A new national cohort study from Latvia, conducted in collaboration with researchers from the clinical tuberculosis infrastructure (ClinTB) at the German Center for Infection Research (DZIF) at the Research Center Borstel, Leibniz Lung Center (FZB), provides important insights into the treatment of multidrug-resistant tuberculosis (MDR-TB). The study shows that long-term disease-free survival rates are significantly higher than previous standard indicators suggest. The results, published in the renowned journal The Lancet Regional Health Europe, are based on the analysis of data from 1299 adult patients treated between 2005 and 2021.
Multidrug-resistant tuberculosis poses a significant challenge to healthcare systems worldwide. Whilst the effectiveness of treatment is traditionally assessed on the basis of treatment outcomes at the end of therapy, the new study shows that these criteria underestimate the actual long-term success of treatment. According to WHO standard definitions, only 4.8% of patients in Latvia were considered cured. However, during long-term follow-up, 76.9% of those affected remained permanently relapse-free.
The researchers linked clinical data with national registry information for long-term follow-up, enabling them, for the first time, to systematically evaluate long-term treatment outcomes in a former European country with a high incidence of MDR-TB. A key factor in treatment success was the use of at least three effective drugs in the individual treatment regimen.
Furthermore, the analysis showed that very short treatment durations of less than nine months, using the treatment options available at the time, were associated with an increased risk of relapse or death. Treatment durations of between ten and seventeen months, however, achieved comparable results to longer courses of treatment. After the end of the observation period, MDR-TB treatments became more effective. Today, the treatment duration for MDR-TB has aligned with the six months required for drug-sensitive tuberculosis.
“The study underscores the importance of long-term follow-up in MDR-TB and suggests that tuberculosis control programmes should broaden their measures of success. Including recurrence-free survival rates allows for a more realistic assessment of the quality of care and the actual benefit to patients,” says Sophie Meier, a medical PhD student at the FZB and the University of Lübeck under DZIF researcher Professor Christoph Lange.
“The findings also support the role of expert panels, known as consilia, in selecting treatments and assessing treatment success for MDR-TB. In Latvia, the decisions made by the consilium were significantly superior to the results obtained by applying WHO definitions for MDR-TB treatment outcomes. Consilia are also an element of effective ‘antimicrobial stewardship’ against the development of new antibiotic resistance,” says PD Dr Thomas Brehm from the FZB and University Medical Center Hamburg-Eppendorf (UKE), DZIF researcher and senior author of this study.
The findings of this study provide important impetus for future treatment strategies for MDR-TB and support the use of individualised treatment regimens with sufficiently effective drugs. Prospective studies are now required to test these findings in the context of new, shortened treatment regimens using modern active substances. If necessary, the definitions of treatment outcomes for MDR-TB will need to be revised.
This African Vaccination WeekSanofi South Africareaffirms its commitment to vaccine awareness, access and public health partnerships to close the immunisation gap
Photo by Mufid Majnun on Unsplash
Johannesburg, 20 April 2026 – Marked each year from 24 to 30 April, African Vaccination Week focuses on the need for equitable access to lifesaving vaccines across the continent.
It’s also a timely reminder that while vaccination remains one of the most effective tools in public health, gaps in coverage are a real concern, in South Africa and globally. UNICEF says immunisation prevents an estimated 4.4 million deaths every year,1 yet WHO reported that 14.3 million children worldwide missed out on all routine vaccines in 2024.2 Global coverage for the third dose of DTP-containing vaccine stood at 85% in 2024, while first-dose measles coverage was 84%.2
“Vaccination remains one of the smartest and most effective investments in public health,” says Jean-Baptiste Bregeon, Country Lead and Head of Vaccines, Sanofi South Africa. “Improving coverage is not only about having vaccines available. It’s about building trust, strengthening health systems, supporting healthcare workers and making sure people have the information they need to act. African Vaccination Week is a reminder that protecting lives takes sustained effort and strong partnerships, and Sanofi remains committed to playing its part in South Africa.”
In South Africa, the need is clear. The National Department of Health reported in 2024 that 80% of children in the country had received all their vaccinations by the age of one.3 That is progress, but it also means one in five children had missed one or more doses and was not fully protected. UNICEF South Africa has separately highlighted the urgency of reaching children who have missed routine immunisation entirely. There were 58,000 more zero dose children in 2024 and 278,000 without vaccination, leaving them vulnerable to vaccine preventable diseases.4 Measles vaccination coverage, for example, declined from 80% in 2023 to 76% in 2024.4
Recurring outbreaks of measles, cholera, polio and diphtheria have added pressure to the health system, while disruption to routine immunisation has left more children vulnerable to vaccine-preventable diseases and increased the risk of further outbreaks.5
This year’s campaign aims to intensify vaccination and surveillance activities in districts with high numbers of under-vaccinated and unvaccinated children. Vaccines included in South Africa’s national immunisation schedule are available free of charge at primary healthcare facilities.
Sanofi says its focus in South Africa over the next two to three years will be to continue supporting the Department of Health to improve vaccine coverage across the country, with a focus on access, availability, education and awareness.
“Improving vaccine uptake requires a practical, local approach that recognises the realities of South Africa’s healthcare system, including uneven coverage, pressure on frontline services, and the challenge of reaching communities across both urban and rural settings,” says Bregeon.
That’s why partnership matters, he adds. “Improving immunisation outcomes takes coordinated action across government, healthcare providers, communities and industry. Strong supply is important, but so is public confidence, clear communication and consistent follow-through at clinic level.”
This African Vaccination Week, Sanofi calls on all South Africans to ensure their vaccinations are up to date and encourages healthcare providers to continue championing immunisation as a cornerstone of preventive health.”
Most children with a severely broken wrist can be treated without surgery, according to a major NIHR-funded UK trial led by researchers at the University of Oxford. The findings suggest that a non-surgical, cast-first approach delivers similar long-term recovery while reducing the risks associated with surgery and costs.
Broken wrists are among the most common injuries in children accounting for about half of children’s fractures. Severely displaced distal radial fractures, where the bones move out of place, are often routinely treated with surgery. However – unlike adults – children have a remarkable ability to straighten broken bones, in a process called remodelling.
Researchers questioned whether a plaster cast would achieve the same long-term result without exposing children to the risks of an operation.
Professor Matt Costa, senior author and Professor, Orthopaedics Trauma Surgery at the Kadoorie Institute, University of Oxford said: ‘These fractures can look very severe on an X-ray, which has traditionally led to surgery to straighten the bone. But because children’s bones are still growing, they have a remarkable capacity to heal. Until now, there has been limited high-quality evidence on whether surgery was always necessary.’
The CRAFFT trial (Children’s Radius Acute Fracture Fixation Trial) was funded by the National Institute for Health and Care Research (NIHR) and supported by the NIHR Biomedical Research Centre: Oxford. It recruited 750 children aged 4–10 from 49 hospitals across the UK. Participants were randomly assigned to receive either surgical fixation or treatment with a plaster cast.
Patients were measured at regular intervals against a set of criteria. At three months, children who had surgery reported slightly better arm function, but the difference between groups was very small. By six and 12 months, there was no difference in recovery, suggesting that early advantages with surgery do not persist.
There were complications following surgery, including infections, scarring and nerve irritation. Non-surgical treatment, which avoids anaesthesia and operative intervention, was shown to reduce NHS costs by around £1,600 per patient on average.
The trial was designed with input from families, who helped define what level of improvement would be meaningful enough to warrant surgery. The observed difference between treatments fell below this threshold.
Professor Dan Perry, NIHR Research Professor and Children’s Orthopaedic Surgeon at Alder Hey Children’s Hospital and the University of Liverpool, and lead author, said: ‘It is astonishing that children have the ability to grow bent, broken bones straight again. It really is a superpower that is unique to children. From both a clinical and health system perspective, these findings are important. Adoption of these results could reduce the number of children exposed to the risks of anaesthesia and surgery, and ease pressure on healthcare services without compromising recovery.’
The results, published in The Lancet, support wider adoption of a cast-first approach for most children with these injuries.
Graphical abstract by Montesdeoca et al., JACS 2026.
Most tumours grow so rapidly that vascular growth cannot keep up, and oxygen-depleted areas form within them. A new active agent could make it possible to treat them with photodynamic therapy.
Photodynamic treatment of cancer is based on administering an initially inactive substance that is only activated in the tumour via targeted light irradiation. It then generates reactive oxygen species that kill the cancer cells. However, this method reaches its limits when no oxygen is present, as is the case with many fast-growing tumours. Professor Johannes Karges’ research group at Ruhr University Bochum has achieved a breakthrough that makes the treatment of such tumours possible: When oxygen is absent, an alternative action mechanism comes into effect. This uses hydrogen peroxide, a natural metabolic product of the cells. The researchers report their findings in the Journal of the American Chemical Society from April 6, 2026.
An entirely new action mechanism
Photodynamic therapy, or PDT, is an established method for treating cancer and is widely used in clinical practice. Karges and his team have developed an entirely new action mechanism that functions independently of the oxygen concentration within the tissue: Light converts the ruthenium-based active agent into an excited electronic state. When oxygen is present, energy is transferred to molecular oxygen, creating singlet oxygen, which has a harmful effect on cells. “This process corresponds to the conventional, oxygen-dependent mechanism of photodynamic therapy,” says Karges.
When oxygen is absent, another mechanism comes into effect. The cause is the coordination of intracellular iron to the active agent. This interaction alters the electronic characteristics of the system such that instead of a transfer of energy, an ultra-fast, metal-to-metal transfer of electrons occurs from the excited ruthenium centre to the iron centre. The hydrogen peroxide is thereby converted into highly reactive hydroxyl radicals. “Because hydrogen peroxide is a natural metabolic product of the cell, this process can occur independently of the molecular oxygen,” explains Karges. The hydroxyl radicals that have formed cause oxidative damage to central cellular structures and thus kill the cancer cells.
This means that the substance remains active even under severe conditions where past therapies have failed. In the current study, the researchers demonstrated this with breast cancer cells. “This method can be used for many different types of tumours, in principle,” says Karges. “However, we have not yet begun trying this out with human subjects and are working to develop this.”
A study conducted at the University of São Paulo shows that the pathogen can persist in these tissues for long periods, be transmitted unexpectedly, and trigger new outbreaks of the disease.
The rhinovirus can infect B lymphocytes, which produce antibodies, and CD4 T cells, which conduct the local immune response (image: PDB/Wikimedia Commons)
By Karina Toledo | Agência FAPESP – A study conducted at the University of São Paulo (USP) in Brazil reveals that tissues such as the tonsils and adenoids can serve as hiding places for the rhinovirus, which causes the common cold and is responsible for most respiratory infections worldwide.
Using samples from 293 children who underwent surgery to remove these tissues, the study showed that the pathogen can infect immune cells known as lymphocytes and remain there for long periods without causing symptoms. This allows the virus to potentially be transmitted to others without warning.
“The virus has a ‘date’ with the child population. Every year, about two or three weeks after school starts in temperate regions, there’s a rhinovirus outbreak. And children pass it on to their parents and grandparents. We’ve always wondered: What does the start of school have to do with it? Well, children gather in closed spaces, and some of them with the virus in their throats can spark an outbreak at school, even if they’re asymptomatic,” comments rhinovirologist Eurico de Arruda Neto, a professor at the Ribeirão Preto School of Medicine (FMRP-USP) and coordinator of the research, supported by FAPESP (projects 13/06380‐0, 13/16349‐2 and 17/25654‐4).
As the researcher explains, it was already known that the rhinovirus infects the epithelium (the outermost layer of the mucosa) of the nose and throat, hijacks the cellular machinery to multiply, and causes the host cell to rupture once this process is complete, releasing progeny capable of generating new infections. For this reason, scientists consider it a lytic virus, one that causes cell lysis, or rupture. This rapid and destructive cycle quickly draws the attention of the immune system, which, in most cases, eliminates the virus from the body within about five to seven days.
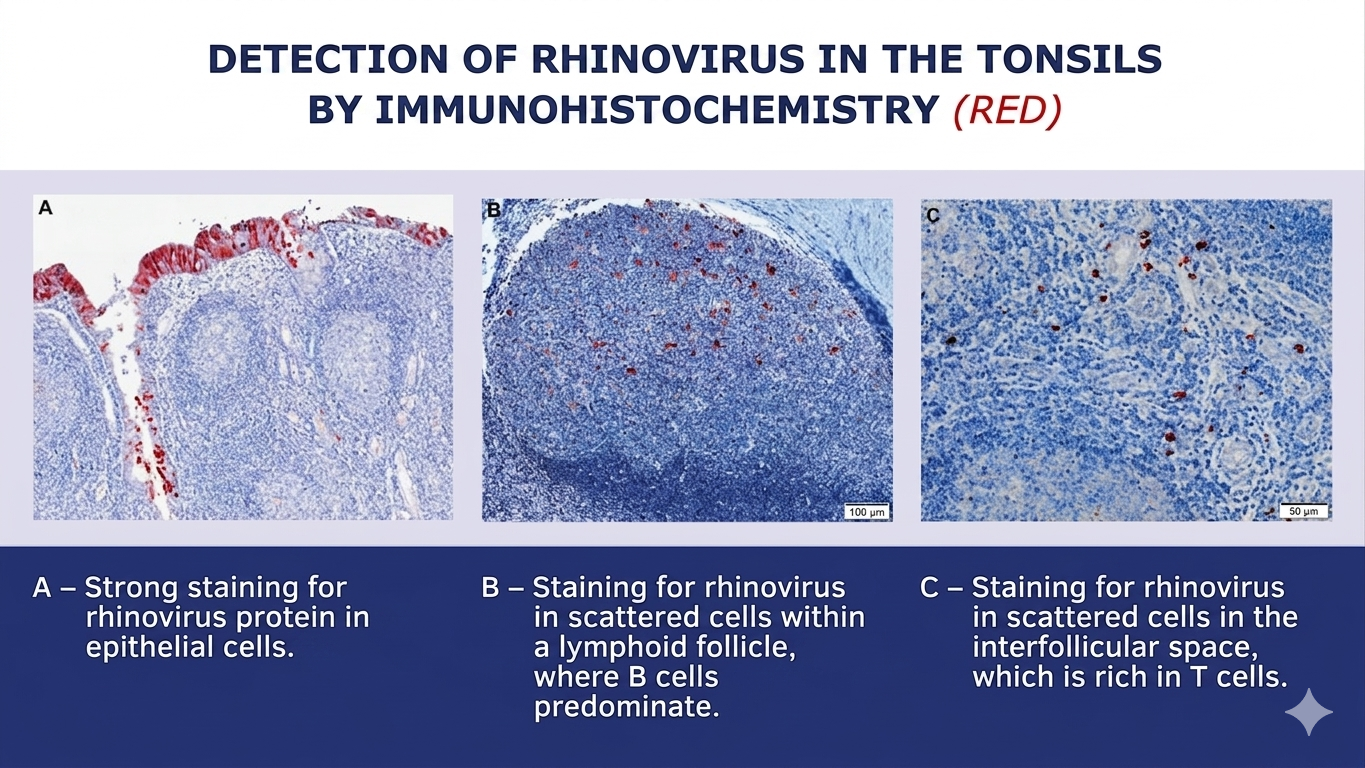
The major finding of the study was that the rhinovirus can reach the deeper layers of tonsil and adenoid tissues in addition to the epithelium. There, it can infect B lymphocytes, which produce antibodies, and CD4 T lymphocytes, which conduct the local immune response. These cells have a long lifespan and store the “memory” of the immune system. Rather than killing them, the rhinovirus remains inside these cells for extended periods, in a state of persistence similar to that seen with herpes viruses, HPV, and cytomegalovirus.
“The samples we analyzed are from children who underwent surgery due to snoring, sleep apnea, or recurrent infections related to tonsillar and adenoid hypertrophy. At the time of surgery, they were necessarily asymptomatic. Nevertheless, we detected the rhinovirus in a large number of participants,” says Arruda.
In addition to the tonsils and adenoids, the children’s nasal secretions were analyzed as well. According to data published in the Journal of Medical Virology, the virus was present in at least one of the three sites (tonsil, adenoid, or secretion) in 46% of the volunteers. Viral proteins and other signs that the rhinovirus was replicating – and therefore capable of infecting another person – were also observed in these tissues.
The research was conducted in collaboration with Ronaldo Martins, a virologist from the Ribeirão Preto School of Pharmaceutical Sciences (FCFRP-USP), as well as professors Wilma Anselmo-Lima, Edwin Tamashiro, and Fabiana Valera from the FMRP-USP.
(image: press release)
Virus garden
In previous studies, Arruda’s team detected adenovirus (another cause of the common cold), influenza A (flu), and SARS-CoV-2 (COVID-19) in samples of tonsils and adenoids from children who had undergone surgery. The latter two are known to cause longer-lasting infections in some patients. In the case of the rhinovirus, however, this came as a surprise.
“I get the impression that no matter what common virus we look for, we’ll find it. And not just in the tonsils and adenoids, but in other lymphoid tissues throughout the body, such as lymph nodes. We already have some preliminary evidence that lymphoid tissues are a sort of ‘garden’ for viruses. And our hypothesis is that this is a good thing. It acts as a booster for immune memory, meaning antibodies continue to be produced even long after initial exposure,” says Arruda.
However, in the case of people with asthma, this can be problematic. One hypothesis raised by the authors of the article is that infectious viruses in tonsil CD4 T lymphocytes may release inflammatory substances that act on the lungs and cause asthma attacks. It is already known that colds and the flu are among the most common causes of asthma attacks, especially in young children.
Additionally, a previous study by the group detected respiratory viruses in normal adenoids (without hypertrophy), which are located next to the Eustachian tube. This may explain why some children suffer from recurrent otitis media.
“This virus can pass from the adenoids to the middle ear and cause inflammation there. The child won’t sneeze or cough, but the ear will become inflamed, closing the narrow Eustachian tube and leading to a buildup of fluid in which the local bacterial flora begins to proliferate,” the researcher explains.
Clinical implications
Based on these findings, Arruda believes that pediatricians should be mindful of the possibility of diagnostic confusion regarding the causes of childhood illnesses.
“For example, a child with hypertrophic tonsils arrives at the emergency room with a respiratory infection and bronchiolitis symptoms caused by respiratory syncytial virus, but the throat swab test detects rhinovirus from a previous infection. In other words, tests performed on secretions may not always reflect what’s actually happening in the lungs,” says the researcher. “We have evidence that this viral persistence can also occur in people with normal-sized tonsils and adenoids.”
Another hypothesis to be investigated, Arruda says, is whether viruses that persist in lymphoid tissues can cause problems for immunosuppressed patients. “Patients who undergo bone marrow transplants, for example, frequently develop lung infections and bronchiolitis. Doctors, nurses, and medical students are usually blamed for bringing the virus into the high-risk ward. But could it be that the virus was already present in the patient’s tonsils or adenoids and has now been reactivated due to low immunity? It doesn’t have to be transmission from outside to inside. That’s what we’ve started to investigate in mice,” he explains.




{kind=link}