Australian hospitals will lead a first-in-human clinical trial of a new investigational genetic therapy that aims to lower cholesterol in people at increased risk of cardiovascular disease. The Victorian Heart Hospital, operated by Monash Health in partnership with Monash University, will be the first clinical trial site globally to begin testing the investigational therapy STX-1150, developed by Scribe Therapeutics.
The therapy is designed to reduce LDL (‘bad’) cholesterol by targeting a gene in the liver called PCSK9, a well-established regulator of cholesterol levels and cardiovascular risk. Elevated LDL cholesterol is a major cause of atherosclerotic cardiovascular disease, including heart attacks and strokes.
STX-1150 uses a next-generation CRISPR-based approach known as epigenetic silencing. Delivered as a one-time infusion, the therapy is designed to reduce cholesterol levels for an extended period without permanently altering a person’s DNA.
Principal Investigator of the study Professor Stephen Nicholls, Director of the Victorian Heart Hospital and Victorian Heart Institute, and Professor of Cardiology at Monash University, said the trial represented another major step forward in developing more durable approaches to cardiovascular prevention.
‘The best way to treat heart disease, the leading cause of death globally, is to prevent it,’ Professor Nicholls said.
‘While existing cholesterol-lowering therapies are highly effective, many people still struggle to maintain long-term treatment due to cost, access, side effects, or the burden of ongoing medication.’
‘This new investigational therapy is designed to provide sustained cholesterol reduction following a single treatment, which could significantly change how we manage cardiovascular risk in the future. This represents the new frontier of cardiovascular medicine.’
‘It is incredibly exciting that Victorians and Australians will again play a leading role in the development of next-generation genetic therapies for heart disease.’
The Phase 1 study will assess the safety, tolerability and biological effects of STX-1150 in adults with elevated LDL cholesterol who are at increased cardiovascular risk.
The trial plans to enrol up to 64 participants across sites in Australia and New Zealand, with participants monitored for one year following treatment.
The study follows regulatory clearance from Australia’s Therapeutic Goods Administration and builds on growing international interest in genetic approaches to cardiovascular disease prevention.
About the study
The Phase 1 trial will evaluate STX-1150 in adults with elevated LDL cholesterol and increased cardiovascular risk.
The study is designed as an open-label, single ascending dose trial followed by a dose expansion phase.
Up to 64 participants are planned to be enrolled across Australia and New Zealand.
The Victorian Heart Hospital will serve as the initial clinical trial site.
Participants will be followed for one year after treatment.
Two new vaccines to prevent tuberculosis (TB) are safe for use in adults and children, but they do not offer protection against all forms of TB, finds a large trial from India published by The BMJ.
TB remains a major global public health concern. In 2023, an estimated 10.8 million people worldwide were reported to have TB and the rate of new cases increased by 4.6% between 2020 and 2020, highlighting the growing scale of the problem. BCG is currently the only licensed vaccine against TB. Yet although it is effective against severe forms of TB in young children, it does not offer protection for adolescents and adults.
To address this gap, researchers in India conducted a large trial to evaluate whether two new TB vaccines (VPM1002 and Immuvac) can protect against all forms of tuberculosis (pulmonary and extrapulmonary), prevent latent (dormant) infection, and generate an immune response against the TB bacterium.
The study enrolled 12 717 household contacts (aged 6 years and older) of recently diagnosed TB patients across 18 sites in six Indian states between July 2019 and December 2020.
Participants were randomly allocated to receive a first dose of either VPM1002, Immuvac, or a placebo (4 239 in each group) and were followed up for 38 months. A second dose was administered to 11,829 participants one month later. A total of 12 295 participants (96.7% of those enrolled) completed 38 months of follow-up.
While neither vaccine offered general protection against TB or prevented latent TB infection, both demonstrated an ability to prevent the progression to active TB in those who developed latent TB.
The researchers found that although both vaccines did not show effectiveness against all TB and pulmonary TB (PTB), one of the vaccines, VPM1002 showed effectiveness (50.4%) against extrapulmonary TB (EPTB) across all age groups, including those aged 36-60 years (79.5%). These findings suggest a potentially significant public health benefit, because extrapulmonary TB, which affects organs beyond the lungs, is often associated with a higher risk of mortality than pulmonary TB.
A promising key finding was the protection seen against TB in children, whereby VPM1002 provided protection against all TB, PTB and EPTB in the 6 to under 14 year age group, while Immuvac provided protection against EPTB only in the 6 to under 10 year age group.
However, neither vaccine protected children and adults who were underweight. This suggests that nutritional support may be needed along with vaccination, especially for younger children, report the authors.
Both vaccines were found to be safe and induced an immune response.
The researchers acknowledge that the covid-19 pandemic affected the study, leading to the exclusion of some participants who missed the second dose and sometimes delayed follow-ups. Furthermore, the findings may not apply in other countries or ethnicities.
Nevertheless, this was a large, well-designed study that reflects a real world scenario because it included both children and adults, regardless of pre-existing conditions like diabetes and risk factors, as reported by authors. Further research on commonly targeted high-risk groups for TB could be undertaken, they conclude.
Current clinical guidelines stress that lower LDL cholesterol levels significantly reduce the risk of major cardiac events. Essential strategies for treatment include heart-healthy lifestyle changes and pharmacological interventions using statins, ezetimibe, and PCSK9 inhibitors. Early intervention is vital, as the cumulative exposure to high cholesterol over time – often termed “LDL years” – determines the onset of vascular disease. But a major question has remained as to whether more aggressive lip-lowering targets is worth the potential side effects such as kidney damage.
Now, a new clinical trial published in NEJM provides evidence that an intensive target of less than 55mg/dL is superior for preventing secondary complications. In the Ez-PAVE trial, researchers in South Korea investigated whether this more intensive provided better protection than the conventional goal of less than 70mg/dL. The study found that patients in the intensive group experienced a significant reduction in cardiovascular events over a three-year period. The researchers conclude that their findings support stricter lipid-lowering guidelines, which can safely and effectively improve long-term patient outcomes.
An international, randomised, double‑blind, placebo‑controlled phase 3 study, the largest of its kind for mpox, found that tecovirimat did not improve clinical outcomes for adults with clade II mpox compared with placebo, while demonstrating a similar safety profile. Results of the STOMP/A5418 trial, published in the New England Journal of Medicine underscore both the urgent need for alternative therapeutics and the critical importance of randomised trials during public health emergencies.
This Phase 3 study randomised 412 participants (344 with laboratory‑confirmed mpox), to receive either tecovirimat or a matching placebo for 14 days. Randomisation was stratified by early versus later symptom onset and by the presence of severe pain. Participants had active skin or mucosal lesions and self‑reported daily symptoms, pain scores, and lesion status through Day 29, with confirmatory clinical assessments at scheduled visits. Biospecimens, including lesion swabs, oral and rectal swabs, and blood samples, were collected at multiple time points to assess viral DNA clearance. The primary endpoint was time to clinical resolution of all lesions, and key secondary endpoints included pain reduction, complete lesion healing, and virologic response.
Conducted across seven countries at 49 sites, the phase 3 study showed that tecovirimat did not shorten the time to lesion resolution, reduce pain, or speed viral clearance compared with placebo. These results align with interim findings released in December 2024, which led the trial’s independent Data and Safety Monitoring Board to halt further enrolment due to statistical futility.
“In the midst of a global public health emergency, the ACTG team rapidly conducted this randomized controlled trial to deliver a clear answer for patients and clinicians,” said William A. Fischer II, MD, associate professor of pulmonary and critical care medicine at the UNC School of Medicine, and director of emerging pathogens research at the UNC Institute for Global Health and Infectious Diseases. “These findings advance our understanding of mpox and help the field refocus efforts on identifying safe, effective and accessible treatment strategies, particularly for people at highest risk of severe disease.”
Although the trial did not demonstrate efficacy, tecovirimat demonstrated a favourable safety profile, with no major safety concerns identified – an important confirmation as thousands of patients worldwide have already received the drug under expanded access protocols.
“The STOMP trial provides essential evidence at a critical time and demonstrates why randomized controlled trials are an indispensable part of outbreak response,” said Joe Eron, MD, chief of infectious diseases and chair of the ACTG network. “But now we must keep going to find safe and effective treatment for people as this virus continues to circulate globally.”
The study’s conclusions are expected to influence clinical practice and public health guidance worldwide. With mpox still causing outbreaks in multiple regions, researchers emphasise that developing and evaluating new antiviral candidates remains a top priority.
Dr Sheetal Kassim, the site lead for the Desmond Tutu Health Foundation’s clinical trial site at Groote Schuur Hospital. (Photo: Nasief Manie/Spotlight)
By Elri Voigt
A cutting-edge, South African-led HIV vaccine trial built on decades of research recently kicked off in Cape Town. Spotlight unpacks what exactly is being studied, and how the resilience, tenacity and urgency of a group of dedicated South African researchers made it possible.
Antiretroviral medicines can suppress HIV in the body and keep people healthy, but we do not yet have a viable cure for HIV or an effective vaccine. It is not for lack of trying. For decades now, researchers across the globe have been working hard to develop a vaccine against HIV. While there have been several major disappointments along the way with vaccines failing in large studies, a new clinical trial in South Africa might soon find vital answers that could reinvigorate the field.
The study was originally set to start in 2025, but researchers had to pivot and find new funders when the United States abruptly terminated much of its international research funding. After some scrambling, a stripped-down version of the study has now started. Rather than being cowed by having to delay, and reduce the size of the study, it seems that forging ahead without US support have sparked a pervasive sense of optimism.
“It feels like the most coherent, involved clinical trial I’ve ever been involved in – so that’s why I’m so excited. I feel like it’s going to lead to big things because it’s bringing so many people with it,” says Professor Penny Moore, a leading virologist who is heading up the laboratory work for the study.
That optimism is tangible at the clinical trial site in the Old Main Building at Groote Schuur Hospital in Cape Town. During our visit, one can’t help noticing how the Desmond Tutu Health Foundation’s signature rainbow logo and colourful walls and furniture breaks through the dark hospital corridors and ancient elevators.
The colourful waiting room at the Desmond Tutu Health Foundation’s clinical research site at Groote Schuur Hospital where a South African led HIV vaccine trial is taking place. (Photo: Nasief Manie/Spotlight)
Like the sugar coating on a Smartie
In the clinical trial, called BRILLIANT 011, researchers are testing two immunogens, says Dr Sheetal Kassim. She is the site lead for the Desmond Tutu Health Foundation’s clinical trial site at Groote Schuur Hospital and Principal Investigator for the trial. An immunogen is an engineered agent designed in a laboratory, she explains, to cause a specific immune response. The aim of this trial, Kassim says, is to see if these two immunogens are able to trigger the development of cells that have the potential to later become special immune cells called broadly neutralising antibodies.
Once HIV is in someone’s body, it is able to stick around mainly by taking over immune cells called CD4 cells. It evades the immune system by constantly mutating so the antibodies sent to find it don’t recognise it. Eventually the infected CD4 cells burst and die, but HIV keeps replicating, weakening the immune system.
Broadly neutralising antibodies are special antibodies that can recognise and fight a range of different HIV strains, no matter how much it has mutated, says Moore.
HIV is covered in something called glycans that make it hard for antibodies to reach it, she explains. Think of these glycans as the hard sugar coating around a Smartie. A broadly neutralising antibody can recognise the parts of the virus that won’t change when it mutates. This allows the broadly neutralising antibody to be able to reach through that hard outer coating, bind to the virus and destroy it.
Two immunogens, given at the same time
In late January, the researchers enrolled the first of an expected 20 healthy participants, who do not have HIV, and are at a low risk for getting HIV. By mid-February, seven participants had received their first shots.
It is a phase one study, which is to say it is still very early days. A phase one trial looks at the safety of a drug or vaccine in a small number of individuals, while a phase two trial looks at safety in slightly larger groups and gives some early indication of efficacy. A phase three trial is much larger and looks mainly at efficacy.
The researchers are testing the immunogenicity – essentially the ability to elicit an immune response against HIV – and safety of the two immunogens in humans for the first time. A special adjuvant – known as SMNP – is being added to the agents to enhance their effect.
The hope is that the study results will help identify a potential vaccine candidate to test in future, larger studies, says Kassim. “We’re not going to come out of this study and say we have a vaccine that can prevent or cure HIV,” she says. “But we will have information on these immunogens that will help us in the future.”
It has already been shown that the two immunogens can target the type of antibody cells that have the potential to become broadly neutralising antibodies and essentially switch them on. Think of it as a talent finding agency, says Kassim, that can find the next “star” that can become an important broadly neutralising antibody.
The two shots are injected into the muscle of the arm on three separate visits, she says. The first is given after a rigorous health screening. The second is given one month later and the final dose is given three months later. Doing it this way, primes the immune system with the first shots and then the doses that follow boost the initial effects.
Putting ‘the puzzle pieces together’
Research studies like this one is still in the “experimental medicine” phase, Professor Linda-Gail Bekker, CEO of the Desmond Tutu Health Foundation, tells Spotlight. She says results from this study will help “put the puzzle pieces together” to get a clearer picture of which immunogens should eventually be tested in a phase three efficacy trial.
The trial is novel because of the use of two immunogens instead of one. Professor Glenda Gray, Chief Scientific Officer at the South African Medical Research Council (SAMRC), refers to it as an “ambitious and aggressive approach”. She tells Spotlight that usually researchers follow a sequential pattern, testing one immunogen, then another and eventually testing them together. The problem with this is that if they don’t work together, you’ve lost up to five years of research.
“We also have this philosophy of ‘failing fast’,” Gray says. “[I]nstead of wasting money and time and effort, we need to know whether our strategy is going to work or not in the beginning.”
A proudly South Africa trial
Beyond the cutting-edge science, it’s clear that what makes this trial so unique is the people involved.
Bekker describes the trial as “proudly South African”. She says: “It’s just terrific that we’re doing this end-to-end. We’re involving the community, the recruiters are people from the country, the people who are taking the blood are people from the country, the people who are doing the laboratory science are from the country, and we’re doing it for people in our country.”
Moore adds: “We’ve got so many people in the background working on these trials at the clinical sites and here in my lab…There’s this huge mass of people all working together on this trial.”
BRILLIANT 011 is one of 22 trials currently running at the Groote Schuur Hospital site, Henriette Kyepa the Unit Manager for the site, tells Spotlight. The doors open at 07:00 and the last participant leaves by 15:00, and since at least 40 participants are being seen each day, she describes the goings on as “bustling”.
The hospital has an illustrious medical history, with the first human heart transplant having been performed in the Old Main building – the Christiaan Barnard Heart Museum is just a few floors down. The Desmond Tutu Foundation’s research site has been operating at the hospital for more than 10 years.
During a tour of the unit, Spotlight was led through a waiting area, pharmacy, and two nursing areas – where patient’s vitals are checked and data captured. Staff manning the different stations were busy, but friendly and took requests for photographs in their stride. There are four doctors’ rooms and a procedure room, equipped with things like a crash cart in case anyone has a bad reaction to a drug or device that’s being tested. The site also includes private counselling rooms and a purple, gender inclusive bathroom. Down the hall, there is a hospital ward and a small laboratory, which is shared with the University of Cape Town Clinical Research Unit, for patients that need timed blood draws for studies where drug levels are being monitored.
But before they come to the site, the first point of contact for many potential trial participants – for BRILLIANT 011 and other studies – are the community recruiters. This is a team of three outreach workers led by Amelia Mfiki, who is the community liaison officer for the Desmond Tutu Health Foundation and lead recruiter. Their job is to keep the local communities updated on what the site is doing, get their feedback and to find participants who fit the eligibility criteria for different studies.
If someone is interested in a study, Mfiki explains, they are sent to the site for an information session, where the trial, eligibility criteria and the commitment required to participate is clearly unpacked. If they meet the criteria and want to participate, they go through a further informed consent process and screening. With a big smile, she tells Spotlight there has been a lot of requests for information about the BRILLIANT 011 trial.
Once enrolled, clinical trial participants will spend a lot of time with the nursing staff. Among them is Viwe Soko, a senior nurse who says “making people smile” is part of his job.
How they’ll test if it works
The BRILLIANT 011 trial participants will need to come back roughly two weeks after each jab to have white blood cells – which contain the cells that can become broadly neutralising antibodies – extracted from their blood through a process called leukapheresis. This is how the researchers are looking for those “star” antibodies that have the potential to become broadly neutralising antibodies.
Basically, the leukapheresis machine draws a participant’s blood and runs it through a centrifuge that separates the white blood cells from all the other cells in the blood, explains Moore. The white blood cells are collected into a sterile blood bag, while the rest of the blood goes back into the participant. (Here’s a useful video showing how it works).
Hundreds of millions of white blood cells are collected each time a participant goes through this process, according to Moore. “The reason we need a crazy number [of cells] is because the responses that we’re looking for are rare as hen’s teeth,” she says.
The cells are then processed in the laboratory at Groote Schuur Hospital and sorted into different tubes containing 20, 50 and 100 million cells respectively, frozen, and then sent more than 1 000 km away to Moore’s laboratory at Wits University in Johannesburg.
Once there, the thawed antibodies are run through a special machine called a flow cytometer, which is able to spit out individual cells of interest via an ultra-thin stream. The cells are mixed with a dye to make them easy to spot, says Moore. Then a laser and computer, under the supervision of a highly trained scientist sorts the cells to isolate the types of antibodies they’re interested in.
These precursors of the broadly neutralising antibodies are “structurally weird”, said Moore, some of them have really long “arms” that can reach through HIV’s hard outer coating, or really short “arms” to get close to it.
At the end of the process, there might be 100 relevant cells which then go through a process called next generation sequencing. The researchers are looking for two specific genetic signatures that will show that the right antibody was produced. Moore likens this to a cell that has “a purple head and an orange arm” and is extremely rare. Once they find all the cells with these signatures, they count them.
At its core, Moore says, they’ll know the immunogens have worked if they find more “cells with purple heads and orange arms” than has been seen in other vaccine trials that only used one immunogen.
“I think this is some of the most important work I’ll ever do,” Moore says. “It feels like 20 years of basic science has finally paid off.”
She has been monitoring the antibody responses for the CAPRISA 002 cohort for the last two decades. It is within this cohort, that a handful of women living with HIV who had naturally produced broadly neutralising antibodies were discovered and since studied. This is part of the foundation on which the BRILLIANT 011 trial has been built.
Because of all the lab work and specialised equipment required, this kind of study is expensive to run. For the study period, it costs about R1 million for each participant to be in the trial, according to Gray. This trial has a budget of R25 million, the bulk of which has been supplied by the Gates Foundation. Some emergency funding from the SAMRC was used to make up the rest.
‘Nobody gets the urgency’ like South Africa
This amount is a far cry from the five-year USAID grant worth over $45 million, that was originally awarded to the BRILLIANT Consortium in 2023. This ambitious African-led Consortium, led by Gray and run out of the SAMRC, had big plans for HIV vaccine research and capacity development across Sub-Saharan Africa. As Spotlight previously reported, the Consortium planned to conduct three HIV vaccine trials, about one a year, and develop laboratory capacity for this kind of research across the African continent.
In the end, they only had the USAID grant for a year, just enough time to set everything up for BRILLIANT 001, a much flashier version of the trial that is currently running. It was set to take place at sites in Uganda, Kenya, Zimbabwe, South Africa and Nigeria, and recruit 60 participants, according to Gray.
“We were actually due to start it [BRILLIANT 001] in February of 2025. And then it was stopped,” Bekker says. “And so, we went through the five stages of grief and finally got to the point of acceptance. And with acceptance came a real sort of verve to try and find alternative funding.”
Essentially, the researchers were racing against the clock on multiple fronts.
The immunogens, which had been donated by labs in the Netherlands and the United States were already in the country and had expiration dates that meant the study could not be delayed indefinitely (in the end the study would start in time for this to no longer to be a concern).
But more importantly there was the roughly eight million people living with HIV in the country.
“I think nobody gets the urgency like a South African,” Bekker says. “It’s very real in our lives that this virus continues to devastate [and] change the lives of people we love and serve and work with. So that sense of urgency is very real within us.”
The team wrote up a new funding proposal and study protocol, which Bekker describes as a much lighter version, “pared down to the absolute bones”. They presented this to the Gates Foundation, which agreed to provide funding for this leaner version, and the team pushed to get everything else in place.
Gray weighs in on how, just as the process was taking off again and the protocol had been submitted to the South African Health Products Regulatory Authority (SAHPRA), which has to review and approve all clinical trials conducted in the country, the adjuvant they had planned to use was recalled by the manufacturer. Luckily, they had had some warning this might happen and had a protocol using another adjuvant ready to go. And just a year after the original trial was meant to start, they were able to kick off BRILLIANT 011.
“No one works in these timelines,” says Gray, adding that part of the reason they were able to pull this off was because of how well the team works together. “Everyone puts in more than their pound of flesh, they work incredibly hard…everyone believes in the kind of programme that we’re trying to put together,” she adds.
‘I want to help my community’
Participants for the 011 trial are reimbursed for their time and travel using a SAHPRA approved model. However, Kassim says there appears to be a more altruistic motive among participants, with some sharing sentiments like: “I want to help people. I want to help my community.”
Bekker notes a similar theme that’s held true over the last two decades of HIV vaccine research. “It’s incredibly encouraging, but it’s also incredibly humbling that, in a country like ours, where people have so many other challenges, that they could … [have] an entirely altruistic motivation, that they are digging deep within themselves and saying: ‘I’m motivated because I want to see an end to the suffering’.”
“If we truly want to bring this epidemic to an end and eliminate transmission, we will need a vaccine,” says Bekker. “And imagine, a world where you could get your vaccination, at age 10 or even younger, and then not have to think about HIV ever again.”
Disclosure: The Gates Foundation is mentioned in this article. Spotlight receives funding from the Gates Foundation but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council.
Griffith University researchers may have unlocked the secret to treating sepsis, with a Phase II clinical trial in China successfully concluding with promising results.
Photo by Alex Fedini on Pixabay
Griffith University researchers may have unlocked the secret to treating sepsis, with a Phase II clinical trial in China successfully concluding with promising results. The sepsis drug candidate, a carbohydrate-based drug called STC3141, was co-developed by Distinguished Professor Mark von Itzstein AO and his team from Griffith’s Institute for Biomedicine and Glycomics, and Professor Christopher Parish and his team at The Australian National University.
“The trial met the key endpoints to indicate the drug candidate was successful in reducing sepsis in humans,” Professor von Itzstein said.
STC3141 was administered as an infusion via a cannula and counteracted a significant biological molecule release phenomenon which occurred in the body during the course of sepsis.
The small-molecule experimental drug was a carbohydrate-based molecule and could treat sepsis by reversing organ damage.
Sepsis was known to affect millions of hospitalised patients across the world each year and occurred when the body’s immune response to an infection attacked and injured its own tissues and organs.
“When sepsis is not recognised early and managed promptly, it can lead to septic shock, multiple organ failure and death,” Distinguished Professor von Itzstein said.
The trial, conducted by Grand Pharmaceutical Group Limited (Grand Pharma), involved 180 patients with sepsis, one of the leading causes of death and long-term disability worldwide.
Currently, there is no specific anti-sepsis therapy available, and sepsis is considered a clinical unmet need.
Professor von Itzstein said Grand Pharma would now look to progress to a Phase III trial to continue testing the efficacy of the novel treatment.
“It’s hoped we could see the treatment reach the market in a handful years, potentially saving millions of lives,” he said.
Executive Director of the Institute for Biomedicine and Glycomics, Professor Paul Clarke, said: “I am thrilled to see the results of the trial which ultimately aims to save lives.”
“The Institute and its researchers collectively work on translational research to deliver real and immediate impacts both in Australia, and globally to transform lives.”
The new cochlear implant is implanted invisibly under the skin, unlike this standard design. Photo by Brett Sayles
A highly sought-after clinical trial testing completely under-the-skin cochlear implants is expanding earlier than expected. Promising preliminary results showed no serious adverse events or unexpected device effects.
The Medical University of South Carolina, which has one of the larger cochlear implant programmes in the country, is one of several sites in the United States taking part in the Acclaim study. Three patients were implanted in the first wave of the trial and have been using their devices for at least six months. Now, MUSC has the chance to enrol more.
“New patients are coming this week, and we’re going to resume device placement as soon as possible. We have people flying in from all over the country to be part of the trial as well as South Carolinians,” said Teddy McRackan, MD He’s medical director of the MUSC Health Cochlear Implant Program.
Some participants are traveling to Charleston to get the experimental implants because slots in the 56-person national trial are limited, and they like the idea of cochlear implants without external parts.
The Acclaim implants would be the first such devices to hit the market if they obtain approval from the Food and Drug Administration. McRackan said they use the body’s natural hearing bone movements to detect sound instead of the external microphones used in traditional cochlear implants.
“The trial has made it clear that hidden cochlear implants appeal to a lot of people,” said audiologist Elizabeth Camposeo, AuD. She’s assistant director of the MUSC Health Cochlear Implant Program.
“Seeing our patients going through this trial just feels like such a massive opportunity. I didn’t know how hard we were struggling to overcome the physical stigma of visible implants. There were many patients we screened for the trial who we could help with a traditional implant but who did not want any part of it. These people are profoundly hearing impaired, like 10 out of 10 terrible hearing, and they absolutely would not consider a traditional implant.”
They have plenty of company. Just 5% of adults in the United States who could hear better with traditional cochlear implants have them, according to the American Cochlear Implant Alliance.
To measure the Acclaim implants’ effectiveness, participants will check in for testing at one month, three months, six months, one year and two years after their implants are activated. Implantation requires surgery and then one month for healing before doctors turn on the devices.
Once the implants are activated, Camposeo said researchers will start analysing data about how much sound they detect and how well patients understand speech. “Similar to when you have your eyes checked, how close are you to 20/20 vision, we check sound detection. More importantly, we test speech understanding. We play a word. You repeat it back. We play a sentence. You repeat it back in both quiet and noise, because the world is a noisy place.”
A noisy place, and a place where potentially groundbreaking devices can be developed quickly, McRackan said. “I don’t think anybody thought two years ago that the Acclaim device would be at this point now. I think it’s kind of amazing how fast things are progressing.”
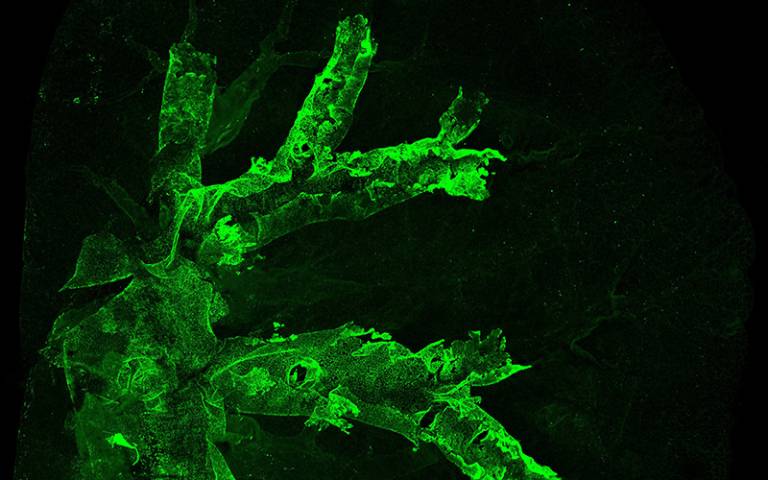
Image of a lung lobe showing cells expressing the basal cell marker Krt5 spreading. Credit: UCL.
In the UK, people at high risk of lung cancer will soon be able to receive the first ever experimental vaccine designed to prevent the disease, in a world-first clinical trial led by researchers at UCL and the University of Oxford.
The research team has been awarded up to £2.06 million from Cancer Research UK, supported by the CRIS Cancer Foundation, to run a clinical trial of LungVax over the next four years.
This phase I trial will investigate the best dose of LungVax to give to people at high risk of lung cancer, as well as looking for any potential side-effects from different doses of the vaccine.
The trial is expected to begin in summer 2026, subject to regulatory approvals.
Professor Mariam Jamal-Hanjani, co-founder and lead for the LungVax clinical trials, from UCL Cancer Institute, UCLH and the Francis Crick Institute, said: “Fewer than 10% of people with lung cancer survive their disease for 10 years or more. That must change, and that change will come from targeting lung cancer at the earliest stages.
“The LungVax clinical trial is the crucial first step in bringing this vaccine to people at the highest risk of the disease. We will be looking carefully at how people respond to the vaccine, how easy it is to deliver, and who might benefit from it most in the future.
“Preventative vaccines will not replace stopping smoking as the best way to reduce the risk of lung cancer. But they could offer a viable route to preventing some cancers from emerging in the first place.”
Lung cancer cells are different from normal cells. They have ‘red flag’ proteins made by cancer-causing mutations within their DNA. These are called neoantigens and tumour associated antigens and appear on the surface of cells at a very early stage of lung cancer formation.
The LungVax vaccine carries a series of genetic instructions which train the immune system to recognise these tumour antigens on the surface of abnormal lung cells. In trialling the vaccine, the aim is to get the immune system to recognise these early abnormal cells, and kill them before they start to become cancer. The vaccine uses technology developed by the University of Oxford during the COVID-19 pandemic to deliver these instructions to the immune system.
Professor Sarah Blagden, co-founder of the LungVax project from the University of Oxford, said: “Lung cancer is lethal and blights far too many lives. Survival has been stubbornly poor for decades. LungVax is our chance to do something to actively prevent this disease.
“Years of research into the biology of cancer, understanding the fundamental changes which occur in the very earliest stages of the disease, will now be put to the test. This funding means that, for the first time, we hope that people will be able to receive LungVax in clinical trials from next year.”
To find out how safe and effective the vaccine is, the trial will initially focus on people who have been diagnosed with early-stage lung cancer and have had it successfully removed but are at risk of it returning. The vaccine will also be tested in people who are undergoing lung cancer screening as part of the NHS Lung Cancer Screening Programme in England.
If the trial delivers promising results, the vaccine could then be scaled up to larger trials for people at risk of lung cancer.
There are around 48 500 cases of lung cancer every year in the UK. Around 72% of lung cancers are caused by smoking, which is the biggest preventable cause of cancer worldwide.
Graeme Dickie, 55, from Kilbarchan in Renfrewshire, is helping the scientists prepare for the LungVax clinical trial. In 2013, aged 42, he was diagnosed with stage II lung cancer. By 2017, it had progressed to stage IV. He has never smoked. Over the years, he’s undergone surgery to remove part of his left lung, and more than 80 rounds of chemotherapy. When those treatments stopped working, Graeme began a new targeted treatment drug, mobocertinib, that he continues with today.
Graeme said: “I am proof that research saves lives. I have been able to enjoy many more happy years with my family thanks to scientists working hard, year after year, to bring new tests and treatments.
“For me, research is vital. I won’t be able to benefit directly from LungVax personally, but I know that my story will help others to access better interventions at an early stage.”
Image of a lung lobe showing cells expressing the basal cell marker Krt5 spreading. Credit: UCL.
A UK trial involving 16 500 mechanically ventilated intensive care unit (ICU) patients found no 90-day survival benefit for conservative supplemental oxygen over usual oxygen therapy. Nevertheless, the study, published in JAMA, did demonstrate the accuracy and cost-effectiveness of conducting a large trial with a simple intervention.
Oxygen is one of the most commonly administered treatments to patients in ICUs, but liberal oxygen therapy to avoid the risks of hypoxaemia may lead to harm, so finding the right level could optimise outcomes. Trials to date have shown mixed results.
For COVID patients admitted to the ICU with severe hypoxaemia, survival without life support was extended with conservative oxygen therapy. In a paediatric ICU study, conservative oxygen therapy resulted in a reduction in a composite of organ support at 30 days or death. A meta-analysis of 13 trials showed no differences between liberal and conservative oxygen therapy.
Even with just a small difference in survival benefit, with tens of millions of patients mechanically ventilated in the ICU would still mean significant numbers of lives saved. Other tests of new drugs and procedures in the ICU are hampered by high cost, as Seitz et al. noted in an accompanying editorial, so this sort of trial comparing two approaches to a common therapy is much more affordable.
The UK Intensive Care Unit Randomised Trial Comparing Two Approaches to Oxygen Therapy (UK-ROX) trial was initiated to determine if there was a difference between conservative and usual oxygen therapy.
The trial randomised 16 500 patients across 97 ICUs in the UK to either conservative oxygen therapy or usual oxygen therapy, in adults receiving mechanical ventilation and supplemental oxygen in the ICU. The primary outcome was mortality at 90 days. Conservative oxygen therapy targeted a peripheral oxygen saturation (Spo2) of 90% (range, 88%-92%), while usual oxygen therapy was at the discretion of the treating clinician.
Patients were early in mechanical ventilation (median, 5 hours), were severely ill (median predicted mortality risk, 35%), had a range of critical illnesses (eg, > 5000 patients with sepsis and > 1500 patients with hypoxic-ischaemic encephalopathy) and with significant hypoxaemia (eg, > 11 000 patients with a Pao2:Fio2 ratio, consistent with acute respiratory distress syndrome). Obtaining informed consent from the patients was, of course, largely not feasible, so this requirement was waived for the study.
Exposure to supplemental oxygen was 29% lower for those in the conservative oxygen therapy group compared with the usual oxygen therapy group. Of the patients randomised to conservative oxygen therapy, 35.4% died by 90 days compared with 34.9% of patients receiving usual oxygen therapy.
No differences were seen for secondary outcomes, including ICU stay, days free of life support and mortality at various time points. No interactions for confirmed or suspected COVID, ethnicity or other illnesses were observed.
Post hoc analysis showed weak evidence of increased harm from conservative oxygen therapy among the first 10 patients in each site but no difference for the random enhanced data collection sample compared with standard data collection.
Seitz et al. pointed out that the high level of adherence to the conservative target resulted in a mean oxygen saturation of 93.3%, versus 95.1% for usual care. The differences in oxygen saturation (1.9%) and Fio2 (0.04) between the trial groups in UK-ROX were about half the magnitude of some prior trials, due to not aiming for widely separated targets, and usual care varies considerably depending on location and clinical considerations.
Therefore, the researchers concluded that the findings do not support an approach of reducing oxygen exposure by targeting an Spo2 of 90% in mechanically ventilated adults receiving oxygen in the ICU. They suggest that future research may involve using AI to determine specific situations where conservative or liberal oxygen therapy may have beneficial outcomes.
References:
Martin DS, Gould DW, Shahid T, et al. Conservative Oxygen Therapy in Mechanically Ventilated Critically Ill Adult Patients: The UK-ROX Randomized Clinical Trial. JAMA. 2025;334(5):398–408. doi:10.1001/jama.2025.9663
Seitz KP, Casey JD, Semler MW. Patient, Treatment, Outcome—Large Simple Trials of Common Therapies. JAMA. 2025;334(5):395–397. doi:10.1001/jama.2025.9657
Millions of adults around the world are diagnosed with ADHD every year, and there is a great need for research in the field. Yet much clinical research on adult ADHD suffers from serious methodological shortcomings that make it difficult to use the results in practice, researchers from the University of Copenhagen and the University of Sao Paulo show in a new study.
Originally developed for children, the diagnosis of ADHD is often difficult to make in adults. This is partly because the diagnostic criteria are based on behaviour in children. When diagnosing adults, however, these criteria are often based on adults’ subjective experiences, eg, of having difficulty concentrating or being very impulsive.
“The rising number of adults diagnosed with ADHD raises important questions about diagnostic validity – especially since many were never identified in childhood and are now seeking help, sometimes prompted by ADHD content on social media. That made us curious: how have randomised controlled trials on ADHD dealt with this diagnostic challenge?” explains Dr Igor Studart, who is first author of the study published in European Psychiatry.
Moreover, ADHD shares its symptoms with a number of other mental disorders such as depression, schizophrenia, and bipolar disorder, making it crucial to exclude these disorders when diagnosing ADHD. This requires a thorough diagnostic assessment by an experienced psychologist or psychiatrist.
But it is not always the case that such a thorough assessment is made. The study now shows that even psychiatric research into ADHD often neglects this fundamental work.
“We have examined how 292 of the most credible studies in evidence-based medicine – the so-called randomised controlled trials – diagnosed their adult subjects,” says Professor of Psychiatry and Consultant Psychiatrist Julie Nordgaard, who conducted the study together with Associate Professor and Senior Researcher Mads Gram Henriksen and Dr Igor Studart.
She continues:
“We conclude that half of the studies did not ensure a broad and thorough diagnostic assessment of the patients before the trial to rule out other disorders. This means that they can’t actually know, if their subjects have other mental disorders such as depression or schizophrenia. And that’s not all. More than half of the studies included subjects, who have also been diagnosed with other mental disorders, making the diagnosis even more difficult to allocate”, Julie Nordgaard explains.
According to the researchers, these methodological shortcomings are problematic, because they imply that it is impossible to know which disorders and symptoms the treatment investigated in these trials potentially had an effect on.
“This makes the research results from many of these clinical trials difficult to utilise. Yet, the results of randomised controlled trials are considered particularly trustworthy, and they may inform the guidelines we use to treat adult ADHD patients, even though the results from many of these trials should be assessed very carefully,” says Mads Gram Henriksen.
A need for consistent and robust diagnoses
According to the researchers, one of the problems with the diagnostic assessment in many of the clinical trials is that it seems to have been carried out by people who are not trained to do so. And often with methods that are not thorough enough.
“In 61% of the studies, they do not state who diagnosed the subjects. In only 35% of the studies, it is stated that a psychiatrist or psychologist made the diagnosis. But diagnostic assessment should always be performed by an experienced professional with the necessary training to ensure that the diagnosis is made correctly, and this should be stated in the studies’ method section,” explains Mads Gram Henriksen.
In some cases, the assessment and thus the diagnosis was made by the subject themselves, and in one particularly egregious case, it was done with the help of a computer, the researchers explain.
“In psychiatry, we really need that all diagnoses, not just ADHD, are made with the same uniform criteria and by trained professionals. Otherwise, we cannot rely on the results or compare them across studies,” says Julie Nordgaard and concludes:
“Especially in a situation where a diagnosis such as ADHD in adults is increasing, we need to be very thorough and have a solid foundation. Otherwise, we risk too many people getting a wrong diagnosis and not being able to give them the most effective treatment. Or they risk receiving unnecessary treatment that causes side-effects.”