Scheduling Surgeons: Researchers Identify Factors for Hospital Efficiency
Booking operating rooms with surgical precision starts with more accurate predictions of how surgeons spend their time

Researchers at the University of Massachusetts Amherst have analysed nearly 86 500 surgeries at Baystate Medical Center to identify the top factors that influence inefficiencies in surgeon schedules. Having an efficiently organised surgical schedule has the potential to lower costs and reduce surgeon burnout, which would also improve patient outcomes.
As shortfalls in the availability of surgeons grow, the ability to meet surgical demands will only worsen, with implications for both healthcare delivery and costs.
“The most expensive part in this process of getting a surgery is the surgeon,” says Muge Capan, assistant professor in the Riccio College of Engineering at UMass Amherst and an author of the new paper published in the Journal of the American Medical Informatics Association. “Surgeons are highly skilled and they perform high-risk tasks. When we think about utilising a resource, we don’t want them to sit idle – but we also don’t want to overutilise them because these are not machines, these are people. Finding that right balance is a challenging problem.”
However, to efficiently schedule, hospitals need to predict how long a procedure will take. This includes the surgery itself as well as many other factors that surround an operation – has the surgeon recovered from their previous operation? Is the room clean? Is the proper equipment in place? “There is a lot of uncertainty there at the system level,” says Capan.
Currently, surgeries are scheduled in blocks, which is not compatible with the unpredictable nature of a hospital. “If you’re scheduling tennis lessons, it works because a tennis lesson is exactly one hour,” says Capan. “You block the court for one hour, you play, you leave, next group. But blocks don’t make sense for surgeries, because they’re so uncertain.” As a result, operating rooms (ORs) can sit empty since any block of time less than two-and-a-half hours is unusable for most surgeries.
In the pursuit of engineering a better schedule, Capan and her team collaborated with surgeons to predict their schedule by focusing on the person, not the operating room.
Surgeons are highly skilled and they perform high-risk tasks… we don’t want them to sit idle – but we also don’t want to overutilise them because these are not machines, these are people. Finding that right balance is a challenging problem.
Muge Capan, assistant professor in the Riccio College of Engineering at UMass Amherst
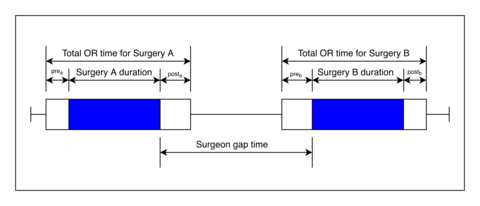
“There’s so much research on the operating room itself – what happens between the time a patient leaves the OR to the time the next patient enters the OR,” says Jonathan Akhagbosu, first author on the paper and UMass Amherst industrial engineering Ph.D. candidate. “But we wanted to look at it from a surgeon’s point of view: What happens between when a surgeon finishes one case and proceeds to the next case?”
The researchers named this time between operations “gap time.” In their study, they used machine learning to analyse three years of medical records from Baystate Medical Center in Springfield to determine the characteristics of a surgery that can predict these gaps in a surgeon’s schedule.
A selection of the top factors associated with larger gap times are: if the surgeon’s previous or following case is an emergency, the preceding surgery is related to the chest (thorax), the following procedure is on the heart, or the surgery is highly demanding.
Also, the last factor on the list – the assessment of how taxing an operation is on the surgeon – the researchers used mathematical models to create a new measurement called surgical case demand. Cases fall into one of three tiers. Type 1 consists of short, scheduled procedures of low-severity illness and elective surgeries, such as the removal of fatty lumps from the skin (lipoma excision) or simple dental rehabilitation. Type 2 events are more demanding, such as a mastectomy or knee replacement. And type 3 surgeries are the most onerous: the condition is more severe and they happen during off-hour times. Examples include emergency brain or abdominal operations and spine procedures.
It’s also worth noting that eye (ophthalmology) and orthopedic surgeries were associated with shorter gap times.
Capan envisions that predicting schedules can help recapture some of this lost time. “If there’s going be a gap, let’s figure out if that gap is long enough that I could squeeze in something else,” says Capan. “This is called ‘collectible time’ in the literature. Collectible time means it’s a useful gap. So what we learned about gap time could potentially help us understand collectible time.”
Source: University of Massachusetts