The South African healthcare system is currently facing a period of intense pressure. Between staffing shortages and a rise in medical legal claims, the gap between basic nursing education and the actual demands of patient care is a major concern. To improve patient safety and support our healthcare workers, we must focus on practical, hands-on experience and constant skill building.
Why nursing challenges matter in South Africa
Nursing errors are rarely the fault of one person. In South Africa, they are usually the result of a system under strain. Nurses are dealing with overcrowded wards, long shifts, and a very high number of patients with complex conditions like HIV and TB. When staff are exhausted and overworked, the risk of making a mistake increases.
These errors have a massive impact. For patients and their families, it leads to a loss of trust. For hospitals, it leads to expensive legal battles. South Africa is currently dealing with billions of Rands in medical claims, but this is money that should be spent on better equipment and hiring more people. If we want a stronger healthcare system, we must reduce the risks that lead to these errors in the first place.
Hands-on training makes the difference
Nursing education has traditionally leaned heavily on theoretical learning, but knowing the theory of a procedure is very different from doing it in a busy hospital. Practical, skills-based training is what helps a nurse transition safely from the classroom to the ward.
Donald McMillan, MD at Allmed
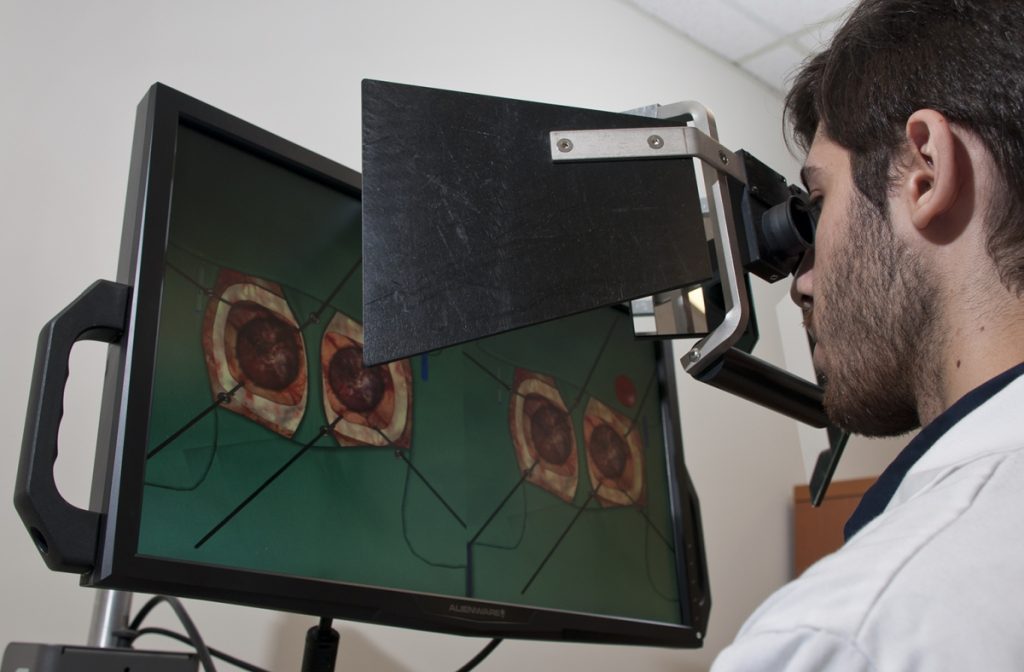
One of the most effective tools for this is simulation-based training. This involves using specialised training rooms that look like real hospital wards, complete with advanced mannequins that can mimic medical emergencies. Here, nurses can practice critical skills like inserting drips, reading ECGs, or managing emergency care in a safe environment. This allows them to build confidence and “muscle memory” before they ever treat a real patient. This type of training is essential for preparing nurses for the high-pressure reality of South African clinics.
Continuous professional development builds confidence
Medicine is always changing. New treatment guidelines, technologies, and medicines are introduced all the time, changing the way care is delivered. Continuous Professional Development (CPD) helps nurses keep pace with these changes, ensuring their skills remain relevant, their knowledge up to date, and their patients receive the best possible care throughout every stage of their careers.
However, CPD is about more than just following rules; it is about building professional confidence. When nurses have the chance to learn new things and specialise in areas like intensive care or pharmacology, they feel more capable and valued. In a country where many nurses choose to work overseas, providing these opportunities for growth at home is a great way to keep our best talent in South Africa.
A systemic approach for better care
Enhancing the quality of nursing care in South Africa requires a coordinated, multi-stakeholder approach. Training institutions, hospital administrators, and regulatory bodies must collaborate to create an ecosystem that supports the nurse at every career stage. This systemic approach should focus on three specific areas:
Integrated mentorship: Establishing formal programmes where expert clinicians provide real-time bedside teaching to new graduates.
Accredited upskilling: Providing accessible pathways for nurses to specialise in critical areas such as ICU, neonatal care, and oncology.
Technological alignment: Utilising digital tools to track competency levels and identify specific areas where additional training is required.
By making practical training and ongoing learning a priority, we do more than just prevent mistakes. We empower our nurses to be the skilled professionals they want to be. When nurses are competent and confident, they provide better care, which helps rebuild public trust and makes the South African healthcare system stronger for everyone.
As HIV, TB and other treatments are updated in our public healthcare system, it is critical that healthcare workers and counsellors stay on top of the latest developments. One innovative programme makes use of short lessons delivered over WhatsApp to provide such training.
Over her years working as an information pharmacist at the University of Cape Town’s Medicines Information Centre (MIC), Briony Chisholm noted that many health workers in rural clinics face difficulties accessing training in crucial aspects of their work.
“The lack of easy access to training was in areas where it was really needed, such as the HIV (treatment) guidelines that are constantly being updated,” says Chisholm. “It’s not enough to have training sessions when new guidelines come out; you ideally should be training all the time.”
Drug-drug interactions
At the end of 2019, government introduced new standard first-line HIV treatment that includes an antiretroviral medicine called dolutegravir. As we previously reported, by 2023 around 4.7 million people in South Africa were taking dolutegravir-based treatment.
But the introduction of a new medicine in the public healthcare system, especially at this scale, is rarely straight-forward.
“Dolutegravir is considered as a ‘wonder child’ in ARV treatment, because it provides a high barrier to resistance, is easier to take, and has far fewer side effects than older ARVs. However, it also has interactions with other key drugs, particularly those used for the treatment of TB, diabetes and some anti-epileptic medications,” she says.
Through numerous queries received on the MIC’s National HIV and TB Healthcare Worker Hotline, Chisholm and her colleagues became aware that some healthcare workers were struggling with managing drug interactions. “Some healthcare workers didn’t know about these interactions; others knew about them but not how to deal with them. For example, if a patient is on the TB drug rifampicin, but also needs to take dolutegravir, there’s a need to adjust the dose of dolutegravir. Similarly, adjustments are needed with the diabetes medicine, metformin.”
Chisholm now lives in the Eastern Cape village of Nieu Bethesda. When dolutegravir was introduced, she had just completed her part-time post-graduate Diploma in HIV and TB management through UCT and signed up for her Masters. She and a colleague had, in 2016, done a road trip to about 200 clinics in seven provinces to promote the MIC’s Hotline.
“We saw that most South African healthcare workers are dedicated and keen to learn. You hear all this terrible news about health and corruption, and then you go to these clinics which are ticking along under sometimes difficult conditions, doing amazing work. It’s inspiring!”
A key realisation was the challenges experienced by health workers at these rural clinics to access much-needed training.
“Getting nurses to a central point for training and the need for transport, accommodation and food, as well as having them absent from the clinic for anything between one and five days, is challenging. It’s expensive and involves a great deal of organising,” says Chisholm.
Doing the research
Chisholm then started conducting research on what healthcare workers know about dolutegravir-related drug interactions. Her study, published in 2022, found that about 70 percent of respondents understood that dolutegravir interacts with other drugs, but there were gaps in people’s knowledge of specific interactions and the dosing changes needed to manage those interactions.
The study found that access to guidelines and training were positively associated with knowledge of drug-drug interactions. “There was a clear indication that we needed more accessible training,” Chisholm says.
“The Department of Health offers online training through live webinars, and recordings of these, but they are often one or two hours long. Nurses in busy clinics don’t necessarily have this time to sit through training sessions.”
Testing the efficacy of short training sessions
Chisholm then designed a project to test the efficacy of short training sessions focusing on teaching one or two learning points from the national guidelines in ten to fifteen-minute live lessons using WhatsApp.
“I thought, ‘we’re in a country where not everyone has access to big computer screens, but they all have a cell phone and use WhatsApp – so let’s go as simple as we can’,” she says. “The idea was not to teach the entire set of guidelines but to pick out important parts of them and ensure that if something changes in the guidelines, you get it out to people, quickly.”
Chisholm tested the feasibility of WhatsApp-based microlearning with health workers and counsellors at 50 clinics around Nieu Bethesda. “I ran a range of short case-based lessons on WhatsApp groups and then measured the changes in knowledge and patient care, as well as other factors like uptake, feasibility and accessibility,” she explains.
She found that WhatsApp-based microlearning for healthcare workers is “effective, feasible and well received” and 98 percent of those who participated said they would take part if training sessions were held weekly throughout the year.
While using WhatsApp for medical interactions is not new, Chisholm says a structured syllabus using microlearning for short, punchy sessions is a first.
“This type of learning is equally accessible to a rural clinic as to one in central Hillbrow. We can access people wherever they are. Nobody has to spend money getting anywhere and clinical services are not disrupted. And it doesn’t matter if they’re not in the live session: when they have a moment, they can go into their WhatsApp and read back on the lesson,” she says.
Working with the department of health on 6MMD
Chisholm has been working with the National Department of Health on their Six-Month Multi-Month Dispensing (6MMD) programme. The programme allows people living with HIV who are doing well on treatment and have suppressed viral loads to get a six-month supply of ARVs in one go. This makes life considerably easier for people, since they only need to go to the clinic twice a year; whilst also reducing workloads in the clinics. The programme started in August 2025 and is still being phased in across the country.
“In the pilot phase, the Department of Health did some really good online training and they used our WhatsApp training as an add-on to the longer form training,” says Chisholm.
“We started with one group and ran an eight-week course of 15-minute lessons once a week on WhatsApp. Sessions were case-based and included which patients are eligible for 6MMD, and which patients are not,” she explains. By the end of 2025, around 2 000 healthcare workers had been reached through these sessions.
Lynne Wilkinson, a technical expert with the International AIDS Society which supports the Department of Health on 6MMD, says the microlearning is “a great way to ensure we get to all the clinicians in the country and explain how the 6MMD programme works”.
She adds: “When a new policy comes out, it takes a long time for implementation to be scaled because ground level clinicians aren’t always aware of the changes or don’t have an opportunity to engage with how to implement the changes.”
Daniel Canham, a professional nurse and facility team lead for the NGO, TB HIV Care, at Idutywa Village Community Health Centre in the Eastern Cape, says they’ve found the microlearning sessions for 6MMD very useful. “It’s no secret that the waiting times in clinics are quite extensive, so we are trying to enrol all those qualified for 6MMD as quickly as possible to ease the burden on the clinic,” he says.
“The microlearning on 6MMD has been very helpful. Our staff don’t have to be out of the facility to attend it. They can run their normal activities and attend sessions of ten minutes maximum,” says Canham.
“Our professional nurses joined the WhatsApp microlearning sessions in September last year,” says Faith Maseko, a nurse lead based at Phola Park Clinic in Thokoza in Gauteng who works for the WITS Research Health Institute (RHI). The RHI supports the health department in the management of HIV and employs more than 30 nurses.
“When nurses are trained virtually, some of the information is forgotten, but when you’re on WhatsApp, you can go back and access the information that was shared. The scenarios provided are very useful. If you see a patient, with a similar scenario you can go back and see what was discussed and apply it to your own situation,” she says.
Department of Health backing
Foster Mohale, spokesperson for the National Department of Health, says the WhatsApp-based microlearning has been “an effective low-cost, high-reach supplement to formal 6MMD training”.
He adds: “Training gaps translate directly into service gaps, affecting quality, retention, and progress toward epidemic control. Microlearning addresses this risk by enabling continuous, bite-sized reinforcement of policy and implementation guidance, rather than relying solely on once-off training events. This approach supports frontline healthcare workers in applying 6MMD consistently under real-world service pressures.”
Mohale says evidence from the department’s broader capacitation strategy shows that lifelong, continuous learning, rather than episodic training, is essential for resilient health systems.
“WhatsApp microlearning aligns with this principle by supporting rapid dissemination of updates, peer learning, and sustained mentorship. When integrated with structured models and aligned to national guidelines, it can be effectively applied across HIV, TB, maternal and child health, non-communicable diseases, and health systems strengthening more broadly,” he says.
Study has implications beyond medical education, suggesting other fields could benefit from AI-enhanced training
Artificial intelligence (AI) is becoming a powerful new tool in training and education, including in the field of neurosurgery. Yet a new study suggests that AI tutoring provides better results when paired with human instruction.
Researchers at the Neurosurgical Simulation and Artificial Intelligence Learning Centre at The Neuro (Montreal Neurological Institute-Hospital) of McGill University are studying how AI and virtual reality (VR) can improve the training and performance of brain surgeons. They simulate brain surgeries using VR, monitor students’ performance using AI and provide continuous verbal feedback on how students can improve performance and prevent errors. Previous research has shown that an intelligent tutoring system powered by AI developed at the Centre outperformed expert human teachers, but these instructors were not provided with trainee AI performance data.
In their most recent study, published in JAMA Surgery, the researchers recruited 87 medical students from four Quebec medical schools and divided them into three groups: one trained with AI-only verbal feedback, one with expert instructor feedback, and one with expert feedback informed by real-time AI performance data. The team recorded the students’ performance, including how well and how quickly their surgical skills improved while undergoing the different types of training.
They found that students receiving AI-augmented, personalised feedback from a human instructor outperformed both other groups in surgical performance and skill transfer. This group also demonstrated significantly better risk management for bleeding and tissue injury – two critical measures of surgical expertise. The study suggests that while intelligent tutoring systems can provide standardised, data-driven assessments, the integration of human expertise enhances engagement and ensures that feedback is contextualised and adaptive.
“Our findings underscore the importance of human input in AI-driven surgical education,” said lead study author Bianca Giglio. “When expert instructors used AI performance data to deliver tailored, real-time feedback, trainees learned faster and transferred their skills more effectively.”
While this study was specific to neurosurgical training, its findings could carry over to other professions where students must acquire highly technical and complex skills in high-pressure environments.
“AI is not replacing educators – it’s empowering them,” added senior author Dr Rolando Del Maestro, a neurosurgeon and current Director of the Centre. “By merging AI’s analytical power with the critical guidance of experienced instructors, we are moving closer to creating the ‘Intelligent Operating Room’ of the future capable of assessing and training learners while minimising errors during human surgical procedures.”
Graduates and third year students are encouraged to apply for the new Postgraduate Diploma to drive business ownership and job creation.
The University of the Witwatersrand (Wits) announced its Postgraduate Diploma in Innovation and Entrepreneurship. The diploma aims for graduates and third-year students in engineering, science, and health sciences to become catalysts for business ownership and job creation. Apply for the PG Dip in Innovation and Entrepreneurship before 30 November 2023.
Professor Christo Doherty, the course coordinator says: “We particularly encourage candidates who are contemplating pursuing a Master’s or PhD in any of these fields, so they can embark on advanced degrees armed with the knowledge of how to commercialise their research. Graduates of this programme will have a wealth of career opportunities. Equipped with the aptitude and mindset for innovation and creation, they represent the future generation of entrepreneurs and job creators. They will not merely seek jobs; they will create them.”
The programme was developed and is led by the Wits Innovation Centre, and will bridge the gap between academic research and real-world innovation. It will empower students to translate their research into tangible solutions that drive meaningful change in society. The Diploma seeks to harness the entrepreneurial spirit of young scientists and engineers to ensure that their research outcomes do not languish on dusty shelves but ignite the flames of practical application. Professor Nithaya Chetty, the Dean of the Wits Faculty of Science says: “South African universities must now give attention to both discovery research and innovation. This is a novel diploma that will combine collaborative teaching and learning to fast-track researchers into careers as innovators and entrepreneurs”.
The PGDip in Innovation and Entrepreneurship is a multi-faculty initiative characterised by a hands-on approach, with a year-long research project at its core. Students will collaborate closely with an interdisciplinary team of lecturers, gaining invaluable insights and guidance throughout their journey. The curriculum covers critical subjects such as The Fundamentals of Business for Innovators, Innovation and the Commercialization of Research, Creating Ventures for Innovators, and Applying Design Thinking to Innovation. The programme’s objective is to expedite the transformation of students’ research and ideas into commercially viable endeavours or solutions with significant societal impact.
From 2025, the programme will expand to include humanities, commerce and other faculties.
As work hours increase, new doctors are at greater risk of depression, according to a study in the New England Journal of Medicine. Working 90 or more hours a week was associated with changes in depression symptom scores three times larger than the change in depression symptoms among those working 40 to 45 hours a week.
Additionally, compared to those working normal hours, those working more hours had greater odds of scores equating to moderate to severe depression.
By means of advanced statistical methods, the researchers emulated a randomised clinical trial using data on more than 17 000 first-year medical residents, accounting for many other factors in the doctors’ personal and professional lives. Less than 5% met the criteria for moderate to severe depression.
They found a “dose response” effect between hours worked and depression symptoms, with an average symptom increase of 1.8 points on a standard scale for those working 40 to 45 hours, ranging up to 5.2 points for those working more than 90 hours. They conclude that, among all the stressors affecting physicians, working a large number of hours is a major contributor to depression.
The data come from the Intern Health Study, based at the Michigan Neuroscience Institute and the Eisenberg Family Depression Center. Each year, the study recruits new medical school graduates to take part in a year of tracking of their depressive symptoms, work hours, sleep and more while they complete the first year of residency, also called the intern year.
The impact of high numbers of work hours
Though the interns in the study reported a wide range of previous-week work hours, the most common work hour levels were between 65 to 80 hours per week.
The authors say their findings point to a clear need to further reduce the number of hours residents work each week on average.
“This analysis suggests strongly that reducing the average number of work hours would make a difference in the degree to which interns’ depressive symptoms increase over time, and reduce the number who develop diagnosable depression,” said Amy Bohnert, PhD, the study’s senior author and a professor at the U-M Medical School. “The key thing is to have people work fewer hours; you can more effectively deal with the stresses or frustrations of your job when you have more time to recover.”
Yu Fang, MSE, the study’s lead author and a research specialist at the Michigan Neuroscience Institute, notes that the number of hours is important, but so are the training opportunities that come from time spent in hospitals and clinics. “It is important to use the time spent at work for supervised learning opportunities, and not low-value clinical service tasks,” she says.
The field of psychiatry research risks a “lost generation” due to the difficulties of COVID, warn the authors of an editorial published in The Lancet. The burden of the pandemic has strained the critical aspect of the mentor-mentee relationship and the difficult period between the end of training and beginning research as an independent professional.
The authors, Erika E Forbes and David J Kupfer, are directors of the US-based Career Development Institute for Psychiatry, which provides teaching and mentoring programme for those embarking on a career into academic psychiatry, note that the pandemic has had a significant impact on this stage of development. The same challenges noted by the authors no doubt apply to the field of clinical psychology as well, which is also dependent on mentoring.
Both mentors and mentees are exhausted from health-related uncertainty, from Zoom meetings, and struggling to effectively collaborate, they wrote.
They note that starting a career as a scientist is a challenge even in the most stable times, but is now particularly gruelling, something they have recently borne witness to.
“At our April 2022 annual workshop, our fellows were dispirited, telling us that they feel neglected, undermined, and in some cases emotionally abused by the mentors at their home institutions. Many cannot envision a way forward.”
Though the authors are optimistic about adapting to COVID, with the limited of virtual settings and the new acknowledgement of how daily struggles impact work, they cannot deny that cannot deny that “psychiatry research is in a mentoring crisis.”
“There is a danger of losing a generation of talented, promising scientists, and this could stall progress in understanding and treating psychiatric illnesses,” they warn. To deal with this, mentors must still provide the “traditional elements of mentoring”, ie, guidance, advocacy, training, and access to professional networks, along with embracing technology and empathy. It is crucial to understand the mentee and provide them with more of the same basic support, because the usual challenges are amplified.
Mentoring is different in the COVID era, they stress. “If we accept that research will not go back to the pre-pandemic ways, adapt our behaviour to current realities, and enhance our commitment to supporting and guiding others, early-career scientists will again be able to thrive,” the authors conclude.
From left to right: Junior doctor Aniket Bharadwaj with trainers Dr Ruby Woodard and Dr Jonny Martin, diagnosing a hologram patient. Credit: University of Cambridge
A new effort from Cambridge University brings medical training in ‘mixed reality’ one step closer with modules that allow student doctors to interact with a ‘holographic’ patient.
Traditional simulation has numerous costs including maintaining simulation centres, their equipment and the faculty and staff hours to operate the labs and hire and train patient actors. This new technology could provide more flexible, cost-effective training that can be accessed all over the world.
HoloScenarios is a new training application based on life-like holographic patient scenarios, is being developed by Cambridge University Hospitals NHS Foundation Trust (CUH), in partnership with the University of Cambridge and US tech company GigXR. The first module focuses on common respiratory conditions and emergencies.
“Mixed reality is increasingly recognised as a useful method of simulator training,” said project leader Dr Arun Gupta, consultant anaesthetist at CUH and director of postgraduate education at CUH.
“As institutions scale procurement, the demand for platforms that offer utility and ease of mixed reality learning management is rapidly expanding,” he said.
Learners wearing mixed-reality headsets can interact with each other and a multi-layered, medically accurate ‘holographic’ patient. This creates a unique environment to learn and practice vital, real-time decision making and treatment choices.
Medical instructors with their own headsets can make changes on the fly, by changing patient responses or introducing complications – whether in person in a teaching group or over the internet.
Learners can also watch, contribute to and assess the holographic patient scenarios from Android, iOS smartphone or tablet. This means true-to-life, safe-to-fail immersive learning can be accessed, delivered and shared across the world, with the technology now available for license to learning institutions everywhere.
Professor Riikka Hofmann at Cambridge’s Faculty of Education is leading an analysis of the technology as a teaching method.
“Our research is aimed at uncovering how such simulations can best support learning and accelerate the adoption of effective mixed reality training while informing ongoing development,” said Prof Hofmann.
“We hope that it will help guide institutions in implementing mixed reality into their curricula, in the same way institutions evaluate conventional resources, such as textbooks, manikins, models or computer software, and, ultimately, improve patient outcomes.”
Junior doctor Aniket Bharadwaj is one of the first to try out the new technology. “Throughout medical school we would have situations where actors would come in an act as patients. With the pandemic a lot of that changed to tablet based interactions because of the risk to people of the virus,” he said.
“Having a hologram patient you can see, hear and interact with is really exciting and will really make a difference to student learning.”
The first module features a hologram patient with asthma, followed by anaphylaxis, pulmonary embolism and pneumonia. Further modules in cardiology and neurology are in development.
Delivered by the Gig Immersive Learning Platform, HoloScenarios aims to centralise and streamline access and management of mixed reality learning, and encapsulate the medical experience of world-leading doctors at CUH and across the University of Cambridge.
While the proposed National Health Insurance (NHI) could make use of existing private healthcare human resources, the necessary tax increases to fund it could drive more healthcare professionals from the country, the Professional Provident Society (PPS) has said. Economic and other factors, such as the Durban unrest, have already caused a surge of emigrations of professionals since July last year. In addition, foreign students graduates who study critical skills in South Africa (such as nurses and GPs) will no longer have an easy route to permanent residency.
The PPS, which counts about 30 000 healthcare professionals among its membership, pointed out the vulnerability of South Africa’s tax base – which has shrunk to only 6.9 million taxpayers, down from 7.6 million the year from the year before.
While it raised a number of concerns about the NHI, the group stated that it was broadly supportive of establishing universal healthcare in the country, and this goal could still be accomplished by using a dual public-private system. The PPS further noted that the government could benefit from the exceptional administrative capabilities and existing patient management systems.
However, NHI is dependent on strong, competitively remunerated human resources, with PPS pointing out that “South Africa has experienced a mass exodus of nurses in the 90s; we cannot risk that again. Both the government and private sector need to find a solution for South Africa and it cannot ‘import solutions’.”
“Professionals are a big proportion of healthcare delivery and the tax base. Their voices need to be considered.
“We urgently need to see the funding model, the implementation of the Health Market Inquiry (HMI) and details of how the system will work.”
The PPS said in a 2019 report that the highest risk to effective universal health cover in South Africa is losing highly skilled professionals to emigration. Healthcare professionals have a great deal of geographic freedom, and it is becoming easier to work in their trades the world over. COVID with its restrictions may have slowed emigrations by skilled professionals, but since July 2021, experts have seen a surge backed up by 18 months of pent-up demand.
The PPS noted that research has shown “that the decision to emigrate is a complex one that is driven by various personal and societal pull and push factors.” The NHI could be yet another push factor adding to the list of healthcare professionals’ sore points. “Healthcare worker migration from South Africa in the past has been driven by policy decisions and socio-economic and political considerations.
“In 2001, the number of nurse emigrants was roughly 20% of the total number working within the public sector in South Africa. That, together with being ranked as having the eighth-highest global number of emigrating physicians in the year 2000, created a dire situation for the sustainability of healthcare in South Africa at the time.”
Among general professionals, PPS’s research has indicated that many are considering emigration. A majority of respondents surveyed (73%) cited NHI as a potential reason for emigration, with 15% unsure and only 12% not considering leaving at all.
In addition to losses from emigration, the Department of Home Affairs has ended a 2014 waiver which allowed a quicker path to a residency permit for foreign students who acquire critical skills in South African higher learning institutions. Going forward, foreign students will no longer be able to apply for permanent residency visas without complying with the usual requirements such as providing proof of five years’ work experience. This is seen as detrimental to South Africa’s ability to attract and retain skilled professionals. This may further impact NHI implementation as the necessary skilled human resources are squeezed further as fewer foreign students may choose to study and then work in South Africa.
Since March of 2020, the COVID pandemic has put an unprecedented strain on hospitals as large surges of intensive care unit patients overwhelmed hospitals. To meet this challenge, Beth Israel Deaconess Medical Center (BIDMC) expanded ICU capacity by 93% and maintained surge conditions during the nine weeks in the first quarter of 2020.
“As COVID was sweeping through the nation, we at BIDMC were preparing for the projected influx of highly infectious, critically ill patients,” said lead author Sharon C. O’Donoghue, DNP, RN, a nurse specialist in the medical intensive care units at BIDMC. “It rapidly became apparent that a plan for the arrival of highly infectious critically ill patients as well as a strategy for adequate staffing protecting employees and assuring the public that this could be managed successfully were needed.”
After setting up a hospital incident command structure to clearly define roles, open up lines of communication and develop surge plans, BIDMC’s leadership began planning for the impending influx of COVID patients in February 2020.
BIDMC – a 673 licensed bed teaching hospital affiliated with Harvard Medical School – has nine specialty ICUs located on two campuses for a total of 77 ICU beds. Informed by an epidemic surge drill conducted at BIDMC in 2012, it was determined that the trigger to open extra ICU space would be when 70 ICU beds were occupied. When this milestone was met on March 31, 2020, departmental personnel had a 12-hour window to convert two 36-bed medical-surgical units into additional ICU space, providing an additional 72 beds.
“Because the medical-surgical environment is not designed to deliver an ICU level of care, many modifications needed to be made and the need for distancing only added to the difficulties,” said senior author Susan DeSanto-Madeya, PhD, RN, FAAN, a Beth Israel Hospital Nurses Alumna Association endowed nurse scientist. “Many of these rooms were originally designed for patient privacy and quiet, but a key safety element in critical care is patient visibility, so we modified the spaces to accommodate ICU workflow.”
Modifications included putting windows in all patient room doors, and repositioning beds and monitors so patients and screens could be easily seen without entering the room. Lines of visibility were augmented with mirrors and baby monitor systems as necessary. Care providers were given two-way radios to decrease the number of staff required to enter a room when hands-on patient care was necessary. Mobile supply carts and workstations helped streamline workflow efficiency.
Besides stockpiling and managing medical equipment including PPE, ventilators and oxygen, increasing ICU capacity also required redeploying 150 staff trained in critical care. The hospital developed a recall list for former ICU nurses, as well as medical-surgical nurses that could care for critically ill patients on teams with veteran ICU nurses.
Education and support was provided from . In-person, socially-distanced workshops were developed for each group, after which nurses were assigned to shadow an ICU nurse to reduce anxiety, practice new skills and gain confidence.
“Staff identified the shadow experience as being most beneficial in preparing them for deployment during the COVID surge,” said O’Donoghue. “Historically, BIDMC has had strong collaborative relationships with staff from different areas and these relationships proved to be vital to the success of all the care teams. The social work department played a major role in fostering teams, especially during difficult situations.”
One of the redeployment teams was the ICU proning team. Proning is known to improve oxygenation in patients with acute respiratory distress syndrome is a complex intervention, takes time and is not without its potential dangers to the patient and staff alike. The coalition maximised resources and facilitated more than 160 interventions between March and May of 2020.
“Although the pandemic was an unprecedented occurrence, it has prepared us for potential future crises requiring the collaboration of multidisciplinary teams to ensure optimal outcomes in an overextended environment,” O’Donoghue said. “BIDMC’s staff rose to the challenge, and many positive lessons were learned from this difficult experience.”
“We must continue to be vigilant in our assessment of what worked and what did not work and look for ways to improve health care delivery in all our systems,” said DeSanto-Madeya, who is also an associate professor at the College of Nursing at the University of Rhode Island. “The memories from this past year and a half cannot be forgotten, and we can move forward confidently knowing we provided the best care possible despite all the hardships.”
To help address the critical shortage of expert medical specialists in the country, including surgeons, Wits University opened the Wits Advanced Surgical Skills Lab. It has been estimated that the country needs double the number of surgeons to meet its needs, a situation worsened by losing many surgical experts to the competitive overseas market due to the lack of sufficient highly specialised facilities, infrastructure, and advanced academic training programmes.
“Wits trains more doctors, surgeons, specialists and sub-specialists than any other university in southern Africa. The new R22-million Wits Advanced Surgical Skills Lab will help to enhance the training of surgeons, across disciplines, in a state-of-the-art environment, with the best equipment available,” said Professor Damon Bizos, Head of Wits Surgical Gastroenterology, and the Clinical Head of Surgery at the Wits Donald Gordon Medical Centre. “We need to replenish these specialised skills and replicate them in adequate measure in order to deliver essential services to South Africans and Africans.”
Located on the ninth floor of the Faculty of Health Sciences building in Parktown, the Wits Advanced Surgical Skills Lab officially opened on Tuesday, 12 October 2021. The state-of-the-art facility is designed in line with international best standards. along with teaching facilities that make the Wits surgical training programme one of the best in the world.
“If we fail to replenish the pool of surgeons in South Africa, both the training of all South African doctors and the delivery of healthcare for all will be compromised. The loss of these skills will result in the loss of services in both the private and public sectors,” said Professor Zeblon Vilakazi, Wits Vice-Chancellor and Principal. “South Africa needs to retain highly skilled and specialised surgeons. By creating opportunities for doctors to undergo highly specialised training locally, rather than abroad, the likelihood of losing these doctors to other countries is lessened.”
The Wits Advanced Surgical Skills Lab will be able to provide the interdisciplinary training needs of surgical disciplines including general surgery; orthopaedics; gynaecology; ear, nose and throat; cardiothoracic; urology; maxillofacial; ophthalmologic; neuro; and plastic surgery. It will also include the training of specialists, doctors, nurses and other allied health practitioners.
“The basic and intermediate courses will help inculcate basic surgical competence and skills development, whilst advanced courses will ensure that experienced practitioners remain at the forefront of advances in the field,” added Prof Bizos. “We will offer access to in-house training as well as industry-sponsored surgical training courses and symposia. Train-the-trainer programmes and research into skills training will also be integral.”
The Wits Advanced Surgical Skills Laboratory boasts a large ‘wet lab’ with eight stations; laparoscopic towers and endoscopy (upper endoscopy and colonoscopy); has facilities available for training on cadavers; lead-lined walls to accommodate imaging; a new lecture room for 35 participants; and full audiovisual and videoconferencing facilities.
“Access to safe, high-quality surgery care remains an ongoing challenge in South Africa and beyond. There is a well-defined unmet need, and the training of surgeons and surgical care providers is an essential component of the strategy to improve surgical care and address the unmet need. Modern day approaches to training require that we must address both the technical competency and non-technical skills of the surgeon. This must be achieved in a standardised and measurable way. To do so has meant that we, as the trainers of the next generation of practitioners, must embrace new technologies and training opportunities,” said Professor Martin Smith, the Head of the Department of Surgery in the Faculty of Health Sciences at Wits University. “We are very grateful that through the support of the University and the contributions of a number of donors we have been able to establish a facility to enhance and improve this training.”