Researchers have discovered why influenza can lead to life-threatening complications during pregnancy.
Source: Pixabay CC0
In most people, influenza stays in the upper respiratory tract – mainly the nose – and clears without spreading further. But during pregnancy, the virus can extend beyond the lungs into the cardiovascular system, increasing the risk of severe complications for mothers and babies.
Now a new preclinical study using animal models reveals precisely why the virus can spill into the bloodstream during pregnancy, opening the door for targeted treatment. The study is a bilateral partnership between Trinity College Dublin, with collaborators from RMIT University and the University of Adelaide and is published in Science Advances.
Researchers identified a viral sensor in the immune system, known as TLR7, that can become overactive during pregnancy, amplifying inflammation and spreading disease into the bloodstream.
Blocking TLR7 could help prevent the harmful inflammation that makes flu in pregnancy so dangerous. This work can help protect developing babies by stopping the placenta from becoming overly inflamed during flu infection.
Professor John O’Leary, School of Medicine, Trinity, said: “This international research is of high impact in relation to our understanding of viruses and pregnancy and the role of the maternal immune response.”
What is the potential impact of this research?
Earlier studies from RMIT have shown that severe flu in pregnancy can have long‑term impacts on babies’ brain development, by inflaming blood vessels and reducing the flow of oxygen and nutrients from mother to baby.
This new study pinpoints the underlying cause of that damage, reshaping our understanding of flu‑related risk in pregnancy and opening the door to more targeted therapies.
RMIT co-lead author, Prof. Stavros Selemidis, said future treatments could focus on the immune system rather than the virus itself.
“Our study shows that in pregnancy, the problem isn’t just the flu virus – it’s the immune system overreacting. That’s where future treatments could really make a difference,” he explained.
“We’re ready to work with partners to help develop the next generation of therapies and clinical guidelines.”
Next steps for this work: The team is planning further research on how to target TLR7 to reduce the risk of severe influenza and pregnancy complications.
Memory cells in the nose slow the influenza virus as soon as it enters the body. They reduce viral levels and may help protect against more severe illness. A new study from the University of Gothenburg may help guide the development of better influenza vaccines.
Today’s influenza vaccines are given as injections in the arm and mainly stimulate immune responses in the blood. At the same time, researchers are working to develop influenza vaccines that can be administered through the nose – an effort this study helps inform. The goal is to strengthen the body’s defences where the virus first encounters the immune system.
Memory cells remain in the nose
The researchers identified a group of memory cells, known as CD4 memory T cells, that remain in nasal tissue after an influenza infection. When the body encounters the virus again, these cells can rapidly reactivate and help other parts of the immune system fight the infection. The study shows that these cells can reduce viral replication in the nose and thereby contribute to better protection against illness.
“We show that CD4 memory T cells can remain in nasal tissue after an influenza infection and rapidly reactivate when the virus returns. This means the immune system can respond directly at the site where the virus first enters the body,” says Nimitha R. Mathew, a researcher at the Sahlgrenska Academy, University of Gothenburg, and one of the study’s lead authors.
In studies in mice, the researchers showed that these immune cells help limit viral levels and reduce tissue damage in the nose during a subsequent infection.
Similar cells found in humans
The researchers also analysed cells from the nasal mucosa of healthy adults. There, they found the same type of influenza-specific memory cells, suggesting that a similar local immune defence may also exist in humans. The study is published in the Journal of Experimental Medicine.
“Many people likely already have these kinds of memory cells in their noses after previous infections, but they are not always enough to stop the virus completely. The important thing about our findings is that we now know which immune cells can limit the virus where infection begins. That knowledge can be used when developing future nasal vaccines,” says Davide Angeletti, professor at the Sahlgrenska Academy, University of Gothenburg, and also one of the study’s lead authors.
Article: Nasal CD4⁺ tissue resident memory T cells provide cross protective immunity to influenza; 10.1084/jem.20251793
Many regions in the Northern Hemisphere experienced a slightly earlier start to their flu season, driven in some part by a novel variant of influenza A(H3N2). As our flu season also kicks off slightly earlier than usual, Spotlight reports on the detection of this variant in South Africa and what we might expect from this year’s flu season.
As the mercury slowly starts dropping across the country, so does the risk of picking up flu. For many, this might only mean a few days of illness and discomfort, but for some, especially the elderly, it can be life-threatening.
Despite temperatures throughout most of the country remaining moderate so far, this year’s flu season has started, somewhat ahead of schedule. This is according to the National Institute for Communicable Diseases (NICD) in a press release issued on Wednesday.
What we refer to as flu, is commonly caused by one of two types of influenza viruses, influenza A and influenza B. These two are further typed into different lineages, the most common for influenza A is A(H1N1) and A(H3N2) and for influenza B, the B-Victoria and B-Yamagata.
The Yamagata lineage has not been detected since 2020 and is thought to have gone extinct, said Dr Sibongile Walaza. She is a medical epidemiologist and head of epidemiology at the Centre for Respiratory Disease and Meningitis at the NICD.
A key reason why influenza viruses continue to circulate year after year is how fast they mutate and learn to dodge our immune defenses. These mutations eventually result in different subtypes of lineages that are called clades, within which there can be further sub-clades.
It was a sub-clade of the A(H3N2) virus, known as sub-clade K, that led to the flu season starting earlier than usual in some parts of the Northern Hemisphere. The World Health Organization (WHO) reported that the variant was identified in 2025 and spread fast.
“This [sub-clade] contributed to an earlier start to the influenza season in many countries, with several reporting higher‑than‑usual levels of activity. ‘Subclade K’ accounted for the majority of influenza viruses reported across regions,” the WHO stated in a press release.
Sub-clade K was also responsible for an unusual spike in flu cases in South Africa in October and November 2025. Walaza told Spotlight there weren’t enough flu cases detected to cross the seasonal threshold for an additional flu wave, but the increase so late in the year, outside of the typical flu season, was unusual.
Early start
Usually, South Africa’s flu season starts sometime in April or May and spans the winter months, said Walaza, but it is difficult to predict exactly what will happen in any particular year.
This year’s flu season officially started in the second week of March, according to the NICD’s latest report, albeit at a low transmission level for now. 134 samples were tested between 16 and 22 March. Of those, 12 (9%) tested positive for influenza, 12 (9%) were cases of RSV and 3 (2.2%) tested positive for SARS-CoV-2.
In a rather unusual occurrence, the NICD reported that the start of this year’s RSV season coincided with that of the flu season. RSV refers to respiratory illness caused by the Respiratory syncytial virus. The RSV season usually starts before the flu season, but infections can occur all year round.
“The fact that both the flu and RSV seasons are starting at the same time means clinicians could potentially see a high burden of patients with respiratory illness in medical facilities in the coming weeks,” the NICD said in the press release.
Two potential scenarios
Professor Tulio de Oliveira, the director of the Center for Epidemic Response Innovation at Stellenbosch University, said the reality is that we do not know what to expect for this year’s flu season.
“[At]t the moment, we are working with potentially two different scenarios,” he told Spotlight.
The one scenario is that we may be in for a more extreme flu season, he explained, since last year was an unusually mild season and population immunity against the viruses that cause flu may currently be lower. The other scenario, depending on which flu virus circulates, is that South Africa may have some herd immunity because of the unusual spike in flu cases near the end of last year.
In other words, it all comes down to which flu viruses, and their subtypes end up circulating.
“I think this year we’ll have the three influenza lineages [A(H3N2), A(H1N1)pdm09 and influenza B-Victoria] circulating, but in terms of which one is going to be dominant in the season, it’s difficult to tell in advance,” Walaza said.
What we know about sub-clade K
Based on what we’ve seen so far, it does seem that sub-clade K is more transmissible, but it doesn’t appear to cause more severe disease, according to Walaza. De Oliveira added that sub-clade K has between seven and 10 mutations on the surface protein that allow it to bind to a cell’s receptor and enter the body, making it more infectious.
Whether or not it will be the driver of our flu season this year remains to be seen, but Walaza said that within the sporadic cases of flu detected and sequenced so far this year, most of the cases have been sub-clade K. In an NICD report from March, of the 24 influenza samples that were sequenced between 29 December 2025 and 22 March 2026, 11 were confirmed as being sub-clade K.
Experts will be keeping a close eye on circulating flu viruses with real-time genomic surveillance.
“South Africa is considered to be one of the top virus genomic surveillance places in the world,” De Oliveira said. “[A]t the moment, we don’t see a big reason for concern [about the flu season],” he said. “We do genomic surveillance every week, both with public and private laboratories – and if we see anything unusual, that’s going to be highlighted very promptly.”
Trends seen in previous flu seasons
Overall, in the last ten years, influenza A seems to be the driver of the majority of flu cases in South Africa, said De Oliveira, usually causing a big wave of flu cases at the start of the season. This is usually followed by a smaller wave of influenza B cases. In this time period, the influenza A subtype that dominates during the flu season appears to alternate between A(H1N1) one year and A(H3N2) the following year, but it also doesn’t always follow this pattern.
Zooming in more closely, Walaza said that over the last six years, 2020 and 2021 were outliers, with reduced transmission during 2020 due to the measures taken to curb the spread of the SARS-CoV-2 virus and out of season influenza transmission in 2021. Since 2022, the number of people getting flu every year has returned to roughly similar levels as before 2020.
Last year’s flu season was slightly unusual since it had started in late March, according to Walaza, but wasn’t as intense as some of the previous years as transmission remained at a low threshold level. Flu cases peaked in mid-May and then rose again slightly in October and November.
Data on influenza comes from three sentinel monitoring programmes managed by the NICD, which cover both the public and private healthcare sectors, said Walaza. A sample of healthcare facilities in the public sector and doctors in the private sector are asked to supply swabs taken from people with influenza-like illnesses or respiratory illnesses. Some general practitioners in the private sector are also enrolled in a programme called Viral Watch.
She said that the swabs are sent to the NICD laboratory and tested for the presence of different viruses, including SARS-CoV-2, influenza, RSV, parainfluenza, human metapneumovirus and rhinoviruses. If the samples test positive for flu, the sample is further tested to identify the lineage. This data is included in the weekly reports published on their website.
Members of the public can contribute to flu surveillance through an online web platform called CoughWatch. People are invited to enroll and provide weekly information on whether they have symptoms of flu or other respiratory illnesses. This is aimed at picking up trends among people who aren’t necessarily getting sick enough to go to the doctor or clinic, said Walaza and can hopefully serve as an early warning system for increases in respiratory illnesses, including flu.
CoughWatch has already opened for enrollment this year. (More information can be found here).
Flu vaccination uptake in South Africa remains low
Each year, the WHO releases recommendations on what should be in upcoming flu vaccines for the Northern Hemisphere and then later the Southern Hemisphere, usually announced around six months before the start of the respective flu seasons.
This year’s flu shot’s formulation is a trivalent one, said Walaza meaning it contains inactivated strains of all three influenza strains, including coverage for the A(H3N2) sub-clade K. Because it contains an inactivated virus, the vaccine itself cannot give someone the flu.
The level of protection offered by flu shots vary, but generally it ranges in effectiveness against preventing infection from about 30% to 60%. This means the shot will offer most people protection from severe disease and death, but it won’t necessarily prevent them from getting sick with the flu altogether.
One of the things that makes it difficult to predict effectiveness ahead of time is the possibility that a strain might circulate that is not well covered by the flu shot. De Oliveira said this “mismatch” is what we saw play out in some of the regions in the Northern Hemisphere in their last flu season.
Despite the partial mismatch between the vaccine used in the northern hemisphere and sub-clade K, several surveillancereports from the Northern hemisphere show that the vaccine nevertheless provides some protection against severe flu caused by sub-clade K.
The WHO also recently touched on this, saying that: “While current influenza vaccines help reduce the burden of disease, their effectiveness can vary by season, product, and population group. Protection is limited to one season”. The majority of flu vaccines purchased each year are by upper-middle and high-income countries, the WHO noted.
Usually, South Africa’s National Department of Health procures about 1 million flu shots for the public health sector, said Walaza and sometimes not all these doses are used.
While flu shots are made available each year, the uptake of these shots in the private sector appears to be low. Based on data collected through the NICD’s Viral Watch initiative – last year the uptake of the influenza vaccine in the private sector, among those enrolled in the programme, was only around 3.4%. This is based on data collected from 768 people enrolled, of those, 26 had gotten a flu shot. As far as Spotlight could establish, there currently isn’t any routine publicly available data on uptake in the public sector. One study of around a thousand people aged 65 and older, found that just over 32% of them had gotten the flu jab in 2018.
Spotlight asked the National Department of Health how many flu vaccines were procured for this year’s flu season. A response had not been received by the time of publication.
Low flu vaccine uptake can in part be attributed to South Africa having much milder winters and less severe flu seasons than the Northern Hemisphere, said De Oliveira.
Lack of awareness of the flu vaccine can also play a role, according to Walaza. She encourages more education and efforts by healthcare workers to inform at risk groups of the flu shot and when it will be available.
The flu shot is recommended for people who are at risk of severe disease, including older persons, pregnant women, people who are immunocompromised or with chronic medical conditions, as well as healthcare workers. But anyone aged six months and older can get the shot.
“The influenza vaccine will be available in pharmacies from the first week of April. The early start to the season means that this year, the vaccine is only becoming available as the season is getting started, so members of the public who fall into groups at high risk for severe influenza are urged to get their vaccines as soon as possible,” the NICD press release stated.
The potential of next generation flu vaccines
Earlier this year, the WHO released results from an assessment report on the value of having improved flu vaccines. “If improved, next-generation, or universal influenza vaccines are available and widely used between 2025 and 2050, they could prevent up to [an estimated]18 billion cases of influenza and save up to 6.2 million lives globally,” the report stated.
“This assessment makes clear the potential benefits that improved influenza vaccines could offer across different settings,” said Dr Philipp Lambach, WHO technical lead of the project. “It provides all those working on future influenza vaccine investments, policy development and research priorities a common set of evidence to catalyse vaccine development.”
According to the WHO, as of February 2026, there are 46 next-generation influenza vaccines in clinical development.
Researchers from University of Maryland Schools of Public Health and Engineering in College Park and the School of Medicine in Baltimore wanted to find out how the flu spreads, so they put college students already sick with the flu into a hotel room with healthy middle-aged adult volunteers. The result? No one caught the flu.
“At this time of year, it seems like everyone is catching the flu virus. And yet our study showed no transmission – what does this say about how flu spreads and how to stop outbreaks?” said Dr Donald Milton, professor at SPH’s Department of Global, Environmental and Occupational Health and a global infectious disease aerobiology expert who was among the first to identify how to stop the spread of COVID-19.
The study, out in PLOS Pathogens, is the first clinical trial in a controlled environment to investigate exactly how the flu spreads through the air between naturally infected people (rather than people deliberately infected in a lab) and uninfected people. Milton and his colleague Dr Jianyu Lai have some ideas about why none of the healthy volunteers contracted the flu.
“Our data suggests key things that increase the likelihood of flu transmission – coughing is a major one,” said Lai, post-doctoral research scientist, who led data analysis and report writing for the team.
The students with the flu had a lot of virus in their noses, says Lai, but they did not cough much at all, so only small amounts of virus got expelled into the air.
“The other important factor is ventilation and air movement. The air in our study room was continually mixed rapidly by a heater and dehumidifier and so the small amounts of virus in the air were diluted,” Lai said.
Lai adds that middle-aged adults are usually less susceptible to influenza than younger adults, another likely factor in the lack of any flu cases.
Most researchers think airborne transmission is a major factor in the spread of this common disease. But Milton notes that updating international infection-control guidelines requires evidence from randomised clinical trials such as this one. The team’s ongoing research aims to show the extent of flu transmission by airborne inhalation and exactly how that airborne transmission happens.
The lack of transmission in this study offers important clues to how we can protect ourselves from the flu this year.
“Being up close, face-to-face with other people indoors where the air isn’t moving much seems to be the most risky thing – and it’s something we all tend to do a lot. Our results suggest that portable air purifiers that stir up the air as well as clean it could be a big help. But if you are really close and someone is coughing, the best way to stay safe is to wear a mask, especially the N95,” said Milton.
The team used a quarantined floor of a Baltimore-area hotel to measure airborne transmission between five people with confirmed influenza virus with symptoms and a group of 11 healthy volunteers across two cohorts in 2023 and 2024. A similar quarantine set-up was used in an earlier study and exhaled breath testing was used in several pioneering studies by Milton and colleagues on influenza transmission.
During the most recent flu study, participants lived for two weeks on an isolated floor of the hotel, and did daily activities simulating different ways that people gather and interact – including conversational ice-breakers, physical activities like yoga, stretching or dancing. Infected people handled objects such as a pen, tablet computer and a microphone, before passing the objects among the whole group.
Researchers measured a wide range of parameters throughout the experiment, including participant symptom monitoring, daily nasal swabs and saliva samples and blood collection to test for antibodies. The study measured the viral exposure in volunteers’ breathing area as well as the ambient air of the activity room. Participant exhaled breath was also measured daily in the Gesundheit II machine, invented by Milton and colleagues at Harvard T.H. Chan School of Public Health.
Finding ways to control flu outbreaks is a public health priority, says Milton. Flu is responsible for a considerable burden of disease in the United States and globally – up to 1 billion people across the planet catch seasonal influenza every year and this season has seen at least 7.5 million flu cases so far in the United States alone, including 81 000 hospitalisations and over 3000 deaths.
NHS doctors are going on strike just as the UK is facing a surge in cases of “superflu”, which would have by itself placed an even greater burden than the public health service usually faces this time of year as services are stretched thin.
According to The Guardian, this is the 14th such action since disputes over junior doctors’ pay and jobs began in March 2023. Since then, they have won the right to be called “resident doctors” in line with the US because the British Medical Association (BMA) felt that the previous term was demeaning and misleading.
Resentment between government and doctors grows
After the government’s last offer was rejected, BMA members voted in an online ballot 84% in favour of industrial action. UK Prime Minister Keir Starmer called the walkouts “irresponsible” amid a surge in super-flu cases. Meanwhile, the UK’s Secretary of State for Health and Social Care, Wes Streeting, asked junior doctors to ignore the BMA and show up for work. He dismissed the resident doctors’ 26% pay claim as a “fantasy demand”, and has also said that the strike could be “the Jenga piece” that finally brings about the collapse of the NHS just when it is needed the most.
The strike will begin on Wednesday 17th December at 7am and will continue until the following Monday at 7am.
The magnitude of the problem has echoes of South Africa’s own struggles to find training placements – but at a far larger scale. Some 30 000 newly graduated doctors are having to compete for around 10 000 training posts. Even the government’s best offer could only add 2000 extra jobs.
Dr Jack Fletcher, the chair of the BMA’s resident doctors committee, said: “There are no new jobs in this offer. He has simply cannibalised those jobs which already existed for the sake of ‘new’ jobs on paper. Neither was there anything on what Mr Streeting has said is a journey to restoring our pay – that has clearly hit the buffers.”
Is ‘superflu’ even real?
Experts have however cast doubt on the UK government’s narrative of a dangerous new influenza mutation a “superflu”. Mathematician Christina Pagel, University College London professor, said that the “superflu” term was based on “highly misleading statistics” and that the flu season had merely arrived a few weeks early.
Government spin or not, the strikes have sounded alarm in the NHS, which is struggling to deal cope with a record flu hospitalisations for this time of year, filling 1700 beds. More and more hospitals are unable to contend with these numbers and having to declare a “critical incident”.
A hormone known for regulating energy balance also helps the body cope with influenza by triggering protective responses in the brain, a study led by UT Southwestern Medical Center researchers shows. The findings, published in the Proceedings of the National Academy of Sciences (PNAS), suggest that targeting this pathway could offer a new pharmacological approach for treating the flu.
“Our work demonstrates that FGF21, a stress-induced hormone that regulates whole-body metabolism, acts on the brain to protect against the hypothermia and weight loss caused by influenza infection,” said senior author Steven Kliewer, PhD, Professor of Molecular Biology and Pharmacology at UT Southwestern.
The study found that levels of fibroblast growth factor 21 (FGF21) rose in both humans and mice during flu infection. In mice, the hormone activated a brain region that regulates the noradrenergic nervous system, prompting heat production from tissues that help regulate body temperature in mice.
This thermogenic response helped stabilise body temperature and improved the response to flu infection. Mice lacking FGF21 or its receptor in these neurons recovered more slowly, while treatment with pharmacologic FGF21 improved recovery. The hormone did not change viral levels, indicating that it protects the body by mitigating the physiological stress of infection rather than directly targeting the virus. Collectively, these results suggest FGF21 could help the body respond more effectively to a range of infections, not just influenza.
“For serious cases of influenza infection, the care is mostly supportive,” Dr Kliewer said. “Our findings suggest a new pharmacological approach for treating the flu. Further studies are required to determine if these findings are applicable to other infections.”
The research builds on decades of work from the Mangelsdorf/Kliewer Lab at UTSW, which previously identified FGF21 as a hormone produced by the liver in response to metabolic stresses such as fasting and alcohol exposure. The new study extends that work to infection, showing that FGF21 uses the same liver-to-brain signalling pathway to help the body maintain metabolic balance during illness.
Scientists have discovered why older people are more likely to suffer severely from the flu, and can now use their findings to address this risk. In a new study published in PNAS, experts discovered that older people produce a glycosylated protein called apoplipoprotein D (ApoD), which is involved in lipid metabolism and inflammation, at much higher levels than in younger people. This has the effect of reducing the patient’s ability to resist virus infection, resulting in a more serious disease outcome.
The team established that highly elevated ApoD production with age in the lung drives extensive tissue damage during infection to reduce the protective antiviral type I interferon response.
The research was an international collaboration led by scientists from the China Agricultural University, University of Nottingham, Institute of Microbiology (Chinese Academy of Sciences), National Institute for Viral Disease Control and Prevention (Chinese Centre for Disease Control and Prevention) and the University of Edinburgh.
Aging is a leading risk factor in influenza-related deaths. Furthermore, the global population is aging at an unprecedented rate in human history, posing major issues for healthcare and the economy. So we need to find out why older patients often suffer more severely from influenza virus infection.”
Professor Kin-Chow Chang from the School of Veterinary Medicine and Science at the University of Nottingham, and co-author on the paper
In this new study, the team investigated the mechanisms behind increased severity of influenza virus infection with age using an aging-mouse model and appropriate donor human tissue sections.
They identified ApoD as an age-related cell factor that impairs the activation of the immune system’s antiviral response to influenza virus infection by causing extensive breakdown of mitochondria (mitophagy) resulting in greater production of virus and lung damage during infection. Mitochondria are essential for cellular production of energy and for induction of protective interferons.
ApoD is therefore a target for therapeutic intervention to protect against severe influenza virus infection in the elderly which would have a major impact on reducing morbidity and mortality in the aging population.
Professor Chang, added: “There is now an exciting opportunity to therapeutically ameliorate disease severity of the elderly from influenza virus infection by the inhibitory targeting of ApoD.”
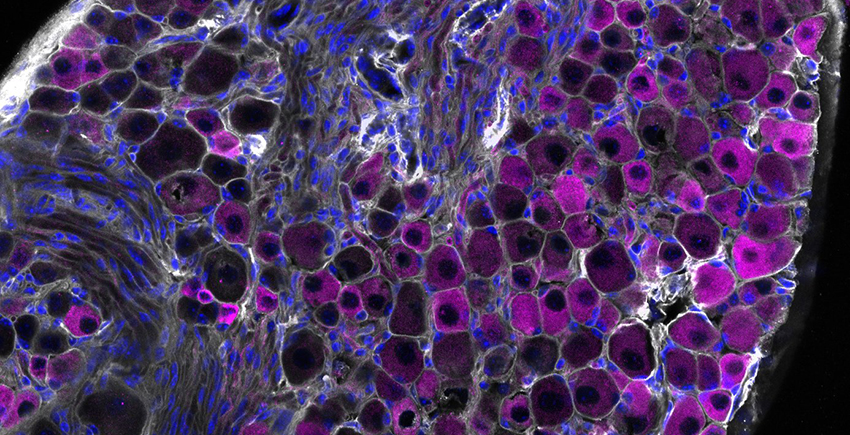
Study finds sensory cells that detect tissue damage, irritants also rein in harmful immune responses to protect the lungs
Clusters of mouse vagus nerve sensory cells reveal the presence of TRPV1, a molecular sensor that detects irritants, heat, and inflammation. A new HMS study reveals nerve cells with this sensor play a central role in taming inflammation and tissue damage in the lung during flu infection. Image: Chiu Lab.
A group of nerve cells known for their role in detecting chemical irritation, tissue damage, heat, and pressure now emerge as critical defenders against the worst ravages of the flu caused by an overactive immune response, according to new research by scientists at Harvard Medical School and the Harvard T.H. Chan School of Public Health.
The cells, called TRPV1 vagal nociceptors, live in the vagus nerve, which sends signals from internal organs – including the heart, lungs, and gut – to the brain to help regulate heart rate, breathing, digestion, and other functions. In the lungs, these cells trigger the protective cough reflex that forces the airways to expel foreign particles, mucus, and other irritants.
But the new research, published in Science Immunologyand conducted in mice, shows that in the setting of flu, these cells do much more – they rein in the immune system and avert the smoldering inflammation that often occurs in the aftermath of a viral infection and can injure healthy tissue.
Each year, the flu sickens millions and kills between 290 000 and 650 000 people worldwide, according to the World Health Organization. While the immune system helps fight off the virus, an excessive inflammatory response can inflict tissue damage and worsen illness. The findings are especially relevant in the wake of the COVID-19 pandemic, which revealed how an aberrant immune response following viral infection can sometimes lead to serious organ damage and even organ failure.
“Our research shows that the infected lung is a battleground where nerves and immune cells engage in a delicate dance to safeguard our health,” said co-senior study author Isaac Chiu, professor of immunology in the Blavatnik Institute at HMS. “Understanding this powerful neuro-immune signaling axis will be increasingly important as we design better ways to prevent and treat immune-mediated damage in viral infections, which can sometimes be worse than the direct damage caused by the virus itself.”
The findings, he added, raise the possibility that vagus nerve function may be one variable that explains why some people with the flu go on to develop long-lasting and devastating immune-driven damage in their lungs while others recover once the initial infection is resolved.
“Flu infections are highly variable in severity and there is a need to understand why certain groups of people, such as the elderly, experience worse disease,” said study first author Nicole Almanzar, a doctoral student in the Chiu Lab. “Our study demonstrates that the nervous system is actively involved in regulating the response of the lungs to infection, offering a new perspective on viral infections that could help explain why particular factors increase risk of severe infections.”
The new study illuminates the complex interaction between body and brain and adds to a growing body of research showing that the nervous and immune systems engage in highly orchestrated crosstalk during infection to modulate body defenses.
One of Chiu’s earlier studies found that during bacterial infections of the lung, the same set of vagal nerve neurons suppressed the immune defences. In the new study, however, the immune-taming function of these cells worked to shield the lung from excessive damage during viral infection.
“Context clearly matters,” Chiu said.
Disabling the neurons worsened flu damage in the lungs
In a set of experiments, researchers exposed a group of mice with genetically disabled or chemically silenced TRPV1 neurons to influenza A virus. Mice without these nerve cells fared notably worse than mice with functioning TRPV1 cells. Even though the overall amount of virus in the lungs was the same in both groups, mice lacking TRPV1 neurons suffered more severe lung pathology, higher levels of harmful inflammation, and lower survival rates. Interestingly, Almanzar noted, even though the overall viral load remained the same, the spread of the virus within the lobes of the lungs was more pronounced in mice without these protective neurons.
The researchers also found that the absence of TRPV1 neurons altered the lung’s immune landscape. The lungs of mice lacking these neurons had an overabundance of neutrophils and macrophages – two types of immune cells that, in excess, can worsen tissue damage. At the same time, interferon signalling – one of the body’s most important viral-defence pathways – was seriously impaired in these immune cells.
In another experiment, the researchers used an antibody to deplete inflammation-driving cells in flu-infected mice lacking TRPV1 neurons. These animals had notably better survival than untreated mice lacking these protective neurons. The observation further underscores how nerve cells help prevent harmful immune reactions that can sometimes be more dangerous than the virus itself.
The researchers noted that they do not yet know precisely how TRPV1 neurons restrain the march of inflammatory cells at the molecular level – a question they plan to explore in subsequent work.
“The vagus nerve is powerfully controlling inflammation, but how it does so remains a mystery to be solved,” Chiu said. “But we’re excited that it plays such a strong role in viral infections.”
Harnessing the immune brake for therapy
Moving forward, this insight opens the door to exciting new avenues for therapy. Instead of only targeting the flu virus or dampening immune activity, the research team said, future treatments could mimic the function of nerve cells to ensure the delicate balance between protective and damaging immune responses is not thrown off.
The idea is not that far-fetched, the researchers said, noting that the FDA recently approved a therapy for rheumatoid arthritis by vagus nerve stimulation.
“Imagine if you could harness this brake to control inflammation in the lungs and beyond,” Chiu said. “By stimulating related circuits where the vagus nerve shuts down immune cells, one could envision treating immune-mediated dysfunction of many kinds, including that caused by viral infections.”
In a potential game-changer for how we treat the flu, scientists at the Hebrew University of Jerusalem have unveiled a new drug pairing that outperforms oseltamivir – the most widely used anti-influenza medication – against even the deadliest flu strains, including bird(avian) and swine flu.
The surprising duo? One of them is theobromine, a compound found in chocolate.
In a study recently published in PNAS, researchers, led by Prof Isaiah (Shy) Arkin, have developed a novel combination therapy that targets a key weakness in the influenza virus: its ion channel, a microscopic gate the virus uses to replicate and spread. By blocking this gate, the team effectively cut off the virus’s ability to survive.
Their study, conducted at Israel’s new Barry Skolnick Biosafety Level 3 facility, tested this combo, consisting of theobromine and a lesser-known compound called arainosine, against a broad range of flu viruses. In both cell cultures and animal trials, the treatment dramatically outperformed oseltamivir (Tamiflu), especially against drug-resistant strains.
“We’re not just offering a better flu drug,” said Prof Arkin. “We’re introducing a new way to target viruses – one that may help us prepare for future pandemics.”
Why It Matters
The stakes are high: Influenza continues to sweep the globe each year, with unpredictable mutations that challenge vaccines and existing drugs. In the U.S. alone, seasonal flu costs an estimated $87 billion annually in healthcare and lost productivity. Past pandemics – like the 2009 swine flu – have inflicted even deeper global costs, and the cost of future pandemics was estimated to rise even further up to $4.4 trillion.
Meanwhile, outbreaks of avian flu have devastated poultry industries and sparked fears of cross-species transmission to humans. Just one recent outbreak in the U.S. led to the loss of 40 million birds and billions in economic damage.
Current flu treatments, like oseltamivir, are losing ground as the virus adapts. Most drugs in use target a viral protein that mutates frequently, rendering treatments less effective over time. That’s where Arkin’s team saw an opening.
A New Strategy for Old Viruses
Instead of fighting the virus head-on with traditional antivirals, the researchers zeroed in on the M2 ion channel – a crucial viral feature that helps the virus replicate. Past efforts to block this channel have largely failed due to drug resistance. But the new theobromine–arainosine combo sidesteps this resistance, even neutralising hard-to-treat strains.
The team discovered the combo by scanning a library of repurposed compounds, many originally developed for other diseases, and testing their effects on both drug-sensitive and drug-resistant versions of the virus.
Broader Implications
The implications extend beyond influenza. Because many viruses, including coronaviruses, also rely on ion channels, this new approach could form the basis of future antiviral strategies.
The next steps include human clinical trials, but the early results offer hope not just for a better flu treatment, but for a smarter way to fight viral disease in general. ViroBlock, a startup company emanating from the Hebrew University, has been entrusted to develop the discoveries to reach the public.
For decades, medical professionals debated whether a common antiviral medication used to treat flu in children caused neuropsychiatric events or if the infection itself was the culprit.
Now researchers at Monroe Carell Jr. Children’s Hospital at Vanderbilt have debunked a long-standing theory about oseltamivir, known as Tamiflu.
According to the study, published in JAMA Neurology, oseltamivir treatment during flu episodes was associated with a reduced risk of serious neuropsychiatric events, such as seizures, altered mental status and hallucination.
“Our findings demonstrated what many pediatricians have long suspected, that the flu, not the flu treatment, is associated with neuropsychiatric events,” said principal investigator James Antoon, MD, PhD, MPH, assistant professor of Pediatrics in the Division of Pediatric Hospital Medicine at Monroe Carell. “In fact, oseltamivir treatment seems to prevent neuropsychiatric events rather than cause them.”
Key points:
Influenza itself was associated with an increase in neuropsychiatric events compared to children with no influenza, regardless of oseltamivir use.
Among children with influenza, those treated with oseltamivir had about 50% reduction in neuropsychiatric events.
Among children without influenza, those who were treated with oseltamivir prophylactically had the same rate of events as the baseline group with no influenza.
“Taken together, these three findings do not support the theory that oseltamivir increases the risk of neuropsychiatric events,” said Antoon. “It’s the influenza.”
The team reviewed the de-identified data from a cohort of children and adolescents ages 5-17 who were enrolled in Tennessee Medicaid between July 1, 2016, and June 30, 2020.
During the four-year period, 692 295 children, with a median age of 11 years, were included in the study cohort. During follow-up, study children experienced 1230 serious neuropsychiatric events (898 neurologic and 332 psychiatric).
The clinical outcomes definition included both neurologic (seizures, encephalitis, altered mental status, ataxia/movement disorders, vision changes, dizziness, headache, sleeping disorders) and psychiatric (suicidal or self-harm behaviours, mood disorders, psychosis/hallucination) events.
“The 2024-2025 influenza season highlighted the severity of influenza-associated neurologic complications, with many centres reporting increased frequency and severity of neurologic events during the most recent season,” said Antoon. “It is important for patients and families to know the true risk-benefit profile of flu treatments, such as oseltamivir, that are recommended by the American Academy of Pediatrics.”
“These flu treatments are safe and effective, especially when used early in the course of clinical disease,” added senior author Carlos Grijalva, MD, MPH, professor of Health Policy and Biomedical Informatics at Vanderbilt University Medical Center.
Investigators hope the findings will provide reassurance to both caregivers and medical professionals about the safety of oseltamivir and its role in preventing flu-associated complications.