
AIDS 2026: Momentum Builds for Monthly HIV Prevention Pill, but Key Data Not Yet in

By Marcus Low for Spotlight
If an HIV prevention pill that provides a month of protection at a time performs well in two ongoing clinical trials, it could become the next big thing in HIV prevention after the lenacapavir injection. A new licensing agreement is paving the way for South Africa’s Aspen Pharmacare to produce the pill should the study findings be positive and the drug be registered.
In June, South Africa’s health department started rolling out the six-monthly lenacapavir HIV prevention injection to around 10% of public sector clinics. While the rollout of this jab still has a long way to go, the next generation of HIV prevention products is already on the horizon.
Two of those new products stand out. One is a new formulation of lenacapavir that looks as if it can provide 12 months of protection at a time. While results so far are promising, the pivotal data on this once-yearly HIV prevention jab is only expected in a year or two.
The other product that has many people in the HIV world excited is a monthly HIV prevention pill that contains a highly potent antiretroviral medicine called alimatravir (it was previously called MK-8527). It starts working within around an hour after someone takes it and appears to provide a month of protection at a time. One benefit of the pill, compared to the lenacapavir injection, is that it would be easier to distribute at scale, given that there is no need for a nurse to administer an injection.
As Spotlight reported in some depth last year, alimatravir looked very promising in a phase 2 study, although for now the jury is still out on the drug’s safety and efficacy. It is currently being evaluated in two pivotal phase 3 clinical trials called EXPRESSIVE-10 and EXPRESSIVE-11. Both these studies started last year and are expected to be completed by around mid-to-late 2027. Medicines are typically only registered for use after positive results in such phase 3 studies.
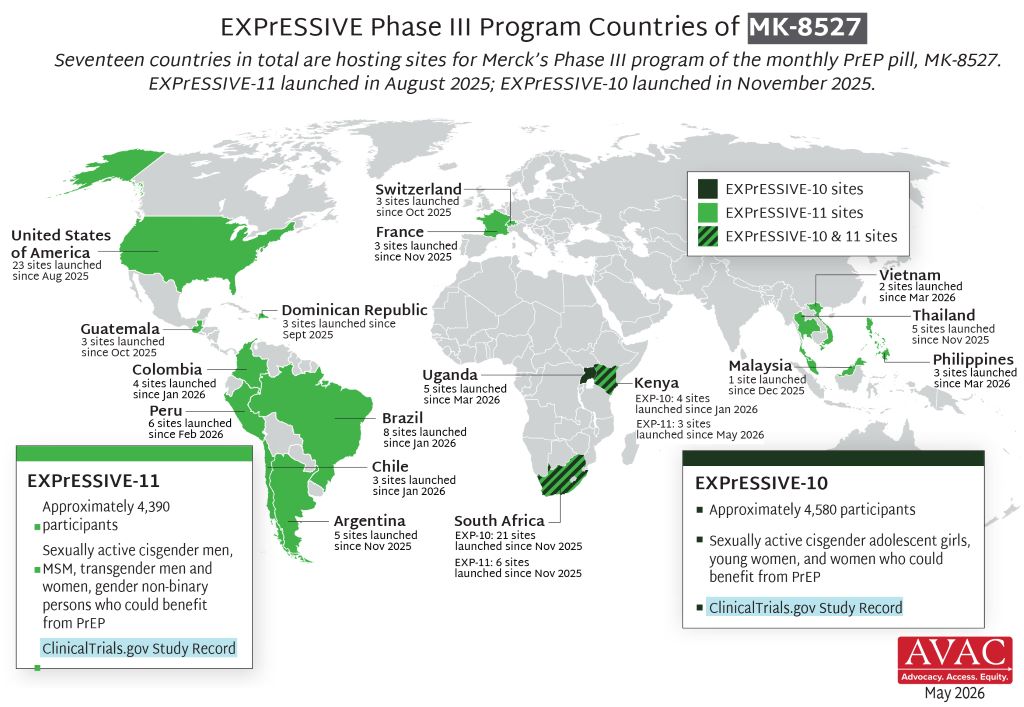
“The monthly pill offers an alternative for people who would like a long acting, less frequently dosed PrEP but not needle friendly … so it really is about giving more options especially on the pill side,” Professor Linda-Gail Bekker, primary investigator in South Africa on the EXPRESSIVE-10 study, told Spotlight. “You could imagine that just having to remember to take a small easy to swallow pill on the day you pay your bills monthly could be very easy for people. We understand that the packaging is also going to be very user friendly- looking more like a gum packet than a bottle of antiretroviral pills which may also reduce stigma.” (PrEP refers to pre-exposure prophylaxis like HIV prevention pills or injections.)
Licence to make generics
The prospects for future access to alimatravir got a major boost last week when the pharmaceutical company Merck (known as MSD outside of the United States and Canada) announced that it granted licences to seven different companies to produce generic versions of the monthly pill. One of the seven companies is South Africa’s Aspen Pharmacare. The others are Uganda’s Quality Chemical Industries Limited, Kenya’s Universal Corporation Ltd, and Aurobindo, Cipla, Emcure and Viatris in India.
Early responses to the licences have mostly been positive.
Having a generic company with a licence in South Africa is excellent news, said Bekker.
“It is particularly exciting to see manufacturers in Kenya, South Africa and Uganda included in these licenses,” Mitchell Warren, Executive Director of AVAC (a global HIV advocacy group), told Spotlight by e-mail. “These are the first generic PrEP licenses in East and Southern Africa, meaning manufacturing can happen where trials are happening, where need is greatest and where we have the largest PrEP markets.”
“Through our agreement with MSD (Merck), we have the opportunity to support the future supply of an innovative HIV prevention option while strengthening local pharmaceutical manufacturing and healthcare resilience across the continent,” Stephen Saad, Aspen Group Chief Executive, said in a media statement. Under the agreement, the company says it will receive a technical package from Merck, together with licensing rights covering 129 countries, including all African countries.
Speaking to Spotlight, Stavros Nicolaou, Aspen’s Head of Strategic Trade, described alimatravir as “ground-breaking and a potential game-changer”. He commended Merk for starting the licensing process so early. He framed the licence as an important step forward for both South Africa’s HIV response and for local production of antiretrovirals, although he also raised concerns about the procurement of locally manufactured antiretrovirals – the percentage of South Africa’s antiretroviral tenders awarded to local manufacturers has been trending downward.
According to earlier reporting by Business Day, Nicolaou has declined to give any indication as to a potential price for the pill, but he did tell the publication that they could potentially supply it for both South Africa’s public and private sectors.
There are indications that a relatively low price is on the cards. Research being presented at AIDS 2026 this week found that alimatravir could be mass produced and sold at a profit for as little as $15 (around R250 to R300) per person per year. This is less than half the $40 per person per year that South Africa is expected to pay for generic lenacapavir injections in a year or two from now.
“Merck expects to provide initial supply and continue supplying product as needed while licensed generic manufacturers complete development, obtain the necessary regulatory approvals and prepare to provide supply in the licensed territories. The goal is to help avoid delays in access by providing an initial supply pathway until generic manufacturing capacity is established and brought online,” the company said in a media statement.
Earlier licensing
The timing of the licensing announcement is somewhat unusual – such announcements are typically only made after phase 3 trials have been concluded and it is confirmed that the drug is safe and effective.
“Granting licensing agreements to generic manufacturers while clinical trials are still enrolling, before it is known if the product is effective, should significantly reduce the time to market for the product,” Warren said in an earlier AVAC media statement. “The timeline announced today gives us ample opportunity to work with ministries of health, donors, communities, and Merck to plan for broad access to the monthly PrEP pill.”
Warren told Spotlight that the small amount of active drug in alimatravir and the fact that it is an oral dose should make the technology transfer from Merck to generics quite quick. “The hope would be that genetic alimatravir reaches the market within months of the approval of the originator, compared to more than a year for lenacapavir,” he said.
Nicolaou was also upbeat about how quickly things are unfolding. He said that Merck’s decision to execute licences while the phase 3 clinical trials are ongoing allows for an earlier registration pathway (if phase 3 findings are positive, alimatravir will have to be filed for registration with regulators like the South African Health Products Regulatory Authority). He also pointed out that it is a small tablet and that it should be easier to manufacture than HIV prevention injections.
Nicolaou told Spotlight that the plan is for Aspen to do formulation of alimatravir in South Africa, but that they are not currently planning to produce the active pharmaceutical ingredient – this will likely be sourced from Chinese or Indian suppliers.
Some activist criticism
But while the timing has generally been welcomed, there has also been some criticism over the licenses.
A statement from activist group HealthGap points out that Latin American countries like Brazil, Argentina, and Colombia are not included in the list of 129 countries covered by the license, even though some of the phase 3 trial sites for alimatravir are in these countries. The HealthGap statement calls for compulsory licenses to be issued.
In an earlier statement, Merck said that, in recognition of the significant unmet need in Latin America, “Merck is in active discussions with organizations, including Fiocruz (a key player in medicines production and procurement in Brazil), with a goal to enable rapid availability and broad supply of alimatravir in the region”.
Disclosure: The Gates Foundation has provided financial support for clinical trials of alimatravir. Spotlight receives funding from the Gates Foundation, but is editorially independent – an independence the editors guard jealously. Spotlight is a member of the South African Press Council.
*This story was published by Spotlight – health journalism in the public interest. Sign up to the Spotlight newsletter.





