A group of infectious disease and public health experts are calling on the Department of Health and Minister Aaron Motsoaledi to reintroduce a national action plan addressing antimicrobial resistance (AMR).
An open letter from over 70 doctors, scientists and public health advisors states that antibiotic resistance is becoming a “growing threat” in the country and poses a threat to universal health coverage through the National Health Insurance.
Latest figures show that over one-million deaths a year worldwide are directly caused by AMR. This number is projected to increase. Nearly five-million people die with an antibiotic-resistant infection. Over the next 25 years, nearly 40-million people are projected to die from AMR.
The open letter also called on the department to reinstate a ministerial advisory committee on AMR or to establish a similar scientific body.
“The lack of a robust scientific advisory body limits the government’s capacity to develop evidence-based policies,” the letter reads. The establishment of a scientific body would “empower the government to make strategic, data-driven decisions to combat this pressing health threat effectively”.
The former Ministerial Advisory Committee was disbanded in November 2023.
Marc Mendelson, an infectious disease specialist at Groote Schuur Hospital who has been outspoken about the threat of AMR for many years, said: “AMR is a current pandemic which is wreaking havoc, is not being attended to properly and not being taken seriously enough in South Africa.”
Mendelson said that there are “more and more people having to be treated for highly resistant bacterial infections in our healthcare system”. AMR leads to an increase in morbidity, mortality, hospital costs, and also has socio-economic consequences, he said. Common medical interventions such as surgery “becomes much riskier” with AMR.
Department of Health spokesperson Foster Mohale said that the department would only comment once the letter was formally presented, which is expected to happen at 5pm on Thursday.
Self-esteem scores more than doubled within one year of weight-loss surgery, according to a new study* presented at the American Society for Metabolic and Bariatric Surgery (ASMBS) 2025 Annual Scientific Meeting.
Researchers from Geisinger Medical Center found that after bariatric surgery self-esteem scores rose to 77.5 from 33.6 – a more than 40-point increase. The higher the score on a scale from 0 to 100, the higher the level of self-esteem and quality of life. The amount of weight loss appears to fuel the increase in self-esteem — scores were highest among those who lost the most weight despite demographics differences including gender, age, and race or type of bariatric procedure.
Researchers used a prospectively maintained database to identify 5,749 patients aged 18 and older with body mass index (BMI) of 35 or more who had metabolic and bariatric surgery between 2006 and 2019. Patients completed the Impact of Weight Quality of Life (iwQOL) survey pre-operatively and 12 months after the operation to assess weight stigma and their quality of life.
“Understanding weight stigma and psychosocial factors associated with obesity is essential to offering holistic care. While these factors should not dictate the decision to have bariatric surgery, they should be an important part of the conversation,” said study co-author Justin Dhyani, MD, Geisinger Medical Center in Danville, PA.
Weight stigma is associated with adverse health outcomes including depression, anxiety, disordered eating, and low self-esteem. Among adults with obesity, the prevalence of weight discrimination is 19% to 42%, with higher rates reported among those with higher BMIs and women.
“Weight stigma is a serious issue that places an extra psychological burden on patients struggling with obesity and there is no excuse for it,” said Ann M. Rogers, MD, MD, FACS, FASMBS, President, ASMBS, who was not involved in the study. “This study shows we need to understand what patients are going through and be supportive and empowering of them as they navigate their health and make decisions about treatment.”
Genetic material shed by tumours can be detected in the bloodstream three years prior to cancer diagnosis, according to a study led by investigators at Johns Hopkins.
The study, partly funded by the National Institutes of Health, was published in Cancer Discovery.
Investigators were surprised they could detect cancer-derived mutations in the blood so much earlier, says lead study author Yuxuan Wang, MD, PhD, an assistant professor of oncology at the Johns Hopkins University School of Medicine. “Three years earlier provides time for intervention. The tumours are likely to be much less advanced and more likely to be curable.”
To determine how early cancers could be detected prior to clinical signs or symptoms, Wang and colleagues assessed plasma samples that were collected for the Atherosclerosis Risk in Communities (ARIC) study, a large National Institutes of Health-funded study to investigate risk factors for heart attack, stroke, heart failure and other cardiovascular diseases. They used highly accurate and sensitive sequencing techniques to analyse blood samples from 26 participants in the ARIC study who were diagnosed with cancer within six months after sample collection, and 26 from similar participants who were not diagnosed with cancer.
At the time of blood sample collection, eight of these 52 participants scored positively on a multicancer early detection (MCED) laboratory test. All eight were diagnosed within four months following blood collection. For six of the eight individuals, investigators also were able to assess additional blood samples collected 3.1–3.5 years prior to diagnosis, and in four of these cases, tumour-derived mutations could also be identified in samples taken at the earlier timepoint.
“This study shows the promise of MCED tests in detecting cancers very early, and sets the benchmark sensitivities required for their success,” says Bert Vogelstein, MD, Clayton Professor of Oncology, co-director of the Ludwig Center at Johns Hopkins and a senior author on the study.
“Detecting cancers years before their clinical diagnosis could help provide management with a more favourable outcome,” adds Nickolas Papadopoulos, PhD, professor of oncology, Ludwig Center investigator and senior author of the study. “Of course, we need to determine the appropriate clinical follow-up after a positive test for such cancers.”
While scientists have long known that different senses activate different parts of the brain, a new Yale-led study indicates that multiple senses all stimulate a critical region deep in the brain that controls consciousness.
The study, published in the journal NeuroImage, sheds new light on how sensory perception works in the brain and may fuel the development of therapies to treat disorders involving attention, arousal, and consciousness.
In the study, a research team led by Yale’s Aya Khalaf focused on the workings of subcortical arousal systems, brain structure networks that play a crucial role in regulating sleep-wake states. Previous studies on patients with disorders of consciousness, such as coma or epilepsy, have confirmed the influence of these systems on states of consciousness.
But prior research has been largely limited to tracking individual senses. For the new study, researchers asked if stimuli from multiple senses share the same subcortical arousal networks. They also looked at how shifts in a subject’s attention might affect these networks.
For the study, researchers analysed fMRI (functional magnetic resonance imaging) datasets collected from 1,561 healthy adult participants as they performed 11 different tasks using four senses: vision, audition, taste, and touch.
They made two important discoveries: that sensory input does make use of shared subcortical systems and, more surprisingly, that all input, regardless of which sense delivered the signal, stimulates activity in two deep brain regions, the midbrain reticular formation and the central thalamus, when a subject is sharply focused on the senses.
The key to stimulating the critical central brain regions, they found, were the sudden shifts in attention demanded by the tasks.
“We were expecting to find activity on shared networks, but when we saw all the senses light up the same central brain regions while a test subject was focusing, it was really astonishing,” said Khalaf, a postdoctoral associate in neurology at Yale School of Medicine and lead author of the study.
The discovery highlighted how key these central brain regions are in regulating not only disorders of consciousness, but also conditions that impact attention and focus, such as attention deficit hyperactivity disorder. This finding could lead to better targeted medications and brain stimulation techniques for patients.
“This has also given us insights into how things work normally in the brain,” said senior author Hal Blumenfeld, the Mark Loughridge and Michele Williams Professor of Neurology who is also a professor in neuroscience and neurosurgery and director of the Yale Clinical Neuroscience Imaging Center. “It’s really a step forward in our understanding of awareness and consciousness.”
Looking across senses, this is the first time researchers have seen a result like this, said Khalaf, who is also part of Blumenfeld’s lab.
“It tells us how important this brain region is and what it could mean in efforts to restore consciousness,” she said.
The potential role of vitamin D in preventing and treating colorectal cancer (CRC) has attracted growing research interest – especially as CRC rates are rising, particularly among younger adults. This isn’t a new area of study. Low vitamin D levels have long been linked to a higher risk of developing colorectal cancer.
One large study involving over 12 000 participants found that people with low blood levels of vitamin D had a 31% greater risk of developing CRC compared to those with higher levels. Similarly, another study reported a 25% lower CRC risk among individuals with high dietary vitamin D intake.
Data from the Nurses’ Health Study – a long-term investigation of American nurses – showed that women with the highest vitamin D intake had a 58% lower risk of developing colorectal cancer compared to those with the lowest intake.
Now, a review highlights vitamin D’s promise in colorectal cancer prevention and treatment – but also underscores the complexity and contradictions in current research.
While observational data, which follow people’s use of vitamin D, and mechanistic studies, to investigate how vitamin D works in the laboratory, suggest protective effects, this isn’t confirmed by larger trials.
In fact, randomised controlled trials (RCTs), in which some people receive vitamin D and others don’t, the gold standard by which treatments are judged, reveal inconsistent outcomes. This highlights the need for a balanced approach to its integration into public health strategies.
Vitamin D is synthesised in the skin in response to sunlight and exerts its biological effects through vitamin D receptors (VDRs) found throughout the body, including in colon tissue. When activated, these receptors help regulate gene activity related to inflammation, immune response and cell growth – processes central to cancer development and progression.
Preclinical studies have shown that the active form of vitamin D (calcitriol) can suppress inflammation, boost immune surveillance (the immune system’s ability to detect abnormal cells), inhibit tumour blood vessel growth and regulate cell division – a key factor in cancer development, as demonstrated in my recent research.
Epidemiological studies, which track health outcomes across large populations over time, consistently find that people with higher blood levels of vitamin D have a lower risk of developing CRC. This paints a hopeful picture, suggesting that something as simple as getting more vitamin D – via sun exposure, diet, or supplements – could lower cancer risk.
But the story gets more complicated.
Mixed results
When it comes to medical decision-making, randomised controlled trials (RCTs) are the gold standard. These studies randomly assign participants to receive either a treatment (like vitamin D) or a placebo, helping eliminate bias and isolate cause-and-effect relationships.
Unfortunately, RCTs on vitamin D and CRC have produced mixed results.
For example, the VITAL trial – a major RCT involving over 25 000 participants – found no significant reduction in overall colorectal cancer incidence with 2000 IU/day of vitamin D supplementation over several years.
However, a meta-analysis of seven RCTs did show a 30% improvement in CRC survival rates with vitamin D supplements, suggesting potential benefits later in the disease course rather than for prevention.
On the other hand, the Vitamin D/Calcium Polyp Prevention Trial found no reduction in the recurrence of adenomas (pre-cancerous growths) with supplementation, raising questions about who benefits most, and at what dosage.
Adding to the uncertainty is the question of causation. Does low vitamin D contribute to cancer development? Or does the onset of cancer reduce vitamin D levels in the body? It’s also possible that the observed benefits are partly due to increased sunlight exposure, which itself may have independent protective effects.
The big picture
These discrepancies highlight the importance of considering the “totality of evidence” – treating each study as one piece of a larger puzzle.
The biologic plausibility is there. Observational and mechanistic studies suggest a meaningful link between vitamin D and lower CRC risk. But the clinical evidence isn’t yet strong enough to recommend vitamin D as a standalone prevention or treatment strategy.
That said, maintaining sufficient vitamin D levels – at least 30ng/mL – is a low-risk, cost-effective health measure. And when combined with other strategies like regular screening, a healthy diet, physical activity, and personalised care, vitamin D could still play a valuable role in overall cancer prevention.
Vitamin D is not a miracle cure – but it is part of a much broader picture. Its role in colorectal cancer is promising but still being defined. While it’s not time to rely on supplements alone, ensuring adequate vitamin D levels – through sun exposure, diet, or supplements – remains a smart choice for your health.
Colorectal cancer is a complex disease, and tackling it requires an equally nuanced approach. For now, that means focusing on evidence-based lifestyle changes, regular screenings, and staying informed as new research unfolds.
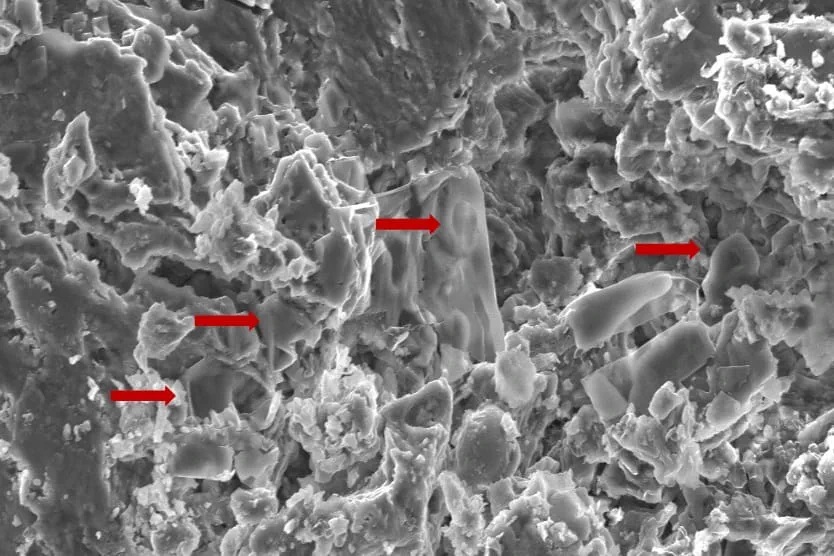
New study highlights the importance of preserving fossilised soft tissues
An image of fossilised erythrocyte-like structures. Credit: Anglia Ruskin University
New techniques used to analyse soft tissue in dinosaur fossils may hold the key to new cancer discoveries, according to a new study published in the journal Biology.
Researchers from Anglia Ruskin University (ARU) and Imperial College London analysed dinosaur fossils using advanced paleoproteomic techniques, a method that holds promise for uncovering molecular data from ancient specimens.
The researchers discovered red blood cell-like structures in a fossil while studying a Telmatosaurus transsylvanicus, a duck-billed, plant eating “marsh lizard” that lived between 66-70 million years ago in the Hateg Basin in present-day Romania.
The new study used Scanning Electron Microscopy (SEM) techniques to identify low-density structures resembling erythrocytes, or red blood cells, in the fossilised bone.
The findings raise the possibility that soft tissue and cellular components are more commonly preserved in ancient remains than previously thought.
By identifying preserved proteins and biomarkers, scientists believe they can gain insights into the diseases that affected prehistoric creatures, including cancer, potentially influencing future treatments for humans.
The authors of the new study highlight the necessity of prioritising the collection and preservation of fossilised soft tissue, rather than just dinosaur skeletons, as future advancements in molecular techniques will enable deeper insights into disease evolution.
A separate study had previously identified evidence of cancer in Telmatosaurus transsylvanicus, indicating its deep evolutionary roots.
More precise treatment options with robotic technology
Friday, 20 June 2025:Prostate cancer is a major risk to men’s health, with South African men facing a one in eight chance of developing this most common of male cancers.
Urologists Dr Hannes Brummer and Dr Johan Coetzee, who practise at Netcare Greenacres Hospital, are encouraging men to prioritise prostate cancer screening this Men’s Health Month.
“Usually, men do not feel any symptoms until prostate cancer has progressed significantly, which is why they need to be proactive about booking their routine prostate cancer screenings,” explains Dr Coetzee.
“With the advanced prostate specific antigen [PSA] screening blood test available from GPs these days, there is so much more opportunity for prostate cancer to be detected earlier when it is still at a highly treatable stage.”
“For men who are diagnosed with prostate cancer following a needle biopsy, the treatment options available have improved to such an extent that there is more hope than ever before. Even where surgery is needed, prostate cancer does not necessarily pose a significant disruption to your life,” Dr Brummer adds.
“A prostate cancer diagnosis can be daunting. We have walked this path with so many men, and robotic assisted surgery offers some important advantages for the removal of cancerous tissue in the prostate gland, in particular the precision of this minimally invasive option.”
Over 1 000 robotic assisted procedures have been performed at Netcare Greenacres Hospital since the introduction of this technology in August 2017.
At Netcare Greenacres Hospital, Dr Brummer and Dr Coetzee use the da Vinci X robotic assisted surgical system to operate through tiny punctures in the skin using slender instruments more dexterous than the human hand.
Dr Brummer and Dr Coetzee emphasise that the surgeon remains in control of the robotic system at all times. With magnified 3D imaging capabilities, including a large fixed-focus area at the highest resolution, the nerves, blood vessels and tumour are visible with great clarity for the intricate procedure.
“This robotic system is especially useful for operating on the prostate, as we can more clearly distinguish the nerves controlling erectile function and urinary continence. In most cases, there is less need for blood transfusion and reduced risk of complications,” Dr Brummer explains.
“Another of the advantages of this robotic technology for prostate tumours is that there is much less tissue damage in this sensitive area. Compared with traditional surgery, this means men usually experience much less downtime with less discomfort after the procedure. This translates into shorter hospital stays and faster recovery with robotic assisted prostatectomies overall.”
General manager of Netcare Greenacres Hospital, Reon van Rensburg, joined the urologists in reinforcing the importance of prostate cancer awareness. “Let’s talk to our brothers, fathers, sons and grandsons about health issues, and get to know your family risk for both prostate cancer and breast cancer.”
Van Rensburg thanked Dr Brummer and Dr Coetzee for their continued dedication to making the world-class minimally-invasive robotic assisted surgical option available for patients local to Gqeberha and from as far afield as Knysna, George and East London, inland regions of the Eastern Cape, and parts of the southern Free State, the Northern Cape and the north-eastern region of the Western Cape.
“This Men’s Health Month, let’s pledge to be decisive about booking those routine health checks. Making the time now and every year could help to save your life in future,” Dr Brummer and Dr Coetzee concluded.
Knee braces, water therapy, and exercise are the most beneficial non-drug therapies, per meta-analysis of more than 100 clinical trials involving nearly 10 000 people
Knee braces, water therapy and exercise are the most promising non-drug therapies for treating knee osteoarthritis, according to a new meta-analysis publishing June 18, 2025 in the open-access journal PLOS Oneby Yuan Luo of the First People’s Hospital of Neijiang, China.
Knee osteoarthritis (KOA) is a common and often debilitating condition that affects millions of older adults, causing pain and stiffening of the knee joint. Treatment often includes anti-inflammatory drugs, which are linked to gastrointestinal and cardiovascular adverse events.
In the new study, researchers examined the current evidence on non-drug therapies for treating KOA. They looked at data from 139 clinical trials involving nearly 10 000 people to compare 12 different non-drug treatments. These included laser therapy, electrical stimulation, braces, insoles, kinesiology tape, water-based therapy, exercise, and ultrasound. By combining results from all these studies into a powerful network meta-analysis, the team could rank the therapies based on how well they worked.
Knee braces came out on top across most categories, including reducing pain, improving function, and relieving stiffness. Hydrotherapy—exercises or treatments performed in warm water—was particularly effective at easing pain and general exercise was also consistently effective, improving both pain and physical function. High-intensity laser therapy and shock wave therapy showed some benefits, while ultrasound consistently scored the lowest in effectiveness.
The authors caution that differences in study design, small sample sizes, and variability in treatment duration between the 139 included studies may limit the precision of the rankings. However, they conclude that physical therapy has promising effects on KOA, offering potential treatments without the risks of anti-inflammatory drugs. Future studies should examine the clinical efficacy of combined therapies, as well as their cost-effectiveness.
The authors add: “Knee braces, hydrotherapy, and exercise are the most effective non-drug therapies for knee osteoarthritis. They reduce pain and improve mobility without the gastrointestinal or cardiovascular risks linked to common pain medications. Patients and clinicians should prioritize these evidence-based options.”
“Our analysis of nearly 10 000 patients reveals that simple, accessible therapies like knee bracing and water-based exercise outperform high-tech options like ultrasound. This could reshape clinical guidelines to focus on safer, lower-cost interventions.”
Health workers have long relied on Body Mass Index as a way to measure whether people are within a healthy weight range. Now, a collection of top researchers have made the case for a new way to understand and diagnose obesity. In part two of this special Spotlight series, we take a look at what this new framing might mean for South Africa.
If we are going to tackle the global rise in obesity, our understanding of the condition needs to change. That is according to a Lancet Commission convened by a global group of 58 experts from different medical specialties. While we have historically thought of obesity as a risk factor for other diseases like diabetes, the commission’s recent report published in the journal Lancet Diabetes and Endocrinology concludes that obesity is sometimes better thought of as a disease itself – one that can directly cause severe health symptoms (see part one of this series for a detailed discussion of this argument).
By categorising obesity as a disease, public health systems and medical aid schemes around the world would be more likely to cover people for weight-loss drugs or weight-loss surgery, according to the report. At present, these services are often only financed if a patient’s obesity has already led to other diseases. This is given that obesity is not viewed as a stand-alone chronic illness.
But if we’re going to redefine obesity as a disease, or at least some forms of it, then we need good clinical definitions and ways to measure it. For a long time, this has posed challenges, according to the Lancet report.
The perils of BMI
At present, health workers often rely on Body Mass Index (BMI) to gauge whether a patient is within a healthy weight range. BMI is measured by taking a person’s weight in kilograms and dividing it by their height in meters squared.
A healthy weight is typically considered to be between 18.5 and 25. A person whose BMI is between 25 and 30 is considered to be overweight, while someone with a BMI of over 30 is considered to have obesity. But according to the Lancet report, this is a crude measure, and one which provides very little information about whether a person is actually ill.
One basic issue is that a person can have a high BMI even if they don’t have a lot of excess fat. Instead, they may simply have a lot of muscle or bone. Indeed, the report notes that some athletes are in the obese BMI range.
Even when a high BMI does indicate that a person has obesity, it still doesn’t tell us where a person’s fat is stored and this is vital medical information. If excess fat is stored in the stomach and chest, then it poses more severe health risks than when it is stored in the limbs or thighs. This is because excess fat will do more harm if it surrounds vital organs.
The lead author of the Lancet report, Professor Frances Rubino, says that the pitfalls of BMI have long been understood, but practitioners have continued to use it.
“BMI is still by and large the most used approach everywhere, even though medical organisations have [raised issues] for quite some time,” he tells Spotlight.
“The problem is that even when we as individuals or organisations say BMI is no good, we haven’t provided an alternative. And so, inevitably, the ease of calculating BMI and the uncertainties about alternatives makes you default back to BMI.”
To deal with this problem, the report advocates for several alternative techniques for measuring obesity which offer more precision.
The first option is to use tools that directly measure body composition like a DEXA scanner. This is a sophisticated x-ray machine which can be used to distinguish between fat, bone and muscle. It can also be used to determine where fat is concentrated. It’s thus a very precise measurement tool, but the machines are expensive and the scans can be time-consuming.
Alternatively, the report recommends using BMI in combination with another measure like waist-to-hip ratio, waist-to-height ratio or simply waist circumference. If two of these alternative measures are used, then BMI can be removed from the picture.
These additional metrics are clinically useful because they provide information about where fat is stored. For instance, a larger waistline inevitably indicates a larger stomach. Indeed, studies have found that above a certain level, a larger waist circumference is linked to a higher chance of dying early, even when looking at people with the same BMI.
The report thus offers a more accurate way to measure obesity in the clinical setting. But its authors argue that this is only the first step when making a diagnosis. The second is to look at whether a patient’s obesity has actually caused health problems as this isn’t automatically the case. They acknowledge for instance that there are some people with obesity who “appear to be able to live a relatively healthy life for many years, or even a lifetime”.
The report refers to these cases as “preclinical obesity”. Such patients don’t have a disease as such, according to the report, but still have an increased risk of facing health issues in the future. As such, the report’s authors argue that they should be monitored and sometimes even treated, depending on factors like family history.
By contrast, cases of obesity which have directly caused health problems are referred to as “clinical obesity”. These cases, according to the report, should be treated immediately just like any other serious disease. It lists a series of medical symptoms associated with clinical obesity that would allow health workers to make an appropriate diagnosis.
The recommendation is thus for health workers to determine whether a person has obesity through the metrics listed above, and then to determine whether it is clinical or preclinical by evaluating a patient’s symptoms. This will inevitably guide the treatment plan.
How does this relate to SA?
Professor Francois Venter, who runs the Ezintsha research centre at WITS university, says the Lancet report offers a good starting point for South Africa, but it has to be adapted for our own needs and context.
“It’s a big step forward from BMI which grossly underdiagnoses and overdiagnoses obesity,” says Venter, who adds that additional metrics like waist circumference are a “welcome addition”.
The view that clinical obesity is a disease that needs to be immediately treated is also correct, according to Venter. Though he adds that the public health system in South Africa is not in a financial position to start handing out weight-loss medicine to everyone who needs it.
“The drugs are hugely expensive,” says Venter, “and they have side effects, so you need a lot of resources to support people taking them.” But while it may not yet be feasible to treat all cases of clinical obesity in South Africa, Venter believes we should use the diagnostic model offered by the Lancet Commission to begin identifying at least some people with clinical obesity so that they can begin treatment.
“You have to start somewhere, and for that you need a good staging system,” he says. “Let’s use the Lancet Commission and start to see if we can identify a few priority people and screen them and start to work on the drug delivery system.”
Yet while Venter believes that the commission makes important contributions, he also cautions that we need more data on obesity in Africa before we can apply all of its conclusions to our own context.
“If you go to the supplement of the Lancet Commission, there’s not a single African study there. It all comes from Europe, North America and Asia. It’s not the commission’s fault but [there is a lack of data on Africa].”
This is important as findings that apply to European or Asian populations may not necessarily hold for others. Consider the following case.
As noted, the commission states that BMI is not sufficient to determine whether someone is overweight and must therefore be complemented with other measures. But it states that if someone’s BMI is above 40 (way above the current threshold for obesity), then this can “pragmatically be assumed” without the need for further measures.
But this may not hold in Africa, says Venter.
“The commission says that if your BMI is over 40, which is very big, you can infer that this person has got obesity and they are sick and need to lose weight. I don’t know if we can say that in Africa, where we often have patients who are huge, and yet they are very active, and when you [look at] their blood pressure and all their metabolics, they’re actually pretty healthy,” he notes. “So, I think they’re sometimes jumping to conclusions about African populations that we don’t have data on,” adds Venter.
Is South Africa ready to move past BMI?
Another concern is that while the Lancet Commission may offer useful recommendations for advanced economies, its starting assumptions may not be as relevant for countries like South Africa.
For instance, while specialists agree that BMI is a crude measure of obesity, direct measures like DEXA scans are “out of our reach economically”, according to Professor Susan Goldstein, who leads PRICELESS-SA, a health economics unit at the South African Medical Research Council.
And while supplementing BMI with the other metrics like waist circumference may be doable, health experts told Spotlight that at present healthcare workers in South Africa aren’t even measuring BMI alone.
Dr Yogan Pillay, a former deputy director-general at the national health department who now runs TB and HIV delivery at the Gates Foundation, told Spotlight: “I can’t tell you how few people in the public sector have their BMI monitored at all. Community health workers are supposed to be going out and measuring BMI, but even that’s not happening”.
Goldstein also suggests that the monitoring of BMI in South Africa is limited. “If you go into the clinic for your blood pressure, do they say: ‘How’s your BMI?’ No, I doubt that,” says Goldstein. “It’s just not one of the measures that [gets done].”
She adds that South Africa could introduce the combination of metrics proposed by the commission, like waist circumference combined with BMI, but says it would simply require “a lot of re-education of health workers”.
Prevention vs treatment
For Goldstein, the commission is correct to regard clinical obesity as a disease which needs to be treated, but we also shouldn’t view medication as the only way forward.
“We have to remember that prevention is very important,” says Goldstein. “We have to focus on food control, we have to look at ultra-processed foods, and unless we do that as well [in addition to medication] we are going to lose this battle.”
The National Health Department already has a strategy document for preventing obesity, but some of its recommendations have been critiqued for focusing on the wrong problems. For instance, to prevent childhood obesity, the strategy document recommends reforming the Life Orientation curriculum and educating tuck shop vendors so that both students and food sellers have more information about healthy eating. But as Spotlight previously reported, there are no recommendations to subsidise healthy foods or to increase their availability in poor areas, which several experts believe is more important than educational initiatives.
Venter also highlights the importance of obesity prevention, though he emphasises that this shouldn’t be in conflict with a treatment approach – instead, we need to push for both.
“The [prevention] we need to do is fix the food supply… and the only way you do that is to decrease the cost of unprocessed food.” But while this may help prevent future cases of obesity, it doesn’t help people who are already suffering from obesity, says Venter. And since such people comprise such a large share of the population, we can’t simply ignore them, he says.
“Even if you fix the entire food industry tomorrow, those [people who are already obese] are going to remain where they are because simply changing your diet isn’t going to do diddly squat [when you already have obesity],” he adds. (Part 1 discusses this in more detail).
Goldstein adds that increasing access to treatment would also inevitably reduce the costs of “hypertension, diabetes, osteoarthritis, and a whole range of other illnesses if it’s properly managed”.
One way to advance access to medication would be for the government to negotiate reduced prices of GLP-1 drugs, she says. (Spotlight previously reported on the prices and availability of these medicines in South Africa here.)
Funding
A final concern that has been raised about the Lancet commission is about its source of funding.
“I don’t know how one gets around this,” says Goldstein, “but there were 58 experts on the commission, 47 declared conflicts of interest.”
Indeed, the section of the commission that lists conflicts of interest spans over 2 000 words (roughly the size of this article). This includes research grants and consulting fees from companies like Novo Nordisk and Eli Lilly, which produce anti-obesity drugs.
In response, Rubino told Spotlight that “people who work in the medical profession obviously work and consult, and the more expertise they have, the more likely they are to be asked by somebody to advise. So sometimes people have contracts to consult a company – but that doesn’t mean that they necessarily make revenue if the company has better sales. You get paid fees for your services as a consultant”.
Rubino says this still has to be declared as it may result in some bias, even if it is unconscious, but “if you wanted to have experts who had zero relationship [to companies] of any sort then you might have to wonder if there is expertise available there… the nature of any medical professional is that the more expertise they have, the more likely that they have engaged in work with multiple stakeholders”.
For Venter, there is some truth to this. “It’s very difficult to find people in the obesity field that aren’t sponsored by a drug company,” he says. “Governments don’t fund research… and everyone else doesn’t fund research. Researchers go where the research is funded.”
This doesn’t actually solve the problem, says Venter, as financing from drug companies can always influence the conclusions of researchers. It simply suggests that the problem is bigger than the commission. Ultimately, he argues that the authors should at least be applauded for providing such granular details about conflicts of interest.
Rubino adds that while researchers on the commission may have historically received money from drug companies for separate research studies or consulting activities, none of them received money for their work on the commission itself.
“This commission has been working for more than four years since conception… An estimate of how many meetings we had is north of 700, and none of us have received a single penny [for doing this],” he says.
Disclosure: The Gates Foundation is mentioned in this article. Spotlight receives funding from the Gates Foundation but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council.
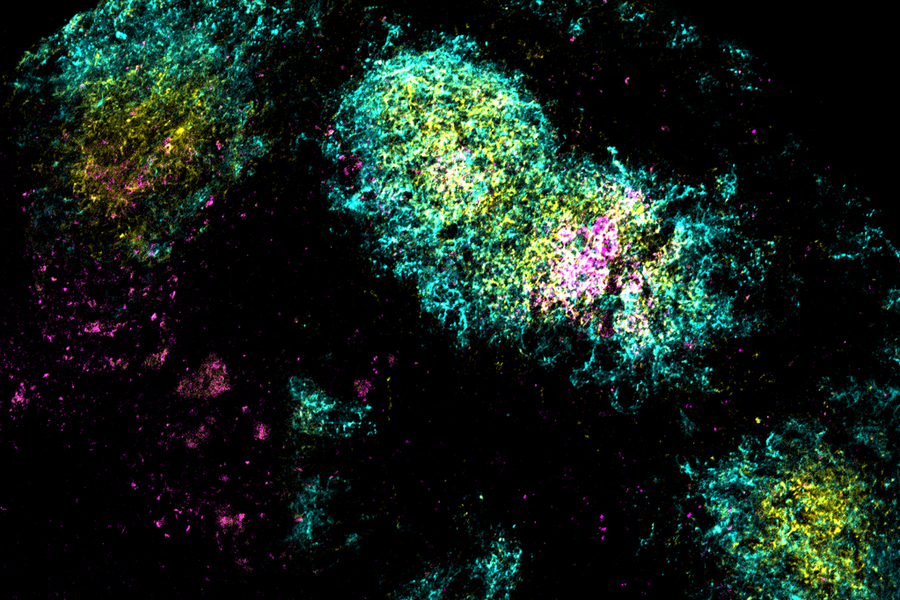
By delivering an HIV vaccine candidate along with two adjuvants, researchers showed they could generate many more HIV-targeting B cells in mice.
Anne Trafton | MIT News
Image shows the vaccine antigen (pink) being concentrated in a germinal center (yellow) within B cell follicles (cyan), triggered by the researchers’ combination adjuvant vaccine.
Credits: Image: Courtesy of the researchers
Researchers at MIT and the Scripps Research Institute have shown that they can generate a strong immune response to HIV with just one vaccine dose, by adding two powerful adjuvants — materials that help stimulate the immune system.
In a study of mice, the researchers showed that this approach produced a much wider diversity of antibodies against an HIV antigen, compared to the vaccine given on its own or with just one of the adjuvants. The dual-adjuvant vaccine accumulated in the lymph nodes and remained there for up to a month, allowing the immune system to build up a much greater number of antibodies against the HIV protein.
This strategy could lead to the development of vaccines that only need to be given once, for infectious diseases including HIV or SARS-CoV-2, the researchers say.
“This approach is compatible with many protein-based vaccines, so it offers the opportunity to engineer new formulations for these types of vaccines across a wide range of different diseases, such as influenza, SARS-CoV-2, or other pandemic outbreaks,” says J. Christopher Love, the Raymond A. and Helen E. St. Laurent Professor of Chemical Engineering at MIT, and a member of the Koch Institute for Integrative Cancer Research and the Ragon Institute of MGH, MIT, and Harvard.
Love and Darrell Irvine, a professor of immunology and microbiology at the Scripps Research Institute, are the senior authors of the study, which appears today in Science Translational Medicine. Kristen Rodrigues PhD ’23 and Yiming Zhang PhD ’25 are the lead authors of the paper.
More powerful vaccines
Most vaccines are delivered along with adjuvants, which help to stimulate a stronger immune response to the antigen. One adjuvant commonly used with protein-based vaccines, including those for hepatitis A and B, is aluminum hydroxide, also known as alum. This adjuvant works by activating the innate immune response, helping the body to form a stronger memory of the vaccine antigen.
Several years ago, Irvine developed another adjuvant based on saponin, an FDA-approved adjuvant derived from the bark of the Chilean soapbark tree. His work showed that nanoparticles containing both saponin and a molecule called MPLA, which promotes inflammation, worked better than saponin on its own. That nanoparticle, known as SMNP, is now being used as an adjuvant for an HIV vaccine that is currently in clinical trials.
Irvine and Love then tried combining alum and SMNP and showed that vaccines containing both of those adjuvants could generate even more powerful immune responses against either HIV or SARS-CoV-2.
In the new paper, the researchers wanted to explore why these two adjuvants work so well together to boost the immune response, specifically the B cell response. B cells produce antibodies that can circulate in the bloodstream and recognise a pathogen if the body is exposed to it again.
For this study, the researchers used an HIV protein called MD39 as their vaccine antigen, and anchored dozens of these proteins to each alum particle, along with SMNP.
After vaccinating mice with these particles, the researchers found that the vaccine accumulated in the lymph nodes — structures where B cells encounter antigens and undergo rapid mutations that generate antibodies with high affinity for a particular antigen. This process takes place within clusters of cells known as germinal centers.
The researchers showed that SMNP and alum helped the HIV antigen to penetrate through the protective layer of cells surrounding the lymph nodes without being broken down into fragments. The adjuvants also helped the antigens to remain intact in the lymph nodes for up to 28 days.
“As a result, the B cells that are cycling in the lymph nodes are constantly being exposed to the antigen over that time period, and they get the chance to refine their solution to the antigen,” Love says.
This approach may mimic what occurs during a natural infection, when antigens can remain in the lymph nodes for weeks, giving the body time to build up an immune response.
Antibody diversity
Single-cell RNA sequencing of B cells from the vaccinated mice revealed that the vaccine containing both adjuvants generated a much more diverse repertoire of B cells and antibodies. Mice that received the dual-adjuvant vaccine produced two to three times more unique B cells than mice that received just one of the adjuvants.
That increase in B cell number and diversity boosts the chances that the vaccine could generate broadly neutralizing antibodies — antibodies that can recognize a variety of strains of a given virus, such as HIV.
“When you think about the immune system sampling all of the possible solutions, the more chances we give it to identify an effective solution, the better,” Love says. “Generating broadly neutralizing antibodies is something that likely requires both the kind of approach that we showed here, to get that strong and diversified response, as well as antigen design to get the right part of the immunogen shown.”
Using these two adjuvants together could also contribute to the development of more potent vaccines against other infectious diseases, with just a single dose.
“What’s potentially powerful about this approach is that you can achieve long-term exposures based on a combination of adjuvants that are already reasonably well-understood, so it doesn’t require a different technology. It’s just combining features of these adjuvants to enable low-dose or potentially even single-dose treatments,” Love says.
The research was funded by the National Institutes of Health; the Koch Institute Support (core) Grant from the National Cancer Institute; the Ragon Institute of MGH, MIT, and Harvard; and the Howard Hughes Medical Institute.
This story is republished courtesy of MIT News (web.mit.edu/newsoffice/), a popular site that covers news about MIT research, innovation and teaching.