Professor Shabir Madhi has been appointed as an honorary Commander of the Most Excellent Order of the British Empire (CBE) by King Charles III.
Wits Professor of Vaccinology Shabir Madhi led the Oxford University sponsored Oxford/AstraZeneca Covid-19 vaccine clinical trials in South Africa
Wits University and the University of Oxford contributed scientifically to informing the public health response to the Covid-19 pandemic in South Africa and globally.
Madhi receives the Order in recognition of his services to science and public health in a global pandemic.
Madhi led South Africa and the continent’s first Covid-19 vaccine trials in 2020/2021 as founder and Director of the South African Medical Research Council (SAMRC) Wits Vaccines and Infectious Diseases Analytics (Wits VIDA) Research Unit.
An internationally recognised leader in his field, the National Research Foundation A-rated scientist was involved in multiple clinical and serology epidemiology studies on Covid-19, in addition to his research on vaccines against other life-threatening diseases.
The first of (subsequently two) Wits University-led South African Covid-19 vaccine trials, Madhi led the Oxford/AstraZeneca Covid-19 vaccine clinical trials in South Africa, in association with the University of Oxford.
Professor Sir Andrew Pollard, Director of the Oxford Vaccine Group, University of Oxford, and Madhi’s UK counterpart in these Covid-19 vaccine trials, says of Madhi’s CBE appointment: “I am delighted that Professor Shabir Madhi CBE has been honoured by King Charles for his remarkable contributions to global public health and particularly for his extraordinary leadership in the midst of a global pandemic. It has been a huge privilege for me to work alongside him and his team on the development of the globally impactful Oxford-AstraZeneca vaccine.”
Over the course of the pandemic (2020-2022), Madhi had been an outspoken, articulate, and ardent advocate of Covid-19 vaccination as well as for increased access to these and other vaccines in Africa.
On his appointment as CBE, Madhi says: “The privilege of being conferred this honour is credit to the tremendous effort of the incredible Wits VIDA research team that I have the privilege of leading at Wits University – before, during and beyond the Covid-19 pandemic. As a collective, and together with colleagues at the University of Oxford and in South Africa, we are proud to have contributed scientifically to informing the public health response to the Covid-19 pandemic in South Africa and globally.”
Mediaeval tyrant and inspiration for vampires, protein analysis reveals health secrets about Vlad the Impaler
New research analysing ancient protein residues left in letters written by the sadistic 15th century tyrant – and vampire inspiration – Vlad Dracula the Impaler suggests that he suffered from a number of health conditions. One of these conditions seemingly confirms one of the more outlandish tales about him – that he cried tears of blood.
Vlad the Impaler got his nickname because he impaled thousands of people on stakes: enemies (mainly the Ottoman Empire), criminals and anyone suspected of conspiring against his rule. He was eventually defeated in 1460, but the newly invented printing press spread the tale of his gruesome deeds all over Europe. Tales surrounding him may have inspired the iconic character of Bram Stoker’s Count Dracula in 1897. Nevertheless, more modern vampire stories such as Netflix’s ‘Castlevania’ make use of Vlad as inspiration.
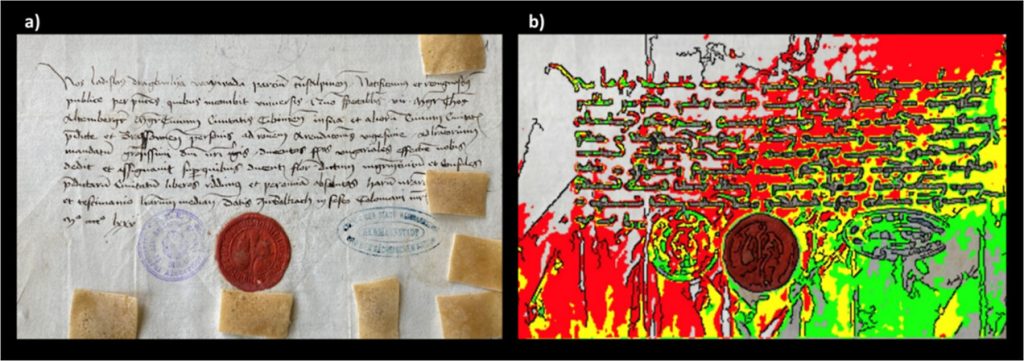
This terrifying reputation made him an interesting topic for a bit of genetic archaeology in a paper published in Analytical Chemistry. Using sophisticated proteomic techniques, scientists analysed three letters written in 1457 and 1475 by the voivode of Wallachia, Vlad III, also known as Vlad the Impaler, or Vlad Dracula. This allowed them to tease out information about the man who wrote the letters as well as general information about the environmental conditions of 15th century Wallachia, a place of regional trade and conflict as well as disease transmission.
While centuries-old paper is unlikely to hold entire DNA strands, scientists were still able to piece together genetic information about the writer. The technique depends on the notion that a person’s writing hand will tend to rest on the paper being written upon, rubbing off a surprising amount of organic molecules in the process. They applied ethylene vinyl acetate to the papers, and with mass spectrometry, they discovered over 500 peptides – short chains of amino acids – with about 100 being of human origin, which they looked up in database searches.
Figure 1. (a) First letter (archive catalog number is II 365), dated August 4, 1475, here investigated, also showing the positions of the EVA strips (brownish rectangles) applied to its surface for capturing biological material; (b) mapping of the fluorescence of phenylalanine, tyrosine, and tryptophan under flash UV illumination (see the original article). Anal. Chem. 2023, 95, 34, 12732-12744
The researchers noted that while many mediaeval people may have handled these papers, it is also presumable that the most prominent ancient proteins can be attributed to the one who wrote and signed them – Prince Vlad the Impaler.
First, they discovered proteins pointing to ciliopathy, which affects the cellular cilia or the cilia anchoring structures, the basal bodies or ciliary function. This can manifest in a wide range of disorders, ranging from cerebral malformation to liver disease and intellectual disability.
They also uncovered signs of an undetermined inflammatory disease which likely involved his skin and respiratory tract.
Proteomics data also suggests that, according to some stories, he might also have suffered from a pathological condition called haemolacria – he could shed tears admixed with blood. This appears to confirm what some stories said about Vlad – that he sometimes cried tears of blood. While it is a known medical condition, it would have no doubt been terrifying for superstitious mediaeval people to behold when seen in someone with a reputation like Vlad the Impaler’s.
Non-human peptides also proved to be a window into the conditions of the time, hinting at common foods, pests and diseases. Database searches of the identified, as potential endogenous original components, 3 proteins from bacteria, 24 from viruses, 4 from fungi, 17 from insects (suggesting fruit flies), and 5 from plants (including rice, wheat and thale cress). Of the bacteria, they noted that some peptides related to Enterobacterales are specific to Yersinia pestis, the pathogenic bacterium causing plague, whereas another group is specific to E. coli.
Dr Imtiaz Sooliman, founder of The Gift of the Givers Foundation, has appealed for negotiations, compromise and peace in the Middle East. The respected South African aid organisation has had a presence in Gaza for nine years.
Gift of the Givers doesn’t have an office in Gaza. Instead, the team of three people moves around distributing medical supplies, food and water. They are also involved in a women and child care centre, a health facility, and schools.
Sooliman says the organisation wants to send more people. “We are preparing to send medical teams but only if it’s not any risk to them.” He says a ceasefire or safe corridor is needed before the teams can enter Gaza. The organisation has 40 medical personnel ready to go in, Sooliman told GroundUp.
On Sunday Gift of the Givers reported that the team has been under severe physical and mental stress.
In 2014 Israel attacked Gaza for seven weeks. Sooliman said his team is reporting that this time it’s completely different. “They said it’s so difficult to move around. There’s so much anxiety and so much fear. The amount of bombs being dropped has never happened before.”
On Tuesday the UN High Commissioner for Human Rights said that 4200 people have been killed, and over one million people displaced, in just ten days, while large areas of the Gaza strip have been reduced to rubble.
The death toll includes a large number of women and children, as well as at least 11 Palestinian journalists, 28 medical staff and 14 UN workers. It also includes over 1300 Israelis, mostly civilians, killed by Hamas on 7 October.
Sooliman said that Gaza’s people face challenges with access to food and water. “Because there’s no electricity, the sewage plants don’t work. Because they can’t do burials, the decomposed bodies are going to cause infections. Because hospitals don’t have antibiotics, there’s a threat of infection there.
“They managed to do some mass funerals yesterday. As the bodies are coming in they are doing it straight away. There are thousands of bodies lying under the rubble that they can’t reach. They don’t have the equipment, they don’t have the personnel, but above all, it’s bloody dangerous to get there,” said Sooliman.
Sooliman said that he had a meeting with the Egyptian ambassador and South Africa’s Foreign Affairs Department on Monday in an attempt to get a humanitarian aid corridor open. “We are also looking at flying supplies on a cargo plane from South Africa and sending trucks to the border in Cairo.”
Asked how this situation compared to other humanitarian relief efforts the organisation had been involved in, Sooliman responded: “This is the worst situation in the world because there is no exit route. You can’t get out. The area is so small. It’s so easy to bomb it … Nobody can have a safety plan. Where are you going to hide? There’s no such thing as safety in Gaza.”
Gaza is only 350km2. It could fit into Cape Town nearly seven times, yet it has half Cape Town’s population.
Sooliman described Israel’s call to evacuate more than one million people from the north to the south of Gaza as “quite ludicrous”. “How can you move 1 million people in 24 hours when there’s no fuel and no cars? Where are you going to go to? Everything is bombed. How do you move an intensive care unit patient?”
He also called for restraint from both sides. “Civilians cannot be attacked in a war and that applies to both sides … At the end of the day, both sides must remember that there is no winner in war. Everybody loses out. The only way to solve this problem in the Middle East is to make peace, act rationally and make compromises.”
“This is not a thing about Jews against Muslims; it’s human against human. It’s not a religious thing, it’s a human thing … it’s about humanity. It’s in the interests of all parties to make compromises. The only way to solve the problem is to do what is just,” he stressed.
“When you act justly you will have peace, prosperity and peace in the entire region. Nobody loses out. Actually everybody gains more. They should go to the negotiating table, make compromises and give a just solution. If you do that then we never have to send any more supplies to the Middle East again,“ Sooliman added.
Dr Bukiwe Spondo recently received the Rural Doctor of the Year award at the Rural Health Conference held in Chintsa in the Eastern Cape. PHOTO: Supplied
By Biénne Huisman for Spotlight
Describing the rutted gravel road between Butterworth and Tafalofefe District Hospital in the Eastern Cape, Dr Bukiwe Spondo uses the word “terrible” at least eighteen times. Dipping through the Amatole District, the 55-kilometre journey can take several hours. With heavy rain, tractors may be required to dislodge ambulances and often even staff have difficulty getting to work because of the mud.
Since 2007, Spondo and her colleagues have offered a multitude of services at Tafalofefe in the lush but impoverished Centane village. First off, she moved the hospital’s ARV clinic from an out-building to inside the premises – reducing stigma – “because if patients went into that building on the outside, automatically everyone knew,” she says.
In 2012, having observed how patients stopped taking treatment due to travel costs, she started driving up to 40 kilometres a day twice weekly to nine clinics in the area, where up to fifty patients would be queuing to see her. To make life easier for patients, she started pre-packing medication to take to them at the clinics. Later she opened a CHAMP (Clinical HIV /AIDS Management Programme) site at Tafalofefe to see complicated cases referred from the clinics, and a multi-drug-resistant TB (MDR-TB) review clinic in conjunction with Butterworth Provincial Hospital.
“As a rural doctor, you become a social worker, a pharmacist, a priest – you do everything,” she says, laughing.
Rural doctor of the year
Spondo’s efforts have not gone unnoticed. Last month at the Rural Doctor’s Association of South Africa (RuDASA’s) annual Rural Health Conference, she received the Rural Doctor of the Year award. RuDASA chairperson Dr Lungile Hobe conferred the award at the event hosted near Chintsa. Spondo is quick to point out that she also won an Amatole District leadership award last year.
Speaking to Spotlight over Zoom, she says, “So the roads here at Centane are terrible. It becomes a challenge to get ambulances through and the chopper cannot fly either when it’s raining. I mean, the other day a truck was stuck, crossing the road so the ambulance couldn’t pass. We had to take a private car from the hospital to go meet the ambulance halfway.”
She adds that the community hoped that roads would be improved after a devastating accident five kilometres from Tafalofefe in 2020 when an overloaded 65-seater bus plunged into a gorge, causing 25 deaths and 62 injuries. But, she says, the improvements never come.
At Tafalofefe, the two nearest referral hospitals are Cecilia Makiwane and Frere Provincial in East London, situated an additional 110 kilometres or 90-minute drive from Butterworth along the N2 highway. Housed in a pale building, Tafalofefe has 160 beds served by 41 professional nurses and seven doctors – including three community service doctors who joined last year. The additions have increased capacity, for example, emergency caesareans are now available around the clock.
Taking healthcare to the people
The hospital has three 4×4 bakkies [pick-ups] for visiting or transporting patients. It is in one of these that Spondo travels to see patients in remote corners between the Kobonqaba and Kei Rivers on Tuesdays and Thursdays.
“Clinics are part of decentralised primary healthcare goals,” she says. “But the problem was that if there were complicated cases – like if a patient is taking ARVs and then develop side effects, the sisters are not equipped to handle that. For example, if there is a kidney problem, they [cannot] do anything about that.
“And in time, I realised that for these people traveling to the hospital costs too much money. Let’s say, for example, the clinic at Qolora – for a person to travel from Qolora to Tafalofefe is R100. A return ticket is R200. And you know, most people here are unemployed. They can’t afford this. By the time they have saved up enough money to travel to the hospital, it’s too late. Like it would be the end stage of their kidney problem. You could not send this patient for dialysis, nothing could be done to help them. This is why I started my outreach trips.”
In motivating for Spondo to receive the RuDASA award, Tafalofefe’s CEO Masizakhe Madlebe pointed out how her work days start at 7am, only finishing once all patients had been seen, whether at the hospital or at one of the local clinics. In addition, he notes how, over the years, Spondo has mentored youth in the area, including children whose parents had succumbed to AIDS, and school girls on topics like life goals and contraceptives. He adds that Spondo even reached into her own pocket to pay school fees for children without parents.
Spondo relays how she noticed girls as young as twelve years old in their maternity ward, giving birth. “Myself and some nurses we went to two schools in the area to educate them, to discuss goals and contraceptives,” she says. “We started with grade 12 pupils. No teachers were present. It was just us and them. And I was surprised at how free they were talking. I said to them education is more important. I said to them – You see me? I am a doctor. One day you can be a doctor too, but you need to be educated. I told them they could come to Tafalofefe any time if they needed to talk, that I could help them apply for tertiary degrees, to college or to university.”
Spondo has kept a close eye on children orphaned by AIDS in the area. “I tell them to bring me their June, September, and December school reports, so I can see how they’re doing, so I can motivate them,” she says.
“These kids, I’ve seen them grow up. Some of them I saw angry – with everyone, with their own deceased parents. And I explained to them, don’t be angry. It’s not your mother’s fault. It’s not your father’s fault. It was the government’s fault for not giving your parents access to ARVs. But now, take your own ARVs and you will be fine. Some of them have passed high school with distinction, some even now have access to universities.”
Bringing her skills back home
Alongside two brothers whom she describes as “wonderful”, Spondo grew up in the village of Nqamakwe, on the opposite side of Butterworth. Her parents have passed away, but she still considers Nqamakwe her home. Here her family’s farming interests include cattle, goats, and sheep.
She attended Blythswood Secondary School in Nqamakwe – excelling at biology and physics, even though maths was hard work. “Becoming a doctor was just something I always wanted,” she says, relaying how in her formative years she had been a sickly child who often required medical care. This changed, she says, as she cannot remember ever being sick as an adult.
Spondo graduated from medical school at the University of KwaZulu-Natal in 2002, completing her internship at Cecilia Makiwane and her community service at Tafalofefe and Frere in 2004.
Speaking with rapid enthusiasm, she says how happy she is to bring her healthcare skills back home to serve the community that shaped her own humanity.
“I mean, I know these people inside out. I was born in front of them, raised in front of them,” she says. “These are our relatives, our aunts, our grannies. It’s giving back to them, to the community that raised you, that has done everything for you. Who supported you through all these years.”
She adds that Tafalofefe’s clinical manager, Sambona Ntamo, grew up near Butterworth too.
“Who would look after these people if we didn’t?” she asks.
Where does she find the resilience that drives her passion to care for sick people, often queuing at the end of long rutted roads?
“Lots of exercise,” she says, smiling.
At Tafalofefe there is a staff gym with a treadmill, a bicycle, weight lifts, and pilates balls.
“I tell the guys after work it’s gym time, it’s gym time, it’s gym time!” she says. “We’ve got a key and everyone knows that even if they want to go to the gym after midnight, they may get the key and go.”
Photographs capture an air of camaraderie at Tafalofefe. Staff sharing a meal of tripe and creamed spinach on heritage day, a farewell gathering for a retiring nurse with balloons and huge gifts in silver wrapping, [and] women knitting countless bright beanies for babies delivered in the maternity ward. A picture inside the hospital’s paediatric room shows youngsters on plastic motorbikes and mothers holding toddlers wrapped in blankets.
Spondo and her own eight-year-old son, Lutho desperately – which means the greatest one – live in a doctor’s house on the hospital’s premises. They travel to their family home in Nqamakwe over weekends.
For Spondo, being a doctor does not feel like a job. “When you do something you love, it doesn’t feel like a job,” she says. “Being a doctor is something I look forward to every morning. When patients return to me, saying they feel better with a smile on their faces, saying thank you for the treatment – that just makes my day.”
Last month, she won the Mandela Rhodes Foundation’s award for social impact in Africa for a device that can help save the lives of women who suffer excessive bleeding after child birth. PHOTO: Nasief Manie/Spotlight
By Biénne Huisman for Spotlight
As a child growing up in the Ugandan capital of Kampala, Maureen Etuket used a screwdriver to dismantle electronic appliances and toy trucks. “I was around eight, nine years old,” she says. “I guess it just excited me.”
Slightly over a decade later, this curiosity is driving her quest to find solutions to public healthcare challenges.
Last month, Etuket’s Smart PVD device [Postpartum Haemorrhage Volumetric Drape] won the Mandela Rhodes Foundation’s award for social impact in Africa – the 2023 Äänit Prize – with a cash grant of $38 000. At the awards ceremony in Cape Town, judges described the device as “a brilliantly practical intervention that can immediately and directly improve outcomes for patients”.
Inside the Anatomy Building on the University of Cape Town (UCT)’s Health Sciences campus, Etuket explains that she and her team devised a prototype after spending three months in maternity wards at Kawempe National Referral Hospital in Kampala.
“We went almost every day. We had day shifts and night shifts,” she recalls. “I started asking the question to nurses and midwives, how do you know that a woman is likely to get to PPH?” PPH or post-partum haemorrhage is excessive bleeding after a baby’s birth, which could cause a severe drop in blood pressure leading to shock and death if not treated.
“Like, how do you tell? What criteria do you use? And the nurses told me that they had been doing this for a long time. They said they just observe and know. And I thought to myself, if that was working, we would have [fewer] women dying from PPH.”
How does the Smart PVD device work?
“There’s something already on the market – an under-buttock drape bag attached to the bed while a woman is giving birth, which measures amount of blood loss,” says Etuket. “[It’s] basically a bag where the blood flows into. We then created an electronic module that has a probe and a buzzer, which we put inside this bag, and it gives a beeping sound when the blood has reached a certain level. This alarm alerts a midwife to recognise the need to attend to a particular case. So the blood collection module is disposable. And the electronic module, which has the probe and the buzzer, is reusable.”
Etuket declines to share pictures, citing intellectual property rights.
“I really think that this is one of the simplest innovations,” she says. “We’ve been pitching it and talking about it, and everyone that listens is just like it’s common sense, right?” Apart from the Äänit Prize, they have received $16 000 from the Makerere University’s research and innovations fund and $55 000 from the science and technology secretariat in Uganda.
Moving to Cape Town
Etuket moved to Cape Town in 2021, courtesy of a Mandela Rhodes Foundation scholarship. “I applied for a Masters in health innovation at UCT under the Mandela Rhodes Foundation. So, I’m Christian. I believe in the hand of God in everything I do. I made just that one application. Like, there were options to put three universities, three courses, all that. I just wanted health innovation at UCT, and I got it.”
Her Masters supervisor was Professor Sudesh Sivarasu, internationally renowned for medical device innovation and head of UCT’s MedTech laboratory.
“There were so many questions we had at Pumzi Devices about how to transition an innovation to the market and no one really had the answers because it’s a new space. At a certain point, some of us had to travel to Scotland just to sit with experts to guide us through a protocol design process. No one in Uganda really had a clear picture of [this] so that’s what prompted me to do the Masters in health innovation,” says Etuket.
Find your purpose
Presently, she is pursuing a PhD in industrial engineering at Stellenbosch University under the supervision of Professor Sara Grobbelaar and Dr Faatiema Salie. Yet she spends most of her time at UCT, where Sivarasu is her external co-supervisor. Etuket’s PhD’s working title is “Exploring the development of a localisation roadmap for medical devices in South Africa using an Innovation Systems Framework”. She explains that this line of study – systems engineering – is drawing her thinking wider to understand the systems around biomedical design and innovation.
Going forward, Etuket will continue to lecture students back home in Uganda – online – while being open to further her learning and practice where it is apt or required around the world.
At 28 years old, Etuket’s drive and achievements make her a role model for many. However, she is reluctant to wear the label of “a pioneering young black woman,” voicing caution over mantels based on race and gender. “I notice that when we start to have those mindsets, we may end up trampling on people, on men. We have to work together. There is room for all of us,” she says.
The first born of four siblings, Etuket’s father was a computer engineer and her mother an accountant and businesswoman. Elaborating on leadership, she says, “I think it’s important to pray for people. That’s where we get guidance on how to lead. I tell people, not everyone should do a PhD, maybe not everyone should do a Masters, but find your purpose and fulfil it.”
Professor Valerie Mizrahi, a world-leading tuberculosis researcher and director of the Institute of Infectious Disease and Molecular Medicine at the University of Cape Town, is retiring at the end of the year. PHOTO: Nasief Manie/Spotlight
World-leading tuberculosis researcher Professor Valerie Mizrahi was 35 when her mother Etty started losing weight and coughing furiously. After healthcare professionals in Johannesburg failed to accurately diagnose her, it was a doctor in Plettenberg Bay who told Etty: “The good news is you don’t have lung cancer, the bad news is that you have tuberculosis (TB).”
At the time, Mizrahi’s two infant daughters – aged one and three years old – had been spending much time with their granny. And so Mizrahi found herself crushing TB prevention tablets into her children’s porridge with honey.
Etty was treated at the then-Rietfontein Hospital, the precursor to Sizwe Tropical Diseases Hospital in Johannesburg. “My mom got very ill,” recalls Mizrahi. “She almost died of TB. And then 10 years later, she had to have a lobe from one of her lungs removed because she was one of those unfortunate people who got post-TB fibrosis.”
This was the early 1990s. Mizrahi was then with the South African Institute for Medical Research (SAIMR) linked to the University of the Witwatersrand, where she established the Molecular Biology Unit. She had identified TB as a lurking problem in South Africa, particularly in mines and in hospitals, calling it “a worthy foe ripe with opportunity for scientific investigation” – a problem she felt not enough people were talking about. It had been a pivotal moment when TB entered her own home, one that she says galvanised her thinking.
“It was a dramatic eye-opener for me as a basic scientist,” she says. “It was traumatic because of the time it happened in my career. Our family suddenly being thrust into the world of TB control. We had all these questions like we didn’t know where my mum got it, was her TB drug-susceptible, and why it would take so long to find this out. I got to see first-hand how difficult it was to get answers…”
Born in 1958 to Etty and Morris in Harare, Zimbabwe, Mizrahi studied at the University of Cape Town (UCT), forging an unusual career path, veering from mathematics and chemistry to biochemistry, genetics, and microbiology. In a male-dominated field, she became one of the first in South Africa to interrogate TB at a basic science level – that is to say, research aimed at advancing our understanding of the basic science of how TB bacteria survive, replicate, and resist attempts to kill it.
‘the only good TB bacillus is a dead one’
Discussing TB, Mizrahi’s passion is effervescent, her every second sentence punctuated with “okay”. These underscore her statements – subtle pauses allowing for her preceding words to sink in.
Source: CC0
…there’s a reason why TB has persisted for so long. The bacillus is pretty hard to kill. It’s built like Fort Knox.
Prof Valerie Mizrahi
A particular interest for Mizrahi is developing antibiotics “that can kill this bacterium stone cold dead”.
“To me, the only good TB bacillus is a dead one,” she says. “But there’s a reason why TB has persisted for so long. The bacillus is pretty hard to kill. It’s built like Fort Knox. So it’s a monumental challenge. We don’t know where all the bacteria are residing. We know that TB in an infected lung is sitting in really difficult places, hard places for drugs to get to. This notion of going after the bacillus with drugs and just slamming it is a tough problem. Not insurmountable, but there’s a lot of research that needs to be done.”
TB can be cured, but treatment typically takes at least six months and involves taking at least four different antibiotics, with side effects ranging from minor to serious. In addition to research on new antibiotics, there are also several experimental TB vaccines currently in late-phase studies. The only TB vaccine we have was developed more than a century ago and only has some moderate efficacy in kids.
The IDM
Since 2011 Mizrahi has served as director of the Institute of Infectious Disease and Molecular Medicine (IDM) – the University of Cape Town’s (UCT) largest cross-faculty research unit with over 800 affiliated staff and grants running into hundreds of millions of rands.
Mizrahi’s glass-encased office looks directly onto Table Mountain and hospital bend – where, at the time of our interview, N2 traffic out of Cape Town is already at a standstill. Behind her desk, Mizrahi quips. “Yes, this is the most beautiful office at UCT, everyone agrees…” Below, students can be seen milling about on the health sciences campus.
Last year in its Best Global Universities 2022-2023 survey, online portal US News ranked UCT as 24th best university in the world for studying infectious diseases. Mizrahi is ambivalent about the IDM taking credit for this accolade. She notes that this success is founded on problems of a “confounding and overwhelming” scope, with many diseases being proxies for poverty and inequality in South Africa.
The IDM’s focus includes TB, HIV/AIDS, COVID-19, other infectious diseases like sexually transmitted infections, and non-communicable diseases such as preventable cancers, cardiovascular, and psychiatric disorders.
Reflecting on the IDM, she says they have accrued a “research ecosystem – a concentration of expertise, something resembling critical mass” – bringing together specialists across the basic, clinical, and public health sciences, in one place.
“We’ve got Groote Schuur Hospital across the road,” she says. “We have geneticists and biochemists, virologists, and immunologists. There’s a clinician across the corridor from me, bioinformaticians, and microscopists downstairs. If you are the kind of researcher who revels in asking questions and finding people who can answer them, then this is the place for you.”
Going forward, multi-disciplinary research is what excites her. “HIV and TB have been so dominant in the narrative of this country. But now when you look at the figures and the data, we are dealing with a huge burden of non-communicable disease on top of infectious diseases,” she says. “The key question moving forward is how not to think in silos.”
Polymaths and dilettantes
This, she says, takes humility.
“To do this, one has to be very humble. You need to know what you don’t know. People who work really well in interdisciplinary spaces are those who understand the limits of their own specialist knowledge, and the need to listen to where another person is coming from.”
She distinguishes between polymaths and dilettantes. “You have to be careful not to be a dilettante, who knows a little about a lot. Research can be very superficial in that way. So I have my antenna out all the time to distinguish between polymaths, who really are people who know a lot about a lot, and dilettantes who know a little about a lot. And well, in this institute we have a lot of polymaths, brilliant researchers who move across disciplines, very interesting people to work with.”
With a string of awards and an A1-rating from South Africa’s National Research Foundation, earlier this year, Mizrahi was elected a fellow of the Royal Society, the United Kingdom’s National Academy of Sciences. However, she recalls humbling moments along the way – like the time she flew to London seven months pregnant with her second child, for her first-ever interview with the Wellcome Trust committee to secure funding. “I was so confident, but I was ill-prepared,” she says. “They savaged me! I tried to frame it not as a failure but as a learning experience.”
Passing the baton
At the end of this year, Mizrahi will pass on the baton when she retires. Of her achievements, she is proudest of young scholars she has helped to shape. “Their legacies will last much longer than a few more citations of a publication,” she says.
Mizrahi notes more and more women leaders in her field. For example, recently, while delivering a talk at the Weizmann Institute in Israel, she noticed chemist and Nobel laureate Ada Yonath in the room. “Talk about a role model; I was almost in tears.”
Studying at UCT, Mizrahi’s own mentors had mostly been men – something she didn’t even notice, she says, as male professors treated her no different. What did cut her was racial segregation at the time, prompting a political awakening and stints leaving South Africa to work in the United States. First as a postdoctoral fellow at Pennsylvania State University and then at drug company, SmithKline & French in Philadelphia.
Her own background makes her sensitive to marginalised groups, she says. Her grandparents were Sephardi Jews who fled Rhodes Island, today part of Greece, ten years before World War II, to find refuge in Zimbabwe.
Having just read former UCT vice-chancellor Max Price’s book Statues and Storms: Leading a University Through Change, she says, “It took me back to some very difficult times. It’s harrowing and brave and made me realise that even though I was here in the midst of it [#feesmustfall and #rhodesmustfall protests], a senior person of the university, how little I really knew of what was going on. It really is a lesson in crisis leadership.”
There’s no control experiment to life, you can’t go back and redo it.
Mizrahi lives in Sea Point with her one daughter. Her other daughter is based in Vancouver. Here, she likes to park her car at the end of the week, walking around – “either listening to a New York Times podcast or a beautiful piece of music and that’s when I think.”
She describes herself as an introvert who needs personal time to stay sane. She is deeply thoughtful about her roots, wondering about a sense of belonging. “As white people in Africa, I think this is part of the reckoning we go through. I truly identify as being African. Arriving at Johannesburg, just breathing in the air, it feels like home.”
Looking back, Mizrahi notes her mother as a major influence in her life. “Not a highly educated woman. But the wisest, smartest person I know.” Etty still lives in Johannesburg while Morris has passed away. To this day, Etty thinks of herself as a proud TB survivor, says Mizrahi.
On her retirement, the scholar says, “Now it’s about opening up opportunities for others, writing a few papers, and contributing to the TB drug discovery space.”
“I’ve done the best I can,” she says, “I don’t believe in having regrets… There’s no control experiment to life, you can’t go back and redo it. But I don’t know that I could have done it any differently.”
Fifth-year Bachelor of Medicine and Surgery (MBChB) student Moses Malebana’s stellar academic record has paved the way for a special international elective at the University of Graz – making him the maiden recipient of this golden opportunity – and galvanising ties between the University of Cape Town’s (UCT) Department of Medicine and the Medical University of Graz (Med Uni Graz) in Austria.
Malebana will depart in November and return to UCT’s Faculty of Health Sciences in January 2024. And with just a few short weeks before he boards his flight, he said he is excited for what awaits, and plans to absorb every detail of the experience.
“I plan on becoming a giant sponge while there. I am excited and feel privileged that I’ve been selected for this opportunity. I look forward to learning all there is to learn and flying UCT’s and the Department of Medicine’s flag[s] high at Med Uni Graz,” he said.
Tough grind
But this opportunity didn’t just fall into his lap. To be considered for the elective abroad, the application and selection criteria was clear – the candidate needed to prove an unmatched academic record. Each applicant was also tasked with supplying a motivational letter that highlighted why they felt they deserved the opportunity. It’s safe to say that Malebana passed the test with flying colours.
He said he used the motivational letter to reflect and relay personal anecdotes that focused on the sacrifices that led him to study medicine at UCT, and he enjoyed documenting his story.
“I remember seeing the email and thinking that this is my opportunity to reflect on my journey and to just tell my story. It was interesting because I don’t often reflect on things. But when I started, I realised that my whole life up to this point was about making the most of the opportunities that have come my way,” he said.
First-class motivation
In his motivation, Malebana touched on the events in his life that moulded him into the man he is today. And the list is endless – walking for more than an hour to and from school every day in rural Limpopo, contending with a lack of in-school resources, and a shortage of skilled teachers were just some of the challenges he experienced. These hurdles, he added, provided the impetus he needed to give his high school education and his medical studies his all.
“All of this taught me resilience; it motivated me to work even harder to reap the rewards later in life. I worked very hard to get to UCT, and now that I’m here, I’m working even harder to attain success in my degree,” he said. “I don’t take any opportunities for granted. I’m humbled that I’ve been chosen to represent the faculty and the university in Austria,” he said.
As he prepares for his big trip, Malebana said he’s looking forward to understanding the Austrian health system and gaining some valuable insight into how medical doctors practice medicine in that country and how it compares to South Africa.
A whole new world
The elective will consist of several rotations in different areas of internal medicine and Malebana will be based at a teaching hospital affiliated to Med Uni Graz. He said he is most excited about his oncology rotations after developing a keen interest in this area of medicine.
“I have always enjoyed studying and learning more about the management of different cancers. So, I really look forward to seeing how things are done in Austria. I know each day will be filled with something new to learn, whether it’s in oncology or a different area of medicine. I’m eager to get going,” he said.
But over and above the work, Malebana said he is thrilled to have the opportunity to travel outside of South Africa’s borders for the first time, to experience diverse cultures and cuisines, gain insight into a new way of life, and build new, lasting friendships.
“It’s going to be an adventure, that’s for sure – one that I’ve already embraced with my arms wide open. I’m grateful that it has come my way,” he said.
Graduates and third year students are encouraged to apply for the new Postgraduate Diploma to drive business ownership and job creation.
The University of the Witwatersrand (Wits) announced its Postgraduate Diploma in Innovation and Entrepreneurship. The diploma aims for graduates and third-year students in engineering, science, and health sciences to become catalysts for business ownership and job creation. Apply for the PG Dip in Innovation and Entrepreneurship before 30 November 2023.
Professor Christo Doherty, the course coordinator says: “We particularly encourage candidates who are contemplating pursuing a Master’s or PhD in any of these fields, so they can embark on advanced degrees armed with the knowledge of how to commercialise their research. Graduates of this programme will have a wealth of career opportunities. Equipped with the aptitude and mindset for innovation and creation, they represent the future generation of entrepreneurs and job creators. They will not merely seek jobs; they will create them.”
The programme was developed and is led by the Wits Innovation Centre, and will bridge the gap between academic research and real-world innovation. It will empower students to translate their research into tangible solutions that drive meaningful change in society. The Diploma seeks to harness the entrepreneurial spirit of young scientists and engineers to ensure that their research outcomes do not languish on dusty shelves but ignite the flames of practical application. Professor Nithaya Chetty, the Dean of the Wits Faculty of Science says: “South African universities must now give attention to both discovery research and innovation. This is a novel diploma that will combine collaborative teaching and learning to fast-track researchers into careers as innovators and entrepreneurs”.
The PGDip in Innovation and Entrepreneurship is a multi-faculty initiative characterised by a hands-on approach, with a year-long research project at its core. Students will collaborate closely with an interdisciplinary team of lecturers, gaining invaluable insights and guidance throughout their journey. The curriculum covers critical subjects such as The Fundamentals of Business for Innovators, Innovation and the Commercialization of Research, Creating Ventures for Innovators, and Applying Design Thinking to Innovation. The programme’s objective is to expedite the transformation of students’ research and ideas into commercially viable endeavours or solutions with significant societal impact.
From 2025, the programme will expand to include humanities, commerce and other faculties.
Both the Khoi and the San believed in a mythical animal, resembling a cow, whose horns were thought to have medicinal attributes. This centuries-old medicine horn contained herbal remedies used by the Khoi-san. Credit: Rodger Smith
By Zelna Booth
Traditional medicines are part of the cultural heritage of many Africans. About 80% of the African continent’s population use these medicines for healthcare.
Other reasons include affordability, accessibility, patient dissatisfaction with conventional medicine, and the common misconception that “natural” is “safe”.
The growing recognition of traditional medicine resulted in the first World Health Organization global summit on the topic, in August 2023, with the theme “Health and Wellbeing for All”.
Traditional medicines are widely used in South Africa, with up to 60% of South Africans estimated to be reliant on traditional medicine as a primary source of healthcare.
Conventional South African healthcare facilities struggle to cope with extremely high patient numbers. The failure to meet the basic standards of healthcare, with increasing morbidity and mortality rates, poses a threat to the South African economy.
In my opinion, as a qualified pharmacist and academic with a research focus on traditional medicinal plant use in South Africa, integrating traditional medicine practices into modern healthcare systems can harness centuries of indigenous knowledge, increasing treatment options and provide better healthcare.
Recognition of traditional medicine as an alternative or joint source of healthcare to that of standard, conventional medicine has proven challenging. This is due to the absence of scientific research establishing and documenting the safety and effectiveness of traditional medicines, along with the lack of regulatory controls.
What are traditional medicines?
Traditional medicine encompasses a number of healthcare practices aimed at either preventing or treating acute or chronic complaints through the application of indigenous knowledge, beliefs and approaches. It incorporates the use of plant, animal and mineral-based products. Plant-derived products form the majority of treatment regimens.
Traditional medicine practices also have a place in ritualistic activities and communicating with ancestors.
South Africa is rich in indigenous medicinal fauna and flora, with about 2000 species of plants traded for medicinal purposes. In South Africa the provinces of KwaZulu-Natal, Gauteng, Eastern Cape, Mpumalanga and Limpopo are trading “hotspots”. The harvested plants are most often sold at traditional medicine muthi markets.
Uses of medicinal plants
Medicinal plants most popularly traded in South Africa include buchu, bitter aloe, African wormwood, honeybush, devil’s claw, hoodia, African potato, fever tea, African geranium, African ginger, cancer bush, pepperbark tree, milk bush and the very commonly consumed South African beverage, rooibos tea.
The most commonly traded medicinal plants in South Africa are listed below along with their traditional uses:
Cancer bush – Respiratory tract infections; menstrual pain.
Pepperbark tree – Respiratory tract infections; sexually transmitted infections.
Milk bush – Pain; ulcers; skin conditions.
Rooibos – Inflammation; high cholesterol; high blood pressure.
There are many ways in which traditional medicine may be used. It can be a drop in the eye or the ear, a poultice applied to the skin, a boiled preparation for inhalation or a tea brewed for oral administration.
Roots, bulbs and bark are used most often, and leaves less frequently. Roots are available throughout the year. There’s also a belief that the roots have the strongest concentration of “medicine”. Harvesting of the roots, however, poses concerns about the conservation of these medicinal plants. The South African government, with the draft policy on African traditional medicine Notice 906 of 2008 outlines considerations aimed at ensuring the conservation of these plants through counteracting unsustainable harvesting practises.
Obstacles to traditional medicine use
The limited research investigating interactions posed should a patient be making use of both traditional and conventional medicine is a concern.
During the COVID-19 pandemic, many patients used traditional remedies for the prevention of infection or treatment.
Understanding which traditional medicines are being used and how, their therapeutic effects in the human body, and how they interact with conventional medicines, would help determine safety of their combined use.
Certain combinations may have advantageous interactions, increasing the efficacy or potency of the medicines and allowing for reduced dosages, thereby reducing potential toxicity. These combinations could assist in the development of new pharmaceutical formulations.
Key role players from both systems of healthcare need to be able to share information freely.
The need for policy development is key. Both conventional and traditional medicine practitioners would need to be aware of and engage with patients on all the medicines they are taking.
Understanding the whole patient
Patients often seek treatment from both conventional and traditional sources, which can lead to side effects or duplication in medications.
A comprehensive understanding of a patient’s health profile makes care easier.
This could also prevent treatment failures, promote patient safety, prevent adverse interactions and minimise risks.
A harmonious healthcare landscape would combine the strengths of both systems to provide better healthcare for all.
Zelna Booth, Pharmacist and Academic Lecturer (Pharmacy Practice Division, Department of Pharmacy and Pharmacology, University of the Witwatersrand), University of the Witwatersrand
This article is republished from The Conversation under a Creative Commons license.
Dr Mark Blaylock, medical manager at Manguzi Hospital. PHOTO: Supplied.
By Sue Segar for Spotlight
There was a time, about 20 years ago, when, at the Manguzi district hospital in Northern KwaZulu-Natal, (and, of course, at hospitals throughout South Africa too) mothers and their babies were dying of AIDS at shockingly high rates.
“We used to get these patients who were slow progressors,” Mark Blaylock, medical manager at Manguzi, tells Spotlight. “Then there were the rapid progressors – babies who were HIV-positive who would get sick very quickly. There wasn’t much we could do for them. We’d give them vitamins and Bactrim, but ultimately they died. Then we had the ones who got sick a bit later, and those were even worse because now mum has had this baby for five years and they’ve bonded, and are a little family and now they are coming in with AIDS. Obviously, a huge number of mums died too. It was heartbreaking.
“It was the pregnancies that knocked their vulnerable immune systems. We’d watch it over and over again. The mums would come in looking ok and then they’d get pregnant and just go downhill. This was in the pre-ARV era. Pregnancy was a death sentence. I think people have forgotten what it was like in those days.”
Blaylock is talking to Spotlight from Northern KwaZulu-Natal, relaying how things have changed for the better since that terrible era. “It’s quite astounding,” he says. Blaylock returned to the hospital ten years ago after having been away for four.
“I was going through the stats recently, and in those days, 40 percent of all mothers who delivered were HIV positive, and about 40 percent of those babies born to HIV- positive mothers ended up with HIV either from birth or breastfeeding. About 20 percent would pick up HIV at birth and another 20 percent would pick it up subsequently through breastfeeding.
“These days, if we have one baby who is delivered HIV-positive or who picks up HIV, we get really upset. Our six-month HIV-positive rate now for babies is less than 0.6 percent and that is a dramatic change. It makes me so happy. Unfortunately, the young girls are still positive, but at least their babies are not becoming positive.”
Blaylock puts the changes down, “purely”, to prevention of mother-to-child transmission (PMCT) using antiretroviral therapy (ART). “Remember how, at one stage, we only gave HIV treatment if a patient was below a certain CD4 count? That was changed to test-and-treat, so regardless of their CD4 count, patients will get HIV treatment which brings the viral load down dramatically,” he says. “And now we have dolutegravir (an ARV), which is the backbone of our current HIV treatment. The success is due to prevention of mother-to-child transmission (PMTC) as well as the test-and-treat policy.”
‘A mixed bag’
It’s Sunday, a day off for Blaylock, and he’s speaking from a place with the best reception near his house on the edge of the Shengeza Lake. He lives here with his wife, Liz and their 13-year-old home-schooled daughter, Una. The sound of birds in the background makes it hard to hear him on the call. “It’s peaceful. There are hippos all around and lots of birds. It’s Eskom-free, which is even better. I love it. We live with three dogs, three cats, a genet, and I can’t tell you how many snakes. It’s paradise.”
It’s taken a long time to clinch this interview, but Blaylock has finally relented and forwarded us the provincial health department’s media protocol he has to adhere to. On problems in KwaZulu-Natal’s health system, he is reticent, saying only that it’s a “mixed bag”. “There’s a lot of dead wood, but there are real areas of excellence,” he says.
His reticence is understandable.
There was a time, also about 15 years ago, amidst the noise and turmoil of the last few years of state-backed AIDS denialism, when Blaylock was going through his own personal trauma. In April 2008, whilst working as chief medical officer at Manguzi, he was suspended for throwing an official photograph of then-Health MEC Peggy Nkonyeni into a dustbin in the hospital’s foyer. He did this out of anger and frustration, after his colleague at the hospital, Colin Pfaff was charged with misconduct for sourcing funding for antiretroviral drugs for pregnant women, and for implementing dual antiretroviral therapy to save babies from HIV – because politicians were not doing so.
He was also furious about comments made by Nkonyeni, questioning the integrity of rural doctors and suggesting they were racist. The South African National AIDS Council soon after asked the Human Rights Commission to probe the ‘racial tone’ of Nkonyeni’s remarks and to curb her ‘harassment’ of Manguzi doctors.
At the time, Blaylock (and Pfaff) were hailed by many working in the health sector as heroes with a deep commitment to their patients. In a letter to the provincial health department at the time, Blaylock said he had given his “heart and soul” to the under-resourced hospital, going beyond the call of duty.
Needing a change
Blaylock was reinstated but, in December 2008, he decided to leave, saying he needed a change and because the KwaZulu-Natal Department of Health was in “absolute disarray”. He says his old colleague Pfaff went to work as a missionary doctor in Malawi.
There was more to Blaylock’s decision to leave Manguzi than just the public disagreement with Nkonyeni. In our interview, he describes those days as “a really tough decade”. “Working in paediatrics, as I did for my first couple of years at Manguzi, I couldn’t take it anymore, emotionally. I just couldn’t do it, so I taught myself surgery. That was easier, as you could fix people. We were also so broken from losing so many friends, colleagues, and patients from HIV at the time. It was definitely traumatising and emotionally exhausting, not just for me but for Liz.
“There’s no doubt most of us were burnt out,” he says. “We kind of knew it, but we pushed on anyway. We were also quite a bit wilder and younger. We’d blow off steam by recklessly taking tiny boats across the lake, in the big waves, with lots of hippos – or we’d go for runs along the beach or naked midnight swims.”
The years outside SA
After leaving Manguzi, Blaylock moved to Ghana, where he took up a position as a general doctor at ABA Hospital in Tarkwa, north-east of Accra. “The hospital was part of the national health system but contracted to a mine, so we would treat people and then try and charge the government, fairly unsuccessfully, for the treatment,” he says. “I’d always fancied the idea of Ghana. I had this fantasy about Kwame Nkrumah and it being the first country to throw off Britain in Africa – but I didn’t enjoy it as much as I’d hoped. Everywhere you went, the police were pulling you over and asking for bribes.”
A defining moment was when Blaylock says he noticed the anti-malaria medication the hospital was giving patients was “just not working”. “Our malaria patients kept coming back full of parasites. I knew there were similar drugs in South Africa which were fantastic, so there was definitely something wrong.” He says he sent a sample to South Africa for testing and realised that “they weren’t as full of the good stuff as they were meant to be”. “I handed in the report and said ‘deal with it.”
From Ghana, where he married Liz and where his daughter Una was born, the family moved to the Kansanshi Mine Hospital in Zambia where they lived on a “beautiful golf estate, surrounded by poverty”.
“It didn’t feel right at all and was quite unfulfilling work,” he recalls. “I did GP work and there was lots of babbalaria – that’s when mostly the expat wives have a hangover on a Monday morning and they think they have malaria.”
Being “medically bored” in Zambia, Blaylock returned to Newcastle in KZN with the aim of specialising in anaesthetics. He worked in Madadeni Hospital’s anaesthetics department, before getting into a registrar’s programme on the anaesthetics circuit at various hospitals in Durban.
‘Like walking back home’
Then, in 2012, his friend and colleague Etienne Immelman, then working as medical manager of Manguzi, suggested that Blaylock should “come home”. “Etienne had been at Manguzi for more than 20 years when he retired six years ago. We’d always had a friendship and a mutual loyalty. He wanted someone to take over.”
Blaylock decided that indeed, it was time. It meant losing the opportunity to specialise, but he says it “felt right”. He went back as medical officer, before becoming manager.
“When I first arrived back, we were a small team, working hard. We all had the same commitment. It gave me a sense of purpose and belonging which hasn’t left.”
Blaylock said the hospital went through a “wonderful period” with a core team of great doctors. “But I burnt them all out during COVID – we had 164 deaths, but we pulled a lot of people through and many of the doctors have moved on. We have a young team now and they are getting there, but we don’t have the broad skill range we used to have. That is common across most district hospitals nowadays.”
So, is he happy to have come full circle, back to the place that was once a source of deep distress to him? “Yes,” he says. “For me, it’s about the community. This place gives me that, as well as a sense of stability and purpose. If you go into a little shop in Manguzi, everyone knows who you are. You say hallo to each other. You shout at a taxi driver and he says, ‘Hey Mark, don’t be so naughty’. When I came back ten years ago, it was like walking back home. It’s just a nice feeling.”
He says a lot has changed in the area. “People say there’s been no development, but when I first arrived at Manguzi in 2002, we knew every car on the road. Today, the town is overwhelmed with vehicles. There’s more money around. We almost never see malnutrition anymore. A lot of government programmes are working, as much as we like to diss them.”
Taking a stand
Given the toll that taking a stand has taken on doctors like Blaylock and Pfaff, one might be forgiven for wondering whether it was all worth it.
Did it make a difference to how things turned out? “Absolutely,” says Blaylock. “There were people scattered people around South Africa at the time who were doing great things. In our part of the world, it was Victor Friedland at Mseleni Hospital and Colin Pfaff (at Manguzi) who were the big drivers, pushing for the right actions to provide the services that the HIV Clinicians Society at the time thought was the correct one and was affordable. The Western Cape had already started, so we weren’t doing anything that groundbreaking except that it hadn’t been official policy yet,” he says.
“Can you believe that when HIV treatment first came to South Africa, it was going to be done at tertiary hospitals only? Imagine the repercussions for us sending a patient to Durban – in those days the Hluhluwe road was 160 kilometres of dirt road – to go and get their HIV treatment once a month. It was not sustainable.
“The HIV (Clinicians) Society pushed hard to get it decentralised to all hospitals. Then it was just going to be done by doctors and they said we absolutely cannot do it just with doctors. It has to be a nurse-run programme. Their vision became our current system. They weren’t the only people, but they were at the forefront of it at the time.”
‘Keeping it going’
Apart from the many advances in HIV treatment, much else has changed at Manguzi over the last 15 years. Blaylock says these days the hospital’s gastro wards are empty “thanks to the rotavirus vaccine”. “We’ve also seen a turnaround in acute respiratory tract infection,” he says. “The pneumococcal conjugate vaccine has changed that dramatically. We have also seen the pushing out of Continuous Positive Pressure Airway Ventilation (CPAP) for neonatal respiratory distressed newborns to district hospitals. This is a non-invasive way of ventilating babies with immature lungs,” he says.
“Our next great hope is the HPV vaccine, which will be a groundbreaker. It’s been rolled out in the past couple of years, but we’ll only see the effects in ten years or so because cervical cancer takes a few decades to come about. The other thing I really want to get in,” he insists, “is that our therapy department (offers occupational therapy, speech and hearing, and physiotherapy) at Manguzi is astonishingly fantastic. There are a lot of good things happening,” he says. “It is so easy to sit on the things that irritate you, but it is worth trying to remember the wins.”
As with several other rural doctors Spotlight has interviewed over the years, Blaylock seems deeply committed to building on what works at Manguzi and simply getting things done. As he says, “When you’ve invested so much into a hospital, you want to keep going as much as you can.”