drain,” Van Rooyen says.
The concerns raised by activists are echoed in findings from Ritshidze, South Africa’s largest community-led monitoring programme. Ritshidze, which surveys thousands of public healthcare users annually and monitors more than 400 healthcare facilities across the country, was established to track the quality of HIV and TB services from the perspective of people using them.
Its most recent report found early signs that the PEPFAR funding cuts may already be affecting access to HIV services. Approximately, 56% (189 out of 340) of facility staff surveyed reported reduced capacity after the PEPFAR withdrawal while reports of stigma and discrimination remained common.
Vertical services vs integration
While Keegan says he experienced stigma and challenges accessing PrEP through the general public sector, his older cousin Jason* describes an entirely different experience when he first started PrEP.
“I started PrEP three years ago at the Wits RHI Transgender Clinic in Bellville [Cape Town], it was easy, comfortable, safe. I felt empowered and had zero problems getting onto PrEP there,” says Jason, who is also a part of the MSM community. Although he doesn’t identify as a transgender person, he says the clinic staff welcomed him and his peers. It was a space that removed many of the barriers key populations face when accessing healthcare. But it was also one of the many clinics that ceased to exist after the funding cuts.
The National Department of Health maintains that “the PrEP programme has not collapsed, because it is anchored in the public health system”. Their argument has broadly been that people who went to specialist clinics should be redirected to public sector clinics. To address discrimination, provincial health departments have run several programmes aimed at sensitising clinic staff to the needs of key populations. This has included staff involved in administering the lenacapavir injection.
As for PrEP, Mohale says South Africa made “a deliberate decision to move PrEP out of the early pilots that commenced in 2016 into the broader public health system at scale”. Today, he says, “approximately 99% of public primary healthcare facilities offer oral PrEP”.
“The key success factor is that PrEP is not a vertical programme, it is integrated into primary healthcare and combination prevention,” says Mohale.
What all this means for lenacapavir
“This is not merely a medical advance. It is a practical intervention that can transform lives. It reduces barriers to adherence. It expands choice. It strengthens dignity. And it empowers people to take control of their health and their future,” President Cyril Ramaphosa said in a prepared speech at the launch of South Africa’s lenacapavir rollout last Friday.
The first phase of the rollout will see lenacapavir available in 360 health facilities across the country. This is roughly 10% of the country’s public sector clinics. While it remains to be seen how high demand will be, there are clearly limits to what level of demand can be accommodated. Initially, South Africa will only have enough lenacapavir for around half-a-million people. This is partly why specific groups like young women and girls, MSM, and sex workers are being prioritised.
Thus, in the fact that there is some prioritisation of specific groups the lenacapavir rollout partially mirrors the rollout of oral PrEP a decade ago. But unlike the initial oral PrEP rollout, specialised key population clinics will play little part.
Mohale explains that the integration of services is the philosophy underlining the rollout of the lenacapavir programme, a philosophy he says is fundamental to the success of PrEP in South Africa.
Venter disagrees: “Key population programmes exist for a reason – they work. People need verticalised services.”
Meanwhile, a statement released by a coalition of several civil society groups criticised the rollout plan of being “unambitious, low-scale, and in danger of being more about pomp than public health impact”.
“A programme that does not adequately prioritise key and vulnerable populations such as sex workers, outside of clinics, will leave those most in need of HIV prevention services, even more vulnerable,” Katlego Rasebitse, from SISONKE Movement, says in the statement.
A rollout beyond clinics?
The introduction of lenacapavir has mostly been received with resounding optimism. But some have also raised concerns and have cautioned that the rollout won’t be without obstacles.
“Getting hundreds of thousands of otherwise healthy individuals to come to public health facilities to get lenacapavir is not a likely pathway to scale. We have got to be very clear, dropping lenacapavir into clinics is not a pathway to success,” says Warren, who has also praised South Africa and the National Department of Health for launching the national injectable PrEP programme.
“There are many innovative ways to deliver PrEP outside of facilities, like mobile clinics, outreach services, among others. There is a lot of work around implementation science being done in South Africa that can be used to make this programme ambitious enough to be a global PrEP success story,” he says.
There are several implementation science research projects underway looking at innovative ways of delivering PrEP, including lenacapavir, outside of traditional settings.
Unitaid has launched a project, valued at US$22.5 million, that “will support South Africa to expand access to lenacapavir through innovative, community-based delivery and demand-generation approaches that complement national rollout through public health facilities”.
Largely focussed on reaching key populations, the project aims to generate real-word evidence on these innovative delivery models, evidence that “will help inform national scale-up”. It is exploring a range of delivery settings including pharmacies, mobile clinics and even hair salons.
‘I was trying to do the right thing’
When Keegan walked out of the doctor’s consultation room that day in April, he says that he felt angry, self-conscious and deeply uncomfortable. Instead of continuing the process to get onto PrEP, he left the hospital.
“I have been through a lot of trauma in my life, a lot of stigma because of my orientation. It took a lot for me to start healing. This experience brought me back to that space of self-doubt. I left there feeling like I’m nothing. I’m a piece of dirt,” he says.
His cousin, Jason, had an appointment the next day, at the same place for the same reason. Since the closure of the clinic in Belville, Jason had chosen to pay for his monthly PrEP pills himself, instead of facing the challenges anticipated in a regular public health facility, but he says this route had stopped being financially feasible.
“By that time, I had cooled down and Jason convinced me to go back to the hospital with him,” says Keegan.
After the mandatory blood draws and HIV testing, he filled his prescription at the hospital pharmacy.
As Keegan sat down, he says he showed Jason the box.
“That isn’t PrEP Keegan, those are pills for HIV positive people,” said Jason. He had experience with oral PrEP and recognised the ARVs by the packaging. His partner, living with HIV, uses the same medication.
After a protracted process, several conversations with nurses and the doctor. Keegan says he eventually received the correct medication. He told Spotlight that, even though he is educated and informed, he only started PrEP “through luck”. There are many other people from marginalised groups “who probably won’t have my luck”.
“What will they do?” he asked.
“I was trying to do the right thing. The responsible thing for my health. In the end, I didn’t feel like I was doing the right thing. I felt like I was being punished.”
Despite this experience, both Keegan and Jason are excited at the prospect of the twice-yearly injectable PrEP.
“You won’t catch me coming back to this hospital, but I would find a clinic that treats people well. Even if I have to drive for hours, I would, just to have this injection every six months, instead of drinking pills every day,” Keegan says.
* Names have been changed to protect the identity of sources
Republished from Spotlight under a Creative Commons licence.
Specially trained pharmacists will soon be allowed to dispense antiretrovirals without a doctor’s script. Photo by National Cancer Institute on Unsplash
By Catherine Tomlinson
A Supreme Court of Appeal ruling in October 2025 cleared the way for specially trained and permitted pharmacists to dispense antiretroviral medicines without a doctor’s script. Seven months later, no pharmacists are yet providing these services. Spotlight explores the reasons for the delay.
After a three-and a half year court battle between a group of private doctors and the South African Pharmacy Council (SAPC), the Supreme Court of Appeal (SCA) cleared the way for the SAPC to implement pharmacist-initiated management of antiretroviral treatment (PIMART) in October 2025.
The SAPC welcomed the ruling with a bullish press conference promising rapid implementation of PIMART. “The South African Pharmacy Council, together with stakeholders and the Department of Health, will work with speed to ensure that PIMART-trained pharmacists join other primary healthcare practitioners in providing primary care in relation to HIV and Aids,” said Mogologolo Phasha, president of the SAPC, at the time.
Vincent Tlala, CEO and Registrar of the SAPC, also in October 2025, said that the SAPC aimed to issue an e-note inviting pharmacists to apply for the PIMART permits in November. However, seven months later, this has still not happened and no pharmacists in the country are yet permitted to provide PIMART services.
What is PIMART?
PIMART stands for pharmacist-initiated management of antiretroviral treatment. It is a form of task-shifting that allows pharmacists to provide some limited HIV services that are currently only provided by doctors and nurses. The programme seeks to better utilise pharmacists in the country’s HIV response and relieve some of the burden on overcrowded and under resourced public clinics. It will also offer a route into treatment for people who are not willing or able to visit clinics.
It is intended that, under the PIMART programme, pharmacists that have completed a dedicated training programme and have received a special permit from the Director-General of Health will be authorised to provide first-line antiretroviral treatment to people with uncomplicated HIV without a doctor’s script. They will also be allowed to dispense HIV prevention medicines without a doctor’s script – this includes both pre-exposure prophylaxis (PrEP) and post-exposure prophylaxis (PEP). PrEP is taken prior to sex to prevent potential infection while PEP is taken shortly after a possible HIV exposure to prevent infection.
Why is PIMART needed?
PIMART was proposed by the SAPC in response to a request from the health department for the SAPC to design an intervention to enable pharmacists to take on a greater role in the country’s HIV response.
South Africa has adopted the UNAIDS 95-95-95 targets that aim to ensure that 95% of people living with HIV know their status, 95% of people diagnosed with HIV are on treatment, and 95% of people on treatment are virally suppressed (and therefore cannot transmit HIV onwards).
According to new estimates from Thembisa, the leading mathematical model of South Africa’s HIV epidemic, 7.9 million people are living with HIV in South Africa. Ninety six percent of people living with HIV know their status, yet only 82% of people who know they are HIV positive are on antiretroviral treatment.
While South Africa’s health system should be commended for the fact that around 6.2 million people are taking HIV treatment, it is concerning that 1.7 million people living with HIV are not yet on treatment. In recognition of this problem, the health department has launched the “Close the Gap” campaign.
The thinking behind PIMART is that pharmacies can help close the gap by providing an important third option to people who are disinclined or unable to access HIV treatment from public clinics or private sector doctors.
More urgent than ever following US funding cuts
While PIMART was always intended to help identify patients falling through the gaps between South Africa’s public and private health sectors and to link them to care, the need for this third option is now more urgent than ever. US funding cuts over the last 15 months or so have led to the closure of many NGO-run clinics that previously provided HIV treatment and prevention services to populations at high risk of HIV who often face stigma at traditional health facilities. These groups include sex workers, men who have sex with men, and people who inject drugs.
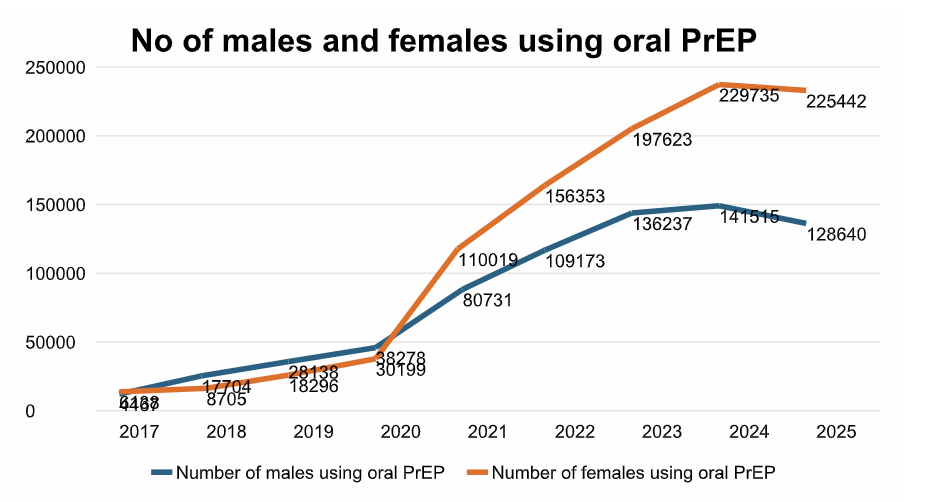
In addition to expanding access to HIV treatment, PIMART aims to increase access to PrEP and PEP to prevent new HIV infections. While the full impact of US funding cuts on these services remains unclear, the cuts likely contributed to the slight decline in PrEP use in South Africa seen in 2025, following seven years of steady growth in PrEP uptake.
Graph by Spotlight. Data courtesy of the Thembisa model.
Finger pointing and lack of accountability
Seven months after the Supreme Court of Appeal ruled that the SAPC could implement PIMART and the SAPC promised to move rapidly in implementing PIMART, pharmacists have still not been invited to apply for permits and no PIMART permits have yet been issued to pharmacists.
When asked why the programme remains unimplemented, the SAPC pointed to the Southern African HIV Clinicians Society’s (SAHCS) PIMART training course as the cause of the delay.
SAHCS is the only entity in the country providing PIMART training to pharmacists. In October 2025, Mokoena said several groups had expressed interest in becoming accredited to provide PIMART training. However, on 14 May 2026, Tlala told Spotlight: “While we have invited existing providers of pharmacy education in South Africa to offer (the course), the South African Pharmacy Council is yet to receive applications for the accreditation of the PIMART supplementary training course.”
He added: “Currently, the Southern African HIV Clinicians Society are the only approved provider for the PIMART short course.”
So, what’s going on with SAHCS’ PIMART training?
PIMART used to be on a very different timeline before it got tangled up in the court processes that led to the October 2025 SCA judgment. Back in July 2021, Spotlight reported that the launch of PIMART was imminent, and indeed, that was roughly the timeline the SAHCS training had been working toward.
In fact, the SAHCS has offered a PIMART training course for pharmacists that want to provide PIMART services since 2019. Professor Natalie Shellack, chairperson of the SAPC Education Committee, said in October 2025 that this course was developed jointly by SAHCS and SAPC.
Over a thousand pharmacists have completed SAHCS’s original PIMART training course as continuous professional development (CPD) training. But after the October 2025 SCA ruling, Lizeth Kruger, Dischem’s Clinical Executive, told Spotlight that due to the time lapse between the initial training and court ruling, Dischem pharmacists “will need to do a refresher course to ensure compliance and up-to-date knowledge”.
While SAHCS’s PIMART course has not yet been accredited by the SAPC as a PIMART course, it is accredited as a CPD course for pharmacists. Tlala told Spotlight in May that it has not been accredited as a PIMART course because of an identified “gap” in the course.
“The gap identified between the short course and the approved qualification standard meant that the approved provider of the short course, the Southern African HIV Clinicians Society, had to conduct a gap analysis and develop a bridging course to enable pharmacists trained in the short course to access the full PIMART scope of services,” said Tlala.
In response to questions about the “gap” in their training course identified by the SAPC, SAHCS’s CEO Dr Fiona Storie told Spotlight on 19 May: “SAHCS has completed a full review and update of the PIMART training course in line with the requirements for accreditation as a supplementary training course (i.e. not just a CPD accredited course).”
“As PIMART training was originally provided from 2019, there is a need for pharmacists to undergo refresher training since the field of HIV medicine is evolving and clinical recommendations change over time,” said Storie. She added: “SAHCS’ recommendation is that pharmacists undertake the newly updated PIMART training course as either a refresher/bridging course or, if not previously trained, as a new course.”
“SAHCS is engaging with SAPC to finalise the accreditation of the updated PIMART course as a refresher course and a new supplementary training course to make it available as soon as possible,” Storie said.
Limiting PIMART’s scope
Tlala told Spotlight that because of the “gap” in SAHCS’s training course, the SAPC has asked the Director-General of Health to grant limited scope PIMART permits.
“The Director-General: Health has been requested to issue a limited scope permit granting PIMART-trained pharmacists’ access to those services fully addressed in the short course previously delivered by the South African HIV Clinicians Society,” he said.
The health department confirmed to Spotlight that this request was received on 23 April 2026.
Neither the SAPC nor the Department of Health responded to Spotlight’s requests for clarification on which PIMART services the SAPC had proposed for inclusion in the limited-scope permits.
Angela Tembo, director of pharmacy health at the research centre Ezintsha, told Spotlight that she understands that the limited scope permits that the SAPC has requested the Director-General of Health to grant “will be limited to HIV prevention (PrEP and PEP) and not treatment”.
“Our understanding is that the delays [in implementing PIMART] relate to ongoing discussions around training requirements, accreditation processes, and the practical implementation pathway following the SCA ruling,” she added.
Tlala said as soon as the Director-General of Health approves the limited-scope permits, the SAPC will publicly communicate the launch of the PIMART programme and the services that may be accessed under such a permit.
“The full PIMART scope of services will only be available once the Southern African HIV Clinicians Society has finalised and submitted a bridging course following gap analysis or, alternatively, once another training provider is accredited to provide the PIMART Supplementary Training course,” he added.
The long-acting HIV prevention injection, lenacapavir, will become available to around half a million people in South Africa. Photo by Anna Shvets
By Marcus Low and Elri Voigt
On June 5, 2026, an HIV prevention injection will for the first time become available at some of South Africa’s public sector clinics. In this Spotlight special briefing, we pull together all you need to know about this “breakthrough” jab.
We’ve come a long way from the worst days of South Africa’s HIV epidemic, but the virus still claims over 50 000 lives per year and, even in 2026, annual new infections remain stubbornly high at over 140 000.
Reducing the rate of new infections is not an easy task. The most effective measure is to make as many as possible of the roughly eight million people who are living with the disease non-infectious. The good news is that most people with HIV become non-infectious once they are stable on antiretroviral treatment. The bad news is that the growth of South Africa’s HIV treatment programme has slowed. The pool of infectious people thus seems set to remain relatively large.
For people who are not living with HIV, the most effective form of protection over the years have been the correct use of condoms. Condoms also have the benefit that they protect against other sexually transmitted infections.
But condoms aren’t the only game in town. Voluntary medical male circumcision substantially decreases men’s risk of contracting HIV, something that also provides indirect protection for women.
And then there are antiretrovirals (ARVs) taken to prevent HIV infection. Landmark studies published in the 2010s showed that taking a tablet that contains the antiretroviral medicines tenofovir and emtricitabine could reduce someone’s risk of contracting HIV to near zero. Such tablets are commonly referred to as oral pre-exposure prophylaxis, or oral PrEP. For several years now, these HIV prevention tablets have been widely available in South Africa’s public healthcare system, although uptake has been somewhat muted. Modelling work from Thembisa, the country’s leading mathematical model on HIV and TB, suggests that only a few hundred thousand people are taking the tablets.
The long-acting revolution
One challenge with HIV prevention pills is that not everyone can, or wants to, take them every day. For some, taking ARVs, or being seen to take ARVs, still comes with an accompanying dose of stigma. For others, remembering to take a pill every day can be tricky. Ultimately, the incentives for healthy people without HIV to take prevention medicines simply aren’t as compelling and immediate as they are for people who already have the virus in their bodies.
As in some other areas of medicine, one solution to this treatment adherence challenge is simply to make it more convenient to take the treatment. Many women, for example, prefer three-monthly contraceptive injections or three-yearly implants to a regular pill. There is some evidence that similar preferences apply to HIV prevention medicines.
So-called long-acting therapies does what the name suggests – act over longer than standard periods. They could take many forms, from slow-release tablets to injections that leave a depot under the skin that slowly releases drugs into the blood stream, to small implantable devices that are typically left in the arm for several years.
The first long-acting HIV prevention option to take the world by storm was an injection. It made headlines in 2020 when a pivotal study found it to be more effective than the daily prevention pills – the difference being largely due to better adherence, rather than differences in the ARVs used. This jab, containing the antiretroviral drug cabotegravir, provides two months of protection against HIV infection at a time.
Two years later, the World Health Organization recommended the jab, called CAB-LA, for HIV prevention, and it was registered for use in South Africa. Rollout beyond an implementation science setting stalled however when the prices the drug’s manufacturer ViiV Healthcare was willing to sell it for were deemed unaffordable by the South African government.
Fortunately, a new prevention jab that provides protection for three times as long as CAB-LA was on the way. In 2024, two large studies, found an injection of the antiretroviral drug lenacapavir given every six months was almost 100% effective in preventing HIV infection. These findings would later be hailed as the journal Science’s 2024 scientific breakthrough of the year. It is this “breakthrough” that is being rolled out in South Africa from June 2026.
Two often-neglected groups in HIV research, adolescents (aged 16 and 17), and women who become pregnant while in a study, were included in clinical trials of lenacapavir. The jab was found to be safe in both populations, which means it can now be offered to adolescents and pregnant women in the South African rollout.
Lenacapavir is injected just under the skin, typically in the stomach area, where it forms a small depot that very slowly releases the drug over time. These depots can form small lumps under the skin. Though harmless and usually not visible, it will be important that people getting the jab know to expect these “subcutaneous nodules”. The other most common side effects seen in the two pivotal studies were pain at the injection site and a skin rash. These reactions and the size of the nodules appear to decrease with subsequent injections.
Prior to their first injection, people will first have to get an HIV test to ensure they aren’t already living with HIV. This is important since treating someone with HIV with just lenacapavir could result in the development of drug resistance. Together with the injection, people starting lenacapavir will also have to take some lenacapavir tablets for two days. Since the depot releases the injected drug very slowly, these tablets are needed to get the drug levels in the body up more quickly so that it can provide full protection as soon as possible. (The Department of Health has published a guideline document setting out how it should all work at the clinic.)
In addition to the lenacapavir and CAB-LA jabs, there is also a long-acting vaginal ring that contains the ARV dapivirine. The ring provides one-month of protection at a time, with a three-month version also under development. The available evidence however suggests that the dapivirine vaginal ring is not as effective at preventing HIV infection as oral PrEP or the two injectable options.
The long road to jabs at clinics
Having the scientific evidence that an injection works is of course only one step in that jab’s long journey to the point where people can get it at clinics. An essential next step was regulatory approval, which lenacapavir received from the South African Health Products Regulatory Authority in October 2025. After regulatory approval was secured, the next question became whether a sufficient supply of the product can be procured in South Africa on acceptable terms.
Lenacapavir is currently only being produced and marketed by the pharmaceutical company Gilead Sciences, who holds the critical patents on the product. In the US, lenacapavir is sold for around $28 000 per person per year. The Global Fund (the world’s largest multilateral funder of health in low- and middle-income countries) and PEPFAR (the United States President’s Emergency Plan for AIDS Relief) are however procuring limited stocks of lenacapavir at a lower price for use in some low- and middle-income countries. It is some of these Global Fund-procured jabs that will be used in the first phases of the lenacapavir rollout in South Africa.
For now, largely due to the limited stocks, the local rollout will target only around half a million people at 360 clinics in areas with high HIV rates, but the plan is to scale-up considerably in the next few years.
The South African government will likely start buying lenacapavir from generic manufacturers in 2027 or 2028. Gilead has so far issued licenses that will allow six different companies to produce lenacapavir and to sell it in 120 different countries, including South Africa.
The Gates Foundation and a partnership including UNITAID, the Clinton Health Access Initiative, and Wits RHI, have concluded separate deals with generic manufacturers that should see these generics sold for a price of no more than $40 (under R800) per person per year. This is lower than what government currently pays for oral PrEP and modelling work suggests it would be affordable for the South African government. Barring any unforeseen hiccups, the pieces are thus in place to facilitate widespread access to lenacapavir in South Africa in the coming years.
For now, none of the generic versions of lenacapavir will be produced in South Africa. Negotiations are however under way that may eventually see a local company licensed to produce the jab. Such local production is seen as important for ensuring security of supply, although it is not clear that local companies will be able to compete with Indian generic drug-makers on price.
At the time of writing, neither the lenacapavir or CAB-LA injections can be purchased at private sector pharmacies in South Africa. Oral PrEP can be purchased for around R300 for a month’s supply. The monthly dapivirine vaginal ring should cost in the region of R500 per ring. (These prices are based on the 30 April 2026 Single Exit Price database published by the health department.)
How many people will want the jabs?
One of the big unanswered questions about lenacapavir is how many people will come forward to get the jabs. We are hopeful that the Department of Health will routinely provide detailed numbers on uptake in the coming months and years.
The initial rollout is largely clinic-based, but researchers will also be assessing how well distribution works through mobile clinics. We need not stop there of course. At the height of the COVID-19 pandemic, public sector users could access SARS-CoV-2 vaccines from nurses at private sector pharmacies. With sufficient political will, the same could be done with lenacapavir. No doubt some young people will rather get their jab at the mall than at the clinic.
Those in control of the rollout will have to think carefully about how they promote and provide the jab. At its core, it is an empowering tool that can help people stay HIV-free, but as often is the case with HIV-linked products, there is a risk of stigma. In addition, even though lenacapavir is not a vaccine, some vaccine scepticism might well transfer over to lenacapavir since it is administered as an injection. As with any large healthcare intervention, one will not have to look far to find lenacapavir-related misinformation on social media.
Either way, just having the jab at clinics and hoping people will come get it might not be good enough if we’re hoping to see good uptake. Fortunately, we have several research groups and NGOs in South Africa who have world-class expertise on just this type of issue. Hopefully government will draw on this unique reservoir as they adjust and shape the lenacapavir rollout.
So what’s next
The rollout of the lenacapavir jab in South Africa will not be the end of our HIV prevention story. Two promising products in the pipeline are a new formulation of lenacapavir that looks like it could provide a full year of protection per shot and a pill containing another antiretroviral that could provide a month of protection at a time. We are keeping a close eye on the ongoing development of these products. There are also still hopes that an effective HIV cure or vaccine might one day be developed, although this is a much longer shot than better long-acting antiretroviral formulations.
In the meantime, though, twice-yearly lenacapavir is rightly dominating the headlines.
Modelling suggests that over the next 20 years, an ambitious lenacapavir rollout could reduce new HIV infections by around 20% to 30%. There can be little doubt that, like condoms and antiretroviral treatment for people living with HIV, providing lenacapavir at scale makes public health sense.
But thinking of lenacapavir mainly in terms of cost-effectiveness and public health benefits risks obscuring its more immediate and transformative human potential. For many people, especially young women, a discreet and convenient form of HIV prevention that they can control may well make the difference between contracting HIV or not.
As experts often point out, when it comes to products that can prevent HIV, choice – as in the world of contraception – is key. Some products will work for one person, but not for others. As circumstances change, a product that might have once worked may no longer be the best option. Having more than one product in the “toolkit of prevention” makes it easier to find what actually works in people’s lives.
For years, the HIV world has been flush with rhetoric about empowering young women – a group that is profoundly affected by HIV. An ambitious lenacapavir rollout might be the most concrete realisation of those ideals yet. We simply have to get it right.
Disclosure: The Gates Foundation is mentioned in this article. Spotlight receives funding from the Gates Foundation, but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council.
Fake and substandard medicines, along with bogus healthcare practitioners, pose a growing threat to patient safety in South Africa.
The sale of fake and substandard medicines is a significant threat to patient safety around the world. In South Africa, the main affected products are painkillers, antibiotics, weight-loss and sexual enhancement products, skin-lightening products, and some chronic medicines.
In pealing back the different layers of this problem, it is essential to get the definitions right.
Substandard products are those that do not meet quality standards and specifications.
Falsified products deliberately misrepresent their identity, composition or source.
Neither of these should be confused with generic medicines, which have the medicines regulator’s green light for being safe, effective, and of good quality.
People are often duped into purchasing substandard and falsified products, especially when the real thing is not available or too expensive. But, as Elna Schütz this week reports for Spotlight, there are also people who buy these medicines fully aware of the risks.
These unregulated medicines are mostly distributed through informal channels, unregulated outlets, online platforms, and cross-border smuggling networks. It is also possible that some substandard and falsified medicines have been infiltrated into otherwise reputable medicines distribution channels.
Data on the scale of the problem is scant, but there is agreement that the problem is substantial. The WHO estimates that around 1 in 10 medicines in low- and middle-income countries are substandard or falsified.
The South African Health Products Regulatory Authority (SAHPRA) is the main body responsible for regulating substandard and falsified medicines. It does this through post-market surveillance and inspections, a whistleblower reporting system, product recalls, and monitoring illegal advertising and online sales. A new National Action Plan and comments from the Minister of Health suggests there is some intent to step up these efforts.
The good news is that we can generally trust that the medicines we buy at pharmacies contain what they are supposed to and that they were manufactured according to good quality standards. As regulatory entities go in South Africa, SAHPRA is generally one of the better-functioning ones.
But, outdated legislation means that SAHPRA doesn’t have all the tools it needs to stamp out the sale of unauthorised medicines. For instance, it has limited powers in relation to advertising and marketing, cannot block a web site, and cannot issue infringement notices, or impose sanctions on entities or individuals whose actions potentially place the public at risk of harm.
The misrepresentation may include using fraudulent certificates, using another practitioner’s registration, or still offering healthcare services while being suspended or erased from the register.
From early 2024 through late 2025, 66 bogus practitioners were caught and arrested, with the majority operating in the economic hubs of the Western Cape, Gauteng, and KwaZulu-Natal.
You can help curb these problems. Suspicious practitioners can be reported to the HPCSA, and suspicious products or sellers can be reported to SAHPRA. People are also advised to buy only from licensed and authorised pharmacies and checking if healthcare providers are registered.
And then there is fake news
In some areas, as with bogus health professionals and falsified medicines, the solution to misrepresentation is clearly to have legally empowered regulators with enough muscle to consistently enforce the law.
But when it comes to misinformation and disinformation – call it fake news if you will – the way forward is much less obvious. In recent years, we’ve seen a toxic mix of political polarisation, conspiracy theories, disinformation campaigns, and twisted social media algorithms – often fuelling a rejection of science and evidence-based policy-making. Beyond just our screens, these trends have unfortunately started to distort the real world, as we’ve seen at various critical health institutions in the United States.
In our view, regulators should have a role in preventing misinformation and disinformation about medicines. But how exactly to make such regulation work in an age of largely unaccountable social media networks is not at all clear.
What we think is clear, is that much of the solution to the problem of health misinformation and disinformation, is simply to keep creating its opposite, high-quality, rigorous, and evidence-based journalism.
This is the core of what we try to do at Spotlight. It is also why we have made our journalism subject to the South African Press Code, work hard to stick to our Editorial Policy and Style Guide, and why we urge you to hold us accountable when we get things wrong, as we will inevitably do from time to time.
From unregulated weight loss injections to unsafe pain tablets, substandard and falsified medical products pose a threat to the health of people. Spotlight reports on how regulators are fighting the problem in South Africa.
“I know that there is a risk, but at this point I feel that the benefits outweigh everything else,” says Anna*, who buys unregulated medicine on the black market.
She was prescribed GLP-1 RA medicines by a doctor after being tested for insulin resistance. She has lost around 30kg and says the positive impact on her body, life, and self-esteem has been massive. GLP1 RAs (Glucagon-Like Peptide-1 Receptor Agonists) medicines, sold under brand names like Ozempic and Mounjaro, are increasingly used for weight loss and to prevent and/or treat diabetes.
When global shortages affected GLP-1 RA stocks in local pharmacies, Anna started buying similar drugs directly from unregistered sellers. For around R1 650, a fancy-looking box with a three-month supply of injections is delivered to her in a small cooler box. “I knew then already that what I was buying was unregulated and potentially inferior or even dangerous,” she says, adding, “but I was finally starting to feel good about myself.”
Apart from being aware that the unregulated drugs could potentially harm her, Anna says she found that the regulated products were often out of stock, expensive, and came with stigma from pharmacists who quizzed her on whether she deserved the products. “If I could have kept doing it the proper way, I would have, but there were just too many obstacles,” she says.
Defining the problem
Weight-loss medicines are only one of several types of health products that are frequently purchased outside of formal channels, according to the South African Health Products Regulatory Authority (SAHPRA).
“Commonly affected products include painkillers, antibiotics, weight-loss and sexual enhancement products, skin-lightening products, and some chronic medicines,” Mokgadi Fafudi, SAHPRA’s manager of regulatory compliance, tells Spotlight.
“Combating the threat of substandard and falsified medical products is one of the urgent global challenges of this decade,” says Faridun Nazriev, the external relations and communications officer at the World Health Organization (WHO) Country Office in South Africa.
“Substandard products are those that do not meet quality standards and specifications, often due to poor manufacturing practices or inadequate quality control. Falsified medical products deliberately misrepresent their identity, composition or source”, according to the WHO. These products, it adds, are often created and distributed with the intent to deceive consumers for financial gain.
Two other definitions should not be confused with these, cautions Dr Andy Gray, a senior lecturer in Pharmacology at UKZN and co-director of the WHO Collaborating Centre for Pharmaceutical Policy and Evidence-Based Practice.
Compounded medicines are custom formulations that may be specific to a patient, but are generally not registered by SAHPRA.
Generic medicines are those that have been tested and found to be as safe and effective as originator medicines, but are generally cheaper. Generic medicines on the market have been approved by SAHPRA and are not in any way substandard.
Gray says the term counterfeit is no longer used by the WHO, because it refers specifically to breaches of intellectual property, like trademarks.
Lack of data
While the WHO estimates that 1 in 10 medicines in low-and middle-income countries are substandard or falsified, all regions are affected and have been seeing an increase, according to a 2024 report from the WHO’s Global Surveillance and Monitoring System.
South Africa also appears to have rising rates. SAHPRA’s 2021/2022 annual report notes that 101 health product quality complaint reports were filed. In 2022/23, that figure nearly tripled to 297.
Fafudi says that the organisation received 588 reports of possible non-compliance in the 2024/2025 year. She says that for the 2025/26 year, this number exceeds 570 cases, though this has not yet been published by SAHPRA.
But such reports are likely only the tip of the iceberg. Gray laments that we don’t have the full picture of how big the problem of substandard and falsified medical products really is.
This is partly because, by its very nature, the sale of substandard and falsified medicines is usually hidden. Fafudi says that these medicines are often sold through informal markets, unregulated outlets, online platforms, and cross-border smuggling networks.
Gray adds that these medications aren’t necessarily always sold through informal means. “They may be infiltrated into wholesalers or state medicine depots, and then distributed,” he says, “Or they may be sold directly to pharmacies or prescribers and then sold to patients.”
A threat to patients
As in Anna’s experience with GLP-1 RAs, there is often a demand for unregulated products because the properly regulated products can’t meet the public demand.
Fentse Maseko, who works in the Department of Pharmacology and Pharmacy at Wits University, researched this issue in her Master’s thesis and advocates in the space. She notes that in many low- and middle-income countries, particularly in remote and underserved areas, limited access to medicines may force patients to seek treatment from informal markets. She adds that in South Africa, porous borders and rising costs also play a role.
Whatever the reasons behind their proliferation, the risks to the healthcare system and individuals are multi-faceted.
“Substandard and falsified medicines are a serious threat to patient safety and public trust,” says Refiloe Mogale, the executive director for the Pharmaceutical Society of South Africa (PSSA). “These products can lead to treatment failure, harm, or even death.”
Maseko warns that it can also add to the growing problem of antibiotic resistance if antibiotics are substandard. It can also strain the healthcare system when second or third-line treatments are needed for issues initially addressed with unregulated products, or caused by them.
The role of the regulator
The main body in South Africa responsible for regulating substandard and falsified medicines is SAHPRA. Fafudi explains that they conduct post-market surveillance and inspections, run a whistleblower reporting system, manage product recalls, and monitor illegal advertising and online sales.
SAHPRA also works with specialised units in the South African Police Service as well as other stakeholders such as customs to enforce joint operations. Fafudi says such joint operations have been conducted on at least a monthly basis.
There are also legal actions, including issuing warnings, seizing or destroying products and criminal prosecution. According to the Medicines and Related Substances Act 101 of 1965, fines or prison sentences not exceeding 10 years may be prescribed.
The PSSA however charges that not enough is being done. “Key gaps are visible in insufficient regulatory capacity, weak border control, limited enforcement scale and the under-resourced National Action Plan,” Mogale says. “The system is overwhelmed by the speed and sophistication of the problem.”
Reporting unregulated products
The public can help address the problem of substandard and falsified medicines. SAHPRA advises buying only from licensed and authorised pharmacies and healthcare providers.
“Be cautious of unusually low prices, miracle cure claims, and poor packaging,” Fafudi warns. “Always check packaging, expiry dates, and consult healthcare professionals before use.”
Suspicious products or sellers can be reported on the SAHPRA website.
Jas Bhana, Chief Executive Officer of the Innovative Pharmaceutical Association of South Africa, adds that the public can also report suspicious products to the National Department of Health or their nearest pharmacy. “Combating this threat requires collective vigilance to safeguard every patient’s right to safe, quality, and effective medicines,” she says.
This goes hand-in-hand with the need for consumers to know the dangers, Maseko explains. “While public education plays an important role in mitigating this risk, effective risk communication remains a challenge, particularly in communities with limited health literacy,” says Maseko.
On a bigger scale, Nazriev explains that the WHO prioritises prevention, detection, and response as the main pillars of action. This includes local regulation as well as collaboration between countries.
“Given the transnational nature of globalised medical product supply chains as well as criminal networks, collaborating across borders and sectors is essential to national, regional and global responses,” he says.
Better regulation
Gray acknowledges that there is a challenge in budgets and laboratory capacity, but even so he calls for more to be done. “SAHPRA needs to move from a largely reactive stance to a more proactive one, sampling medicines from the distribution chain and submitting them for checking, and then report to the public on their findings,” he suggests.
The PSSA recommends implementing a national medicine registry with a track-and-trace system and stricter control of online medicine sales, including mandatory certification and monitoring.
SAHPRA is already planning along some of these lines. “Future plans include strengthening supply chain traceability, enhancing detection systems, regulating online medicine sales, and increasing public awareness campaigns,” says Fafudi.
Part of this direction comes from a National Action Plan (NAP), launched late last year by SAHPRA, with support from the National Department of Health and the WHO.
“All actors within the supply chain, particularly at key pinch points in both the public and private sectors, must be equipped with the knowledge, skills, and equipment to identify and report suspicious products to SAHPRA,” Health Minister Dr Aaron Motsoaledi is reported to have said at the launch of the NAP. “All activities should mitigate the risk of substandard and falsified medical products. This includes increased vigilance at ports of entry, through to post-market surveillance of high-risk products, inspection of manufacturers, distributors and wholesalers.”
Whether all this will be done, and what it will mean for people like Anna who knowingly choose to use unregulated medicines, remains to be seen.
#InsideTheBox is a column by Dr Andy Gray, a pharmaceutical sciences expert at the University of KwaZulu-Natal and Co-Director of the WHO Collaborating Centre on Pharmaceutical Policy and Evidence Based Practice. (Photo: Supplied)
8th May 2026 | Andy Gray
We can generally trust that the medicines we buy at pharmacies contain what they are supposed to and that they were manufactured according to good quality standards. In his latest column, Dr Andy Gray zooms in on the regulatory scaffolding that enables this trust.
One of the health-related Sustainable Development Goal targets is to achieve “universal health coverage, including financial risk protection, access to quality essential health-care services and access to safe, effective, quality and affordable essential medicines and vaccines for all”. The word “quality” appears twice in that target description, as a requirement for the healthcare services delivered, and as an essential element of the medicines and vaccines made available.
‘Quality cannot be tested into a product’
There is a truism in the pharmaceutical industry that quality cannot be tested into a product. Instead, quality is assured by the implementation of a pharmaceutical quality system, referred to as current Good Manufacturing Practice (cGMP).
The primary legal enablement is provided by the Medicines and Related Substances Act, 1965. Section 1(3) of the Act states: “In determining whether or not the registration or availability of a medicine is in the public interest, regard shall be had only to the safety, quality and therapeutic efficacy thereof in relation to its effect on the health of man or any animal, as the case may be.” Evidence for safety and therapeutic efficacy is provided by well-conducted clinical trials. There is a difference, however, between registered medicines and complementary medicines. The latter require a warning on their labels stating: “This unregistered medicine has not been evaluated by the SAHPRA for its quality, safety or intended use”. Complementary medicine manufacturers are being progressively brought in line with GMP.
Evidence of quality is not reliant only on retrospective data, on tests conducted on the medicines used in the clinical trials, and the design of the dosage form to be sold, but also on the means to ensure that every batch made will deliver the same results. By requiring that every manufacturer of a medicine is licensed by the South African Health Products Regulatory Authority (SAHPRA), the Authority can ensure compliance with GMP. The ultimate sanction for not meeting GMP standards is withdrawal of licensure and therefore an immediate stop to all manufacturing activities.
New guidelines
SAHPRA updated its GMP guidelines in April 2026. The guideline defines GMP as “a set of principles and procedures that, when followed, ensure that medicines and related substances are of high quality, safety and efficacy”, and as a “system that ensures medical products are consistently produced and controlled according to quality standards”. Echoing the truism, it states that GMP is “designed to minimise the risks involved in any pharmaceutical production that cannot be eliminated through testing the final product”.
GMP requires the manufacturer to provide detailed description of the systems to be implemented to document every step in the manufacturing process and the control measures in place to ensure quality. These step-by-step descriptions have to cover every component included in the medicine and its packaging, the premises and equipment used, as well as the training and accreditation of the staff involved in the production process. A risk-based approach is used, for example differentiating between sterile and non-sterile production processes. Quality control testing during the production process is critically important.
GMP places a lot of emphasis on the capability of key personnel, but also the way in which authority and responsibility is assigned, accepted and documented, and how each person fits into the management decision-making process. For example, SAHPRA’s GMP guidelines differentiate between the Head of Quality Control, who “should have the authority to establish, verify and implement all quality control procedures such as authority over quality decisions, oversight of testing and results, approval of quality control documentation, laboratory management, validation and method control”, and the Head of Quality Assurance, who “should be part of the decision-making process in all matters that affect the quality of products including development, laboratory, storage, distribution, vendors and third-party contractors”. All staff engaged in production have to be trained on the principles of GMP and the specific duties assigned to them. Continuing training is required, with documented training programmes, training records, and checks to confirm that procedures are being followed.
What if medicines are made outside of SA?
That all sounds straightforward, if the manufacturer is located in South Africa and can easily be accessed by a SAHPRA GMP inspector. However, the majority of medicines consumed in South Africa are imported, and even those that are made locally mostly rely on imported active pharmaceutical ingredients or drug substances.
Although there is provision for exceptions, medicines imported into South Africa have to be subjected to post-importation identification and assay (testing of what it contains) by a local, accredited laboratory, or samples have to be returned to the manufacturer or an overseas testing laboratory.
SAHPRA is a member of two key organisations that are advancing harmonisation of regulatory standards. The International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) publishes extensive quality guidelines. ICH Q10, for instance, describes the requirements for a Pharmaceutical Quality System.
SAHPRA is also a member of the Pharmaceutical Inspection Co-operation Scheme (PIC/S), which aims to pursue the “development, implementation and maintenance of harmonised GMP standards and quality systems of inspectorates”. Apart from its work on harmonising GMP standards, PIC/S enables the training of GMP inspectors and the voluntary sharing of GMP inspection reports. PIC/S membership requires an assessment of a regulator’s inspectorate systems and procedures, so provides a quality check at that level. South African GMP adopted the PIC/S GMP guide in 2006, updating that status in 2017.
SAHPRA’s GMP inspectors are not confined to working only within the boundaries of the country. They also inspect pharmaceutical production plants in other countries and work together with the WHO prequalification programme to extend their reach. That said, even the best-resourced regulatory authorities are struggling to cover a globalised pharmaceutical industry, with many facilities located in China and India. A recent commentary in the New England Journal of Medicine pointed out how few foreign plants making generic medicines had been inspected by the Food and Drug Administration, and the problems they encountered when conducting inspections, calling for improved post-marketing surveillance.
The public, patients and health professionals can therefore make a reasonable assumption that medicines produced in a cGMP-compliant production facility meet the required quality standards. However, that is insufficient on its own. Mature regulators are also required to have effective post-marketing vigilance systems in place. Apart from adverse event reporting, these systems should also enable the reporting of quality problems with medicines.
Substandard or falsified medicines
Effective surveillance of the pharmaceutical market assists in the identification of substandard or falsified (SF) medicines. The necessary control measures also have to be in place to enable recalls and the destruction of identified SF medicines.
The WHO Global Benchmarking Tool (GBT) requires evidence that “Legal provisions and regulations authorize market surveillance and control activities which include product sampling from different points of the supply chain.” SAHPRA does not operate its own testing laboratory, but contracts with a WHO -prequalified facility at North-West University. Proactive sampling of medicines from all points in the distribution chain needs to be strengthened, as part of the National Action Plan to combat SF medicines.
Despite the existence of a Global Surveillance and Monitoring System for SF medical products (both medicines and devices), quantifying the scale of the problem remains challenging. Medical product alerts have been issued in every WHO region, affecting every type of medical product, not only generic medicines. They have been identified in countries with well-resourced, mature regulatory systems and in countries that lack such capacity. Nonetheless, transparent reporting of problems identified, corrective actions taken and regulatory interventions can help to build confidence that quality assurance systems are not only working, but are seen to be working. Quality should not have to be assumed without assurance that effective systems are in place and appropriately monitored.
*Dr Gray is a Senior Lecturer at the University of KwaZulu-Natal and Co-Director of the WHO Collaborating Centre on Pharmaceutical Policy and Evidence Based Practice. This is part of a series of columns he is writing for Spotlight.
Disclosure: Gray serves on three technical advisory committees at the South African Health Products Regulatory Authority.
Note: Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.
Around 3.8 million people in South Africa developed depression in 2024, researchers estimate in a major modelling study. Photo from Pixabay CC0
By Gauta Mashego
Substance abuse is both a symptom and a consequence of untreated mental illness, and government needs to urgently step in to confront this dangerous overlap, argues Gauta Mashego of SECTION27.
Mental health globally has been in crisis for years. The strain on mental health was especially visible when the world stood still during the COVID-19 pandemic. The prevalence of anxiety and depression increased by 25% in the first year of the global outbreak of the SARS-CoV-2 virus, according to the World Health Organization. However, as the pandemic eased and life returned to the usual, open conversations around mental health also tapered off.
In South Africa, as in many low-and-middle income countries, people struggle with mental health disorders such as anxiety and depression. Around 3.8 million people in South Africa developed depression in 2024, estimate researchers in a major modelling study published as a preprint in March on medRxiv.
Mental health is shaped by many factors
Several studies worldwide report a high prevalence of substance use among people with mental illness compared to the general population.
Researchers have found that patients who suffer from psychotic disorders, such as schizophrenia and bipolar mood disorder, were more likely to abuse alcohol and illegal substances. Indeed, findings from a community survey highlighted a substantial burden of co-occurring mental disorders and alcohol use among men in three provinces in South Africa.
What also makes our society vulnerable to both mental health conditions and increased use of drugs and the development of substance use disorders, is our historical context of apartheid as well as socio-economic factors such as poverty, unemployment, and violence. Researchers have argued that mental health problems are related directly to poverty, while others also make the case that the poor are at greater risk than the rich to suffer from mental illness. At the same time, those living with mental illness are more likely to remain trapped in poverty due to high treatment costs, reduced productivity, and stigma around mental illness.
The kids are not alright
Underage drinking further complicates an already complex problem.
Up-to-date statistics of underage drinking in South Africa are limited, however the matter was thrust into the spotlight on Christmas day in 2025 when a disturbing video circulated on social media showing children between the ages of 6 and 12 consuming alcohol in the presence of adults.
Providing insights into the drinking behaviours of adolescents aged between 11 and 18, a 2019 Human Sciences Research Council study in townships across three provinces found that most had their first drink at the age of 13 or 14 years.
Highlighting the extent of underage drinking among Grade 8–11 learners from public schools in all nine provinces, the 2011 South African Youth Risk Behaviour Survey recorded that around 17% of 13-year-olds and 18% of 14-year-olds had engaged in drinking five or more drinks within a few hours on one or more days in the preceding month.
Mental disorders that commonly co-occur with alcohol use disorders in adolescents include antisocial disorders, mood disorders, and anxiety disorders.
Young people’s drinking habits are often linked to factors such as social norms, and the accessibility and affordability of alcohol. Added to this, since young people are often prolific consumers of media, they are frequently exposed to alcohol advertising and marketing, which encourages the consumption of alcohol.
But there is some hope.
The Liquor Amendment Bill aims to amend the Liquor Act of 2003 to prohibit the advertising, promotion or product placement of liquor in all forms of media. The Amendment Bill is at a very early stage in the legislative process, and it is likely to take time before we see any changes to the law (and longer before we see its implementation).
Other legislative changes debated include raising the legal drinking age from 18 to 21 and keeping schools alcohol-free, and more generally to place a moratorium on new liquor licences and stronger enforcement against Liquor Act violations.
South Africa also has a National Drug Master Plan 2019-2024. It was released by the Department of Social Development, and importantly, it recognises addiction as a chronic disease affecting the brain and behaviour.
However, experts say that while it is a great document, the Central Drug Authority which is tasked with implementing the plan, needs more power and resources to implement the plan’s recommendations.
South Africa also has a National Mental Health Policy Framework and Strategic Plan (2023-2030), that was introduced by the Department of Health. Similarly to its previous iteration, the latest plan envisions the integration of mental healthcare into primary healthcare. A key objective of the new plan is to ensure that mental healthcare users have access to care near their places of work. Another aim is to strengthen collaboration between government departments like education and social development to ensure that mental health is incorporated in planning and service development.
However, as it stands, many public healthcare facilities lack mental health professionals, with rural and underserved communities having little to no access to care. Only about 50% of public hospitals offering mental health services have a psychiatrist, while the country has less than one psychologist for every 100 000 people.
Shortages of mental health professionals mean patients often wait months for appointments. For an adolescent or a child who experiences anxiety, depression or suicidal thoughts, these delays can feel unbearable and it is quite possible that they may give up before receiving help. Currently, only one in ten children diagnosed with treatable mental conditions will have access to care.
While South Africa developed extensive legislative and policy frameworks to give effect to the constitutional right to healthcare, including mental healthcare, constitutional promises must make a difference in the lives of people. Unfortunately, millions of people in the country face barriers to mental healthcare, exposing the persistent gap between constitutional promises and lived reality.
When families lack access to counselling, community-based mental health services and early intervention programmes, harmful coping mechanisms continue to be passed down rather than prevented. To achieve the objectives of the Mental Health Policy Framework by 2030 and to catch up with the National Drug Master Plan that lapsed in 2024, stronger political will and meaningful action are urgently required. This is a crisis South Africa can’t evade.
*Mashego is a candidate attorney with SECTION27.
Note: Spotlight is published by SECTION27, but is editorially independent – an independence that the editors guard jealously. Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.
From 5–7 May, the Constitutional Court will hear two of the multiple challenges to the NHI Act. Sasha Stevenson, Executive Director of SECTION27, considers what will be on the line in these first potentially landmark cases that deal with the process that led to the Act.
The public discussion on National Health Insurance has gone from abstract; to alternatively excited or worried about implementation; to dizzying references to a range of court cases filed over the course of 2024 and 2025. It can be difficult to keep up with what NHI may mean for our health system and when the promised system reform may happen.
We may now be approaching a decisive moment, with the Constitutional Court set to hear two of the NHI challenges.
From 5–7 May 2026, the Constitutional Court will be hearing challenges brought by the Board of Healthcare Funders and the Premier of the Western Cape. These two challenges deal with public participation in the making of what is now the NHI Act.
In February 2026, parties challenging the constitutionality of specific sections of the NHI Act agreed with government to put their cases on hold, pending a decision of the Constitutional Court in the May 2026 public participation challenges. The parties bringing constitutional challenges include the South African Private Practitioners Forum, the Hospital Association of South Africa, the South African Medical Association, and the Health Funders Association, among others. They agreed to hold off because a decision of the Constitutional Court on public participation could make the constitutional challenges unnecessary.
So for now, all eyes are on the Constitutional Court, whose judges will decide whether government must go back to the drawing board and follow a different procedure, or whether it may go ahead (and face a slew of constitutional challenges).
The Western Cape’s case
The Western Cape government is challenging the NHI Act because it argues that consultation with the Western Cape government, over legislation that restructures health services provided by provinces, was lacking. They argue that the National Council of Provinces (NCOP) failed to respond to a request for an extension for the Western Cape to submit the outcome of its provincial consultation on the NHI Bill and its voting mandate, and then went ahead without the Western Cape documents.
The NCOP also did not, the Western Cape government alleges, consider or debate any proposed amendments to the NHI Bill arising from the public participation in other provinces. When the Western Cape government submission and public participation report came in, the NCOP merely confirmed its earlier decision to approve the Bill.
In essence, the Western Cape’s challenge is about the NCOP’s role of ensuring that provinces and their residents have a say in the making of new laws, and whether that role was properly played. It argues that the NCOP’s failure to play its constitutional role should result in the NHI Act being declared unconstitutional and invalid.
The Board of Healthcare Funders case
While the Western Cape challenge does not deal with public participation in the NHI law-making writ large, the Board of Healthcare Funders (BHF) case fills this gap.
The BHF argues that both the National Assembly and the NCOP failed to comply with their constitutional obligations to facilitate meaningful and effective public involvement in the NHI law-making process. The BHF contends that the public was not provided with sufficient information to allow for meaningful engagement (such as details about the costs and the benefits package of the NHI Fund); and that law makers were not open to persuasion in the participation process.
The BHF asks that the NHI Act is declared invalid and set aside.
Why should we care about public participation?
The Constitutional Court has held that “[i]t is apparent from the preamble of the Constitution that one of the basic objectives of our constitutional enterprise is the establishment of a democratic and open government in which the people shall participate to some degree in the law-making process.”
There was a huge amount of public participation in the law-making process for the NHI Act, with roadshows, written submissions and oral presentations. Government respondents in the BHF case point to the fact that 338 891 written submissions were made at various stages, and many oral presentations were heard by Parliament. Few could argue that, if you wanted to, you did not have a chance to have your say on the NHI Bill.
But is being able to say something enough?
In a constitutional democracy where citizens participate in law-making between elections as a way of directly influencing the law, if there is no chance of having that influence, merely being able to speak is insufficient.
There is, of course, no obligation on government to adopt proposed changes as a result of public participation. Parliament cannot be required to agree with all submissions, and the validity of a process does not turn on whether amendments were made to take into account submissions. But when few or no amendments are made, it inevitably raises eyebrows.
In the case of the NHI Bill, while there were limited changes to the Bill when it went through the National Assembly, no changes at all were made following the NCOP public participation process. Given the hundreds of thousands of submissions, many of which were substantive, the small number of amendments is surprising. Particularly given that some submissions that were consistently made are now being conceded by the Department of Health, in public or in private. These include submissions related to the position of asylum-seekers, transitional provisions, and the role of medical aids.
SECTION27 and the Treatment Action Campaign made submissions at Draft Bill stage, before the National Assembly, and before the NCOP. As health activists and health rights lawyers, our submissions were carefully considered and proposed amendments to bring the Bill in line with the Constitution and the needs of healthcare users. Our experience was of MPs engaging to a very limited extent with the substance of the submissions, focusing rather on whether we were ‘for’ or ‘against’ the NHI, or their party’s position on it. It was an experience that brought into question how seriously real public participation was being taken.
The Constitutional Court will now be able to consider whether the public participation processes on the NHI Act were in line with the constitutional call for participatory democracy; or whether they were an unconstitutional tick box exercise. Its decision will determine if the NHI Act will be further scrutinised for substantive constitutionality through litigation, or if it should be returned to the legislature for further consideration and participation.
Either way, what NHI may mean for our health system is a question that may yet take some time to answer. On the other hand, what participatory democracy requires of parliament (arguably an even more consequential question) may soon be answered by the Constitutional Court.
*Stevenson is a human rights lawyer and executive director of SECTION27. SECTION27 is representing the Treatment Action Campaign in an application to be admitted as amicus curiae in a court case relating to the NHI.
Note: Spotlight is published by SECTION27, but is editorially independent – an independence that the editors guard jealously. Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.