Scientists at Trinity College Dublin have discovered a new process in the immune system that leads to the production of an important family of anti-viral proteins called interferons. They hope the discovery will now lead to new, effective therapies for people with some autoimmune and infectious diseases.
Reporting in Nature Metabolism, Luke O’Neill, Professor of Biochemistry in the School of Biochemistry and Immunology at Trinity, and his team have found that a natural metabolite called Itaconate can stimulate immune cells to make interferons by blocking an enzyme called SDH.
Co-lead author, Shane O’Carroll, from Trinity’s School of Biochemistry and Immunology, said: “We have linked the enzyme SDH to the production of interferons in an immune cell type called the macrophage. We hope our work will help the effort to develop better strategies to fight viruses because interferons are major players in how our innate immune system eliminates viruses – including COVID-19.”
Co-lead author, Christian Peace, from Trinity’s School of Biochemistry and Immunology, added: “Itaconate is a fascinating molecule made by macrophages during infections. It’s already known to suppress damaging inflammation but now we have found how it promotes anti-viral interferons.”
Working with drug companies Eli Lilly and Sitryx Ltd, the next step is to test new therapies based on Itaconate in various diseases, with some autoimmune diseases and some infectious diseases on the likely list. And the work potentially extends to other disease contexts in which SDH is inhibited, such as cancer, and could reveal a new therapeutic target for SDH-deficient tumours.
Prof O’Neill said: “With Itaconate you get two for the price of one – not only can it block harmful inflammation, but it can also help fight infections. We have discovered important mechanisms for both and the hope now is that patients will benefit from new therapies that exploit Itaconate and its impacts.”
Clinical trials in patients are set to start next year.
In June, we heard what could be this year’s biggest HIV breakthrough: a twice-yearly injection can prevent HIV infection. Findings from a second large study of the jab has now confirmed that it works. Elri Voigt goes over the new findings and unpacks the licenses that are expected to facilitate the availability of generic versions of the jab in over a hundred countries, including South Africa.
The second of two pivotal studies of a six-monthly HIV prevention injection containing the antiretroviral drug lenacapavir has confirmed that the jab works remarkably well.
The first study, called PURPOSE 1, found that the jab is safe and highly effective at preventing HIV infection in women. The second, called PURPOSE 2, found the same for cisgender men, transgender men, transgender women and non-binary people who have sex with men assigned male at birth.
Interim findings from PURPOSE 2 were presented last week at the HIV Research for Prevention (HIVR4P) conference in Lima, Peru.
The researchers compared the safety and efficacy of lenacapavir injections every six months to a daily HIV prevention pill – a combination of emtricitabine and tenofovir disoproxil fumarate, called F/TDF. The results have not yet been published in a peer reviewed journal, but is expected to be soon, according to Principal Investigator for PURPOSE 2 Dr Colleen Kelley, a professor of medicine at Emory University’s School of Medicine.
In the PURPOSE 1 study, none of the 2 134 people receiving the lenacapavir injection got HIV during the study. In PURPOSE 2, there were two HIV infections among the 2 179 people receiving the injection. These numbers are dramatically better than those for HIV prevention pills and for people in the communities where the study was done who were not receiving prevention injections or pills.
These findings mean the evidence is now in place for the manufacturer, Gilead Sciences, to file with regulatory authorities to register lenacapavir injections for HIV prevention. Such registration is required before the jab can be marketed for prevention. Lenacapavir injections are already registered in some countries as a last resort treatment for HIV, but not yet in South Africa.
“Now that we have a comprehensive dataset across multiple study populations, Gilead will work urgently with regulatory, government, public health and community partners to ensure that, if approved, we can deliver twice-yearly lenacapavir for PrEP worldwide, for all those who want or need PrEP,” Daniel O’Day, the chairperson and Chief Executive Officer of Gilead said in a press release. (PrEP, or pre-exposure prophylaxis, refers to taking antiretrovirals to prevent HIV infection.)
Top line findings
The interim results presented at HIVR4P by Kelley, showed that when compared to the background HIV incidence calculated in the study, lenacapavir reduced HIV infections by 96%. And when compared to the F/TDF prevention pill, the injection reduced HIV infections by 89%.
Among the 3 265 participants enrolled in the study, 11 people acquired HIV- two of the 2 179 people who were assigned to the lenacapavir arm and nine of the 1 086 participants assigned to the prevention pill arm. This translated to HIV incidence of 0.93 per 100 person years in the prevention pill arm compared to only 0.1 per 100 person years in the lenacapavir arm.
This was compared to the background incidence, which was determined when screening eligible participants for HIV. Out of 4 634 people screened for the study, 378 or 8.2% were diagnosed with HIV. Based on further laboratory testing, it was estimated that of those 378 people, 45 or 11.9% recently acquired HIV (classified as being within the last 120 days or so). This latter group provided the background HIV incidence, which was estimated to be 2.37 per 100 person years.
This is a novel study design, Kelley told Spotlight, because this calculation was used to estimate the HIV incidence that would have occurred in a placebo group without actually enrolling a placebo group.
“It’s no longer ethical to have a placebo group in HIV PrEP trials because we know that we have effective PrEP agents,” she said. “Yet, it’s almost essential to have a placebo group when you design a clinical trial so that you can really say how effective your medication, your new agent is [compared] to having nothing.”
When asked at a press conference about the two breakthrough infections in the lenacapavir arm, Kelley said the analysis for this is ongoing and will hopefully be available at a future conference and in a journal soon. She said that the two breakthrough infections in the lenacapavir arm were detected by routine testing during the study.
Principal Investigator for PURPOSE 2 Professor Colleen Kelley at the 5th HIV Research for Prevention Conference in Lima, Peru. (Photo: Nicole Bergman/IAS)
Kelley added that around 90% of participants in the two study arms were able to receive their injection on time. “So, we at least know that the injections were delivered in a timely fashion for almost all participants,” she said.
Whether or not the two infections occurred in people who had received the jabs on time and according to the study protocol will be closely watched as more study details is shared in the coming months.
To be enrolled in the study, participants had to meet several criteria. They had to be older than 16, never received HIV prevention injections before, weigh more than 35kg, have good kidney function, not have been tested for HIV in the last 12 weeks, and had to have been sexually active in the last 12 months.
All study participants were given a pill a day and an injection, those in the lenacapavir arm received two 1.5 ml lenacapavir injections every six months and a daily placebo pill, while those in the prevention pill arm received the daily F/TDF pill and a placebo injection every six months.
The study was conducted across seven countries, with 6 sites located in South Africa and others in Argentina, Brazil, Mexico, Peru, Thailand, and the United States, according to study data on Gilead’s website.
Safety data
Overall, Kelley said lenacapavir was safe and well-tolerated despite some side effects, mainly related to the injections. A total of 43 people dropped out of the study due to side effects.
The most common adverse event in the study was injection site reactions. There were more injection site reactions in the lenacapavir arm compared to the prevention pill arm. 29 people dropped out of the study because of these, 26 in the lenacapavir arm and 3 in the prevention pill arm (people in this study arm received placebo jabs).
The most common injection site reaction were subcutaneous nodules – these are harmless, usually invisible, small lumps under the skin. Nodules occur because lenacapavir is injected under the skin where it forms a drug depot. Injection site reactions and nodule size decreased with subsequent injections. This side effect and trend of decreasing reactions was also noted in the PURPOSE 1 study. Other injection site reactions were pain and erythema which is a type of skin rash.
According to Kelley, there were no serious adverse events related to injection site reactions.
When injection site reactions are excluded, according to Kelley, the other adverse events were similar across both arms, with 74% of participants in each arm experiencing an adverse event. The majority were mild or moderate.
Seven participants in each study arm dropped out due to side effects that weren’t related to injection site reactions. Those who discontinued from the lenacapavir arm will be given prevention pills for a year. This is done to protect these participants, Kelley explained, from potentially acquiring HIV when lenacapavir levels wane, as well as to reduce the risk of potential drug resistance developing.
There were a few serious adverse events, although Kelley told Spotlight she does not currently have any additional information on what these were. She explained that a serious adverse event is generally classified as something like hospitalisation, a life-threatening condition, an important medical event or adverse pregnancy outcome.
“Usually when we look at something like this, we look at the rates compared in the two arms of the study and it was 3% in the LEN [lenacapavir] arm and 4% in the F/TDF arm, so they were equal, essentially the same in both study arms,” Kelly said.
There were six deaths during the study, but none were related to the study drugs.
Next steps for lenacapavir
Now that the interim results have been announced, both studies have been unblinded and entered an open-label phase where participants have the choice of switching to or continuing with the injection.
Professor Linda-Gail Bekker, the Chief Executive Officer at the Desmond Tutu Health Foundation, recently said on a webinar hosted by the South African Health Technologies Advocacy Coalition, that study participants are now able to use the PrEP option they’d prefer – either oral PrEP or the injection. This means all participants will be able to access lenacapavir through the studies if they wanted to use it.
But it will likely be a while before anyone outside of these studies can access lenacapavir as HIV prevention.
“This is an incredible intervention. Now we have to make sure everyone can get it and that’s going to be the most important next step, ensuring that everyone who needs this drug has access,” Kelley told Spotlight.
Gilead’s generic licensing agreement and pricing
What we do know so far about the next steps for lenacapavir is that the process to allow for generic manufacturing has started. This month, Gilead released its voluntary licensing agreements with six generic companies for manufacturing cheaper versions of lenacapavir.
Dr Andrew Gray, a senior lecturer in Pharmacology at the University of KwaZulu-Natal, told Spotlight that no South African firms have been included in the voluntary licenses – four of the generic licensees are in India, one is in Pakistan, and one is in Egypt.
“In essence, they [the generic companies] are allowed to sell their generic versions in a number of identified countries, specified by Gilead,” Gray said. The agreement lists 120 countries, including South Africa.
Gilead itself will also be prioritising the registration of lenacapavir in 18 countries, which it said represent about 70% of the HIV burden in the countries named in the license. The list includes South Africa, Uganda, and Botswana. Gilead says it will start filing for registration with regulatory authorities by the end of the year.
It will be important to see how quickly Gilead seeks regulatory approval for lenacapavir with the South African Health Products Regulatory Authority (SAHPRA), Gray said. Registration with SAHPRA will be required before the injection can be rolled out in South Africa.
In putting together this timeline, we’ve spoken to several well-placed experts, but we stress that this is very much a back-of-the-envelope exercise and far from set in stone. (Infograph: Spotlight)
Some countries won’t be able to procure generics
Gilead received criticism for several omissions from the list of countries that the generic manufacturers can sell to. The US-based HIV advocacy group AIDS Vaccine Advocacy Coalition, among others, pointed out the exclusion of several countries which have high HIV incidence. Some of those countries participated in PURPOSE 2- namely Brazil, Argentina, Mexico and Peru.
A spokesperson from Gilead told Spotlight the manufacturer’s access policy included tailored approaches to ensure rapid and broad access of lenacapavir and it objectively considered the countries where a voluntary licence would provide the most benefit.
“Gilead’s voluntary licence primarily covers countries based on economic need and HIV burden, which are primarily low- and lower-middle income countries. The voluntary licence also covers certain middle-income countries with limited access to healthcare,” the spokesperson said.
Acknowledging that some middle-income countries do have a high HIV burden, Gilead is “exploring several innovative strategies to support access to LEN for PrEP (if approved), including tiered pricing, and are working with payors to establish fast, efficient pathways to help reach people who need or want PrEP”, said the spokesperson.
“Ensuring access in middle-income and upper-middle income countries, including those in Latin America, is a priority for Gilead. Planning for these countries, incorporating input from advocates and global health organizations, is ongoing and updates will be shared as discussions progress,” the spokesperson added. “Additionally, Gilead is committed to ensuring that individuals who participated in the PURPOSE studies have been offered and will be able to stay on open label lenacapavir until it is available in their country.”
The company’s decision to license generic manufacturers directly is at odds with earlier calls from several activist groups and UNAIDS to license via the UN-backed Medicines Patent Pool.
Pricing
It will also be important to see if Gilead will disclose a single exit price for the South African market, according to Gray.
In its press release announcing the voluntary licensing agreement, Gilead stated it will “support low-cost access to the drug in high-incidence, resource-limited countries through a two-part strategy: establishing a robust voluntary licensing program and planning to provide Gilead-supplied product at no profit to Gilead until generic manufacturers are able to fully support demand”.
It is too early in the process to reveal a price for lenacapavir yet, the spokesperson from Gilead told Spotlight.
“While Gilead prepares for global regulatory filings, it is too early to disclose the price of lenacapavir for HIV prevention. Our pledge is to price our medicines to reflect the value they deliver to people, patients, healthcare systems and society. For Gilead-branded lenacapavir, we do plan to price it at no profit to Gilead in 18 select high-incidence, resource-limited countries until generic manufacturers are able to fully support demand,” the spokesperson said.
Spotlight previously reported on research that estimated that if produced at sufficient volumes, the price of lenacapavir could be drastically reduced to levels likely considered affordable by the South African government. For instance, if enough volume was produced to supply 10 million people with PrEP, the price for the injection could be as low as $40 (under R800) per person per year. At the moment, Gilead supplies lenacapavir for HIV treatment in wealthy countries for about $40 000 per person per year.
Gilead’s lenacapavir product will be the first to register in South Africa and will almost certainly be the only lenacapavir product available here for several years – that is because it is expected to take generic manufacturers a few years before they can start producing generic lenacapavir. Based on calculations made for other PrEP products, it seems unlikely that the Department of Health would be willing to procure lenacapavir at a price significantly above R1 000 per person per year. The HIV prevention pill currently costs government around R800 per person per year.
Initial prescriptions of benzodiazepines, a class of drugs used to treat anxiety and sleep problems after a stroke may include too many pills for adults ages 65 or older, finds new study in the Stroke journal
Photo by Towfiqu Barbhuiya on Unsplash
Although there has been a slight downward trend in the prescription of benzodiazepines (depressants that relieve anxiety, muscle spasms, produce sedation and reduce seizures) among older adults over the last decade, the rate of first-time prescriptions for these medications after an ischaemic stroke is still sizable, according to research published today in Stroke.
After a stroke, benzodiazepines may be used to calm anxiety and improve sleep, but also have a potential for abuse and addiction. When prescribed to older adults, these medications may increase the risk of falls and broken bones, as well as memory problems, confusion and other harmful effects.
Researchers reviewed data from Medicare claims in the US and analysed 10 years of first-time prescriptions for benzodiazepines among more than 120 000 people, ages 65 and older, who were hospitalised for ischaemic stroke. The rate of benzodiazepine prescriptions during the first three months after stroke were examined, and data were adjusted for race, sex and ethnicity. Then year-to-year prescription patterns were reviewed to identify the number of potentially excessive new benzodiazepine prescriptions given to stroke survivors.
“We reviewed stroke survivors at 90 days after a stroke because that window of time is critical for rehabilitation of motor, speech and cognitive function, as well as mental health. It’s often a very difficult time for patients who experience loss of mobility and independence. Benzodiazepines may inhibit recovery and rehabilitation,” said study co-author Julianne Brooks, MPH, a data analytics manager at the Center for Value-based Healthcare and Sciences at Massachusetts General Brigham in Boston. “For this older age group, guidelines recommend that benzodiazepine prescriptions should be avoided if possible. However, there may be cases where benzodiazepines are prescribed to be used as needed. For example, to treat breakthrough anxiety, a provider may prescribe a few pills and counsel the patient that the medication should only be used as needed. The increased risks of dependence, falls and other harmful effects should be discussed with the patient.”
The study found:
Within 90 days of stroke, 6127 (4.9%) people were started on a benzodiazepine for the first time.
Lorazepam (40%) and alprazolam (33%) were the most-prescribed benzodiazepine medications.
Three-quarters of the first-time benzodiazepine prescriptions were for a supply of over seven days, and more than half of the prescriptions were for a supply between 15 to 30 days.
Prescription rates were higher among women (5.5%) than men (3.8%).
Prescription fill rates were also higher in Hispanic adults (5.8%), though this group was limited by the small number of participants – 1.9% of the overall sample.
Overall, prescription rates were highest in the Southeast (5.1%) and lowest in the Midwest (4%) of the US. “The Southeast region is the stroke belt with a higher rate of strokes, so that could explain some differences in care in that region,” Brooks said.
There was an overall modest nationwide decline of initial prescriptions from 2013 to 2021 of 1.6%.
“We found a pattern of potential oversupply with these initial benzodiazepine prescriptions, which would be enough for patients to become long-term users or possibly addicted. The benzodiazepine prescriptions given under these circumstances may lead to dependence,” Brooks said. “Increased awareness and improved recommendations about the risks of these medications for older stroke survivors are needed.
“Although the overall prescription rate decreased slightly over 10 years, this prescription pattern is still a problem. It’s concerning because older adults are vulnerable to overprescribing and adverse outcomes. We know from previous studies that vulnerable and marginalized populations experience worse outcomes after stroke, so we want to understand the factors that may play a role so we can provide better care,” Brooks said.
The 2019 American Geriatrics Society Beers Criteria maintains a list of medications that health care professionals can reference to safely prescribe medications for adults older than 65. Beers criteria recommends avoiding benzodiazepines in all older adults due to the risk of cognitive impairment, delirium, falls, fractures and motor vehicle crashes.
“Other guidelines also suggest behavioural interventions such as cognitive behaviour therapy for insomnia, antidepressant medications for anxiety disorders and trying non-pharmaceutical interventions first,” Brooks said.
Researchers said more studies are needed to understand if there is a safe level for prescribing benzodiazepines that may be most appropriate for older adults. The main limitation was that this study used a large, national dataset that did not include information about why benzodiazepines were prescribed.
Respiratory syncytial virus (RSV) is the leading cause of hospitalisation in young children due to respiratory complications such as bronchiolitis and pneumonia. Yet little is understood about why some children develop only mild symptoms while others develop severe disease.
To better understand what happens in these cases, clinician-scientists from Brigham and Women’s Hospital, and Boston Children’s Hospital analysed samples from patients’ airways and blood, finding distinct changes in children with severe cases of RSV, including an increase in the number of natural killer (NK) cells in their airways.
The descriptive study, which focuses on understanding the underpinnings of severe disease, may help to lay groundwork for identifying new targets for future treatments. Results are published in Science Translational Medicine.
“As a physician, I help to care for children who have the most severe symptoms, and as a researcher, I’m driven to understand why they become so sick,” said corresponding author Melody G. Duvall, MD, PhD, of the Division of Pulmonary and Critical Care Medicine at Brigham and Women’s Hospital (BWH) and the Division of Critical Care Medicine at Boston Children’s Hospital. “NK cells are important first responders during viral infection – but they can also contribute to lung inflammation. Interestingly, our findings fit with data from some studies in COVID-19, which reported that patients with the most severe symptoms also had increased NK cells in their airways. Together with previous studies, our data link NK cells with serious viral illness, suggesting that these cellular pathways merit additional investigation.”
Duvall and colleagues, including lead author Roisin B. Reilly of the Division of Pulmonary and Critical Care Medicine at BWH, looked at samples from 47 children critically ill with RSV, analysing immune cells found in their airways and peripheral blood. Compared to uninfected children, those with severe illness had elevated levels of NK cells in their airways and decreased NK cells in their blood. In addition, they found that the cells themselves were altered, both in appearance and in their ability to perform their immunological function of killing diseased cells.
Duvall and co-authors have previously described a post-pandemic surge in paediatric RSV infections. While clinicians can only provide supportive care to the most severely sick children, vaccines to prevent RSV are now available for children 19 months and younger, adults 60 years and over, and people who are pregnant.
The portion of our nervous systems responsible for the “fight or flight” response can shape the severity of potentially deadly Clostridioides difficile infections, new research from the School of Medicine reveals in Cell Reports Medicine.
The findings suggest that doctors may be able to save patients from the infections – a plague for hospitals and nursing homes – by using drugs to quiet the hyperactive nervous system response, the researchers say.
“Compared to how much we know about immune system influences in C. difficile infections, the field is just scratching the surface in understanding neuronal contributions to disease,” said researcher William A. Petri Jr., MD, PhD, of UVA Health’s Division of Infectious Diseases and International Health. “Newly identifying components of the nervous system that worsen inflammation will allow us to determine potential therapeutic targets and biomarkers for patients at risk of severe disease.”
C. difficile, is a perpetual burden for healthcare facilities. Extensive antibiotic use, particularly among patients who are hospitalised or in nursing care, can allow it to establish dangerous infections. Further, patients who make it through the severe diarrhoea, nausea, fever and colitis C. difficile can cause are not necessarily in the clear: One in six will develop another C. diff infection within eight weeks, according to the federal Centers for Disease Control and Prevention.
The new UVA research reveals the critical role the nervous system plays in severe C. difficile infections. The researchers found that the “sympathetic” nervous system – the branch that responds to dangerous situations – can be a key driver of serious C. diff.
Normally, our “fight or flight” response is helpful for avoiding danger. It helps us respond quickly, improves our eyesight, boosts our strength. It also can stimulate our immune system and help us recover from injury. But in C. difficile cases, the nervous system can have a hyperactive response that becomes part of the problem, and UVA’s new research explains why.
“Neurons are the first responders that coordinate defences against toxic attacks. Sometimes those responders don’t recruit the right size and kind of artillery and that can make things worse,” said researcher David Tyus, a neuroscience graduate student at UVA. “Interestingly, the receptor we identified as important in C. difficile infection [the alpha 2 adrenergic receptor] has also been linked to irritable bowel syndrome. I’m curious to know if there could be a unifying underlying mechanism between the two disease contexts.”
Promisingly, the researchers found that targeting the receptor in lab mice reduced intestinal inflammation and decreased C. difficile severity and mortality. That suggests that, with further research, doctors may be able to take a similar tact to better treat severe C. diff infections in patients. For example, they may be able to surgically remove a portion of nerves in the gut, or they may be able to develop medicines to target the alpha 2 receptor – as Petri and Tyus are attempting to do.
“Our next step is to determine which cells with the alpha 2 receptor are receiving signals from the sympathetic nervous system and play a role in C. difficile-mediated disease,” Petri said. “We are very excited to think about how our findings translate to clinic and how the sympathetic nervous system might play a role in recurrent infection. I hope that this study sets the foundation for future findings of how neurons affect the course of C. difficile infection outcomes.”
Neurons in the brain of an Alzheimer’s patient, with plaques caused by tau proteins. Credit: NIH
Alzheimer’s disease may damage the brain in two distinct phases, based on new research funded by the National Institutes of Health (NIH) using sophisticated brain mapping tools. According to researchers who discovered this new view, the first, early phase happens slowly and silently – before people experience memory problems – harming just a few vulnerable cell types. In contrast, the second, late phase causes damage that is more widely destructive and coincides with the appearance of symptoms and the rapid accumulation of plaques, tangles, and other Alzheimer’s hallmarks.
“One of the challenges to diagnosing and treating Alzheimer’s is that much of the damage to the brain happens well before symptoms occur. The ability to detect these early changes means that, for the first time, we can see what is happening to a person’s brain during the earliest periods of the disease,” said Richard J. Hodes, MD, director, NIH National Institute on Aging. “The results fundamentally alter scientists’ understanding of how Alzheimer’s harms the brain and will guide the development of new treatments for this devastating disorder.”
Scientists analysed the brains of 84 people, and the results, published in Nature Neuroscience, suggest that damage to one type of cell, called an inhibitory neuron, during the early phase may trigger the neural circuit problems that underlie the disease. Additionally, the study confirmed previous findings about how Alzheimer’s damages the brain and identified many new changes that may happen during the disease.
Specifically, the scientists used advanced genetic analysis tools to study the cells of the middle temporal gyrus, a part of the brain that controls language, memory and vision. The gyrus has been shown to be vulnerable to many of the changes traditionally seen during Alzheimer’s. It is also a part of the brain that researchers have thoroughly mapped for control donors. By comparing control donor data with that from people who had Alzheimer’s, the scientists created a genetic and cellular timeline of what happens throughout the disease.
Traditionally, studies have suggested that the damage caused by Alzheimer’s happens in several stages characterized by increasing levels of cell death, inflammation and the accumulation of proteins in the form of plaques and tangles. In contrast, this study suggests that the disease changes the brain in two “epochs” – or phases – with many of the traditionally studied changes happening rapidly during the second phase. This coincides with the appearance of memory problems and other symptoms.
The results also suggest that the earliest changes happen gradually and “quietly” in the first phase before any symptoms appear. These changes include slow accumulation of plaques, activation of the brain’s immune system, damage to the cellular insulation that helps neurons send signals and the death of cells called somatostatin (SST) inhibitory neurons.
The last finding was surprising to the researchers. Traditionally, scientists have thought that Alzheimer’s primarily damages excitatory neurons, which send activating neural signals to other cells. Inhibitory neurons send calming signals to other cells. The paper’s authors hypothesised how loss of SST inhibitory neurons might trigger the changes to the brain’s neural circuitry that underlie the disease.
Recently, a separate NIH-funded brain mapping study by researchers at MIT found that a gene called REELIN may be associated with the vulnerability of some neurons to Alzheimer’s. It also showed that star-shaped brain cells called astrocytes may provide resilience to or resist the harm caused by the disease.
Researchers analysed brains that are part of the Seattle Alzheimer’s Disease Brain Cell Atlas, which is designed to create a highly detailed map of the brain damage that occurs during the disease. The project was led by Mariano I. Gabitto, PhD, and Kyle J. Travaglini, PhD, from the Allen Institute, Seattle. The scientists used tools – developed as part of the NIH’s BRAIN Initiative – Cell Census Network – to study more than 3.4 million brain cells from donors who died at various stages of Alzheimer’s disease.
“This research demonstrates how powerful new technologies provided by the NIH’s BRAIN Initiative are changing the way we understand diseases like Alzheimer’s. With these tools, scientists were able to detect the earliest cellular changes to the brain to create a more complete picture of what happens over the entire course of the disease,” said John Ngai, Ph.D., director of The BRAIN Initiative®. “The new knowledge provided by this study may help scientists and drug developers around the world develop diagnostics and treatments targeted to specific stages of Alzheimer’s and other dementias.”
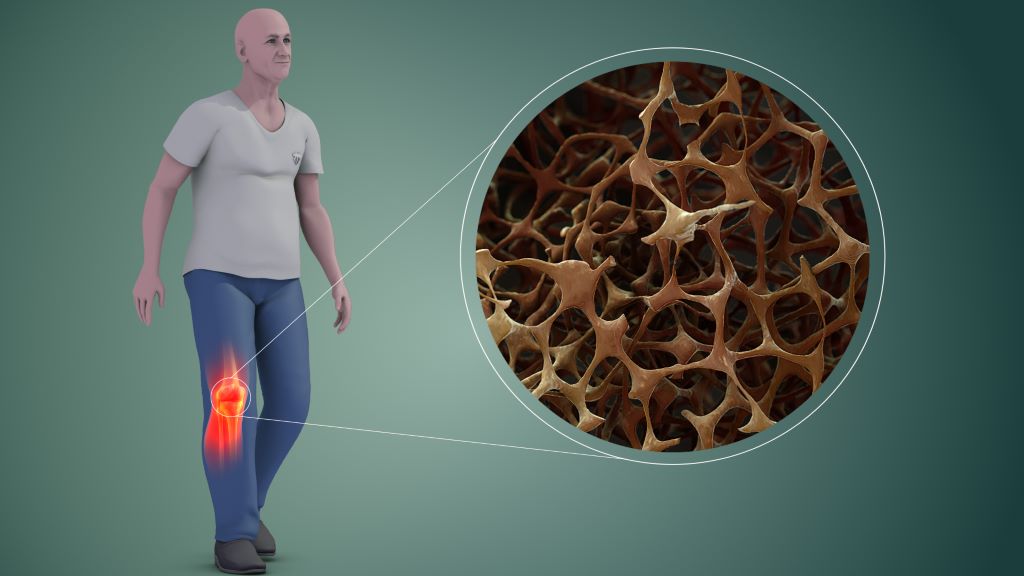
Scientists have identified a protein that blocks the activity of bone-forming cells (osteoblasts) by stopping them from maturing during the journey to sites of bone formation, finds a new study published in Communications Biology.
A team of researchers led by Dr Amy Naylor and Professor Roy Bicknell along with their team including Dr Georgiana Neag from the University of Birmingham have found that protein CLEC14A, which is found on endothelial cells in bone, block the function of bone development cells called osteoblasts.
During bone development, the endothelial cell’s job is to transport immature osteoblasts to sites where new bone is needed. However, when the protein CLEC14A is also present on the outside of the endothelial cell, osteoblasts are prevented from maturing to the point where they can form bone tissue.
This additional understanding of how blood vessel cells control bone-forming osteoblasts under normal, healthy conditions provide an avenue to develop treatments for patients who have insufficient bone formation
Dr Amy Naylor
In this study, osteoblast cells were taken from transgenic mice that either have been bred to produce CLEC14A or not. The osteoblasts were subsequently used in vitro in an induction solution, and the team found that cells taken from the protein-free mice reached maturation after 4 days while those in the presence of CLEC14A matured 8 days later. Furthermore, the CLEC14A-free samples saw a significant increase in mineralised bone tissue at day 18 in the study.
Dr Amy Naylor, Associate Professor in the School of Infection, Inflammation and Immunology at the University of Birmingham said:
“In the last decade, a specific type of blood vessel cell was identified within bones. This blood vessel is called ‘type-H’ and is responsible for guiding bone-forming osteoblasts to the places where bone growth is needed. Now we have discovered that a protein called CLEC14A can be found on the surface of type-H blood vessel cells.
“In the experiments we performed, when CLEC14A protein is present the osteoblasts that were sharing a ride on the endothelial cells produce less bone. Conversely, when the protein is removed, they produce more bone.
“This additional understanding of how blood vessel cells control bone-forming osteoblasts under normal, healthy conditions provide an avenue to develop treatments for patients who have insufficient bone formation, for example in patients with fractures that do not heal, osteoporosis or with chronic inflammatory diseases.”
Chronic pain is often caused by faulty signals emerging deep within the brain, giving false alarms about a wound that has since healed, a limb that has since been amputated, or other intricate, hard-to-explain scenarios. Effective treatment options are sorely needed; now, a new device from the University of Utah may represent a practical long-sought solution, using ultrasound to target pain centres deep inside the brain.
Researchers at the University of Utah’s John and Marcia Price College of Engineering and Spencer Fox Eccles School of Medicine have published promising findings about an experimental therapy that has given many participants relief after a single treatment session.
At the core of this research is Diadem, a new biomedical device that uses ultrasound to noninvasively stimulate deep brain regions, potentially disrupting the faulty signals that lead to chronic pain.
The Diadem Device
The findings of a recent clinical trial are published in the journal Pain. This study constitutes a translation of two previous studies, published in Nature Communications Engineering and IEEE Transactions on Biomedical Engineering, which describe the unique features and characteristics of the device.
The randomised sham-controlled study recruited 20 participants with chronic pain, who each experienced two 40-minute sessions with Diadem, receiving either real or sham ultrasound stimulation. Patients described their pain a day and a week after their sessions, with 60% of the experimental group receiving real treatment reporting a clinical meaningful reduction in symptoms at both points.
“We were not expecting such strong and immediate effects from only one treatment,” says Riis.
“The rapid onset of the pain symptom improvements as well as their sustained nature are intriguing, and open doors for applying these noninvasive treatments to the many patients who are resistant to current treatments,” Kubanek says.
Diadem’s approach is based on neuromodulation, a therapeutic technique that seeks to directly regulate the activity of certain brain circuits. Other neuromodulation approaches are based on electric currents and magnetic fields, but those methods cannot selectively reach the brain structure investigated in the researchers’ recent trial: the anterior cingulate cortex.
After an initial functional MRI scan to map the target region, the researchers adjust Diadem’s ultrasound emitters to correct for the way the waves deflect off of the skull and other brain structures. This procedure was published in Nature Communications Engineering.
The team is now preparing for a Phase 3 clinical, trial which is the final step before FDA approval to use Diadem as a treatment for the general public.
Pretoria, 16 October 2024: A group of African women leaders have come together to form the Africa Breast Cancer Council, with the support of Roche, one of the world’s largest biotech companies.
The Africa Breast Cancer Council is a response to the growing burden of breast cancer on the African continent. Breast cancer is the most commonly diagnosed cancer in women in Africa and causes the most cancer-related deaths. Only one in two women in sub-Saharan Africa are currently expected to survive for five years after receiving a diagnosis.
The Council will leverage their extensive, diverse and complementary experience to guide and drive policy change in their home countries and across the continent. They will encourage increased collaboration, better data collection and improved patient outcomes. The Council’s work will seek to foster systemic improvements in healthcare infrastructure, access, and funding, driving sustainable, scalable impact for breast cancer care. The Council will focus initially on African healthcare systems which are open to partnership and innovation, then move to scale this work across the continent.
Wendy Cupido, Africa Breast Cancer Council Co-chair and General Manager at Roche South Africa and Sub Region said: “Every woman on this Council has a day job that plays an important role in the fight against breast cancer. Our aim in coming together is to channel our knowledge, expertise, relationships and energy into a collective voice, and a collective force, to focus on significant areas of concern.”
Dr Magda Robalo, Africa Breast Cancer Council member, and President and Co-founder of the Institute for Global Health and Development said: “Most African women with breast cancer are diagnosed too late and, even after a diagnosis, many do not receive the treatment they need. This egregious injustice is utterly preventable. In response, the Africa Breast Cancer Council will work to shape policies and advocate for governments to urgently commit the resources needed.”
It can take more than six months for women in Africa to receive a breast cancer diagnosis after noticing symptoms, due in part to healthcare system inefficiencies and limited access to specialised care. This contributes to 60-70% of African women receiving a diagnosis in the late stage, reducing chances of survival and increasing cancer care costs with more expensive therapies and longer hospital stays. This is exacerbated by a lack of awareness of the importance of breast self-examinations, along with widespread stigma surrounding breast cancer treatment. In light of this need, the Council will work at a national level to reduce the time to diagnosis from six months to 60 days.
In South Africa, the average three-year survival rate for breast cancer is below 45%. This is due in part to poor uptake of early screening and detection for breast cancer, exacerbated by significant stigma, leading to late-stage diagnosis and lower survival rates. Lengthy regulatory pathways and a lack of ring-fenced budget for cancer care also present barriers to progress.
Dr Miriam Mutebi, Africa Breast Cancer Council member and Breast Cancer Surgical Oncologist said: “This Council has chosen to launch during Breast Cancer Awareness Month, a recognised annual global movement to drive awareness, early detection and improved outcomes. We are using this month to start raising our collective voice, alongside others committed to reducing the unacceptable toll of breast cancer on African women.”
Researchers at the University of Bern and Bern University Hospital have developed a test to simplify the diagnosis of allergies by testing mast cells. Its effectiveness has now been confirmed in clinical samples from children and adolescents suffering from a peanut allergy. The results, recently published in the European Journal for Allergy and Clinical Immunology (Allergy), could fundamentally improve the clinical diagnosis of allergies in future.
Food allergies are a major health problem worldwide. In some countries, up to 10% of the population is affected, mainly young children. Peanut allergy, in particular, is one of the most common diseases and often manifests itself in severe, potentially life-threatening reactions. The stress of food allergies not only affects the individuals concerned, but also has far-reaching consequences for their families, the health system and the food industry. The oral food challenge test, in which people consume the allergen (such as peanut extract) under supervision to test the allergic reaction, is still considered the gold standard in diagnosis. However, the method is complex and carries health risks. The allergen skin prick test and blood test are often not very accurate, which can lead to misdiagnoses and unnecessary food avoidance.
A team of researchers led by Prof Dr Alexander Eggel and Prof Dr Thomas Kaufmann from the University of Bern, developed an alternative test in 2022. It mimics the allergic reaction in a test tube and thus offers an attractive alternative to standard tests. The Bern researchers have now investigated the effectiveness of the test on samples from children and adolescents with confirmed peanut allergy and a healthy control group in a clinical study in collaboration with partners from the Hospital for Sick Kids in Toronto, Canada. They were able to show that the new test has a higher diagnostic accuracy than the methods used so far.
Mast cell activation test as appropriate alternative
“The most common food allergies are type I allergies. They develop when the body produces immunoglobulin E (IgE) antibodies in response to substances that are actually harmless (allergens),” explains Alexander Eggel. These antibodies bind to specific receptors on the mast cells, which are immune cells that play an important role in allergic reactions and inflammation. They are mainly located in the tissue, for example, in the intestinal mucosa, and are prepared for and sensitised to the allergen by binding to the antibodies. Upon renewed contact with the allergen, it binds directly to the mast cells loaded with antibodies, activating them and triggering an allergic reaction.
“In the Hoxb8 mast cell activation test (Hoxb8 MAT), which we developed, mast cells grown in the laboratory are brought into contact with blood serum from allergic patients. The mast cells bind the IgE antibodies from the serum and are sensitised by them. We can then stimulate the mast cells with different amounts of the allergens to be tested,” says Eggel. Quantifying the activated mast cells suggests how allergic a patient is to the allergen tested without needing to consume the food.
Higher diagnostic accuracy than standard tests
The study used serum samples from a total of 112 children and adolescents who had already participated in a study in Canada and for whom clear diagnostic data on their peanut allergy status were available. The mast cells cultured in the laboratory were sensitised with their serum and then stimulated with peanut extract. “The cell-based test was easy to carry out and worked perfectly. All samples were measured within two days, which was very fast,” says Thomas Kaufmann. The results showed that a large number of sera from allergic patients exhibited allergen dose-dependent activation, while almost all samples from the non-allergic control subjects did not activate the mast cells. “An exceptionally high diagnostic accuracy of 95% could be calculated from these data,” Eggel adds.
In addition, the data measured in the study were analysed in direct comparison with other diagnostic methods established at the hospital. It was found that the Hoxb8 MAT test had significantly higher accuracy than the standard measurement of allergen-specific IgE antibodies in the blood or the frequently used skin test. “Comparison with other clinical tests was crucial to determine which of them reflected the patients’ allergic reaction best. The new mast cell activation test has the advantage that it is functional and therefore incorporates many parameters that are important for triggering the allergy,” says Thomas Kaufmann, adding: “The new test is also based on stable blood serum, which can be drawn using simple blood sampling and then stored in the freezer. This eliminates the challenging logistical obstacles that arise with other methods.” The study also showed that the Hoxb8 MAT test leads to less false negative results.
“What has been shown in this study on the diagnosis of peanut allergies can also be applied to other allergies in a simple way. The technology is a perfect example of how basic research from the University of Bern can be brought to the clinical practice, and might ultimately simplify life for patients and physicians,” concludes Eggel.