GLP-1 medications used to treat diabetes and obesity were associated with a reduced need for hospital care and sickness absence due to psychiatric reasons, a new study shows. The large register-based study was carried out in collaboration between the University of Eastern Finland, Karolinska Institutet in Stockholm and Griffith University in Australia.
Diabetes and obesity are associated with an increased risk of mental health symptoms, and similarly, individuals with mental disorders have an elevated risk of metabolic diseases such as obesity and diabetes. Researchers have long been interested in the connections between these conditions and in how pharmacological treatments may affect both metabolic and mental health disorders.
The present study, published in The Lancet Pyschiatry, included nearly 100 000 participants, over 20 000 of whom had used GLP-1 medications. Participants were followed through Swedish national registers between 2009 and 2022.
The risk of substance use was also reduced
The results showed that the use of GLP-1 medications – particularly semaglutide – was associated with a reduction in sickness absence and hospital care due to psychiatric reasons. During periods of semaglutide use, the reduction was 42% compared with periods when GLP-1 medications were not used. For depression, the risk was 44% lower, and for anxiety disorders, 38% lower.
In addition, semaglutide use was associated with a lower risk of substance use disorders: hospital care and sickness absence related to substance use were 47% lower during periods of semaglutide use compared with periods without GLP-1 medication. The use of GLP-1 receptor agonists was also associated with a reduced risk of suicidal behaviour.
One of the study’s authors, Professor Mark Taylor from Griffith University, says such results were to be expected: “An earlier study examining Swedish registers found the use of GLP-1 medications to be associated with a reduced risk of alcohol use disorder. Alcohol-related problems often have downstream effects on mood and anxiety, so we expected the effect to be positive on these as well.”
However, the magnitude of the association surprised the researchers: “Because this is a registry-based study, we cannot determine exactly why or how these medications affect mood symptoms, but the association was quite strong. It is possible that, in addition to factors such as reduced alcohol consumption, weight loss-related improvements in body image, or relief associated with better glycaemic control in diabetes, there may also be direct neurobiological mechanisms involved – for example, through changes in the functioning of the brain’s reward system,” says Research Director, Docent Markku Lähteenvuo from the University of Eastern Finland.
Other recent evidence on the effects of GLP-1 medications on anxiety and depressive disorders has been somewhat inconsistent, but it has been largely based on small studies.
A new type of daily pill has proven more effective for weight loss and blood sugar control than its currently available counterparts, according to a recent trial. The drug, known as orforglipron, could be a game-changer in the rapidly expanding oral weight-loss drug market.
The advent of the injectable weight-loss drug semaglutide (known better by its brand names Wegovy and Ozempic) marked a distinct shift in the weight-loss drugs market when it became available just a few years ago.
Semaglutide is a class of glucagon-like peptide-1 (GLP-1) medication. These drugs mimic the gut hormone GLP-1, which is released soon after eating. This hormone signals fullness to the brain, slowing digestion and stimulating the release of insulin. By replicating the action of this hormone, GLP-1 drugs have proven highly effective at managing type 2 diabetes and promoting weight loss.
Although semaglutide is widely used, a key issue with the drug is that it needs to be injected into the belly, thighs or back of the arm. This can make it difficult for patients with needle phobia or who don’t want to self-inject due to the inconvenience.
Another logistical issue with injectable GLP-1 drugs is that they require refrigeration throughout the supply chain. This can pose a challenge in low- and middle-income countries.
It’s for these reasons that researchers and developers have started investigating the efficacy of oral versions of semaglutide.
Based on current research, it appears that oral semaglutide is very effective. However, it must be taken on an empty stomach – and users must wait 30 minutes before eating or drinking.
Alongside being expensive to produce, it also has poor bioavailability compared with injectable semaglutide. This means only about 1% of the ingested drug is absorbed and able to exert its effects.
But a recent phase 3 clinical trial has shown that a new type of oral weight-loss pill may have overcome these issues – proving to be more effective than the current oral semaglutide products on the market.
Oral weight-loss pill
The recent 52-week phase 3 trial involved 1,698 adults with type 2 diabetes across six countries. It set out to compare current oral semaglutide products against orforglipron, which is also taken as a daily tablet.
The primary measure researchers were looking for was a reduction in HbA1c. This blood test reflecting average blood sugar levels over three months is the standard indicator of diabetes control. Diabetes is present if HbA1c is 6.5% or more.
From a baseline average HbA1c of 8.3%, it was found that after 52 weeks, orforglipron was able to reduce this value by an average of 1.71–1.91%. In comparison, oral semaglutide only reduced HbA1c by 1.47%.
Not only did orforglipron meet the trial’s goals of proving it was as effective to oral semaglutide, it proved it was superior for lowering blood sugar. The participants who took orforglipron also lost more weight – an average of 6.1kg-8.2kg, compared with 5.3kg in those taking semaglutide.
However, a key issue highlighted by the trial was one of tolerability.
GLP-1 drugs can cause gastrointestinal side-effects such as nausea, vomiting, diarrhoea and constipation. In this latest trial, around 59% of participants on orforglipron reported such symptoms, compared with 37–45% on semaglutide.
The reason for this difference may be the more prominent, daily peak drug concentrations with orforglipron. The consequence was that around 10% of orforglipron participants discontinued treatment due to adverse effects. Just 4-5% of those taking semaglutide discontinued treatment.
Future studies may want to look at how orforglipron compares with injectable semaglutide. Photo by Haberdoedas on Unsplash
The trial’s results show that orforglipron, which was developed by Eli Lilly, can be considered one of semaglutide’s most credible challengers.
Another remarkable thing about orforglipron is that it belongs to a new category of drugs called small-molecule drugs. This means it’s a synthetic chemical compound small enough to be absorbed directly through the gut wall. There, it’s able to act on GLP-1 receptors, even though it isn’t of a similar structure to a GLP-1 hormone.
Oral semaglutide, on the other hand, is a peptide drug. This means the structure of its amino acids (one of the building blocks of protein) closely resembles that of the natural GLP-1 hormone.
As a small-molecule drug, orforglipron is cheaper and simpler to manufacture than peptide-based drugs such as semaglutide.
And as with oral semaglutide, it requires no refrigeration. This gives it a logistical advantage over injectable GLP-1 formulations – a potentially important consideration for expanding access in low- and middle-income countries, where cold chain infrastructure is unreliable.
It remains to be seen, however, how orforglipron will perform against oral semaglutide in the broader market.
Although this latest trial has shown it is superior for controlling blood sugar and aiding weight loss, its higher rate of side-effects and treatment discontinuation may temper enthusiasm. In a crowded and competitive market, long-term adherence – shaped as much by tolerability as by efficacy – is probably a critical differentiator.
Orforglipron is still undergoing trials in patients with obesity but without diabetes.
Salk Institute researchers find protein that connects GLP-1 agonist drugs to long-term, broad genomic responses that can promote pancreatic health and resilience
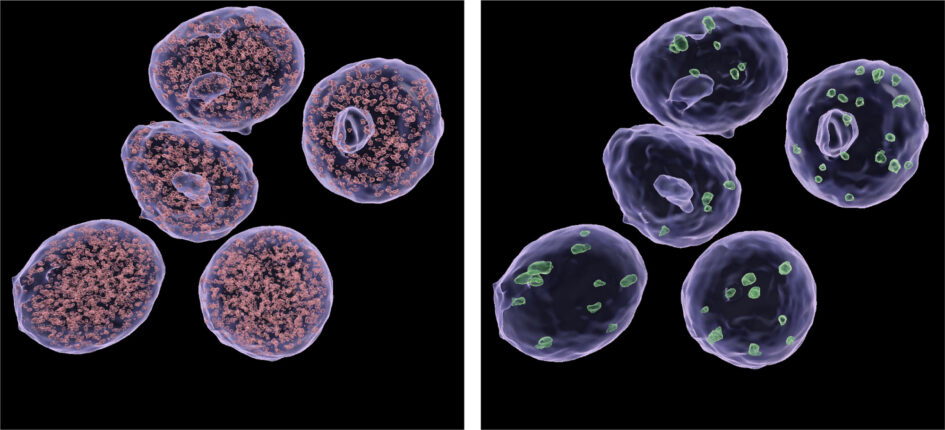
Small (left) and large (right) condensates of the Mediator complex inside nuclei of a pancreatic beta cell-derived cell line. Salk researchers discovered that GLP-1s interact with the multi-protein complex called Mediator to cause a broad genomic response. Click here for a high-resolution image. Credit: Salk Institute
GLP-1s are building a reputation as “wonder drugs.” First characterised for their ability to improve insulin release and treat diabetes, the drugs were later found to promote weight loss and improve cardiovascular health. In addition to these surprising bonus benefits is the ability of GLP-1 drugs to improve pancreatic beta cell health. But how, exactly, are they doing that?
Salk Institute researchers are burrowing down into the mechanistic details behind how GLP-1 drugs promote viability and stress resistance in pancreatic beta cells. Since cellular performance adaptations arise from gene expression changes, the team screened for regulatory proteins that can flip “on” advantageous gene programs during prolonged GLP-1 use. They identified a protein called Med14, part of a larger protein complex called Mediator, that was enabling the GLP-1-dependent changes in gene expression that lead to pancreatic health benefits.
The study was published in Proceedings of the National Academy of Sciences on March 4, 2026, and was funded by federal research grants from the National Institutes of Health and private philanthropy.
“The broad salutary effects of GLP-1 drugs in diabetes, cardiovascular disease, and obesity have sparked a wave of exciting scientific research at the mechanistic level. We’re left wondering, ‘How are GLP-1s causing these effects?’” asks senior author Marc Montminy, MD, PhD, a biochemist, physiologist, and distinguished professor emeritus at Salk. “We were able to single out a protein, Med14, whose activation downstream of GLP-1 helps reprogram pancreatic beta cell gene expression to improve the cells’ viability and insulin production.”
What are GLP-1 drugs?
Often simply called “GLP-1 drugs” or “GLPs,” glucagon-like peptide-1 receptoragonists work by mimicking a hormone our bodies naturally make. The hormone, called glucagon-like peptide-1, helps regulate blood sugar.by promoting the secretion of insulin. They do so by attaching to corresponding GLP-1 receptors on pancreatic beta cells, which then produce and release insulin into the body.
But GLP-1 drugs differ in one significant way from their natural counterpart: Unlike human-made GLP-1 hormones that appear and disappear quickly around mealtimes, artificial GLP-1 receptor agonists can stick around much longer. The Salk researchers suspect this longer-term presence may explain some of the “wonder drug” benefits of GLP-1 drugs. But what, exactly, on the molecular level, are GLP-1 drugs doing when they stick around? And how does their staying power turn into effects like lower risk of stroke or improved osteoarthritis?
“The fact that these drugs based off our hormones are stable seems to be important to the longer-term effects we’re witnessing in pancreatic beta cells and other tissues,” says first author Sam Van de Velde, PhD, a staff scientist in Montminy’s lab. “To understand how we are getting these longer-term effects, we need to study these drugs on a longer time scale – and that’s exactly what we did.”
How do GLP-1 drugs influence pancreatic health?
When the hormone GLP-1 finds a pancreatic beta cell, the ensuing chain of signals, proteins, and gene expression changes that lead to insulin secretion is very well documented. On the other hand, the mechanisms and changes on the longer-term GLP-1 drug scale are poorly understood.
So, the researchers set out on a molecular fishing expedition in a pancreatic beta cell line. The team was hoping to hook a protein (or proteins) that, post-GLP-1 activation, had a particular chemical modification called phosphorylation. And that’s exactly what they found in Med14.
Med14 is a subunit in a multi-protein complex called Mediator, which is a well-described general regulator of gene expression throughout the genome. To confirm whether Med14 was an integral link between GLP-1 drugs and ultimate changes in gene expression and pancreatic beta cell behavior, the researchers decided to mutate Med14, making the protein resistant to phosphorylation.
The gene expression patterns associated with prolonged GLP-1 drug exposure disappeared in a Med14 mutant pancreatic beta cell line and in beta cells of a Med14 mutant mouse model. With working Med14, the helpful gene programs were activated – supercharging pancreatic beta cells to grow and better handle sugar-rich environments after meals.
How else might GLP-1 drugs affect the body?
None of the Salk team’s experiments were conducted in humans, yet the relevance remains. For example, some of the genes regulated by Med14 phosphorylation are known to be linked to type 2 diabetes susceptibility in humans.
“Our findings unexpectedly reveal that phosphorylation of just a small part of the Med14 protein plays a significant role in the response to GLP-1 drugs – and in the metabolic response to hormones more broadly,” says Reuben Shaw, PhD, a professor and holder of the William R. Brody Chair at Salk, and director of the National Cancer Institute-Designated Salk Cancer Center. “Now there are many new questions to answer, from validating our findings in human tissues to seeing whether Med14 has a similar role in other cells and organs.”
The team is especially curious about the effects of prolonged GLP-1 exposure beyond pancreatic beta cells. One of the messenger molecules between GLP-1 and Med14, called cAMP, is a commonly used messenger molecule in many other situations that don’t include GLP-1. With that in mind, could other drugs or hormones activate genetic programs similar to GLP-1? And what’s going on in other metabolically intensive tissues, like fat?
The questions keep coming for the so-called “wonder drug,” and Salk scientists are enthusiastically working to answer them.
For GPs, solutions for treating osteoarthritis are frustratingly limited – it’s like the weather, everyone talks about it but nobody does anything about it. While standard care can relieve symptoms, there is currently no way to regenerate the actual lost cartilage in the joints. Some experimental treatments have proven successful in animal models and in petri dishes, but those are still many years away from being approved and available on the market.
But what if there was a currently available drug that could be repurposed? Since overweight and obesity worsen osteoarthritis symptoms by placing excess strain on weight-bearing joints, GLP-1 agonists such as semaglutide have proven that they can help by promoting rapid weight loss, as demonstrated by the STEP-9 trial.
Research into GLP-1s has now revealed that they may offer a whole constellation of other benefits, such as a potential reduction in stroke risk. Now, it appears that GLP-1 agonists may have a direct effect on osteoarthritis independent of weight loss. In our podcast, we look at a recently published article in Cell Metabolism that suggests that GLP-1 agonists might go beyond just the weight loss – promote actual cartilage regrowth by jumpstarting the joint cells’ energy processing pathways. We also explore some of the caveats of potentially using GLP-1 agonists in this way, such as a lack of understanding of the long term effects, as well as the well-documented occurrence of muscle loss.
By Dr Kashmal Kalan, Medical Director, Alvi Armani
In 2023, global prescriptions for GLP-1 weight loss medications rose by more than 40%, with drugs like Ozempic and Wegovy moving from specialist clinics into everyday conversation. Alongside this surge, a new concern is appearing more frequently in consultation rooms: unexpected hair loss.
For many patients, the timing is deeply unsettling. After months of discipline and visible progress, they start to notice more hair in the shower, on their pillow, or in their brush. The immediate fear is that something has gone wrong – that the medication is damaging their body, that the weight loss has come at a hidden cost, or something more serious.
In most cases, the reality is more nuanced. At Alvi Armani, we are seeing a consistent pattern: hair loss following rapid weight loss is real, but it is rarely caused by GLP-1 medications alone, despite how often this link is assumed. Instead, it reflects how the body responds to sudden physiological stress.
Hair loss often arrives late
The most common diagnosis in these cases is telogen effluvium, a form of temporary shedding that occurs when a large number of hair follicles shift prematurely into a resting phase. The critical detail is timing – the hair does not fall out immediately but rather sheds months after the original trigger.
This delay is what makes the experience so confusing. By the time hair begins to thin, weight loss may already feel stable, lifestyle changes established, and the initial stress long past. But biologically, the body is only now expressing the shock it absorbed earlier.
In some individuals, this shedding also unmasks an underlying genetic tendency toward pattern hair loss, known as androgenetic alopecia. While rapid weight loss does not create this condition, it can reveal it sooner than expected. What begins as temporary shedding may gradually shift into more persistent thinning – a progression that is emotionally difficult precisely because it feels so unexpected.
Why the body sacrifices hair first
Hair is not essential to survival. When the body experiences stress – whether through rapid fat loss, hormonal shifts, illness, or nutritional restriction – it reallocates resources to protect vital systems. Hair growth is one of the first processes to be downregulated.
Importantly, stress-related shedding does not create a new condition. It accelerates what was already encoded in the body. The hair is not “breaking down”; it is responding to a shift in internal priorities.
The speed of change is critical. Gradual, steady weight loss allows the body time to adapt hormonally and metabolically. Rapid loss, particularly when paired with appetite suppression, elevated stress hormones, or inadequate protein intake, creates a perfect storm for hair disruption.
From a biological perspective, shedding is not a malfunction, but rather an adaptive response. But from a patient’s perspective, it feels personal, visible, and deeply unsettling.
Who tends to notice it most
Women often become aware of thinning first, partly because longer hair makes shedding more obvious, and partly because changes in density carry greater emotional weight. Individuals with a family history of hair loss are also more vulnerable, as are those who lose a significant percentage of body weight in a short period of time.
Nutrition matters more than most realise
Hair is metabolically demanding tissue. It requires consistent access to protein, iron, zinc, and a range of micronutrients to maintain its growth cycle. When intake drops sharply because of appetite suppression, restrictive dieting, or poorly supervised medication use, hair becomes collateral damage.
This is why medically guided weight loss is so important. GLP-1 medications can be powerful tools, but they must be paired with nutritional planning. The body can tolerate change; what it struggles with is deprivation disguised as progress.
Temporary or permanent?
For many patients, telogen effluvium resolves within six to nine months once the body stabilises. Hair regrowth is slow, but it does occur.
However, in those with genetic susceptibility, the episode may mark the beginning of more sustained thinning. This does not mean damage has been done, but it does mean the window for early intervention matters. The earlier changes are recognised, the more options exist to slow or stabilise progression.
When hair loss deserves attention
Shedding should not be ignored if it persists beyond three to six months, if overall density continues to decline, or if there is a strong family history of pattern hair loss. Hair changes are often the first visible signal that the body is struggling to adapt to internal stress.
Early assessment allows for accurate diagnosis, realistic expectations, and far better long-term outcomes.
A final thought on balance
GLP-1 medications have transformed the weight loss landscape, and for many people, they offer genuine health benefits. But transformation should never come at the cost of physiological stability.
Hair is not separate from health. It is one of its most sensitive mirrors. Protecting the body protects the hair. Sustainable change, guided by medical support, remains the most reliable way to achieve results that last – without unexpected consequences.
When Americans begin taking appetite-suppressing drugs like semaglutide, the changes extend well beyond the bathroom scale. According to new research, the medications are associated with meaningful reductions in how much households spend on food, both at the grocery store and at restaurants.
The study, published December 18 in the Journal of Marketing Research, links survey data on GLP-1 receptor agonist use with detailed transaction records from tens of thousands of U.S. households. The result is one of the most comprehensive looks yet at how GLP-1 adoption is associated with changes in everyday food purchasing in the real world.
The headline finding is striking: Within six months of starting a GLP-1 medication, households reduce grocery spending by an average of 5.3%. Among higher-income households, the drop is even steeper, at more than 8%. Spending at fast-food restaurants, coffee shops and other limited-service eateries falls by about 8%.
Among households who continue using the medication, lower food spending persists at least a year, though the magnitude of the reduction becomes smaller over time, say co-authors, assistant professor Sylvia Hristakeva and professor Jura Liaukonyte, both in the Charles H. Dyson School of Applied Economics and Management in the Cornell SC Johnson College of Business.
“The data show clear changes in food spending following adoption,” Hristakeva said. “After discontinuation, the effects become smaller and harder to distinguish from pre-adoption spending patterns.”
Unlike previous studies that relied on self-reported eating habits, the new analysis draws on purchase data collected by Numerator, a market research firm that tracks grocery and restaurant transactions for a nationally representative panel of about 150 000 households. The researchers matched those records with repeated surveys asking whether household members were taking GLP-1 drugs, when they started and why.
That combination allowed the team to compare adopters with similar households that did not use the drugs, isolating changes that occurred after medication began.
The reductions were not evenly distributed across the grocery store.
Ultra-processed, calorie-dense foods – the kinds most closely associated with cravings – saw the sharpest declines. Spending on savory snacks dropped by about 10%, with similarly large decreases in sweets, baked goods and cookies. Even staples like bread, meat and eggs declined.
Only a handful of categories showed increases. Yogurt rose the most, followed by fresh fruit, nutrition bars and meat snacks.
“The main pattern is a reduction in overall food purchases. Only a small number of categories show increases, and those increases are modest relative to the overall decline,” Hristakeva said.
The effects extended beyond the supermarket. Spending at limited-service restaurants such as fast-food chains and coffee shops fell sharply as well.
The study also sheds light on who is taking GLP-1 medications. The share of U.S. households reporting at least one user rose from about 11% in late 2023 to more than 16% by mid-2024. Weight-loss users skew younger and wealthier, while those taking the drugs for diabetes are older and more evenly distributed across income groups.
Notably, about one-third of users stopped taking the medication during the study period. When they did, their food spending reverted to pre-adoption levels – and their grocery baskets became slightly less healthy than before they started, driven in part by increased spending on categories such as candy and chocolate.
That movement underscores an important limitation, the authors caution. The study cannot fully separate the biological effects of the drugs from other lifestyle changes users may make at the same time. However, evidence from clinical trials, combined with the observed reversion in spending after discontinuation, suggests appetite suppression is likely a key mechanism behind the spending changes.
The findings carry implications far beyond individual households.
For food manufacturers, restaurants and retailers, widespread GLP-1 adoption could mean long-term shifts in demand, particularly for snack foods and fast food. Package sizes, product formulations and marketing strategies may need to change. For policymakers and public-health experts, the results add context to ongoing debates about the role of medical treatments in shaping dietary behavior – and whether biologically driven appetite changes succeed where taxes and labels have struggled.
“At current adoption rates, even relatively modest changes at the household level can have meaningful aggregate effects,” Hristakeva said. “Understanding these demand shifts is therefore important for assessing food markets and consumer spending.”
With several important developments on the horizon, 2026 is set to be another eventful year in healthcare. Photo by Anna Shvets
19th January 2026 | By Marcus Low
From the limited rollout of a new HIV prevention jab to developments with new weight loss medicines, to high-stakes court cases relating to National Health Insurance (NHI), 2026 is set to be another tumultuous year in healthcare. Here are nine stories that Spotlight will keep a close eye on.
1. How will things go with the local rollout of a new HIV prevention jab?
Given the high rates of HIV in South Africa, the biggest HIV story this year is likely to be the rollout of a new HIV prevention jab at around 360 (roughly 10%) of South Africa’s public sector clinics. The jab, which contains the antiretroviral medicine lenacapavir, provides six months of protection against HIV infection at a time. It could be a gamechanger for people who, for whatever reason, struggle to take daily prevention pills. We will be tracking how and to whom the jab is made available and whether uptake meets expectations.
As we reported last year, work is also underway on a new lenacapavir formulation that could provide 12 months of protection per shot. We’ll be scouring journals and conference programmes for new data on this formulation.
2. Will we see better access to weight loss medicines?
The class of diabetes and weight loss drugs called GLP1-RAs have taken the world by storm in recent years. Until recently, drugs like semaglutide (brand names Ozempic or Wegovy) and tirzepatide (brand names Zepbound or Mounjaro) were only available as injections. The GLP1-RA market is, however, set to be upended by the introduction of some of these medicines in pill form. The United States Food and Drug Administration (FDA) recently registered a semaglutide pill for use for weight loss. Another weight loss pill called orforglipron is also expected to be registered this year. One big question is when these pills will be registered and made available in South Africa and at what price.
Another important GLP1-RA development this year will be the expiration of a key patent on semaglutide in India. This will open the door to generic manufacturers bringing their own versions of semaglutide to market – something that usually leads to substantial price reductions. We will be keeping a close eye on how this situation plays out and analysing what the implications are for people in South Africa.
3. Might we see earlier than expected findings from pivotal TB vaccine trials?
The one TB vaccine we have is over a hundred years old and only provides limited protection for kids. Several experimental vaccines are, however, currently being evaluated in late-stage clinical trials. Arguably, the most notable of these is the M72 vaccine, which is being assessed in a massive phase 3 study, partly conducted in South Africa.
While timelines suggest most of the key TB vaccine studies will not yet have anything to report this year, it is possible that we might see a surprise or two. Findings are sometimes reported early if it becomes apparent ahead of schedule that a medicine or vaccine is clearly working, or clearly not working, as the case may be. Whether or not we see findings this year, it is important to start thinking about what a rollout might look like in our health system should results be as good as hoped. The M72 vaccine had around 50% efficacy in phase 2 trials, so there is reason for optimism.
4. Will we see a concrete plan to address public sector healthcare worker shortages?
Arguably, the most important dynamic in South Africa’s public healthcare system today is that provincial health departments are not employing enough healthcare workers across multiple categories. One reason for this is simply that budgets have generally shrunk over the last decade – obviously corruption and mismanagement in several provincial departments have made things even worse. There was a glimmer of hope in last year’s budget in which we saw a meaningful upturn in health funding for the first time in years, but that was at best a good first step toward recovery. As we enter 2026, our understanding is that all of the nine provinces are still facing severe healthcare worker shortages.
More money for health in the next budget will certainly help, but there is a broader sense that government doesn’t really have a big picture vision for how to address the crisis. We do have a 2030 Human Resources for Health Strategy, but as with many such strategies, it seems to have so far gone largely unimplemented.
5. Will enablers be held accountable for corruption such as that at Thembisa Hospital?
One of last year’s big media moments was a Special Investigating Unit (SIU) press conference in which they described the extensive corruption said to have taken place at Thembisa Hospital. One snag, however, is that while the SIU can recoup funds and take matters to the Special Tribunal, the SIU does not conduct criminal prosecutions – though they can refer matters to the National Prosecuting Authority (NPA) for prosecution. Whether we will see successful NPA prosecutions relating to the Thembisa Hospital corruption is one of the year’s top questions.
Unfortunately, even when the SIU does sterling work and delivers cases to the NPA on a plate, there is no guarantee that the NPA will do its job. One depressing example is that of Buthelezi EMS. Last year, the Special Tribunal ordered Buthelezi EMS (and other companies with similar names) to pay over half-a-billion Rand back to the state. The SIU also referred a related matter to the NPA in 2024 for prosecution, but Spotlight understands that the NPA has rather mind-bogglingly decided to drop the matter.
6. Which, if any, senior health leaders will lose their jobs this year?
While we won’t have national or provincial elections this year, that is no guarantee that we won’t see any health leaders losing their jobs. Over the last two decades, there have after all been many examples of people being ousted between elections, be it for purely political reasons or due to corruption scandals.
Possibly the political leader in the health sector at greatest risk is KwaZulu-Natal MEC for Health, Nomagugu Simelane. Should the currently governing coalition of political parties in the province crumble, as it seems it might do, chances are several new MECs will be deployed, including for the health portfolio.
There is also an outside chance that the country’s top health official, Dr Sandile Buthelezi, Director-General for Health in the National Department of Health, might be forced to step down. As reported by AmaBhungane, Buthelezi played a central role in an “irregular” R836-million oxygen procurement process and is also “at the centre of aHawks investigation into allegations that he solicited a R500 000 bribe”. Our understanding is that Buthelezi has not been charged and that in the absence of charges he will stay in the job.
7. What will happen in the landmark NHI court cases?
Despite a new call for dialogue from Finance Minister Enoch Godongwana, chances for a political settlement over National Health Insurance (NHI) remains very low. The bottom line remains that Health Minister Dr Aaron Motsoaledi refuses to yield an inch on the version of NHI described in the Act and President Cyril Ramaphosa is not willing to force the matter.
Instead, it seems the battle over NHI will this year be fought mainly in the courts. At our count, there are at least eight cases challenging the NHI Act, parts of the Act, or the process resulting in the Act. A first development to look out for is whether or not some of the cases will be combined and heard together. In case you missed it, last year we published a two-part series in which we tried to pin down the issues on which these court cases are likely to turn (see part 1 and part 2).
While we will cover the NHI court cases in some depth, we will also try to foster constructive discussions on health reforms on our opinion pages and in our analysis. In our view, it is dangerously limiting to reduce the debate over South Africa’s healthcare reforms to a simple binary of whether one is for or against NHI.
8. What will be left of the FDA, NIH, and CDC by the end of 2026?
It used to be the case that United States Food and Drug Administration (FDA) decisions and health advice from the United States Centres for Disease Control and Prevention (CDC) carried a lot of weight around the world. In recent months, however, there have been increasing signs of political interference at these institutions and a turn away from evidence-based policy making. It seems inevitable that we will see more of the same in 2026 and the credibility of both the CDC and probably also the FDA will be further diminished.
Similarly, the US National Institutes for Health (NIH) has been the world’s leading funder of health research for many years. But as with the CDC, the work of the NIH has been overly politicised over the last year and its reputation for rigour and scientific excellence has already been severely degraded. As with the FDA and CDC, the outlook is bleak.
9. How well will SA and other countries recover from last year’s US aid cuts?
With the dust settling after last year’s severe and abrupt cuts to US healthcare aid and US funding for medical research, the longer-term impacts of those cuts in South Africa and neighbouring countries should become clearer this year. Among others, we will get the first reliable estimates of key HIV and TB indicators for 2025 (reliable figures for a specific year are typically only published in the subsequent year). New HIV estimates from the Thembisa mathematical model (Spotlight’s preferred source for HIV estimates) should be out around the middle of the year, while new World Health Organization (WHO) TB estimates are usually released in November.
Last year Motsoaledi was widely criticised by activists for underplaying the seriousness of the cuts for South Africa’s HIV response and the scale of specialised services and capacity that was destroyed here. Eventually some extra funds were made available in response to the cuts, but it amounted to only a small fraction of what was lost. The harsh reality is that in some places the aftermath of the aid cuts will be felt for years to come.
At an international level, we are also not convinced that a clear roadmap has been set out for building back better after US withdrawal, though we’d be happy to be proven wrong. What is clear though is that entities like the WHO and UNAIDS are facing unprecedented financial and political pressures – it seems possible that UNAIDS will no longer exist a year from now. Much reform has already been undertaken at the WHO. By the end of the year, we should have some sense of whether things have stabilised and whether a coalition of willing nations is truly committed to keeping the WHO and multilateralism in health alive.
We have outlined only nine health issues in the above, but there are of course many more questions that we could have added to this list. Some of those include:
Whether we will see meaningful improvement in the South African government’s response to non-communicable diseases such as diabetes, cancers, and mental health conditions.
How well implementation of South Africa’s latest TB recovery plan is going, and in particular how we are doing against the target of testing five million people in 12 months.
How climate change will impact people’s health and whether the South African government is prepared for it.
Whether South Africa will see real progress in addressing antimicrobial resistance. After adopting a good policy a few years ago, it appears momentum has been lost.
Whether the state will start taking xenophobia in the healthcare system and around clinics and hospitals more seriously, as a recent court judgment requires it to do.
Whether we will see legislation introduced amending the Patents Act in line with a policy adopted by government in 2018 and whether we’ll see progress on the much-delayed State Liability Bill, which should have relevance for the state’s vulnerability to medico-legal claims.
Whether we will see concrete steps forward with the new electronic health records and data systems government is developing.
What progress we might see with the local production of vaccines and pharmaceuticals – one of the areas in which we are quite optimistic, despite the lack of coherent and enabling government policy.
What impact AI will, or will not, have in our healthcare system this year.
Are there issues not mentioned here that you think Spotlight should cover in 2026? Let us know by commenting below this article or by tagging us on BlueSky.
A new University of California San Diego study offers compelling evidence that GLP-1 receptor agonists may do more than regulate blood sugar and weight. In an analysis of more than 6800 colon cancer patients across all University of California Health sites, researchers found that those taking glucagon-like peptide-1 (GLP-1) medications were less than half as likely to die within five years compared to those who weren’t on the drugs (15.5% vs 37.1%).
The study, led by Raphael Cuomo, PhD, used real-world clinical data from the University of California Health Data Warehouse to assess outcomes across the state’s academic medical centres. After adjusting for age, body mass index (BMI), disease severity and other health factors, GLP-1 users still showed significantly lower odds of death, suggesting a strong and independent protective effect.
The survival benefit appeared most pronounced in patients with very high BMI (over 35), hinting that GLP-1 drugs may help counteract the inflammatory and metabolic conditions that worsen colon cancer prognosis. Researchers believe several biological mechanisms could explain the link. Beyond regulating blood sugar, GLP-1 receptor agonists reduce systemic inflammation, improve insulin sensitivity and promote weight loss – all factors that can dampen tumour-promoting pathways. Laboratory studies also suggest that GLP-1 drugs may directly prevent cancer cell growth, trigger cancer cell death and reshape the tumour microenvironment. However, the study authors emphasise that more research is needed to confirm these mechanisms and determine whether the survival benefit observed in this real-world analysis represents a direct anti-cancer effect or an indirect result of improved metabolic health.
Cuomo notes that while these results are observational, they underscore an urgent need for clinical trials to test whether GLP-1 drugs can improve cancer survival rates, especially for patients with obesity-related cancers.
Mass General Brigham researchers used real-world data to conduct a head-to-head study to investigate cardioprotective effects, finding both medications reduced risk.
Pexels Photo by Freestocksorg
A new study from Mass General Brigham provides head-to-head evidence comparing the cardioprotective effects of tirzepatide and semaglutide. The researchers found both medications reduced the risk of heart attack, stroke, and death from any cause. The study is published in Nature Medicine, with results simultaneously presented at the American Heart Association Scientific Sessions 2025.
Previous research shows that semaglutide protects against cardiovascular events like heart attack or stroke. But it wasn’t clear if tirzepatide, also commonly prescribed for type 2 diabetes, has the same cardiovascular benefits.
Researchers used US claims databases to compare the cardiovascular outcomes of nearly one million adults taking tirzepatide, semaglutide, or other medications for type 2 diabetes.
“Randomised controlled trials are often considered the reference standard in the medical evidence generation process. However, not all questions can be answered using this time- and resource-intensive method,” said first author Nils Krüger, MD, a research fellow in the Division of Pharmacoepidemiology and Pharmacoeconomics in the Mass General Brigham Department of Medicine. “Data generated in clinical practice and used secondarily for research allow us to address a wide range of clinically relevant questions time- and resource-effectively – when applied correctly. Moreover, we can study patients who reflect the reality of everyday clinical care, in contrast to the highly selected participants of randomized experiments.”
The study demonstrated a cardiovascular benefit for patients at risk for adverse cardiovascular events who had type 2 diabetes. Compared with sitagliptin, a diabetes drug that has shown neutral effects on cardiovascular outcomes, semaglutide reduced the risk of stroke and heart attack by 18 percent. Treatment with tirzepatide lowered the risk of stroke, heart attack, and death by 13 percent compared to dulaglutide, another GLP-1 receptor agonist that has been available for many years.
“Both drugs show strong cardioprotective effects. Our data also indicate that these benefits occur early, suggesting that their protective mechanisms go beyond weight loss alone,” said Krüger. The exact biological mechanisms underlying these protective effects remain unknown.
Because these medications have only recently become available, studies confirming their cardioprotective mechanisms – particularly those directly comparing the two dominant GLP-1 agents, tirzepatide and semaglutide – are still lacking.
“According to recently presented database analyses by the respective manufacturers, each company’s own drug appears to reduce cardiovascular risk much more effectively than the competitor’s,” said Krüger. “However, our study found only small differences between tirzepatide and semaglutide in cardiovascular protection among populations at risk of adverse events, underscoring that both agents provide protective benefit and could be integrated into clinical cardiovascular practice.”
“We hope that our study will help clinicians better understand how these new medications work in clinical practice. Our transparent and open science practices, including pre-registration of a public protocol and shared analytic code, are designed to support scientific discussion,” said last author Shirley Wang, PhD, an associate epidemiologist in the Division of Pharmacoepidemiology and Pharmacoeconomics in the Mass General Brigham Department of Medicine.
A new movement in weight management is taking hold in South Africa as the country confronts weight-related illnesses. A powerful class of medication known as GLP-1 therapies is proving highly effective in cutting obesity rates, lowering cancer risk, and improving overall metabolic health. Their growing popularity marks a new frontline in the fight against sugar-driven disease.
A landmark study published in JAMA Oncology has revealed that patients using GLP-1 medications – a class of therapies originally developed for type 2 diabetes – experienced a 17% lower overall risk of cancer.
The data, drawn from over 86 000 patients, showed striking reductions in specific cancers: ovarian cancer risk nearly halved, meningioma cases fell by 31%, and endometrial cancer dropped by 25%.
Dr Tommie Smook, medical practitioner at Dr Smook & Partners (managed by RXME Group), says these findings reinforce the urgent need to fight back against sugar-related disease:
“We are witnessing the medical consequences of unchecked sugar consumption every day in practice. Obesity has become one of the greatest epidemics of our time. If we are serious about safeguarding public health, we must declare a national war on sugar – and GLP-1s are among the most powerful tools we now have to help people reclaim their health.”
What GLP-1s actually do
The body naturally produces GLP-1 – a hormone that regulates blood sugar, appetite, and digestion. GLP-1 medications mimic this process:
• They slow stomach emptying,
• Reduce hunger and cravings,
• Help patients feel satisfied with smaller portions, and
• Stabilise blood sugar levels.
The result is sustained weight loss. Clinical trials consistently show patients losing 10-15% of body weight, particularly when therapy is combined with nutrition, exercise, and professional support. In South Africa, several GLP-1s are now formally registered for obesity and chronic weight management.
But the benefits don’t end at weight loss. International studies have demonstrated improvements in cardiovascular health – lowering blood pressure, reducing inflammation, and decreasing the risk of heart attacks and strokes. Emerging evidence also suggests neuroprotective effects, with potential to reduce risks of dementia and Alzheimer’s disease.
From diabetes treatment to disease prevention
“GLP-1s are no longer just diabetes drugs,” says Dr Smook. “They are transforming the way we think about weight, chronic disease, and prevention. When used responsibly under medical guidance, these therapies can change not only waistlines, but lifespans.”
At Dr Smook & Partners, patients gain access to GLP-1 therapy under the supervision of qualified medical doctors. Medications are prepared only through SAHPRA-approved compounding pharmacies, ensuring quality and safety. This is supported by a multidisciplinary team – dietitians, biokineticists, nurses, and sports physicians, providing holistic care.
Here are the five essentials you should consider before starting GLP-1 therapy:
See a doctor first – these medications require proper screening and monitoring.
Think beyond injections – lifestyle, diet, and exercise remain vital.
Expect an adjustment phase – side effects like nausea are usually temporary.
Protect lean muscle – resistance training and adequate protein intake are essential.
Avoid shortcuts – unregulated, black-market products are unsafe and unpredictable.
A turning point for public health
Obesity is a modern epidemic, and sugar is at the heart of it. GLP-1 medications are not a “quick fix,” but they represent one of the most promising advances in decades – a way to tackle both the causes and consequences of excess weight.
Dr Smook concludes: “The stigma around GLP-1s must end. These therapies are not about vanity – they are about survival. Every patient who regains control of their health is one step closer to breaking sugar’s grip on our society.”