Research published in The FEBS Journal may help overcome challenges to the treatment of malaria – a tropical disease caused by infection of red blood cells with Plasmodium parasites, which are transmitted through infected mosquito bites. The research is based on a strategy that targets an enzyme specific to the parasite, Falcipain-2 (FP2), which is essential for parasite survival and growth within the host.
FP2 allows the parasite to digest human haemoglobin so that it can replicate inside red blood cells, which leads to severe malaria symptoms, including red blood cell destruction. Although FP2 is parasite-specific, it is highly similar to a class of human enzymes called cathepsins. This study therefore sought to determine the detailed structural and functional characterizations of FP2 so that it could be targeting without harming cathepsins.
Previously, the researchers identified that polyethylene glycol (PEG) can form stable interactions with FP2. In this latest study, they focused on how different PEG molecules bind to FP2 and its target, haemoglobin. Their computational analyses identified a binding region, or pocket, of a particular PEG called PEG400 with FP2. This pocket exhibits minimal conservation in human cathepsins. PEG400 was capable of binding FP2 and affecting its digestion of haemoglobin.
“The findings pave the way for designing and incorporating new small molecule inhibitors of FP2 activity, suggesting opportunities for selective antimalarial therapies with a cumulative benefit of reducing off-target specificity,” said corresponding author Sampa Biswas, PhD, who conducted this work while at the Saha Institute of Nuclear Physics, in India, and is currently at InBOL (Indian Barcode of Life) Health Care.
Ahead of World Malaria Day on 25 April, the World Health Organization (WHO) has announced a significant step forward in the fight against malaria with the prequalification of the first treatment developed specifically for newborns and young infants weighing between two and five kilograms. The prequalification designation indicates that the medicine meets international standards of quality, safety and efficacy, and will help to expand access to quality-assured treatment for one of the most underserved patient groups.
The newly prequalified treatment, artemether-lumefantrine, is the first antimalarial formulation designed specifically for the youngest malaria patients. Until now, infants with malaria have been treated with formulations intended for older children, which increase the risk of dosing errors, side effects and toxicity. WHO prequalification will enable public sector procurement, contributing to closing a long-standing treatment gap for some 30 million babies born each year in malaria-endemic areas of Africa.
“For centuries, malaria has stolen children from their parents, and health, wealth and hope from communities,” said Dr Tedros Adhanom Ghebreyesus, WHO Director-General. “But today, the story is changing. New vaccines, diagnostic tests, next-generation mosquito nets and effective medicines, including those adapted for the youngest, are helping to turn the tide. Ending malaria in our lifetime is no longer a dream – it is a real possibility, but only with sustained political and financial commitment. Now we can. Now we must.”
New prequalified tests
On 14 April 2026, WHO also prequalified three new rapid diagnostic tests (RDTs) designed to address emerging diagnostic challenges for malaria. The most common malaria RDTs for P. falciparum parasite work by detecting the protein, known as HRP2. But based on reported studies and surveys in 46 countries, some strains of the malaria parasite have lost the gene that makes this protein – so they become “invisible” to HRP2-based RDTs, leading to false-negative results. In countries in the Horn of Africa, up to 80% of cases were missed, leading to delayed treatment, severe illness, and even death.
The new tests address this issue by targeting a different parasite protein (pf-LDH) that the malaria parasite cannot easily shed. They provide a reliable, quality-assured alternative where HRP2-based tests are failing. WHO now recommends that countries switch to these alternative RDTs when more than 5% of cases are missed due to pf-hrp2 deletions. This ensures accurate diagnosis, appropriate treatment, and protects hard-won malaria control gains – especially for the most vulnerable communities.
by Dr Taneshka Kruger, Project Manager: University of Pretoria Institute for Sustainable Malaria Control (UP ISMC) and Prof Tiaan de Jager, Director: UP ISMC
Eliminating malaria requires effort that goes far beyond our laboratories. It also happens in homes, villages and clinics, where gogos (grandmothers), mothers, young women and other citizen scientists play a vital role in prevention, early action and creating public awareness.
On 25 April, we commemorate World Malaria Day. This day is aimed at raising awareness about one of the world’s oldest and deadliest diseases, while also recognising the progress we’ve made in controlling and eliminating it. This year’s theme, ‘Driven to end malaria: Now we can. Now we must.”, is a reminder that success depends not only on medicine and science, but also on the people who protect families and strengthen communities every day.
Malaria remains a life-threatening disease transmitted by female Anopheles mosquitoes infected with the Plasmodium parasite. Globally, hundreds of millions of cases are reported each year, with the overwhelming burden falling on sub-Saharan Africa. The most vulnerable groups include pregnant women, children under five and older persons.
Why women and children face greater malaria risks
Pregnancy reduces a woman’s immunity to malaria, increasing the risk of infection and severe illness. Malaria during pregnancy can lead to maternal anaemia and serious complications such as miscarriage, premature birth, stillbirth and low birth weight. Low birth weight is one of the leading contributors to neonatal mortality and can affect a child’s long-term development.
Children under five continue to carry the heaviest malaria burden. In Africa, they account for roughly three-quarters of malaria-related deaths. Their immune systems are still developing, making prevention, early diagnosis and prompt treatment essential for survival.
The family members who spot danger first
In many rural communities, mothers – and especially grandmothers – are the backbone of family life. They shape household health practices, encourage clinic visits, and ensure children use preventative measures against malaria, such as sleeping under protective nets, where possible. Their lived experience gives them influence and trust, and when equipped with up-to-date malaria information they become powerful advocates for prevention. They are often the first to notice symptoms such as fever, fatigue or vomiting, and frequently help decide when and how medical care is sought.
Women also care for elderly family members, who may have weaker immune systems and be more vulnerable to complications from malaria. In areas where clinics are far away or transport is limited, their vigilance can be lifesaving.
Young women – whether students, entrepreneurs, community workers or volunteers – also play an increasingly important role in sharing reliable malaria information. They help bridge the gap between scientific knowledge and everyday community life, promoting practical actions such as:
Seeking early testing when symptoms such as fever appear
Reducing mosquito breeding sites through environmental management
Using preventative strategies to avoid mosquito bites
Consistent use of insecticide-treated bed nets where available
Attending antenatal clinics for intermittent preventive treatment in pregnancy (IPTp), in countries where these programmes are offered.
Through each of these actions and more, women’s leadership strengthens community resilience and promotes healthier futures.
Young women spreading life-saving knowledge
One of the most encouraging developments in rural malaria response is the rise of women citizen scientists. Through training programmes supported by research institutions, women from local communities are gaining skills to assist with field data collection and malaria surveillance.
In malaria research conducted by the University of Pretoria Institute for Sustainable Malaria Control in Limpopo’s Vhembe District, women citizen scientists have contributed by:
Engaging tribal authorities and communities about the purpose of the research and how communities can benefit
Collecting health data to assess the impact of malaria control methods on people and the environment
Collecting mosquito samples for vector surveillance and climate-related research
Gathering knowledge, attitude and practice data through surveys
Conducting interviews before and after interventions to assess effectiveness
Running focus groups to better understand community needs, behaviours and challenges.
By participating in field research, these women gain scientific skills while contributing directly to malaria control strategies. Their involvement helps ensure that research is done in local languages, reflects lived realities and leads to practical action communities can trust and use.
Just as importantly, this model expands women’s roles beyond traditional caregiving expectations. It positions them as knowledge holders, data contributors and active partners in scientific discovery. It also shows young girls in these communities that science is accessible, relevant and open to them.
From community member to citizen scientist
When mothers, gogos and young women understand the risks malaria poses – especially to pregnant women and children under five – they are better equipped to protect their families. When they are empowered as citizen scientists, they move from being passive recipients of health messaging to active drivers of change, contributing to local malaria elimination efforts. Their combined role as caregivers, educators and research partners strengthens both households and health systems.
On this World Malaria Day, we should recognise and honour the women who care for feverish children through the night, accompany pregnant daughters to clinics, share trusted advice with neighbours, and step into fields and villages as trained citizen scientists. By investing in women’s knowledge, leadership and participation at home, in communities and in science, we move closer to a future free from this preventable disease.
Ivermectin was originally celebrated as a revolutionary treatment for parasitic disease in humans and animals. It has since evolved into a focal point of misinformation and heated debate.
During the early part of the COVID pandemic, it was touted on social media as a miracle cure for the virus, despite a lack of robust evidence.
The drug is a small organic chemical that can be extracted from the bacterium Streptomyces avermitilis. This bacterium grows in the soil, and was first found near the grounds of a Japanese golf course.
It was first approved for use in animals in 1981 and in humans in 1987. It’s now available in various brands as tablets and creams you apply to the skin.
Assessing the evidence
Governments use human clinical trials to decide whether to approve a medicine for sale.
But clinical trials aren’t the highest level of evidence to inform best practice and guide decisions. For that, there are Cochrane reviews.
A Cochrane review brings together a panel of experts who collate and assess all the relevant evidence on a medication. It takes data from multiple clinical trials, and other studies, and evaluates it following clear and structured steps. It’s able to examine and critique study designs to identify bias and reject bad data.
Cochrane reviews are also regularly updated to take into account new information. The result is a summary that is considered the highest level of evidence to guide decision-making.
So what do Cochrane reviews say about ivermectin for different conditions?
Ivermectin is used to treat a variety of parasitic worm infections. These include the round worms Ascaris lumbricoides, Strongyloides stercoralis, Wuchereria bancrofti, and Brugia malayi.
The latter two worms cause the disease lymphatic filariasis (or elephantiasis) which causes severe swelling in the arms, legs, breasts and genitals.
When ivermectin is used to treat Strongyloides stercoralis, the Cochrane panel found it is better than albendazole and had fewer side effects than thiabendazole.
For Ascaris lumbricoides, the panel concluded ivermectin was as good as albendazole and mebendazole.
For treating lymphatic filariasis, a Cochrane review found ivermectin or diethylcarbamazine should be standard treatment in combination with albendazole.
Rosacea
The Cochrane review for rosacea evaluated 22 different treatments for this skin condition, including a variety of drugs, as well as light therapy, cosmetics and reducing the intake of spicy food.
It concluded that ivermectin applied to the skin was more effective than a placebo, and a bit better than the other standard medication, metronidazole.
Scabies
Cochrane has two reviews on the use of ivermectin for scabies. One specifically evaluated ivermectin and permethrin as treatments. The other evaluated all available treatments for scabies.
The first review concluded both permethrin and ivermectin were just as effective, regardless of whether the ivermectin was administered orally or directly onto the skin.
In contrast, the second review concluded ivermectin does work but topical permethrin appeared to be the most effective treatment.
Malaria
The Cochrane panel looked specifically at whether ivermectin could reduce transmission of the malaria parasite, rather than as a treatment.
Unfortunately there was just a single clinical trial to use as evidence. In that trial, residents of eight villages were given ivermectin and albendazole together, with follow up doses of just ivermectin. The researchers then looked at the rates of child infection over 18 weeks.
Even though the trial didn’t show ivermectin prevented infection, due to the high risk of bias in it, the Cochrane panel couldn’t conclude either way whether ivermectin worked or not.
River blindness
River blindness is caused by another parasitic worm called Onchocerca volvulus.
The Cochrane review concluded there was a lack of evidence either way to know whether it works to prevent infection-based visual impairment and blindness.
It evaluated the data from four clinical trials and two large community-based studies.
One of the reasons the panel was unable to make a firm conclusion was because it thought the drug may work differently against different strains of the parasite and in people of different ethnicity.
Cancer
There are no Cochrane reviews on ivermectin’s use for cancer because clinical interest in the drug for this condition is just starting.
There is a current clinical trial that is evaluating ivermectin in combination with antibody-based drugs for breast cancer.
Early results showed the combination of antibody drugs with ivermectin was safe to patients, but no efficacy data has been published.
COVID
The Cochrane panel rejected the data for seven clinical trials and included 11 other trials. Rejected trials included those which compared ivermectin against other drugs which were known to not be effective against COVID, such as hydroxychloroquine.
The review concluded there was no evidence to support the use of ivermectin for the treatment or prevention of COVID. In making that conclusion, it evaluated treatments that used invermectin or placebo in combination with standard care and whether treatment reduced death, illness, or the length of the infection.
Red Blood Cell Infected with Malaria Parasites Colourised scanning electron micrograph of red blood cell infected with malaria parasites (teal). The small bumps on the infected cell show how the parasite remodels its host cell by forming protrusions called ‘knobs’ on the surface, enabling it to avoid destruction and cause inflammation. Uninfected cells (red) have smoother surfaces. Credit: NIAID
A new clinical trial led by QIMR Berghofer, in collaboration with University of Sunshine Coast Clinical Trials Network has found a medication currently used for some blood disorders could help the body fight malaria more effectively.
The findings mean the drug, ruxolitinib, could potentially be used alongside standard treatment to boost recovery and strengthen people’s immune systems against future infections.
Malaria kills more than 600 000 people each year and three quarters of those deaths are in children under the age of five.
Current treatments for malaria work by killing the parasite that causes most malaria deaths, Plasmodium falciparum. However, even with these treatments, fatality rates from severe malaria remain high.
Furthermore, while patients develop some immunity after infection, this protection is often incomplete, leaving many vulnerable to reinfection.
“While antimalarial treatments are effective at killing the parasite, they don’t directly address the inflammation that contributes to severe illness and death. These findings suggest that we may be able to improve clinical outcomes by targeting the host inflammatory response as well as the parasite itself,” she said.
The research, published in Science Translational Medicine, looked at how the immune system responds to malaria via the body’s ‘early warning system’ known as type 1 interferon signalling.
To do this, researchers enrolled 20 healthy adult volunteers who had never been exposed to malaria. Participants were deliberately infected with Plasmodium falciparum under closely monitored conditions. Eight days later, all participants received standard malaria treatment (artemether-lumefantrine), while 11 were also given ruxolitinib. Three months later, participants were re-infected with malaria to test how their immune systems responded to a second infection.
The research revealed ruxolitinib was safe and well-tolerated, compared with the placebo group, and participants who received ruxolitinib showed a lower inflammatory response, and favourable changes in markers linked to disease severity.
QIMR Berghofer’s Program Director of Infection and Inflammation Professor Christian Engwerda says the results are encouraging.
“One of the biggest challenges in efforts to eliminate malaria is the limited efficacy and duration of protection provided by current vaccines. By boosting the immune system without causing detrimental inflammation with drugs like ruxolitinib, we may be able to overcome these challenges,” he said.
The researchers say it’s important to note that the study was conducted in healthy volunteers who did not live in malaria-endemic regions. Further studies in malaria-endemic regions will be needed to determine whether these findings translate into improved outcomes for patients most affected by the disease.
Researchers have adapted a rapid diagnostic technology that is able to identify undetected cases of malaria, helping tackle the spread of disease.
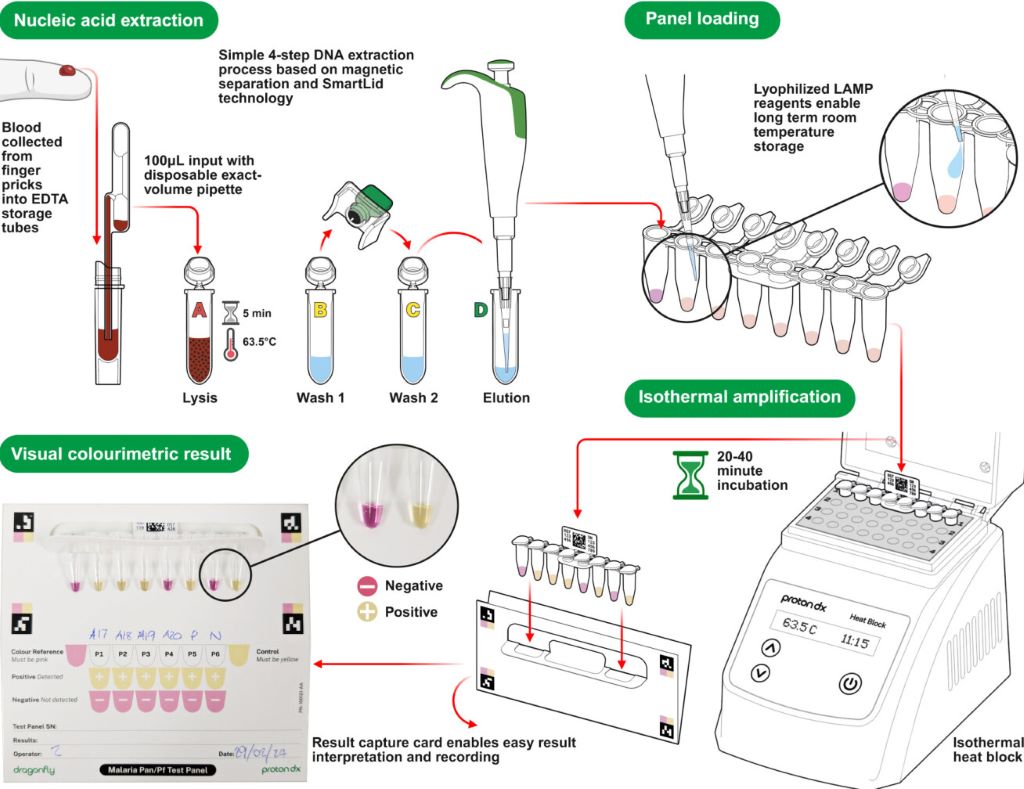
A diagram showing how the Dragonfly technology works (Credit: ProtonDx)
A team of scientists from Imperial College London, the MRC Unit The Gambia, the Clinical Research Unit of Nanoro in Burkina Faso, ProtonDx Ltd, and the NIHR Global Health Research Group have developed and validated a low-cost, point-of-care diagnostic that can rapidly detect low levels of malaria from a finger prick.
The test, called Dragonfly, relies on technology originally created at Imperial and its spinout ProtonDx. The technology allows users to diagnose malaria with high accuracy, without the need for extensive laboratory equipment or infrastructure. Results can be delivered in as little as 45 minutes, and the test is sensitive enough to detect even the lowest levels of malaria parasites in the blood – meaning that people without symptoms of malaria can still be identified.
Malaria is one of the leading causes of preventable deaths worldwide, with around 95% of all deaths occurring in Africa. Asymptomatic infections are a major driver of ongoing transmission, as individuals who carry the disease without showing symptoms do not seek medical treatment. Mosquitos feeding on blood from people without malaria symptoms can still deliver the malaria parasite to other people when they take their next blood meal. The new technology offers hope for combatting this potential spread of infection, by offering a way to identify previously undetectable malaria cases rapidly and on the ground in countries which are most affected by malaria.
The findings, published in Nature Communications, have significant global health implications as this field-deployable molecular diagnostic method offers a sensitive, scalable solution to support test-and-treat strategies for malaria elimination across Africa.
Professor Aubrey Cunnington, from Imperial’s Department of Infectious Disease and Co-Lead of the NIHR Global Health Research Group with Professor Halidou Tinto (from IRSS, Burkina Faso), said: “This is the first time that a diagnostic test for use outside of a laboratory setting has proven sensitive enough to detect low level malaria parasite infections in people who don’t have any symptoms.
“These people are the main source of malaria transmission, and in countries trying to eliminate malaria, there has long been interest in trying to detect these asymptomatically infected people with a screening test performed in their communities, and then giving treatment to those who are positive.
“Until now, no test has been able to detect enough of these infected people to make this a viable proposition, but the Dragonfly test now makes this possible.”
Detecting the undetectable
By collaboratively working as part of the NIHR Global Health Research Group, scientists were able to develop and test this new technology with the help of researchers in the regions affected most by malaria.
Almost 700 blood samples were collected from the community in The Gambia and Burkina Faso to assess the Dragonfly test’s accuracy against gold standard PCR testing and other common methods of testing, including expert microscopy and rapid diagnostic test (e.g., lateral flow immunoassay).
It was found that the Dragonfly tool could detect >95% of all malaria parasite infections, including 95% detection of those where the numbers of parasites were too low to be detected by looking at blood under a microscope.
Although Dragonfly is currently used as a research-used-only device, important progress is being made to understand the potential cost of a final manufactured version – especially when deployed at scale – a critical factor for effective deployment in sub-Saharan Africa. The team is already working closely with the Africa Centres for Disease Control and Prevention to explore opportunities with local manufacturers in the region, ensuring that production and scale-up can be rooted in local capacity. Future studies will also need to assess the robustness of the tool in community settings which are less connected to laboratory facilities.
Dr Jesus Rodriguez-Manzano, last author and technology development lead, from the Department of Infectious Disease, said “This research would not have been possible without the collaborative nature and all the organisations who took part in this study. The technology delivered through this work represents a game changer for malaria control efforts.”
The testing equipment
In the Dragonfly testing process, a capillary blood sample obtained from a simple finger prick is processed in around 10 minutes, without the need for specialised laboratory equipment, to extract high-purity nucleic acids from malaria parasites. The prepared sample is then placed into a detection panel, which is inserted into a portable heater.
After a 30-minute incubation at a constant temperature, results can be read visually using a colour chart: a pink reaction indicates a negative result, while a yellow reaction confirms malaria infection.
The Dragonfly can be manufactured at a fraction of the cost of other platforms, is compact enough to fit into a backpack, and can operate on batteries, an important feature for bringing the tool directly to communities without requiring additional specialised equipment. Testing can be carried out by most people without extensive training, meaning that healthcare providers or scientists do not need to be present for its use.
A collaborative new study involving KEMRI-Wellcome Trust researchers has highlighted a new way to control malaria transmission. The study found that ivermectin, a drug normally used for neglected tropical diseases, led to a 26% reduction in new malaria infections among children aged 5-15 by killing feeding mosquitoes.
Malaria remains a global health challenge, with 263 million cases and 597 000 deaths reported in 2023. Current vector control methods, such as long-lasting insecticidal nets and indoor residual spraying, have become less effective due to insecticide resistance and behavioural adaptations in mosquitoes to bite outdoors and during dusk or dawn, when people are not protected by these measures. This underscores the urgent need for innovative solutions to combat malaria.
The BOHEMIA trial, the largest study on ivermectin for malaria to date, showed a 26% reduction in new malaria infection on top of existing bed nets,providing strong evidence of ivermectin’s potential as a complementary tool in malaria control. Coordinated by the Barcelona Institute for Global Health (ISGlobal) – an institution supported by the “la Caixa” Foundation – in collaboration with the Manhiça Health Research Centre and the KEMRI-Wellcome Trust Research Programme, the study has been published in The New England Journal of Medicine.
Ivermectin is a drug traditionally used to treat neglected tropical diseases like onchocerciasis which causes river blindness and lymphatic filariasis which causes elephantiasis. It has now been shown to reduce malaria transmission by killing the mosquitoes that feed on treated individuals. Given the rising resistance to conventional insecticides, ivermectin could offer an effective new approach totackle malaria transmission, especially in regions where traditional methods have become less effective.
The Unitaid-funded BOHEMIA project (Broad One Health Endectocide-based Malaria Intervention in Africa) conducted two Mass Drug Administration (MDA) trials in the high-burden malaria regions: Kwale County (Kenya) and Mopeia district (Mozambique). The trials assessed the safety and efficacy of a single monthly dose of ivermectin (400mcg/kg) given for three consecutive months at the start of the rainy season in reducing malaria transmission. In Kenya, the intervention targeted children aged 5–15, while in Mozambique it focused on children under five.
In Kwale County, Kenya, children who received ivermectin experienced a 26% reduction in malaria infection incidence compared to those who received the control drug. The trial involved over 20 000 participants and more than 56 000 treatments, demonstrating that ivermectin significantly reduced malaria infection rates – particularly among children living further from cluster borders or in areas where drug distribution was more efficient. Moreover, the safety profile of ivermectin was favourable, with no severe drug-related adverse events and only mild, transient side effects already seen with ivermectin in campaigns against neglected tropical diseases.
Dr Joseph Mwangangi, Senior Principal Research Scientist at the KEMRI-Wellcome Trust Research Programme, added: ‘These results align with the World Health Organization’s (WHO) criteria for new vector control tools.’
Carlos Chaccour, co-principal investigator of the BOHEMIA project said: ‘We are thrilled with these results. Ivermectin has shown great promise in reducing malaria transmission and could complement existing control measures. With continued research, ivermectin MDA could become an effective tool for malaria control and even contribute to elimination efforts.’
In contrast, the implementation of the Mozambique trial in the rural district of Mopeia faced severe disruptions due to Cyclone Gombe in 2022 and a subsequent cholera outbreak, which significantly disrupted operations.
Francisco Saúte, director of the Manhiça Health Research Centre said: ‘One of the most important lessons we learned from the trial in Mopeia is thatstrong community engagement is essential. Building trust with local communities and fostering close collaboration with the Health Ministry, National Malaria Control Program, and local authorities was key to ensuring acceptance of the ivermectin MDA.’
In addition to reducing malaria transmission, ivermectin MDA offers significant collateral benefits. The BOHEMIA team found an important reduction in the prevalence of skin infestations such as scabies and head lice in the ivermectin group in Mozambique, and the community reported a major reduction in bed bugs in Kenya. These effects are particularly valuable when ivermectin is integrated into existing delivery systems, maximising its impact on public health.
The study is part of a larger global effort to assess ivermectin’s potential in malaria control. The findings have been reviewed by the WHO vector control advisory group, which concluded that the study had demonstrated impact and recommended further studies. Findings were also shared with national health authorities as they evaluate the potential inclusion of ivermectin in malaria control programmes.
Regina Rabinovich, BOHEMIA PI and Director of ISGlobal’s Malaria Elimination Initiative said: ‘This research has the potential to shape the future of malaria prevention, particularly in endemic areas where existing tools are failing. With its novel mechanism of action and proven safety profile, ivermectin could offer a new approach using a well-known, safe drug that can add to the effect of other mosquito control tools available today.’
The Global Fund to Fight AIDS, TB and malaria (Global Fund) has notified Health Minister Aaron Motsoaledi that it will reduce funding to South Africa by R1.4-billion.
Global Fund said it would be reducing allocations for the seventh grant cycle from R8.5-billion to about R7.1-billion, a 16% reduction. Of this, 55% would be allocated to the National Department of Health and the rest to non-profit organisations such as the Networking HIV & AIDS Community of Southern Africa, Beyond Zero, and the AIDS Foundation of South Africa.
The fund informed recipient countries in May that it would be revising over 200 grants amidst funding shortfalls.
Global Fund was established in 2002 and provides funding for HIV, TB and malaria programmes in over 100 countries. According to its 2024 results report, 72% of its funding from 2021 to 2024 went to sub-Saharan Africa.
Other African countries also received notification of funding cuts. Mozambique’s allocation decreased by 12%, Malawi’s by 8% and Zimbabwe by 11%.
The shortfall in funding is due to Global Fund not having received money pledged by national governments. Over US$4 billion of the shortfall is due to the United States not fulfilling its pledge.
We reported last month how Mozambique’s health system has crumbled amidst USAID funding cuts.
In South Africa, funding cuts from PEPFAR earlier this year have led to clinics closing down, health staff getting retrenched, and people struggling to access HIV medication.
“As you know, the external financing landscape for global health programs is going through significant changes, with substantial impact on lifesaving services for the fight against the three diseases and health and community systems,” the Global Fund said in its letter to South African representatives.
The letter continued that while the Global Fund has “received some significant donor payments in recent days”, prospects to give the full grant cycle 7 (GC7) pledges “remain highly uncertain” and still face a risk of funding shortfalls.
“This is a difficult and unavoidable decision, which may require your country to reconsider how best to use the remaining GC7 grant amounts together with domestic resources and other sources of funds to keep saving lives,” the Global Fund said.
Foster Mohale, Department of Health spokesperson, said that the funding cut did not come as a surprise. Mohale said the department is “working with the provinces” to ensure that “service delivery” is not disrupted, and to apply measures to ensure “efficient use of limited resources”.
The international community must protect global responses to HIV, tuberculosis (TB), and malaria to serve humanity’s collective interests, according to an opinion article published May 14, 2025, in the open-access journalPLOS Global Public Health by Gorik Ooms from the Institute of Tropical Medicine, Belgium, and colleagues.
Within days of starting his second term as President, Donald Trump ended most United States (US) contributions to global health. Global responses to HIV, TB and malaria are not the only programs affected but were particularly dependent on US support. The US withdrawal from global health could result in 3 million additional HIV deaths and 10 million additional HIV infections, 107 000 additional malaria deaths and 15 million additional malaria infections, and 2 million additional TB deaths, all in 2025.
HIV, TB and malaria are global health security threats that require international collective action. The Global Fund to fight AIDS, TB and Malaria (Global Fund) entered its replenishment cycle for 2027–2029, with a target of $18 billion. A failure of this replenishment would make it impossible for many countries to compensate for decreasing US funding and decreasing Global Fund support.
The abrupt end of most US funding for global health comes at a crucial moment for the fight against the three epidemics. For HIV, funding cuts are disrupting treatment and prevention, and increasing morbidity, mortality and infections especially among marginalised groups. The transmission of TB remains high due to insufficient access to treatment, urbanisation and undernutrition. Control of malaria remains elusive due to emerging resistance to treatments, and insecticides, gaps in prevention, and limited access to healthcare.
According to the authors, the reduction of US bilateral aid calls for re-prioritisation and enhanced coordination of the global fights against HIV, TB and malaria. Currently, the Global Fund is uniquely positioned to undertake this endeavour, as it financially supports HIV, TB and malaria programs in most, if not all, countries affected by US spending cuts. This requires a successful replenishment, which seems improbable given uncertainty about the US position and considering the aid spending cuts announced by other high-income countries. Low- and middle-income countries need to step in, which necessitates an overhaul of the Global Fund governance.
The authors outline four action points. First, all countries, regardless of income level, should support the current replenishment of the Global Fund. Second, the replenishment mechanism should move toward agreed and fair assessed contributions, such as 0.01% of the annual gross domestic product of all countries. Third, the Global Fund should commit to overhauling its governance structures to promote equal representation among geographical constituencies. Fourth, the Global Fund should commit to adhere to the Lusaka Agenda, which captures consensus around five key shifts for the long-term evolution of global health initiatives and the wider health ecosystem.
As noted by the authors, these four actions would save essential elements of the global responses to HIV, TB and malaria and set a central and collaborative mechanism for global health security on a path toward the principles of global public investment.
Dr Gorik Ooms adds: “Richer countries still view global health cooperation primarily as aid, from them to poorer countries. They do not seem to realise how this cooperation also protects their own interests. We must not only find enough funding to sustain it; but also rethink how we work together. Through genuine international cooperation between equal partners.”
Co-author Dr Raffaella Ravinetto concludes: “It is not only a matter of keeping life-saving programs alive. It is also a matter of building and maintaining a solid ecosystem, encompassing health infrastructure, policies and human resources, to make quality health care feasible everywhere. Through solidarity we can serve common interests.”
Image Caption: A person holds medications. Limited access to diagnostics and medicines will worsen treatment quality, inducing resistance to antiretrovirals and medicines for infections.
Red Blood Cell Infected with Malaria Parasites
Colourised scanning electron micrograph of red blood cell infected with malaria parasites (teal). The small bumps on the infected cell show how the parasite remodels its host cell by forming protrusions called ‘knobs’ on the surface, enabling it to avoid destruction and cause inflammation. Uninfected cells (red) have smoother surfaces. Credit: NIAID
Indiana University School of Medicine researchers and their collaborators in Uganda at the Makerere University School of Medicine have uncovered a significant connection between elevated uric acid levels and life-threatening outcomes in children with severe malaria.
Published in Nature Medicine, the study identified hyperuricaemia – high uric acid levels – as a potential contributor to increased mortality and long-term neurodevelopmental challenges in children with severe malaria. These findings open the door to future research that could improve treatment strategies for children affected by severe malaria, a disease caused by mosquito-transmitted parasites and a leading cause of death in African children.
“Our findings show that hyperuricemia is strongly associated with death in the hospital and after discharge and with long-term cognitive impairment in children with severe malaria,” said Chandy C. John, MD, paediatrics professor at IU School of Medicine, who co-led the study. “We also showed several mechanisms by which hyperuricaemia may lead to these outcomes, suggesting that hyperuricaemia is not just associated with bad outcomes but may contribute to them.”
The researchers analysed data from two independent groups of children with severe malaria in Uganda and found that 25% had hyperuricaemia. This condition is caused by excess uric acid, which is a harmful body waste substance found in blood. The primary drivers of hyperuricaemia in study participants were broken-down infected red blood cells and kidney injury, which reduces the body’s ability to get rid of the extra uric acid.
In the study, hyperuricemia was linked to four negative outcomes in children with severe malaria: serious health complications like coma and anaemia, a higher risk of death during hospitalisation, a higher risk of death after discharge from the hospital, and long-term cognitive impairment in survivors.
The study also revealed that children with hyperuricemia had more harmful gut bacteria, which can cross the injured gut lining and cause sepsis. Together, these findings highlight a need for clinical trials to test the effectiveness of uric acid-lowering medications as an additional treatment for severe malaria.
“Additional studies are needed to determine whether lowering uric acid in children with severe malaria might reduce hospital deaths, post-discharge deaths and long-term cognitive impairment,” said Andrea Conroy, PhD, associate professor of paediatrics at the IU School of Medicine and co-leader of the study. “Our hope is that these studies will provide new insights and potentially lead to improved treatments that save lives.”
This research builds on the team’s recent discovery of partial resistance to the primary treatment for malaria in African children with severe malaria. Both studies underscore the importance of prioritizing new strategies to combat malaria, which affected 263 million people and caused nearly 600,000 deaths worldwide in 2023.