This African Vaccination WeekSanofi South Africareaffirms its commitment to vaccine awareness, access and public health partnerships to close the immunisation gap
Photo by Mufid Majnun on Unsplash
Johannesburg, 20 April 2026 – Marked each year from 24 to 30 April, African Vaccination Week focuses on the need for equitable access to lifesaving vaccines across the continent.
It’s also a timely reminder that while vaccination remains one of the most effective tools in public health, gaps in coverage are a real concern, in South Africa and globally. UNICEF says immunisation prevents an estimated 4.4 million deaths every year,1 yet WHO reported that 14.3 million children worldwide missed out on all routine vaccines in 2024.2 Global coverage for the third dose of DTP-containing vaccine stood at 85% in 2024, while first-dose measles coverage was 84%.2
“Vaccination remains one of the smartest and most effective investments in public health,” says Jean-Baptiste Bregeon, Country Lead and Head of Vaccines, Sanofi South Africa. “Improving coverage is not only about having vaccines available. It’s about building trust, strengthening health systems, supporting healthcare workers and making sure people have the information they need to act. African Vaccination Week is a reminder that protecting lives takes sustained effort and strong partnerships, and Sanofi remains committed to playing its part in South Africa.”
In South Africa, the need is clear. The National Department of Health reported in 2024 that 80% of children in the country had received all their vaccinations by the age of one.3 That is progress, but it also means one in five children had missed one or more doses and was not fully protected. UNICEF South Africa has separately highlighted the urgency of reaching children who have missed routine immunisation entirely. There were 58,000 more zero dose children in 2024 and 278,000 without vaccination, leaving them vulnerable to vaccine preventable diseases.4 Measles vaccination coverage, for example, declined from 80% in 2023 to 76% in 2024.4
Recurring outbreaks of measles, cholera, polio and diphtheria have added pressure to the health system, while disruption to routine immunisation has left more children vulnerable to vaccine-preventable diseases and increased the risk of further outbreaks.5
This year’s campaign aims to intensify vaccination and surveillance activities in districts with high numbers of under-vaccinated and unvaccinated children. Vaccines included in South Africa’s national immunisation schedule are available free of charge at primary healthcare facilities.
Sanofi says its focus in South Africa over the next two to three years will be to continue supporting the Department of Health to improve vaccine coverage across the country, with a focus on access, availability, education and awareness.
“Improving vaccine uptake requires a practical, local approach that recognises the realities of South Africa’s healthcare system, including uneven coverage, pressure on frontline services, and the challenge of reaching communities across both urban and rural settings,” says Bregeon.
That’s why partnership matters, he adds. “Improving immunisation outcomes takes coordinated action across government, healthcare providers, communities and industry. Strong supply is important, but so is public confidence, clear communication and consistent follow-through at clinic level.”
This African Vaccination Week, Sanofi calls on all South Africans to ensure their vaccinations are up to date and encourages healthcare providers to continue championing immunisation as a cornerstone of preventive health.”
To limit the damage from the US research cuts, the SAMRC mobilised a rescue fund of about R600 million.
Spotlight Editors
It has been a bruising year or so for medical researchers in South Africa with the US pausing, cancelling, and then resuming some grants. But as bad as things were, what played out wasn’t the worst case scenario, and momentum is now building toward recovery.
For decades, the United States government has been the world’s top funder of medical research. When it started cutting research funding last year, South Africa was caught in the firing line. This is because the US administration decided to specifically target South Africa, but also because South Africa was uniquely exposed due to the sheer volume of US-funded research here.
Over recent decades, South Africa built an impressive network of research groups and infrastructure to support high quality research – all underpinned by a strong regulatory environment, several good universities, and many productive partnerships with research groups from across the world. All this, plus the fact that we have large TB and HIV epidemics, means that South Africa was, and still is, one of the best places in the world to conduct research on these two diseases.
But a weakness of South Africa’s impressive research infrastructure was its overreliance on US funding.
To be clear, this was not an overreliance on aid or charity. South African researchers won grants from the US by coming out on top in rigorous and highly competitive selection processes. Much of the research done here benefited people around the world, including in the US.
Instead, the thing that we overly relied upon was that the US would continue to make medical research grants in a way that is rational and in our common interest.
There was much chaos and uncertainty last year with the pausing, cancellation, and resuming of grants. One small positive is that bad as things were, what played out wasn’t the worst case scenario we seemed to be heading for. At least some projects got their funding flows restored. You can read more about that in this Spotlight article.
But there is no doubt that the situation remains very bleak. While some studies that were already underway will be completed, it seems very unlikely that the US will fund any new studies in South Africa in the coming years. Given the historic scale of US investment here, the total volume of clinical trials conducted in South Africa will almost certainly fall precipitously.
Charting a new course
One ray of light in all this has been the response from the South African Medical Research Council (SAMRC) – probably the best run of all the entities linked to the Department of Health.
To limit the damage from the US research cuts, the SAMRC mobilised a rescue fund of about R600 million. This includes major contributions from National Treasury, the Gates Foundation, the Wellcome Trust and the ELMA Foundation.
Some of this funding has already helped sustain dozens of research projects and protect vital expertise during a period of instability. The current funding supports work in HIV, TB, newborn and child health, as well as non-communicable and other infectious diseases.
One example is a cutting-edge HIV vaccine clinical trial that began in January at the Desmond Tutu Health Foundation’s clinical research site at Groote Schuur Hospital in Cape Town. While still in its early stages, the study aims to help piece together what an effective HIV vaccine might look like.
Beyond the SAMRC’s efforts, universities and research institutions have also stepped in, raising funds to safeguard projects and retain skilled staff whose jobs were at risk.
Even so, we are still facing a massive net loss to money for medical research in South Africa.
What to do?
Funding from international partners will remain vital in South Africa. For now, the US government still invests substantial funds in South Africa, as does several philanthropies and the European Union, through the European & Developing Countries Clinical Trials Partnership. There are also new partnerships such as one we recently reported on between South African and Korean researchers.
Such partnerships are not just about money – science thrives where there is collaboration across national borders. In fact, almost all of the most important TB and HIV clinical trials conducted in South Africa in the last two decades were collaborations between researchers from multiple countries. No matter how you slice it, collaboration with international partners will remain an essential foundation of the medical research landscape in South Africa.
The problem was never that South African researchers took too much money from the US or other donors, or worked too closely with researchers based in other countries. One might quibble on details here and there, but on the whole, US-South African research collaboration in recent decades has been a resounding success.
Rather, the problem was that we invested so little of our own funds that we became overly vulnerable to changes in external funding.
Professor Ntobeko Ntusi, president and CEO of the SAMRC, previously told Spotlight that the SAMRC receives in the region of R2 billion from government per year, including funds from both the Department of Health and the Department of Science and Innovation.
Unlike so many parts of our government, the SAMRC is a well-run entity that got clean audits in each of the last five years. This strongly suggests that money allocated to it won’t be wasted or looted. If we understand recent messaging from the Finance Minister and National Treasury, this is precisely the kind of clean government spending that should be rewarded in future budgets.
Relative to health budgets more generally and to what government has historically spent on entities such as South African Airways, the SAMRC’s budget is tiny. As far as we can tell, the current funding level is largely a product of history – apart from the still widespread atmosphere of austerity, there really isn’t any other reason why the budget shouldn’t be scaled up over the next three years to be double what it is now.
The SAMRC supports a sector in which South Africa has truly world-class capacity – capacity that as we speak remains under threat. More than just the research studies and the jobs for young scientists, what is at stake here is the idea of South Africa as a place where we can do world-class medical research. Allowing funding cuts to extinguish this bright spark, would feel like a victory for Afro-pessimism.
The reality is that if President Cyril Ramaphosa and National Treasury seizes the opportunity, the shock of the US funding cuts could be turned into a bright new beginning for medical research in South Africa – all at a price that in relative terms is very low. Let’s hope they have the vision and ambition to seize the day.
Disclosure: The Gates Foundation is mentioned in this article. Spotlight receives funding from the Gates Foundation, but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council.
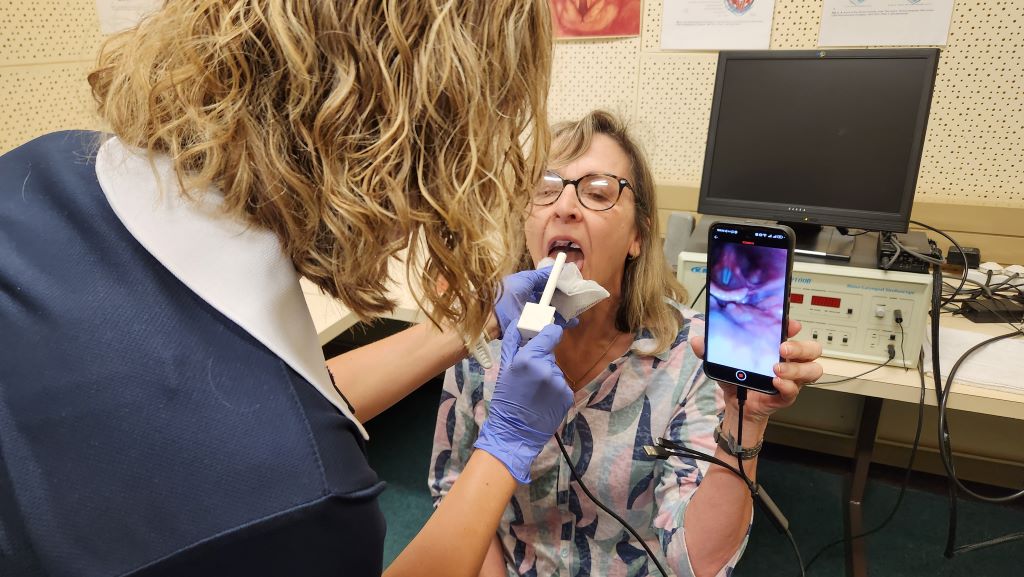
Dr Maria du Toit takes a close-up look at vocal cords, capturing high-resolution images and video using widely available mobile technology. Traditionally, this type of examination requires expensive equipment and specialist doctors, making it difficult to access in many parts of South Africa
Ahead of World Voice Day on 16 April, researchers at the University of Pretoria (UP) are inviting the public to take part in free voice checks using a new, locally developed device that could significantly expand access to vocal health services across South Africa.
The groundbreaking, low-cost, smartphone-compatible device, which is currently being tested as part of ongoing research, enables clinicians and trained users to take a close-up look at the voice user’s vocal cords by capturing high-resolution images and video using widely available mobile technology. Traditionally, this type of examination – known as laryngoscopy – requires expensive equipment and specialist doctors, making it difficult to access in many parts of South Africa.
“Your voice is something you use every day – whether for work, social interactions, or simply being heard. Yet many people ignore early warning signs of vocal problems,” says Professor Jeannie van der Linde, who is leading the research team and is Head of UP’s Department of Speech-Language Pathology and Audiology in the Faculty of Humanities.
Voice disorders are more common than many people realise. Prof Van der Linde adds: “International estimates suggest that up to one in five people will experience a voice problem at some point in their lives, with higher risk for those who rely heavily on their voices for work, such as teachers, healthcare workers and call centre agents. Despite this, access to specialised diagnostic services remains limited, particularly outside major urban centres.”
The research and device are part of a broader effort to rethink how vocal health services are delivered in South Africa. “Our aim was to develop a solution that is more portable, more affordable and easier to integrate into different healthcare contexts,” says Dr Maria du Toit, a Lecturer in Speech-Language Pathology and member of the research team.
“Many people ignore early signs like hoarseness or vocal fatigue, often because they don’t have easy access to assessment services,” Dr Du Toit says. “If we can identify these issues earlier, we can intervene sooner and potentially prevent more significant problems from developing.
The development of the device forms part of ongoing efforts within the department to explore how mobile anddigital technologies can be used to increase the availability of vocal health assessment and care.
Dr Roxanne Malan, a postdoctoral fellow, speech therapist and research team member, highlights the importance of designing technology that balances functionality with affordability and ease of use. “We wanted to ensure that the device is not only clinically useful but also practical in a range of settings, including those withlimited resources,” she says. “The goal is to make vocal health screening more widely available without compromising on quality.”
The technology, which has not been named yet, is being developed at UP and is currently undergoing testing to compare its performance with gold-standard laryngoscopy. “We started feasibility testing in June 2025 and preliminary tests have been very positive, demonstrating that the device is usable and produces high-quality images of the relevant structures,” Dr Malan says. “It consists of a low-cost, off-the-shelf borescope – typically used industrially – adapted with a 3D-printed handle to ensure optimal placement of the scope in the patient’s mouth, as well as the correct angle for visualisation. We have also assessed its safety for human use and its ability to be properly disinfected.”
In addition to testing the device, the World Voice Day initiative seeks to increase general awareness about theimportance of vocal health. “Your voice is central to how you communicate, work and engage with others,” Dr DuToit says. “Taking care of it should be seen as an essential part of overall health, not something to think aboutonly when there is a problem.”
Dr Malan says the team’s vision is for the scope to be readily available as a screening device in public hospitalsand clinics all over South Africa and other low- and middle-income countries. “But we still foresee numerousphases of testing to ensure that it can be used by a range of healthcare professionals, and that it makes asignificant difference in the target healthcare sectors. We will name and launch it at a stage when this has beendone.”
Dr Du Toit says members of the public can support the research by booking their free voice health check. “Byattending, you’re not only taking care of your own vocal health – you’re helping researchers develop solutionsthat could make voice care more easily available to thousands of people who currently don’t have access tothese services.”
Event details: Members of the public are invited to take part in free voice checks on World Voice Day, 16 April 2026, at the Department of Speech-Language Pathology and Audiology at the University of Pretoria’s Hatfield Campus.
Participants will have the opportunity to learn more about their vocal health and contribute to research that aims to make voice care more accessible across South Africa.
Who should consider a voice check?
This free check is especially recommended for:
● Teachers and lecturers
● Singers and performers
● Healthcare workers
● Clergy and public speakers
● Call centre workers
● Anyone who uses their voice extensively
You should also consider attending if you:
● frequently experience hoarseness or voice changes;
● feel your voice tires easily;
● have ongoing throat discomfort when speaking; and/or
● simply want reassurance that your voice is healthy.
Despite South Africa’s laws and policies, access to healthcare remains an issue, particularly for non-citizens. Photo by Hush Naidoo on Unsplash
By Teri Brown and Thembi Mahlathi
The media has reported several incidents where people were turned away at public healthcare facilities because they did not possess South African identity documents. As related cases slowly grind through the courts, Teri Brown and Thembi Mahlathi of SECTION27 connect the dots between what the law says and what people are experiencing.
Over the years, many migrants and undocumented people have reached out to SECTION27, where we both work, for assistance. These were often pregnant women, lactating mothers and children under six years, who were denied access to healthcare facilities.
Initially, it was easy to simply write a letter to hospital and clinic personnel where our clients were being denied access. But as time went on, the situation got significantly worse and more migrants were being denied access to public healthcare facilities. Writing letters and asking for meetings clearly wasn’t enough anymore.
We went to court and in April 2023 got an order in which the South Gauteng High Court held that important sections of the National Health Act applies to all pregnant women, lactating women and children under the age of six years, irrespective of their documentation status. This affirmed that in South Africa, they have the right to access free healthcare services at all public health establishments, including hospitals and clinics.
Public sector hospitals and clinics are required to assess the status of migrants and then apply a lawful means test to determine the healthcare services that can be offered to them. However, this does not appear to be done routinely. Instead, particular focus is often placed on South African identity documents, while other forms of documentation held by migrants are disregarded.
There have been incidents where entry to facilities such as Rahima Moosa Mother and Child Hospital in Coronationville and South Rand Hospital in Rosettenville and several clinics across Gauteng have been denied to people, including South African nationals who have the necessary documentation.
Furthermore, we are aware that to avoid being refused healthcare and to demonstrate the urgency of their need for treatment for themselves or their kids, migrants have sometimes been forced to disclose their HIV status – information which they would otherwise have kept private.
In mid-2025, we started receiving a surge of calls from clients complaining about not being able to enter public sector clinics that they were previously assisted at. They informed us that a group of people stationed outside these clinics requested their identity documents, and when they produced their documents confirming either their refugee status or asylum seeker status, they were unlawfully prevented from entering the clinics. These group of people explicitly told them that they should go to a private clinic for treatment or go back to their home country.
Thus, two years after the April 2023 court order, the denial of access to healthcare had worsened, as it was not only women and children who could not access clinics, but anyone who could not provide South African identity documentation. The situation was also exacerbated by the fact that it wasn’t just healthcare staff denying access anymore, but vigilante groups stationed outside healthcare facilities.
Despite the crisis being widely reported, the state failed to address it effectively. We had no choice but to go back to court, and again the court found in our favour.
In December 2025, the South Gauteng High Court ordered the state to take immediate and decisive action to end the obstruction of access to public healthcare facilities in Gauteng. The case was brought by the civil society organisations the Treatment Action Campaign, Doctors Without Borders, and Kopanang Africa Against Xenophobia (the applicants), all represented by SECTION27.
In this landmark judgment, Judge Stuart Wilson concluded that the state entities tasked with upholding the constitutional mandate to safeguard everyone’s right to access healthcare had failed to prevent the obstruction of access to public health facilities. Consequently, this failure was in violation of the constitutional rights of patients seeking care at the Yeoville and Rosettenville clinics.
Despite this court order, our monitoring found ongoing vigilante activity at the two clinics. The applicants then launched an urgent contempt application, heard in March 2026, arguing that the state had failed to fully comply with Judge Wilson’s court order.
Following this, a court ordered settlement agreement was reached with the Gauteng Department of Health and other respondents. Among other things, it required the authorities to take reasonable steps to ensure safe and unhindered access to the Yeoville and Rosettenville clinics, and to report on the implementation by 18 May 2026. It also makes provision to continue legal proceedings if necessary to enforce full compliance with Judge Wilson’s order.
The laws governing healthcare for migrants in South Africa
Taking a step back from this case, and its specific set of facts, it is worth remembering that South African law really does provide extensive protection to migrants who need to access healthcare services.
The right to access healthcare services is guaranteed by section 27 of our Constitution, which states that everyone has the right to have access to healthcare services, and that no one may be refused emergency medical treatment. The term “everyone” is not restricted to South Africans only. It includes everyone within the borders of South Africa, regardless of their nationality.
This right extends to all children living in South Africa under section 28(1)(c) of the Constitution. This guarantees all children access to basic healthcare services dependent on the availability of resources, to which they can never be completely denied.
After the Constitution, the most important piece of healthcare legislation relevant to migrants is the National Health Act (NHA). The NHA assists in giving effect to the constitutional right to basic healthcare services by outlining who can receive services at public clinics free of charge. It obligates the provision of free healthcare services to women who are pregnant or breastfeeding, or children under six. Moreover, the NHA requires that free primary healthcare be provided to those without medical aid. It also makes it clear that those working in healthcare cannot refuse any person emergency medical treatment.
Along similar lines, South Africa’s Refugees Act states that a refugee is entitled to full legal protection, which includes the rights set out in the Bill of Rights, except those reserved for citizens. The Act formally acknowledges that refugees are entitled to the same basic healthcare services and primary education that South African citizens receive. While the Act does not expressly cover undocumented migrants, it is grounded on the principle of non-discrimination, which supports equal access to essential services.
The denial of healthcare services has significant impacts on many aspects of people’s lives. Migrants often become so desperate to receive care that they feel compelled to disclose their HIV status, which infringes on their rights, particularly the constitutional rights to privacy and dignity. It also creates feelings of stigma and discrimination, further marginalising people who are often already vulnerable.
There are also direct health consequences. Denying treatment to a migrant not only negatively impacts that person’s health it can also result in the continued transmission of infectious diseases to both other migrants and South Africans. For example, HIV and TB typically become non-infectious a while after someone starts treatment. Deciding not to treat someone ends up harming everyone. As untreated conditions worsen, it may require emergency medical attention that could have been avoided through early treatment. All of this places extra pressure on an already fragile health system – extra pressure that could be avoided by providing more migrants with healthcare services as soon as they need it.
The failure to provide healthcare services also affects migrants’ livelihoods and well-being. For those who run their own businesses, being unable to access treatment may prevent them from working altogether and could lead to them and other people, possibly South Africans, losing their jobs. Ultimately, this has a ripple effect on the country’s economy, job security, and perpetuates cycles of poverty and vulnerability.
At its heart then, this issue is about who we choose to be as a society. Turning people away at their most vulnerable moments erodes not only their dignity, but also their humanity and ours. In a country built on the values of equality and dignity, we cannot allow this attack on our basic humanity and decency to succeed. We are, and must be, better than that.
*Brown is a legal researcher and Mahlathi is a paralegal with SECTION27. In the court case discussed in this article, SECTION27 represented the Treatment Action Campaign, Médecins Sans Frontiers, and Kopanang Africa Against Xenophobia.
Note: Spotlight is published by SECTION27, but is editorially independent – an independence that the editors guard jealously. Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.
Republished from Spotlight under a Creative Commons licence.
Many regions in the Northern Hemisphere experienced a slightly earlier start to their flu season, driven in some part by a novel variant of influenza A(H3N2). As our flu season also kicks off slightly earlier than usual, Spotlight reports on the detection of this variant in South Africa and what we might expect from this year’s flu season.
As the mercury slowly starts dropping across the country, so does the risk of picking up flu. For many, this might only mean a few days of illness and discomfort, but for some, especially the elderly, it can be life-threatening.
Despite temperatures throughout most of the country remaining moderate so far, this year’s flu season has started, somewhat ahead of schedule. This is according to the National Institute for Communicable Diseases (NICD) in a press release issued on Wednesday.
What we refer to as flu, is commonly caused by one of two types of influenza viruses, influenza A and influenza B. These two are further typed into different lineages, the most common for influenza A is A(H1N1) and A(H3N2) and for influenza B, the B-Victoria and B-Yamagata.
The Yamagata lineage has not been detected since 2020 and is thought to have gone extinct, said Dr Sibongile Walaza. She is a medical epidemiologist and head of epidemiology at the Centre for Respiratory Disease and Meningitis at the NICD.
A key reason why influenza viruses continue to circulate year after year is how fast they mutate and learn to dodge our immune defenses. These mutations eventually result in different subtypes of lineages that are called clades, within which there can be further sub-clades.
It was a sub-clade of the A(H3N2) virus, known as sub-clade K, that led to the flu season starting earlier than usual in some parts of the Northern Hemisphere. The World Health Organization (WHO) reported that the variant was identified in 2025 and spread fast.
“This [sub-clade] contributed to an earlier start to the influenza season in many countries, with several reporting higher‑than‑usual levels of activity. ‘Subclade K’ accounted for the majority of influenza viruses reported across regions,” the WHO stated in a press release.
Sub-clade K was also responsible for an unusual spike in flu cases in South Africa in October and November 2025. Walaza told Spotlight there weren’t enough flu cases detected to cross the seasonal threshold for an additional flu wave, but the increase so late in the year, outside of the typical flu season, was unusual.
Early start
Usually, South Africa’s flu season starts sometime in April or May and spans the winter months, said Walaza, but it is difficult to predict exactly what will happen in any particular year.
This year’s flu season officially started in the second week of March, according to the NICD’s latest report, albeit at a low transmission level for now. 134 samples were tested between 16 and 22 March. Of those, 12 (9%) tested positive for influenza, 12 (9%) were cases of RSV and 3 (2.2%) tested positive for SARS-CoV-2.
In a rather unusual occurrence, the NICD reported that the start of this year’s RSV season coincided with that of the flu season. RSV refers to respiratory illness caused by the Respiratory syncytial virus. The RSV season usually starts before the flu season, but infections can occur all year round.
“The fact that both the flu and RSV seasons are starting at the same time means clinicians could potentially see a high burden of patients with respiratory illness in medical facilities in the coming weeks,” the NICD said in the press release.
Two potential scenarios
Professor Tulio de Oliveira, the director of the Center for Epidemic Response Innovation at Stellenbosch University, said the reality is that we do not know what to expect for this year’s flu season.
“[At]t the moment, we are working with potentially two different scenarios,” he told Spotlight.
The one scenario is that we may be in for a more extreme flu season, he explained, since last year was an unusually mild season and population immunity against the viruses that cause flu may currently be lower. The other scenario, depending on which flu virus circulates, is that South Africa may have some herd immunity because of the unusual spike in flu cases near the end of last year.
In other words, it all comes down to which flu viruses, and their subtypes end up circulating.
“I think this year we’ll have the three influenza lineages [A(H3N2), A(H1N1)pdm09 and influenza B-Victoria] circulating, but in terms of which one is going to be dominant in the season, it’s difficult to tell in advance,” Walaza said.
What we know about sub-clade K
Based on what we’ve seen so far, it does seem that sub-clade K is more transmissible, but it doesn’t appear to cause more severe disease, according to Walaza. De Oliveira added that sub-clade K has between seven and 10 mutations on the surface protein that allow it to bind to a cell’s receptor and enter the body, making it more infectious.
Whether or not it will be the driver of our flu season this year remains to be seen, but Walaza said that within the sporadic cases of flu detected and sequenced so far this year, most of the cases have been sub-clade K. In an NICD report from March, of the 24 influenza samples that were sequenced between 29 December 2025 and 22 March 2026, 11 were confirmed as being sub-clade K.
Experts will be keeping a close eye on circulating flu viruses with real-time genomic surveillance.
“South Africa is considered to be one of the top virus genomic surveillance places in the world,” De Oliveira said. “[A]t the moment, we don’t see a big reason for concern [about the flu season],” he said. “We do genomic surveillance every week, both with public and private laboratories – and if we see anything unusual, that’s going to be highlighted very promptly.”
Trends seen in previous flu seasons
Overall, in the last ten years, influenza A seems to be the driver of the majority of flu cases in South Africa, said De Oliveira, usually causing a big wave of flu cases at the start of the season. This is usually followed by a smaller wave of influenza B cases. In this time period, the influenza A subtype that dominates during the flu season appears to alternate between A(H1N1) one year and A(H3N2) the following year, but it also doesn’t always follow this pattern.
Zooming in more closely, Walaza said that over the last six years, 2020 and 2021 were outliers, with reduced transmission during 2020 due to the measures taken to curb the spread of the SARS-CoV-2 virus and out of season influenza transmission in 2021. Since 2022, the number of people getting flu every year has returned to roughly similar levels as before 2020.
Last year’s flu season was slightly unusual since it had started in late March, according to Walaza, but wasn’t as intense as some of the previous years as transmission remained at a low threshold level. Flu cases peaked in mid-May and then rose again slightly in October and November.
Data on influenza comes from three sentinel monitoring programmes managed by the NICD, which cover both the public and private healthcare sectors, said Walaza. A sample of healthcare facilities in the public sector and doctors in the private sector are asked to supply swabs taken from people with influenza-like illnesses or respiratory illnesses. Some general practitioners in the private sector are also enrolled in a programme called Viral Watch.
She said that the swabs are sent to the NICD laboratory and tested for the presence of different viruses, including SARS-CoV-2, influenza, RSV, parainfluenza, human metapneumovirus and rhinoviruses. If the samples test positive for flu, the sample is further tested to identify the lineage. This data is included in the weekly reports published on their website.
Members of the public can contribute to flu surveillance through an online web platform called CoughWatch. People are invited to enroll and provide weekly information on whether they have symptoms of flu or other respiratory illnesses. This is aimed at picking up trends among people who aren’t necessarily getting sick enough to go to the doctor or clinic, said Walaza and can hopefully serve as an early warning system for increases in respiratory illnesses, including flu.
CoughWatch has already opened for enrollment this year. (More information can be found here).
Flu vaccination uptake in South Africa remains low
Each year, the WHO releases recommendations on what should be in upcoming flu vaccines for the Northern Hemisphere and then later the Southern Hemisphere, usually announced around six months before the start of the respective flu seasons.
This year’s flu shot’s formulation is a trivalent one, said Walaza meaning it contains inactivated strains of all three influenza strains, including coverage for the A(H3N2) sub-clade K. Because it contains an inactivated virus, the vaccine itself cannot give someone the flu.
The level of protection offered by flu shots vary, but generally it ranges in effectiveness against preventing infection from about 30% to 60%. This means the shot will offer most people protection from severe disease and death, but it won’t necessarily prevent them from getting sick with the flu altogether.
One of the things that makes it difficult to predict effectiveness ahead of time is the possibility that a strain might circulate that is not well covered by the flu shot. De Oliveira said this “mismatch” is what we saw play out in some of the regions in the Northern Hemisphere in their last flu season.
Despite the partial mismatch between the vaccine used in the northern hemisphere and sub-clade K, several surveillancereports from the Northern hemisphere show that the vaccine nevertheless provides some protection against severe flu caused by sub-clade K.
The WHO also recently touched on this, saying that: “While current influenza vaccines help reduce the burden of disease, their effectiveness can vary by season, product, and population group. Protection is limited to one season”. The majority of flu vaccines purchased each year are by upper-middle and high-income countries, the WHO noted.
Usually, South Africa’s National Department of Health procures about 1 million flu shots for the public health sector, said Walaza and sometimes not all these doses are used.
While flu shots are made available each year, the uptake of these shots in the private sector appears to be low. Based on data collected through the NICD’s Viral Watch initiative – last year the uptake of the influenza vaccine in the private sector, among those enrolled in the programme, was only around 3.4%. This is based on data collected from 768 people enrolled, of those, 26 had gotten a flu shot. As far as Spotlight could establish, there currently isn’t any routine publicly available data on uptake in the public sector. One study of around a thousand people aged 65 and older, found that just over 32% of them had gotten the flu jab in 2018.
Spotlight asked the National Department of Health how many flu vaccines were procured for this year’s flu season. A response had not been received by the time of publication.
Low flu vaccine uptake can in part be attributed to South Africa having much milder winters and less severe flu seasons than the Northern Hemisphere, said De Oliveira.
Lack of awareness of the flu vaccine can also play a role, according to Walaza. She encourages more education and efforts by healthcare workers to inform at risk groups of the flu shot and when it will be available.
The flu shot is recommended for people who are at risk of severe disease, including older persons, pregnant women, people who are immunocompromised or with chronic medical conditions, as well as healthcare workers. But anyone aged six months and older can get the shot.
“The influenza vaccine will be available in pharmacies from the first week of April. The early start to the season means that this year, the vaccine is only becoming available as the season is getting started, so members of the public who fall into groups at high risk for severe influenza are urged to get their vaccines as soon as possible,” the NICD press release stated.
The potential of next generation flu vaccines
Earlier this year, the WHO released results from an assessment report on the value of having improved flu vaccines. “If improved, next-generation, or universal influenza vaccines are available and widely used between 2025 and 2050, they could prevent up to [an estimated]18 billion cases of influenza and save up to 6.2 million lives globally,” the report stated.
“This assessment makes clear the potential benefits that improved influenza vaccines could offer across different settings,” said Dr Philipp Lambach, WHO technical lead of the project. “It provides all those working on future influenza vaccine investments, policy development and research priorities a common set of evidence to catalyse vaccine development.”
According to the WHO, as of February 2026, there are 46 next-generation influenza vaccines in clinical development.
It is estimated that around seven in 10 adults in South Africa have ever had depression at some point in their lifetime. Photo by Alex Green on Pexels
By Marcus Low
Around 3.8 million people in South Africa developed depression in 2024, estimate leading local researchers in a major new modelling study.
The prevalence of depression among people aged 15 and older in South Africa has dropped slightly from an estimated 5.1% in 2002 to 4.5% in 2024. While a decrease, this nevertheless means that over two million people in the country had depression in mid-2024.
When taken as a whole, there were an estimated 3.84 million new episodes of depression in South Africa in 2024. Since some people may have had more than one episode, the number of people who developed depression over the year will be slightly lower.
The estimates are from mathematical modelling published as a preprint earlier in March on medRxiv. While Spotlight doesn’t usually report on studies that haven’t yet been peer-reviewed, we made an exception because the estimates fill an important gap in our understanding of depression in South Africa and because of the stature of the authors. The new modelling drew on several nationally representative surveys of depression conducted in South Africa since 2002.
The researchers estimate that around seven in 10 adults in South Africa have ever had depression at some point in their lifetime.
“Previous studies have suggested that only 10-15% of the population ever experiences depression, but our study suggests a much higher proportion, 70%,” Dr Leigh Johnson, the lead scientist on the study, told Spotlight.
“Most of these people experience a single episode of depression and have no recurrences. The common belief is that depression is a frequently recurring condition, but this is true for only a minority of people who experience depression,” he said. Johnson is from the Centre of Integrated Data and Epidemiological Research at the University of Cape Town (UCT) and is also responsible for Thembisa, the leading mathematical model of HIV in South Africa.
The new modelling also suggests some interesting nuances regarding who is most at risk of depression. In mid-2024, prevalence in women was at 5.3%, well above the estimated 3.6% in men. Older people were significantly more likely to suffer from depression than young people.
Living with HIV has long been known to increase the risk of depression, but the modelling suggests that this effect has weakened over time as HIV treatment became more widely available. In 2010, 7.1% of people with HIV had depression compared to 4.9% in the general population. By 2024, 5.9% of people with HIV had depression, compared to 4.5% of the general population. In other words, the gap decreased from 2.2 percentage points to 1.4.
Increasing, but still very low antidepressant usage
While rates of depression have been relatively stable, the researchers estimate that antidepressant usage rates have almost tripled, from around 1% of the population using antidepressants in 2008, to 2.8% in 2024. In Europe, Australia, Canada, and the United States, rates are between 4% and 16%.
The proportion of women taking antidepressants is more than four times higher than in men – a difference that cannot fully be explained by the higher rates of depression in women. Social factors like stigma are likely playing a role.
The differences between the private and public sectors are stark. Around 11% of medical scheme members are estimated to be taking antidepressants, compared to 0.9% in the rest of the population. “Levels of antidepressant use in the uninsured population are very low, despite a substantially greater prevalence of depression in people of lower socioeconomic status”, the researchers point out.
“Our study shows quite extreme inequality in access to antidepressant treatment in South Africa, with rates of antidepressant use in the private sector being about 12 times those in the public sector. Levels of antidepressant use in the private sector are quite similar to those in high-income countries, but in South Africa’s uninsured population there are major barriers to accessing mental healthcare,” said Johnson.
One such barrier, say the researchers, is regulatory obstacles that prevent nurses from prescribing antidepressants. This problem is made worse by the fact that South Africa has shortages of public sector psychiatrists and medical doctors.
“The study highlights the burden of depression in our country, the vast treatment gap, and stark inequities in access between the public and the private sectors despite on-paper availability of treatments we have known work to mitigate the effects of depression for decades,” the study’s principal investigator Professor Lara Fairall told Spotlight.
“There was a clear call to review regulatory barriers to wider access to antidepressants in the 2023 National Mental Health Policy Framework and Strategic Plan, but it has not been followed by definitive action,” she says.
“Unlocking these barriers requires clarity of mandate by multiple state and para-statal bodies including the National Department of Health, the South African Health Products Regulatory Authority and the South African Nursing Council, but the study is a reminder that failure to do so leaves millions of people vulnerable with desperate consequences for themselves, their families and the economy,” says Fairall who works as a health systems researcher at King’s College London and leads the Knowledge Translation Unit at UCT.
Republished from Spotlight under a Creative Commons licence.
Dr Jessica Hamuy Blanco, Product and Clinical Risk Executive at Dis-Chem
As the world marks World TB Day on 24 March under the theme “Yes! We can end TB!”, South Africa faces a clear challenge turning awareness into early action.
“TB is all around us,” says Dr Jessica Hamuy Blanco, Product and Clinical Risk Executive at Dis-Chem. “Many people don’t realise that exposure is common. The bacteria can lie dormant for years and only become active when the immune system is compromised.”
Despite widespread awareness, a critical gap remains between what people know about TB and how quickly they act on symptoms. This gap continues to shape outcomes for thousands living with this preventable and curable disease.
According to the World Health Organisation (WHO), approximately 249 000 people in South Africa developed tuberculosis in 2024.
TB remains close to home
Although preventable and curable, TB continues to spread quietly often because symptoms are ignored and treatment is delayed.
“People don’t always recognise the signs early enough or know where to seek help,” says Dr Hamuy Blanco. “This is where informed, trusted healthcare makes the difference.”
South Africa remains one of the countries hardest hit by TB globally. The disease is closely linked to HIV, with weakened immune systems increasing the risk of TB becoming active. At the same time, socio-economic realities such as overcrowding and limited access to healthcare continue to drive transmission.
Delayed diagnosis means individuals remain infectious for longer, placing families and communities at greater risk.
Early detection can change outcomes
Detecting TB early remains one of the most effective ways to reduce its spread and improve recovery. Treatment typically involves a six- to nine-month course of antibiotics, with strong success rates when completed. However early symptoms are often missed.
“The signs can be missed or ignored,” explains Dr Hamuy Blanco. “A persistent cough, fatigue, night sweats or weight loss are easy to dismiss as stress or a lingering illness. That delay gives TB time to spread.”
Creating space for early conversations, whether at a clinic, pharmacy or with a nurse can make the difference between early intervention and prolonged illness.
Finishing treatment is non-negotiable
Another major barrier to ending TB is interrupted treatment. Many patients begin to feel better within weeks and assume they are cured, while others struggle with side effects or the practicalities of repeated clinic visits.
“When treatment is stopped too soon, the bacteria are not fully eliminated,” says Dr Hamuy Blanco. “This is how drug-resistant TB develops, which is far more difficult and costly to treat.”
Supporting patients through the full course of treatment is essential, with clear communication and ongoing support improving adherence.
Bringing care closer to people
“Accessible healthcare is critical in closing the gap between awareness and action”, says Dr Hamuy Blanco. Retail health clinics and digital health platforms are increasingly helping to make care part of people’s everyday lives.
These routine touchpoints create opportunities for people to ask questions, seek advice and act early helping to normalise testing, reduce stigma and support patients throughout their treatment journey.
“Care needs to fit into people’s daily lives,” she adds. “It should be easy to access, easy to understand and supportive from start to finish.”
Turning intent into impact
TB is both preventable and curable, yet it continues to claim lives because of delayed action and incomplete treatment.
“Ending tuberculosis takes more than medicine. It requires a human-centred approach that supports people from early testing through to completed treatment. By breaking down stigma and acting sooner, South Africa can move from awareness to impact,” she concludes.
To significantly expand access to affordable, quality primary healthcare in underserved communities, the Cipla Foundation’s Sha’p Left initiative has partnered with the FirstRand Empowerment Foundation (FREF). The partnership aims to aggressively scale the cost-effective nurse-driven surgeries in local communities, across the Western Cape, KwaZulu-Natal and Gauteng.
HEALTHCARE CLOSER TO HOME
This collaboration will help to overcome systemic barriers to healthcare, particularly in terms of equitable access for low-income, uninsured individuals. For many people living in peri-urban and rural areas, access to quality primary healthcare services poses a significant challenge. Over-burdened State medical facilities are often congested, resulting in long waiting times for patients.
Sha’p Left is a patient-centred, cost-aware, nurse-driven primary healthcare service, in the heart of local communities. These nurse surgeries are located in easily accessible hubs such as busy taxi ranks to promote ease of access. The greatest benefit of Sha’p Left is that in addition to saving travel time, it helps to empower people both in terms of caring for their health, but also financially: the lack of queues mean that people don’t need to take a full day off work (resulting in a loss of income) to access basic healthcare.
Currently, Sha’p Left serves more than 5 000 patients monthly, with the patient profile comprising a 60% / 40% female / male split. The existing clinics are GMP compliant containerised solutions, as part of environmental sustainability initiatives and lowering overhead costs, solar solutions are being implemented at these clinics.
CHAMPIONING CHANGE
Strengthening community-based primary healthcare supports national health priorities by reducing the burden on State facilities, promotes preventative healthcare and creates an empowering, dignified experience for patients.
The investment by FREF will help Sha’p Left to deploy more nurse surgeries, and these solutions will ultimately help address inequality and reduce poverty as access to quality healthcare is basic human right. The partnership will scale Sha’p Left from 11 to 61 surgeries by the end of 2029.
SUSTAINABLE SOCIAL IMPACT
The business model involves enterprise development in conjunction with qualified, predominantly female clinical nurse practitioners (CNPs) and assists them to establish sustainable, owner-operated clinics in identified communities to provide affordable primary healthcare services.
This fee-for-service model, driven by the “entreprenurses”, provides a dignified and holistic patient experience. The surgeries have dispensing licenses and therefore a consultations includes the necessary medication required, up to Schedule 4 medicines.
The first three nurse surgeries being deployed in 2026, as part of this partnership, are in these areas:
· Senoane (Gauteng)
· KwaNyuswa (KZN)
· Verulam (KZN)
Blending social impact with sustainability creates a blueprint for scaling primary healthcare in South Africa. With FREF’s support, the Sha’p Left model will expand further into communities where access gaps remain widest, ensuring that more South Africans can easily receive the care they need. This investment ensures that good health is not merely a privilege for a select few people, but for all South Africans.
New TB tests have massive potential for South Africa’s struggle to get to grips with the age-old disease. Making the most of these new tests will require both ambition and smart implementation, argue Gaurang Tanna and Dr Yogan Pillay.
Every day, more than 140 people die from tuberculosis (TB) in South Africa, yet TB is both preventable and curable. Too many people are tested too late, allowing the disease to spread silently through communities and turning a curable illness into a fatal one.
Unlike most other diseases, anyone can contract TB – the bacteria are airborne and just the act of breathing makes us vulnerable to contracting TB. The risk of TB is higher for people with suppressed immunity, malnutrition, or living with cancer or HIV.
Reducing deaths from TB depends on earlier diagnosis, yet many people are diagnosed late, often after prolonged illness, and only once they reach hospitals with advanced disease. There are some opportunities for improvement. Firstly, we need to address persistent weaknesses in where and how TB tests are offered. Secondly, we need to address delays in care seeking, and missed opportunities for testing within health facilities. Finally, we need to close the operational barriers that impede testing. An added challenge that the TB disease presents is that it is often present without any symptoms.
In recent years, South Africa took important steps to strengthen its TB response and intensified efforts to find people with the TB disease through implementation of Targeted Universal TB Testing (TUTT). TUTT is a strategy that promotes systematic testing among high-TB risk groups, like people living with HIV, household contacts of individuals with TB, and people with previous TB, irrespective of symptoms.
South Africa now conducts approximately 3.6 million TB tests annually, representing a 50% increase compared to pre-COVID pandemic testing. However, we need to scale this up considerably if we are to reach the more than six million people living with HIV currently receiving HIV treatment in South Africa as well as all those with TB symptoms who are often missed at facilities.
Despite strong commitments, TB testing in South Africa continues to face several structural constraints.
First, the cost of molecular diagnostics limits the scale of testing. Current molecular TB tests cost approximately R230 per test.
Second, inefficient clinic workflows reduce testing coverage. In busy primary healthcare facilities, this leads to missed TB testing, contributing to prolonged diagnostic delays during which transmission continues and disease severity worsens.
Third, many patients, especially children and people living with HIV, can’t produce sputum, which current tests require, further reducing testing coverage.
Fourth, people with the highest burden of TB, particularly men, often do not attend government clinics. Men account for a disproportionate share of TB in South Africa but remain underrepresented in testing programmes, contributing to delayed diagnoses and ongoing transmission.
Evolving and strengthening testing capabilities in line with the ambitions of the next phase of TB control in South Africa requires leveraging emerging diagnostic tools and redesigning how TB testing is delivered.
New diagnostic tools create new opportunities
Just recently, the World Health Organization updated its recommendations on TB diagnostics, endorsing the use of near-point-of-care tests and use of tongue swabs for people who cannot produce sputum to expand access to TB diagnostics and improve diagnostic efficiency. These new tools provide an opportunity to rethink how testing is organised across the health system.
Tongue swabs offer a promising alternative sample type, enabling testing among patients who cannot produce sputum. It has also been demonstrated to be more acceptable for patients and providers and is easier to collect in clinics.
At the same time, near-point-of-care molecular platforms (such as Pluslife, a test that has been approved by the South Africa’s health products regulatory body) offer the potential to diagnose TB closer to the patient. It substantially reduces costs, to about one-third the cost of current molecular tests, while demonstrating comparable diagnostic performance for TB, making large-scale expansion of TB testing more accessible and affordable. By delivering results rapidly, within an hour, this technology could enable a test and treat approach. TB testing, diagnosis, and treatment initiation could all happen during a single primary healthcare visit. This would reduce the time to start treatment and limit the number of patients lost between diagnosis and treatment.
Clinic workflows need to be redesigned
Patients presenting with TB symptoms often move through multiple stages of the clinic process – registration, triage, waiting areas, and clinician consultations – before TB testing is considered. Improving TB testing requires services redesign for patient convenience and accessibility, and to be much more systematic. A few simple changes could be introduced.
Firstly, introduce a fast-track TB queue, allowing individuals to register digitally and drop off samples without completing a full clinic visit.
Secondly, embed TB symptom screening and sample collection at triage or vital-sign stations. Any patient reporting TB symptoms – cough, fever, night sweats, or weight loss – should have a sample collected while waiting to see a clinician.
Thirdly, for people living with HIV, introduce twin TB testing with annual viral load test (or CD4 for newly diagnosed patients) to systematically test all people living with HIV.
Lastly, we could equip facilities with a near-point-of-care testing platform, like Pluslife, to deliver results before the clinical consultation, allowing TB to be diagnosed rapidly and at lower cost to the health system. It would enable patients to start treatment on the same day.
These approaches could directly address the most persistent diagnostic and linkage gaps in South Africa’s TB programme.
Extending TB testing beyond clinics
New diagnostic platforms also enable TB testing to move beyond government clinics.
A substantial proportion of individuals with TB, particularly men, do not present to clinics and delay seeking care. Near-point-of-care molecular platforms could enable TB testing through alternative delivery channels, including community settings (such as taxi ranks), community pharmacies, workplace clinics, and households through community health worker programmes.
Expanding testing beyond clinics will help identify TB earlier among populations that remain underserved by current services.
From policy ambition to implementation
South Africa’s progress over the past four years demonstrates that intensified testing strategies such as TUTT can help increase TB diagnosis. Sustaining this momentum will require redesigning primary health care services to fully use these emerging diagnostic tools. Three priorities should guide this transition.
First, TB sample collection workflows in clinics should be redesigned to ensure that every symptomatic and at-risk person is tested for TB.
Second, new diagnostic tools should be deployed, including the use of tongue swabs for people who cannot produce sputum, as well as low cost near-point-of-care molecular tests to simplify testing and treatment initiation pathways.
Third, TB testing should be expanded through alternative delivery channels to reach people who do not routinely access government clinic services, especially men, who are less likely to seek care in these settings.
By aligning ambition and new technologies with service redesign, South Africa can significantly reduce diagnostic delays, decrease deaths due to TB and accelerate progress towards TB elimination.
*Tanna is a senior programme officer for TB, and Dr Pillay is the director of HIV and TB delivery at the Gates Foundation.
Disclosure: Spotlight receives funding from the Gates Foundation but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council.
Note: Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.
With their innovation of a small but powerful handheld device, researchers at the University of Pretoria (UP) are on course to redefine the tuberculosis (TB) screening process, which could ultimately help to combat the TB pandemic more effectively. TB is one of the deadliest infectious diseases worldwide, claiming more than 1.25 million lives each year, of which about 50 000 deaths occur in South Africa. It is the leading cause of death among people with HIV.
MARTI (mycolate antibody real-time immunoassay) is the name of the handheld device that can provide very high certainty that a person at risk does not have TB. Using just one drop of blood – and no laboratory – it is set to change the way TB is detected. It may even be adapted for use in both human and veterinary healthcare. The diagnostic is fast, accurate, affordable and – the intellectual part of it – proudly South African.
An internal validation trial was recently completed to confirm the accuracy of the test. These trial results show remarkable promise in terms of the specificity, sensitivity and accuracy of the diagnostic test, coming close to the range of targets set by the World Health Organization for the “perfect” test, making MARTI an ideal screening and diagnostic tool. An earlier trial demonstrated great potential in using this test to monitor TB treatment; these results were published in the journal Biomarkers in Medicine.
“Many people aren’t aware that TB doesn’t always sit in the lungs – it can be present in bones, joints and the brain,” says Professor Jan Verschoor, former research leader of UP’s Tuberculosis Research Group in the Department of Biochemistry, Genetics and Microbiology and now an emeritus professor of biochemistry who has been leading this discovery. “The ‘gold standard’ TB test that involves growing cultures from lung sputum can take about six weeks, by which time, many more people could have been infected by the patient or the patient’s health could have deteriorated beyond the prospect of cure. From a simple finger-prick blood sample, the MARTI test gives us a result in 30 minutes. This has profound cost and public health implications in a country like South Africa, where we conduct three to five million TB tests a year.
Tuberculosis bacteria. Credit: CDC
Caused by Mycobacterium tuberculosis, this resilient bacterium has long evaded simple detection methods, particularly in regions where healthcare infrastructure is limited. But now, an unexpected hero has emerged in the war on TB: a molecule in the bacterium’s waxy coat – specifically its mycolic acid (MA) – holds the key. These wax-like substances form a nearly impenetrable barrier, making the bacterium both drug-resistant and difficult to detect.
But while other scientists focused on breaking through this barrier, Prof Verschoor took a different approach: what if the wax itself could be used to detect the disease? He was the first to demonstrate that antibodies to the waxes are reliable indicators of active TB, irrespective of whether someone had been vaccinated or was coinfected with HIV.
A key aspect of the innovation came from Carl Baumeister, a PhD candidate under Prof Verschoor. He made the leap from slow laboratory-based biosensing to a handheld device that detects anti-MA antibodies accurately and affordably in less than 30 minutes. The result is a test that’s as clever as it is simple and cost-effective.
Detecting these anti-MA antibodies requires sophisticated sensing technology: the surface of a screen-printed carbon electrode is pre-coated with a thin layer of MA. MARTI works by flowing a drop of blood over this electrode. If a patient has TB, the sensor detects these antibodies in the blood sample; if a patient does not have TB, no signal would be generated since there are no anti-MA antibodies in the blood sample.
“The device fits in the palm of your hand and requires only a single drop of blood – no sputum, no needles, no laboratory,” says Carl Baumeister, Head of Operations of the UP spin-off company MARTI TB Diagnostics. “This may become a game-changer to diagnose TB in paediatric and HIV-positive patients, where obtaining sputum samples is often neither feasible nor safe. The same could apply to the 20% of all extra-pulmonary cases.”
“If MARTI says you don’t have TB, you can trust it,” Baumeister says. “That’s a critical trait when trying to rule out cases during an outbreak or in mass screening campaigns, much like what was needed during the COVID-19 pandemic.
Unlike other TB diagnostics, MARTI offers something rare and powerful: near-perfect negative predictive value in typical screening applications.
The internal validation trial across six healthcare facilities in Tshwane was led by Prof Veronica Ueckermann, Head of Infectious Diseases at Steve Biko Academic Hospital and UP’s Faculty of Health Sciences.
“Collecting, transporting, processing and analysing the samples from the various sites within the temperature and time constraints of the validation trial protocol posed a significant logistical challenge – but we succeeded,” says Mosa Molatseli, a senior research scientist who heads up the MARTI laboratory.
Recognising its potential, UP established the start-up company MARTI TB Diagnostics (Pty) Ltd to develop and eventually commercialise MARTI.
“This is designed to ensure that the technology remains in South African hands while attracting investment and serving global needs,” says Gerrie Mostert, interim CEO of the company. “The next steps are to get investors, funding and partner organisations on board, obtain regulatory approval and start manufacturing the kit. Ultimately, MARTI should be rolled out to clinics worldwide.”