Cipla Medpro South Africa reaffirmed its commitment to ensuring the uninterrupted supply of critical antiretroviral (ARV) medicines to the Department of Health. It is essential that people living with HIV have uninterrupted access to these life-saving medicines. Any disruption of supply puts patients at risk of developing resistance to the drugs or adversely affecting health outcomes. According to Statistics South Africa, the number of people living with HIV in the country is estimated to be approximately 8 million (12,7% of the population)[1].
Recently, two suppliers who were awarded the current antiretroviral (ARV) tender, Barrs Pharmaceuticals Industries (Pty) Ltd and Innovata Pharmaceuticals (Pty) Ltd (subsidiaries of Avacare Health), have entered business rescue.
Cipla acknowledges the uncertainty this may create within the ARV supply chain and underscores its readiness to assist in maintaining stability and continuity.
Cipla has been manufacturing tenofovir/lamivudine/dolutegravir (TLD) for the government for the past 7 years, and has been one of the main suppliers of ARVs to the government for more than 12 years. Cipla has made significant investments in its local manufacturing facility, upgrading the capacity of the ARV production line with the installation of a new Countec bottle line and have increased its tablet filing capacity by 190%. The company is able to locally produce 475 million tablets annually and has upscaled its manufacturing capabilities to ensure sufficient capacity to meet current demand and support near‑term growth, while reinforcing Cipla’s commitment to secure and reliable ARV supply.
“We have mobilised resources to help maintain equitable access to quality, affordable critical medication. Cipla confirms its willingness to support national requirements under the current tender agreement and, if needed, contribute meaningfully to any supplementary procurement processes to safeguard patient access to essential treatment. We want people to live a long and healthy life as part of our commitment to caring for life,” said Paul Miller, CEO of Cipla Africa.
“In addition, we believe this tender presents an opportunity to further advance government’s commitment to strengthening local manufacturing capacity. By ensuring greater support for locally produced medicines, future allocations could meaningfully contribute to South Africa’s industrial development agenda while maintaining continuity of supply,” said Miller.
The total ARV tender is for a period of three years, and is worth an estimated R15.5bn, of which the TLD component comprises R12.6bn.
The US government paused all foreign assistance in January 2025. This abrupt decision affected the delivery of life-saving HIV medicines and the provision of HIV prevention services to millions of people. A UNAIDS report estimates there could be an additional 6 million new HIV infections and 4 million Aids-related deaths by 2029 if the world does not act.
In November 2025, a global health initiative, The Global Fund, raised US$11.34 billion for HIV/Aids, tuberculosis and malaria. Melanie Bisnauth, a public health professional in healthcare systems strengthening and HIV/Aids leadership, discusses how far this latest funding could go and how African nations can tackle the dwindling funding for HIV/Aids control.
What is the funding status for HIV/Aids?
Raising US$11.34 billion is significant but it falls short of the US$18 billion target. The Global Fund is trying to raise US$18 billion for its work from 2027 to 2029. The Global Fund is a worldwide partnership to end the epidemic of HIV/Aids, tuberculosis and malaria and ensure a healthier, safer and more equitable future for all.
It is only a partial response to the global funding gaps.
The US pledged US$4.6 billion to the Global Fund during the fund’s summit in November 2025, on the side of the G20 meeting in South Africa. It was a reduction from its previous pledge of US$6 billion to support prevention, treatment, care and related services for the three diseases. But it is also an indication that the US has not abandoned all multilateral global health efforts. It remains the largest single contribution to the Global Fund 2027 to 2029 cycle.
The shortfall may strain existing programmes and delay expansion of life-saving interventions for HIV/Aids, tuberculosis and malaria.
HIV remains a major global public health issue, having claimed an estimated 44.1 million lives to date. An estimated 40.8 million people were living with HIV at the end of 2024, 65% of whom are in the WHO African region.
Job losses could create inefficiencies or service reductions. Building a sustainable HIV response and meeting key goals was already challenging before the sharp funding decline in 2025. Over 11 million people had unsuppressed viral loads in 2024.
Overall, while the funds raised demonstrate continued global solidarity, they are insufficient to fully compensate for the US withdrawal and broader declines in donor support.
There are potentially long-term consequences. Reduced funding and service disruptions threaten to reverse years of progress. Infections could rise, especially in communities where viral suppression was already low. Lack of service delivery and supply of treatment will weaken trust in health systems and can lead to treatment interruptions, drug resistance and poorer health outcomes.
As the Global Fund’s executive director said at the Replenishment Summit, “the old model” of development funding is over. This model is the heavy reliance on international funding like USAID and other donor organisations.
It’s essential for countries to become more self-reliant. But the statement warned that too abrupt a transition could be dangerous.
I fear that the COVID-19 pandemic has already taken a toll on the quality of care provided. Healthcare systems are already overburdened.
National governments have to step up and locally support their healthcare systems, collaborate and build together, and strengthen their health funding structures.
What should the response be for better HIV funding in Africa?
Africa’s HIV response should be multi-pronged.
After attending the Africa Summit in Geneva in May 2025, stakeholders, country representatives, donor agencies and NGOs expressed a key message: those involved in the sector should not reinvent the entire wheel. There is value in the knowledge gained from programming, technical expertise, data insights, partnerships, communities and global health networks should be used to strengthen, adapt and scale what already works.
This will ensure that Africa’s HIV response remains community-centred, evidence-driven, and resilient in the face of emerging challenges.
The global health climate has changed and communities have lost trust because of severely disrupted or even completely cut programmes. African governments must allocate their own resources for HIV programmes, through budget prioritisation, health insurance schemes, and innovative financing such as public-private partnerships. Improvements, such as integrating HIV services into primary care, using data-driven targeting, and negotiating lower drug costs can maximise impact.
Strengthening regional collaborations and pooled procurement through organisations like the African Union or regional health bodies can improve bargaining power and reduce dependency on external aid. A balanced mix of donor support, domestic financing and operational efficiency is essential to maintain gains and expand access to treatment for all in need.
It is important not to rely solely on international support or one funding body. Diversifying funding portfolios is critical.
What effects has the withdrawal of US funds had?
Reduced US contributions led to immediate financial shortfalls, threatening ongoing HIV prevention and treatment programmes.
For example, some clinic supply and services faced disruption in delivery and supply of antiretroviral therapy, and stock-outs of treatment and malaria nets.
The world is still likely to feel the impact in the coming months. For example:
Progress towards epidemic control could slow, potentially increasing illness and death.
Programmes that relied heavily on US support have already scaled back services or will do so.
Funding uncertainty remains a major concern. Governments will have to reallocate limited domestic resources or seek alternative donors.
Global health co-ordination, technical assistance and advocacy efforts may be weakened. In the past these supported robust HIV responses in Africa in progress toward the UNAIDS targets.
Reliance on fragmented funding streams will increase.
How can African countries better fund their HIV programmes?
They can take steps that involve a mix of domestic revenue generation, efficiency gains and strategic partnerships:
diversify funding through raising domestic revenue, such as earmarked taxes
expand the reach of social health insurance coverage
leverage corporate investment and innovation through public-private partnerships
negotiate pooled procurement of drugs and diagnostics regionally to reduce costs
involve communities in decision making, which will help strengthen sustainability
integrate HIV programmes into broader health systems – it improves efficiency, reducing duplication and operational costs.
Eastern Cape HIV Programme demonstrates success in resource-constrained setting
Photo by Pexels on Pixabay
A new randomised controlled trial conducted in the Eastern Cape has shown that adding structured patient navigation to same-day antiretroviral therapy (ART) can make a meaningful difference for people newly diagnosed with HIV. The trial found that patients who received support from trained navigators were far more likely to stay in care and keep their viral load low over six months. Those with navigator support had a 79% retention rate, compared with 64% under standard care.
Among patients who achieved a viral load of fewer than 50 copies per millilitre, 64% remained in care, compared to just 39% without this extra support(1). Patient navigation combines personal support, such as home or virtual check-ins and WhatsApp reminders, with practical help like linking people to services and monitoring their progress. It was especially effective for people who started treatment on the same day as their diagnosis.
“This approach humanises HIV care. It builds a bridge between the clinic and the community, helping patients stay connected to treatment and ultimately saving lives,” said lead author Siyakudumisa Nontamo, Facility Team Lead: Care & Treatment Programme at TB HIV Care.
In August 2024 the Human Sciences Research Council released findings from the Sixth South African HIV Prevalence, Incidence, and Behaviour Survey (SABSSM VI) for the Eastern Cape. The results show that HIV prevalence in the province stabilised, moving from 15.9% in 2017 to 13.7% in 2022. This is an estimated 980 000 people living with HIV, down from about 1 million in 2017. Access to treatment has improved significantly. ART coverage increased from 67.8% in 2017 to 83.5% in 2022, meaning about 723 000 people in the province are now receiving treatment. However, gaps remain among young people: only 70.9% of adolescents and youth aged 15–24 living with HIV are on ART, compared to 84.8% of adults aged 25-49. Among females, coverage is much lower for young women (68.7%) than for women aged 25-49 (88.2%). ART use also varies across districts, ranging from 69.4% in Nelson Mandela Bay to 92.0% in Alfred Nzo(2). Nationally, the proportion of people living with HIV who are currently on antiretroviral treatment (ART) rose to 80.9% in 2022, up from 63.7% in 2017.
Despite major advances in antiretroviral therapy, retention in care remains a persistent challenge within South Africa’s HIV programme, especially in rural provinces such as the Eastern Cape. Many patients initiate treatment but later disengage due to stigma, transport difficulties, and limited ongoing support. The study shows that low-cost, human-centred interventions can significantly strengthen treatment outcomes. The trial, titled “Impact of Patient Navigation on Retention in Care and HIV Viral Load Suppression Among Newly Diagnosed Persons Living with HIV in the Eastern Cape,” compared standard HIV care to an approach where trained patient navigators provided ongoing support to patients starting antiretroviral therapy (ART). Beyond improved retention and viral suppression, the trial also showed that patients supported by navigators experienced fewer deaths and dropouts, with substantially lower losses to follow-up and reduced mortality than those receiving standard care, ultimately strengthening HIV programmes(1).
Patient navigation, in particular, helps bridge the gap by pairing practical healthcare coordination with empathy and community-based follow-up. Navigators assist patients with managing appointments, maintaining adherence, and accessing psychosocial services, thereby fostering trust, continuity, and sustained engagement in care. This approach aligns with South Africa’s national HIV strategy, which prioritises differentiated, patient-centred models of care to achieve the UNAIDS 95-95-95 targets.
At scale, TB HIV Care’s programmes are grounded in person-centred, integrated service models that reflect the real lives and needs of people affected by HIV and TB. This study reinforces TB HIV Care’s belief that support beyond clinic walls is essential for achieving lasting impact. In the 2024/25 reporting period, the organisation reached more than 1.9 million people with HIV testing services and initiated 27,873 individuals on ART, achieving a 95% viral suppression rate among clients in care.
“By bridging the gap between diagnosis and ongoing care, patient navigation aligns with our outreach for key populations and our shift toward holistic service delivery. We look forward to translating this evidence into practice, ensuring fewer people fall through the cracks and more sustain treatment success”, said Professor Harry Hausler, CEO at TB HIV Care.
Additional findings from the Sixth South African HIV Prevalence, Incidence, and Behaviour Survey (SABSSM VI) for the Eastern Cape.
In the Eastern Cape, HIV remains most common among adults aged 25-49, with a prevalence of 27.7%, and women in this age group are especially affected at 35.4% compared to 17.1% for men.
The survey also found geographic differences: HIV prevalence among men was highest in urban areas (8.7%), while among women it was highest in rural informal or tribal areas (19.8%).
By district, prevalence was highest in Chris Hani (14.4%), Amathole (14.1%), Alfred Nzo (13.9%), and lowest in Nelson Mandela Bay (9.7%).
At a national level, the survey showed that 81.4% of all people living with HIV were virally suppressed. The survey found encouraging progress in the Eastern Cape, where viral load suppression (VLS) among people living with HIV rose to 79.3% in 2022, up from 66.3% in 2017. However, children aged 0-14 years had much lower suppression levels, at 61.4%. Among people aged 15-49 years living with HIV, 78.6% were virally suppressed. Within this group, women had far higher suppression rates (83.9%) than men (65.4%).
About the Randomized Controlled Trial
The randomised controlled trial involved participants from HIV testing sites in the O.R. Tambo District (Flagstaff, Mthatha Gateway, and Tsolo Clinics). It was approved by the Eastern Cape Health Research Committee and Walter Sisulu University’s Ethics Committee. The study was supported by the Chemical Industries Education and Training Authority (CHIETA) and the South African Medical Research Council’s Strategic Health Innovation Partnerships (SHIP).
References:
Nontamo, S., Kamsu, G.T., Ndebia, E.J., et al. Impact of Patient Navigation on Retention in Care and HIV Viral Load Suppression Among Newly Diagnosed Persons Living with HIV in the Eastern Cape – South Africa. Access.
Human Sciences Research Council. Sixth South African HIV Prevalence, Incidence, and Behaviour Survey (SABSSM VI). Access.
Pharmacists can initiate people with HIV on antiretroviral treatment, the Supreme Court of Appeal has ruled. Photo: GroundUp Staff
The Supreme Court of Appeal (SCA) has dismissed, with costs, an appeal by a doctor’s organisation, the IPA Foundation, aimed at stopping specially trained pharmacists from treating people with HIV and TB.
The IPA first took its dispute with the South African Pharmacy Council (SAPC) to the Gauteng High Court in Pretoria. In 2023, Judge Elmarie van der Schyff ruled in favour of the pharmacists, giving a judicial go-ahead for the council to introduce its Pharmacy-Initiated Management of Antiretroviral Treatment (PIMART) initiative.
However the IPA Foundation, intent on having the initiative set aside, took this ruling on appeal to the SCA. In that court, five judges this week ruled against it. The ruling came nearly 11 months after the case was heard, far more than the three months that judicial norms provide for when a judgment is reserved.
Justice Tati Makgoka, writing for the court, said the initiative was created in response to a persistent rise in new HIV infection rates.
The SAPC, at the department’s request, deemed PIMART suitable for addressing this issue.
“As the high court correctly found, the SAPC evaluated the risks associated with pharmacists initiating first-line ART [antiretroviral treatment] and TPT [tuberculosis preventive therapy] as well as providing medicines for PrEP [Pre-Exposure Prophylaxis of HIV] and PEP [Post Exposure Prophylaxis of HIV], considering the risks when deciding to approve the PIMART training.
“The uncontested evidence presented by the SAPC demonstrates that the approved accreditation process for PIMART was rigorous and thorough,” Makgoka said.
In her previous judgment, Van Der Schyff had noted that a pilot project had emphasised the value of the initiative, which was in line with the World Health Organisation’s vision to promote widely accessible primary health care.
“The untapped value of pharmacists in fighting HIV was also emphasised by the efficient role pharmacies played in meeting health care needs and providing health care services during the Covid-19 pandemic,” she said.
“The need to widen access to first line ART and TPT therapy on a community level is not a figment of SAPC’s imagination but a dire need that is also evinced in other countries.”
The IPA Foundation had approached the Pretoria court, under the Promotion of Administrative Justice Act (PAJA), seeking to review and set aside the SAPC’s decision to implement PIMART.
IPA claimed that the SAPC had failed to give interested parties an adequate opportunity to comment before the initiative was implemented. It further contended that PIMART unjustifiably encroached on the domain of medical practitioners and was in conflict with legislation.
On appeal, the IPA persisted with these arguments.
Dealing with the background, Justice Makgoka said the SAPC had published a notice in the government gazette in March 2021 regarding the proposed adoption of PIMART, giving interested parties 60 days to comment. This resulted in government approval later that year.
It was only after this that the IPA submitted its comments and objections.
Following engagements, the IPA lodged the review application in the high court.
On the issue that the IPA and its members claimed they were not given sufficient notice of PIMART, because it was advertised in the government gazette during the Covid-19 pandemic – Makgoka said there was no suggestion that the pandemic had “paralysed the administrative functions” of the IPA.
Remarkably, the judge said, the IPA had not suggested that the notice did not come to its attention, finding that adequate notice had been given. Makgoka said that several other organisations had submitted comments during the prescribed period.
He said the IPA had also not challenged the validity of the Pharmacy Act, which specified publication in the gazette and in the absence of that, it was not open for it to say the publication was inadequate.
Makgoka said the IPA had introduced the issue of “rationality” only in its notice of appeal. However, the court had dealt with this because there was no prejudice to the SAPC.
In ruling on this issue, he said PIMART was a crucial intervention in the public interest, which had been devised by a group of medical experts.
“Through PIMART, the SAPC aimed to improve access to healthcare. Contrary to the IPA’s contentions, PIMART is an essential intervention in the fight against HIV/AIDS. Its introduction constitutes a rational legislative and practical measure with the competence of the SAPC as an organ of the state in enhancing access to healthcare for HIV treatment, in fulfilment of the state’s obligation under the Constitution,” Makgoka said.
“These are legitimate and compelling public interests.”
He said the IPA was wrong in believing that PIMART was a blanket licence for pharmacists to treat HIV patients.
“Its scope is limited and applies only to accredited pharmacists. It will not alter the scope of practice for medical practitioners. The fact is that medical practitioners do not have the exclusive rights to care for people living with HIV/AIDS. This is a collaborative effort involving various health professionals.”
The IPA had also submitted that pharmacists were not authorised to prescribe schedule 3, 4 and 5 medicines without a prescription.
However, the judge said, the Medicines Act carved out an exception to this with authorisation of the Director-General. It was through this that PIMART-accredited pharmacists could apply for permits to prescribe schedule 3 – 5 substances.
The appeal was dismissed with costs.
Certainly not all doctors oppose the idea of pharmacists initiating patients with HIV on treatment: the South African HIV Clinicians Society stated: “We look forward to supporting the rollout of PIMART which will further contribute to South Africa’s HIV response and progress towards the 2030 target of eliminating HIV as a public health concern.”
Neurons in the brain of an Alzheimer’s patient, with plaques caused by tau proteins. Credit: NIH
UVA Health scientists are calling for clinical trials testing the potential of HIV drugs called NRTIs to prevent Alzheimer’s disease after discovering that patients taking the drugs are substantially less likely to develop the memory-robbing condition.
The researchers, led by UVA’s Jayakrishna Ambati, MD, previously identified a possible mechanism by which the drugs could prevent Alzheimer’s. That promising finding prompted them to analyse two of the nation’s largest health insurance databases to evaluate Alzheimer’s risk among patients prescribed the medications. In one, the risk of developing Alzheimer’s decreased 6% every year the patients were taking the drugs. In the other, the annual decrease was 13%.
“It’s estimated that over 10 million people around the world develop Alzheimer’s disease annually,” said Ambati, founding director of UVA’s Center for Advanced Vision Science and the DuPont Guerry III Professor in the School of Medicine’s Department of Ophthalmology. “Our results suggest that taking these drugs could prevent approximately 1 million new cases of Alzheimer’s disease every year.”
NRTIs restrain inflammasomes
NRTIs, or nucleoside reverse transcriptase inhibitors, are used to prevent the HIV virus from replicating inside the body. But Ambati and his team previously determined that the drugs can also prevent the activation of inflammasomes, important agents of our immune system. These proteins have been implicated in the development of Alzheimer’s disease, so Ambati and his colleagues wanted to see if patients taking the inflammasome-blocking drugs were less likely to develop Alzheimer’s.
To do that, they reviewed 24 years of patient data contained in the U.S. Veterans Health Administration Database – made up heavily of men – and 14 years of data in the MarketScan database of commercially insured patients, which offers a broader representation of the population. They looked for patients who were at least 50 years old and were taking medications for either HIV or hepatitis B, another disease treated with NRTIs. They excluded patients with a previous Alzheimer’s diagnosis.
In total, the researchers identified more than 270 000 patients who met the study criteria and then analysed how many went on to develop Alzheimer’s. Even after adjusting for factors that might cloud the results, such as whether patients had pre-existing medical conditions, the researchers determined that the reduction in risk among patients on NRTIs was “significant and substantial,” they report in a new scientific paper.
The researchers note that patients taking other types of HIV medications did not show the same reduction in Alzheimer’s risk as those on NRTIs. Based on that, they say that NRTIs warrant clinical testing to determine their ability to ward off Alzheimer’s.
If successful, the benefits could be tremendous, as Alzheimer’s rates are climbing dramatically. Nearly 7 million Americans are living with the disease today, but that number is expected to climb to 13 million by 2050. Further, the estimated annual cost of care for Alzheimer’s and other dementias could rise from $360 billion to almost $1 trillion, the Alzheimer’s Association reports.
“We have also developed a new inflammasome-blocking drug called K9, which is a safer and more effective version of NRTIs,” Ambati said. “This drug is already in clinical trials for other diseases, and we plan to also test K9 in Alzheimer’s disease.”
Sex workers in Vosloorus, Johannesburg and Springs talked to GroundUp about their struggle to access health services, particularly antiretroviral treatment, since the closures of US funded clinics. Photos: Kimberly Mutandiro
It’s afternoon on Boundary Road in Vosloorus. Sex worker Simangele (not her real name) hopes to secure her next client.
Making enough money to pay rent has always been a concern for Simangele. But now she has a new worry: how to keep up with her antiretroviral treatment.
Two months ago the closure of a mobile clinic — where Simangele and other sex workers in Vosloorus went for checkups and to collect their treatment — left her without access to the life-saving medication.
The mobile clinic was run by the Wits Reproductive Health and HIV Institute (WITS RHI) which heavily relied on US funding. The institute has been providing critical sexual and reproductive health services since 2018. The programme was one of many health facilities forced to halt services at the end of January in the wake of US funding cuts for global aid.
Speaking to GroundUp, Simangele says she ran out of antiretroviral medicines (ARVs) over a month ago and has resorted to borrowing a few tablets from a friend. “I don’t know what I will do because the tablets my friend gets give me side effects,” she says. (Antiretrovirals treat HIV. They have to be taken daily for life.)
She says the clinic closed without any warning or before they could give them transfer letters to public healthcare facilities. She is now dreading having to go to a public facility where she says sex workers are frequently discriminated against, particularly those who are undocumented.
We spoke to a dozen other sex workers in Joburg and in Springs who are worried about defaulting on their antiretroviral treatment following the closure of the Wits RHI clinics. The clinics also provided pre-exposure prophylaxis (PrEP) (to prevent HIV-negative people contracting HIV), and treatments for sexually transmitted infections, TB, sexual reproductive health services, and counselling.
A sex worker shows the last few ARVs she has left.
Another sex worker said, “The minute we go to public clinics, they will need documents, which some of us do not have … Wits made time to listen to our problems as sex workers. Even when we faced challenges with clients, they never judged us.”
Sisi (not her real name), who rents rooms and assists sex workers in Vosloorus, said she’s aware of several sex workers who have defaulted and no longer have access to condoms, lubricants, and treatment for sexually transmitted infections. “The Wits clinic did not discriminate against people without documents and would sometimes provide food, branded T-shirts, caps, and even jobs,” she said.
“Many of us will die”
We visited Zig Zag Road in Springs, where several sex workers said they were out or almost out of ARVs. When asked why they didn’t just go to a local clinic, they told GroundUp about instances where they experienced stigma while trying to access treatment at public clinics.
“I used to receive PrEP to help prevent HIV (from the Wits clinic). We would also receive birth control services. Now I can’t go to a public clinic because we are mocked for being sex workers,” said Siphesihle.
Ntombi, who waits for clients along End Street, attended one of the Wits clinics in Hillbrow which closed down. She said those on PrEP were given transfer letters before the clinic closed.
Other workers nearby told GroundUp that they now pay up to R250 for PrEP, which is more than they can afford.
Sisonke calls for urgent response to crisis
The Sisonke National Movement, which advocates for the rights of sex workers, has been raising the alarm since the closure of US-funded facilities. Before the closures, Sisonke was in talks with National Department of Health through the South African National AIDS Council about the provision of services to sex workers and other vulnerable groups, said the organisation’s spokesperson Yonela Sinqu.
She said that the department never answered activists when they asked what would happen should donor funds no longer be available for these facilities.
She said the plea for assistance without referral letters is made to all provinces, not only Gauteng. However, Gauteng is the only province that has approached us with the crisis of people without referrals, she said.
Department of Health spokesperson Foster Mohale has not responded to requests for comment.
Photo by Miguel Á. Padriñán: https://www.pexels.com/photo/syringe-and-pills-on-blue-background-3936368/
By Ufrieda Ho
Amid major disruptions caused by aid cuts from the United States government, the health department aims to enrol a record number – an additional 1.1 million – of people living with HIV on life-saving antiretroviral medicine this year. Experts tell Spotlight it can’t be business as usual if this ambitious programme is to have a chance of succeeding.
Government’s new “Close the Gap” campaign launched at the end of February has set a bold target of putting an additional 1.1 million people living with HIV on antiretroviral treatment by the end of 2025.
Around 7.8 million people are living with HIV in the country and of these, 5.9 million are on treatment, according to the National Department of Health. The target is therefore to have a total of seven million people on treatment by the end of the year. Specific targets have also been set for each of the nine provinces.
The initiative is aimed at meeting the UNAIDS 95–95–95 HIV testing, treatment and viral suppression targets that have been endorsed in South Africa’s National Strategic Plan for HIV, TB, and STIs 2023 – 2028. The targets are that by 2030, 95% of people living with HIV should know their HIV status, 95% of people who know their status should be on treatment, and 95% of people on treatment should be virally suppressed (meaning there is so little HIV in their bodily fluids that they are non-infectious).
Currently, South Africa stands at 96–79–94 against these targets, according to the South African National Aids Council (SANAC). This indicates that the biggest gap in the country’s HIV response lies with those who have tested positive but are not on treatment – the second 95 target.
But adding 1.1 million people to South Africa’s HIV treatment programme in just ten months would be unprecedented. The highest number of people who started antiretroviral treatment in a year was the roughly 730 000 in 2011. In each of the last five years, the number has been under 300 000, according to figures from Thembisa, the leading mathematical model of HIV in South Africa. According to our calculations, if South Africa successfully adds 1.1 million people to the HIV treatment programme by the end of 2025, the score on the second target would rise to just above 90%.
The record for the most people starting antiretroviral treatment in a single year was approximately 730 000 in 2011. (Graph by Spotlight, based on Tembisa data.)
The ambitious new campaign launches at a moment of crisis in South Africa’s HIV response. Abrupt funding cuts from the United States government – the PEPFAR funding – has meant that the work of several service-delivery NGOs have ground to a halt in recent weeks.
These NGOs played an important role in getting people tested and in helping find people and supporting them to start and restart treatment. The focus of many of these NGOs was on people in marginalised but high-risk groups, including sex workers, people who use drugs and those in the LGBTQI community. As yet, government has not presented a clear plan for how these specialised services might continue.
“We will need bridging finance for many of these NGOs to contain and preserve the essential work that they were doing till we can confer these roles and responsibilities to others,” says Professor Francois Venter, of the Ezintsha Research Centre at the University of the Witwatersrand.
He says good investment in targeted funding for NGOs is a necessary buffer to minimise “risks to the entire South African HIV programme” and the looming consequences of rising numbers of new HIV cases, more hospitalisations, and inevitably deaths.
Disengaging from care
South Africa’s underperformance on the second 95 target is partly due to people stopping their treatment. The reasons for such disengagement from HIV care can be complex. Research has shown it is linked to factors like frequent relocations, which means people have to restart treatment at different clinics over and over. They also have to navigate an inflexible healthcare system. A systematic review identified factors including mental health challenges, lack of family or social support, long waiting times at clinics, work commitments, and transportation costs.
Venter adds that while people are disengaged from care, they are likely transmitting the virus. The addition of new infections for an already pressured HIV response contributes to South Africa’s sluggish creep forward in meeting the UNAIDS targets.
The health department has not been strong on locating people who have been “lost” to care, says Venter. This role was largely carried out by PEPFAR-supported NGOs that are now unable to continue their work due to the withdrawal of crucial US foreign aid.
Inexpensive interventions
Other experts working in the HIV sector, say the success of the Close the Gap campaign will come down to scrapping programmes and approaches that have not yielded success, using resources more efficiently, strategic investment, and introducing creative interventions to meet the service delivery demands of HIV patients.
Key among these interventions, is to improve levels of professionalism in clinics so patients can trust the clinics enough to restart treatment.
Professor Graeme Meintjes of the Department of Medicine at the University of Cape Town says issues like improving staff attitudes and updating public messaging and communications are inexpensive interventions that can boost “welcome back” programmes.
“The Close the Gap campaign must utilise media platforms and social media platforms to send out a clear message, so people know the risks of disengagement and the importance of returning to care. The longer someone interrupts their treatment and the more times this happens, the more they are at risk of opportunistic infections, severe complications, getting very sick and needing costly hospitalisations,” he says.
Clinics need to provide friendly, professional services that encourage people to return to and stay on treatment, Meintjes says, and services need to be flexible. These could include more external medicine pick-up points, scripts filled for longer periods, later clinic operating hours, and mobile clinic services.
“We need to make services as flexible as possible. People can’t be scolded for missing an appointment – life happens. Putting these interventions in place are not particularly costly, in fact it is good clinical practice and make sense in terms of health economics by avoiding hospitalisations that result from prolonged treatment interruptions,” he says.
The Close the Gap campaign, Meintjes adds, should reassure people that HIV treatment has advanced substantially over the decades. The drugs work well and now have far fewer side effects, with less risk of developing resistance. More patients are stable on the treatment for longer and most adults manage their single tablet once-a-day regime easily.
Insights from our experiences
Professor Linda-Gail Bekker, Chief Executive Officer at the Desmond Tutu Health Foundation, says to get closer to the target of 1.1 million people on treatment by year-end will mean using resources better.
“Additional funding is always welcome, so are new campaigns that catalyse and energise. But we also need to stop doing the things we know don’t have good returns. For instance, testing populations of people who have been tested multiple times and aren’t showing evidence of new infections occurring in those populations,” she says.
There is also a need for better data collection and more strategic use of data, Bekker says. Additionally, she suggests a status-neutral approach, meaning that if someone tests positive, they are referred for treatment, while those who test negative are directed to effective prevention programmes, including access to pre-exposure prophylaxis (PrEP) for people at high risk of exposure through sex or injection drug use.
But Bekker adds: “We need to be absolutely clear; these people aren’t going to come to us in our health facilities, or we would have found them already. We have to do the work that many of the PEPFAR-funded NGOs were doing and that is going to the last mile to find the last patient and to bring them to care.”
She says the impact of the PEPFAR funding cuts can therefore not be downplayed. “The job is going to get harder with fewer resources that were specifically directed at solving this problem.”
Venter names another approach that has not worked. This, he says, is the persistence of treating HIV within an integrated health system. Overburdened clinics have simply not coped, he adds, with being able to fulfil the ideal of a “one-stop-shop” model of healthcare.
Citing an example, he says: “Someone might come into a clinic with a stomach ache and be vomiting, they might be treated for that but there’s no investigation or follow-up to find out if it might be HIV-related, for instance. And once that person is out of the door, they’re gone.”
Campaign specifics still lacking
The Department of Health did not answer Spotlight’s questions about funding for the Close the Gap campaign; what specific projects in the campaign will look like; or how clinics and clinic staff will be equipped or supported in order to find the 1.1 million people. There is also scant details of the specifics of the campaign online.
Speaking to the public broadcaster after the 25 February campaign launch, Health Minister Dr Aaron Motsoaledi said South Africa is still seeing 150 000 new infections every year. He said they will reach their 1.1 million target through a province-by-province approach. He used the Eastern Cape as an example.
“When you look at the 1.1 million, it can be scary – it’s quite big. But if you go to the provinces – the Eastern Cape needs to look for 140 000 people. Then you come to their seven districts, that number becomes much less. So, one clinic could be looking for just three people,” he said.
Nelson Dlamini, SANAC’s communications manager, says the focus will be to bring into care 650 000 men, as men are known to have poor health-seeking habits. Added to this will be a focus on adolescents and children who are living with HIV.
He says funding for the Close the Gap campaign will not be shouldered by the health department alone.
“This is a multisectoral campaign. Other departments have a role to play, these include social development, basic education, higher education and training, etc, and civil society themselves,” Dlamini says.
The province-by-province approach to reach the target of finding 1.1 million additional people is guided by new data sources.
“Last year, SANAC launched the SANAC Situation Room, a data hub which pulls data from multiple sources in order for us to have the most accurate picture on the status of the epidemic,” says Dlamini.
These include the Thembisa and Naomi model outputs and data from the District Health Information System and Human Sciences Research Council, he says adding that SANAC is working to secure data sharing agreements with other sectors too.
Dlamini however says the health department, rather than SANAC, will provide progress reports on the 10-month project.
Colourised scanning electron micrograph of HIV (yellow) infecting a human T9 cell (blue). Credit: NIH
Highly effective treatments for HIV have existed since the mid-1990s. But while these treatments keep people healthy, we do not yet have a safe and scalable way to completely rid the body of the virus. In this Spotlight special briefing, Elri Voigt takes stock of where we are in the decades-long search for an HIV cure.
As the science stands, the vast majority of the roughly eight million people in South Africa living with HIV will have to take treatment for the rest of their lives. This is because the antiretrovirals used to treat HIV prevents the virus from replicating but cannot eliminate it from the body. As soon as treatment is stopped, the virus rebounds, resulting in illness and eventually an early death.
A handful of people have been cured of HIV, but these “cures” involve very risky bone marrow transplants given as part of cancer treatment. The harsh reality is that 40 years into the HIV epidemic, and despite major scientific advances, we don’t yet have a viable cure for the roughly 40 million people on the planet who are living with the virus.
The good news, as one will see at any major AIDS conference these days, is that researchers around the world are working very hard to find a cure. In this #InTheSpotlight special briefing, we take a closer look at what progress has been made on this fascinating scientific journey and ask what the possible routes are toward an HIV cure.
What do we actually mean by a cure?
Dr Sharon Lewin, a leading figure in the world of HIV cure research and the inaugural director of the Peter Doherty Institute for Infection and Immunity in Melbourne, explains that a true “cure” for HIV would mean that there is not a single HIV infected cell left in a person’s body.
By contrast, “remission” would mean that the virus is still in the body, but it is being kept under control by the immune system. This could theoretically happen if the amount of HIV infected cells in a person’s body has been reduced to very low levels and the immune system’s ability to control those remaining cells has been enhanced. Basically, Lewin says, it is when the immune system does what antiretroviral therapy (ART) does without needing to take medication. Another term for this is ART-free viral load control.
There are some people living with HIV called “elite controllers” whose immune systems can naturally, without ART, control HIV. There are also extraordinary elite controllers, says Lewin, who through their immune response have been able to get rid of every single piece of the virus that they had in their bodies. Studying what is special about these rare people has been a key area of research in recent years.
Along with concepts like cure, remission, and control, it also helps to understand where vaccines fit in. As Jessica Salzwedel, the senior programme manager for research engagement at New York-based NGO AVAC, explains, a potential HIV vaccine might be therapeutic and not necessarily preventative. A therapeutic vaccine would be given to someone who is already living with HIV, in the hope that the vaccine would prime their immune system to better fight HIV or potentially clear it.
Why don’t we have a viable cure yet?
Finding cures for viral infections is not unheard of. In fact, one of the most consequential medical breakthroughs of the last decade or so was the development of a highly effective cure for hepatitis C. Unfortunately, it seems HIV is a much tougher nut to crack.
HIV works largely by invading a type of immune cell called a CD4 cell. Once inside, HIV writes its own genetic information into the cell’s DNA and then uses the cell’s machinery to produce more HIV. Eventually, the infected CD4 cell bursts and dies. Different types of antiretrovirals work by gumming up different stages of this process by which HIV invades and exploits CD4 cells. Most antiretroviral treatment regimens used today contain two drugs that target two different stages of this process. These medicines can drive HIV replication in the body down to near zero – which is why people who are stable on ART can live essentially normal, healthy lives.
Unfortunately, that is not the full story. As Lewin explains, the virus has a range of “tricks” that allows it to stay in someone’s body for much longer. One of those tricks is that HIV uses one of the immune system’s greatest assets against it. A person’s immune system contains cells that function as an immunological memory – essentially memory cells – which are designed to survive for a very long time. These memory cells, which include special CD4+ (CD4 positive) T-cells, contain information about which antigens it has encountered during a person’s lifetime. This helps the immune system recognise and kill those antigens faster the next time they enter the body.
HIV writes its own genetic code into some of these memory cells, which helps it stay in the body for as long as that person is alive. Lewin explains that once someone is on treatment, these immune system cells infected with HIV go silent and the virus stops replicating. These silent cells that contain infectious virus are rare, about one in every million, and can’t be found easily by the immune system, allowing the virus to hide in an inactive state but still able to release virus should the cell one day be activated.
These memory cells are found mainly in the lymph nodes, although they can also hide away in the gut, the spleen, and even the brain. Collectively, these HIV-infected cells in hiding are known as the latent reservoir. Should someone stop taking antiretroviral treatment, some of the cells in this latent reservoir could reactivate and start replicating again.
Lewin says researchers are getting better at finding these latent HIV-infected cells, but there still isn’t a way to easily tag these cells and destroy them.
Three lines of investigation
According to Lewin, researchers are exploring three broad strategies in search of an HIV cure.
Firstly, with a strategy called “shock and kill”, researchers try to reactivate (shock) the virus in the cells where it is hiding and then destroy (kill) it once it is flushed out. Such an approach will likely require at least two medicines – one to shock and one to kill. Unfortunately, attempts to find treatments that reliably shock HIV-infected cells out of their slumber has not borne much fruit so far.
Secondly, with “block and lock”, researchers hope to permanently silence the HIV that is hiding away in a person’s body. The aim here is to keep HIV latent for good, so that we never need to worry about killing it. This approach might involve using ART together with a latency promoting agent, of which several are currently being researched. “Block and lock” approaches have been picking up momentum in recent years.
Thirdly, with gene editing, researchers aim to “edit” cells to make them resistant to HIV or remove HIV from them. For example, CD4 cells can be modified to not have the specific receptor called CCR5 that HIV requires to gain entry into the cell. Essentially, if you remove the CCR5 receptor from a cell, HIV has no way in and the cell becomes immune to HIV. In this area, there have been some tantalising developments, but nothing yet that amounts to a workable cure. For example, in one study, people had their blood drawn, the CCR5 receptors removed from the CD4 cells in the blood, and then had the blood reinfused. It worked somewhat, but not nearly well enough to call it a cure.
These three categories are not the only way to think about potential cures.
Broadly, we can think about there being two big “buckets” of approaches for an HIV cure, says Salzwedel. The first “bucket” of approaches targets the virus, and those approaches are trying to remove HIV from the cell or “silencing” it so even if it is still present there is no replication. The other “bucket” of approaches looks at the host – or the person living with HIV – and improving their immune system so it can adequately kill HIV or make the cells that have HIV in them easier to spot so these cells can’t hide from the immune system. She says a combination of approaches from both “buckets” will probably need to be used for a cure.
A resource of HIV cure trials maintained by Treatment Action Group, a New York-based advocacy organisation, lists hundreds of clinical trials currently underway that are trying these different approaches or combinations of approaches.
What about the people who have been cured?
As mentioned earlier, one area of research has involved trying to understand “elite controllers”. Another critically important group of people in the search for a cure are the seven or so people who were living with HIV, but who have been cured. Some of these people, like Timothy Ray Brown and Adam Castillejo, have become minor celebrities in the HIV world.
Lewin explains that people like Brown and Castallejo, both of whom have essentially no HIV left in their bodies, had to go through interventions that can’t be replicated in everyone. Both had a type of blood cancer and were living with HIV. They had to undergo chemotherapy which wiped out their bone marrow, including the cells that had HIV in them. They were then given a whole new bone marrow system through a donation from someone who was naturally resistant to HIV since their CD4 cells do not have CCR5 receptors. This allowed the latently infected cells to be “flushed out” of their bodies. One of the other people cured of HIV received a bone marrow transplant from umbilical cord blood.
Such transplants are not things you can do for everyone who is living with HIV, its expensive and the severe risks of the procedure can only be taken in people living with both HIV and certain cancers. Even so, these cases, says Salzwedel, has shown us that it is possible to cure HIV and made us aware of some of the challenges.
Lewin says that cases like those of Brown and Castallejo helped advance gene editing approaches because they showed that not having CCR5 receptors makes CD4 cells essentially immune to HIV. This led to studies using special gene scissors – a technique called CRISPR – to find the gene for the CCR5 receptor in cells and remove it. CRISPR has also been used experimentally to remove HIV from cells.
So far only a small number of studies have been conducted using CRISPR-based gene editing approaches in an attempt to cure HIV – and these were mostly in the lab or in mice and monkeys. The first human gene editing study for CCR5 was done ex vivo – meaning cells were taken out of the body, edited, and then reinfused into the body. The first clinical trial of CRISPR for HIV in vivo – meaning it is done inside the body – is currently underway and early results were presented in July at the AIDS 2024 conference. While initial results in monkeys were promising, the early findings in humans were disappointing. EBT-101, the specific type of CRISPR treatment, did not prevent HIV from returning once treatment was stopped – although one study participant’s HIV only started replicating again after 16 weeks. A longer follow-up study is currently open in the United States for enrolment.
Gene editing could also potentially be used to strengthen the immune system. This could work, Lewin explains, by inserting a new gene that produces an antibody against HIV into cells and then putting those cells back into the body. “So instead of giving an infusion of an antibody, your own body makes the antibody. And that’s been done successfully in people with HIV on ART in two separate clinical trials and more recently in infant monkeys where ART was stopped,” she says. “The investigators injected CRISPR that delivered two different antibodies to infant monkeys who are infected with a monkey adapted form of HIV virus and on ART. The infant monkey’s muscle cells then start making the antibodies, and when they stopped ART, the antibodies kicked in and kept the virus under control, so that’s the most successful type of gene therapy,” Lewin says.
Boosting the immune response
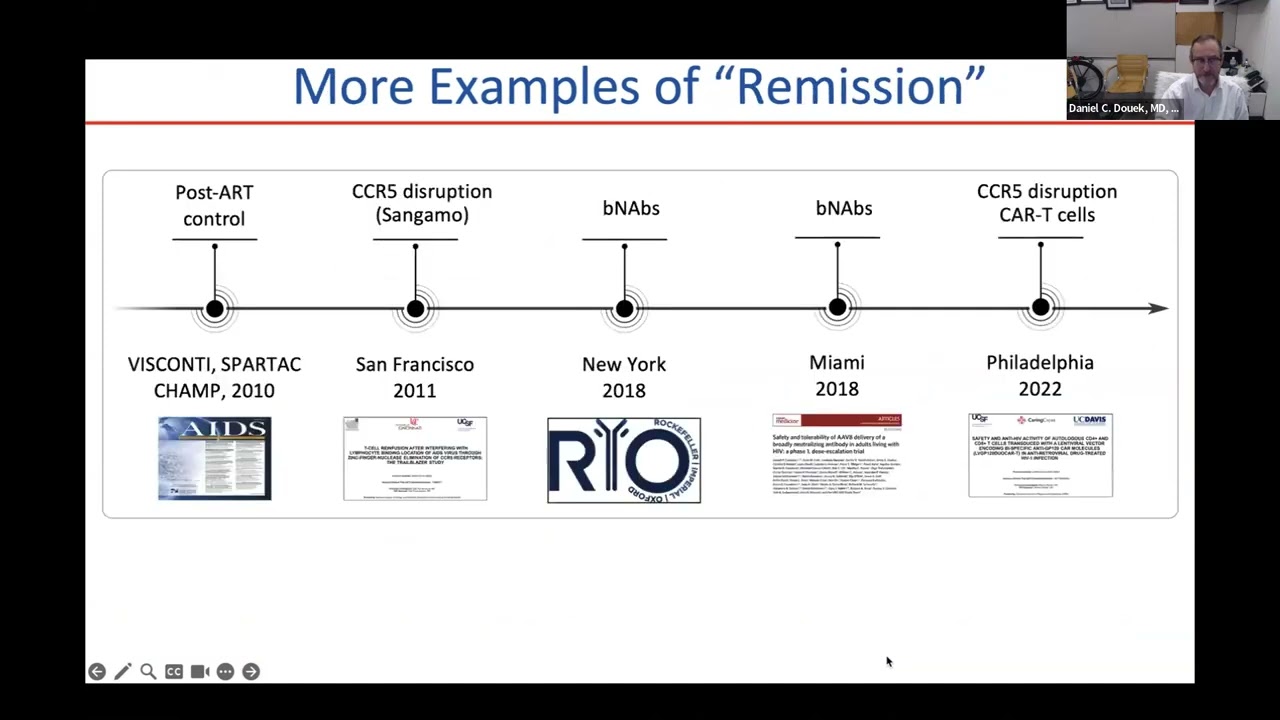
Another promising avenue is broadly neutralising antibodies (bNAbs) – the broadly refers to the ability of these antibodies to neutralise a range of different HIV viral strains. Broadly neutralising antibodies can work as an antiviral while present in the body, but they can also trigger the immune system to control the virus and, according to Lewin, figuring out how bNAbs do this is a very important part of current cure research. Broadly neutralising antibodies that are HIV specific, work by binding with the virus and eliminating it while also enhancing a person’s immune system so it can control the virus that remains in the body by hiding in the immune system’s memory cells. Broadly neutralising antibodies potentially have this beneficial effect on immune control by activating CD4 and CD8 responses – part of the immune system’s defence – to kill HIV cells. There have been several clinical trials where a subset of participants who have been given bNAbs have been able to control the HIV virus for six months after stopping ART and when the bNAbs are no longer detected in blood. The scientific challenge is that this beneficial effect was only seen in a subset of participants and the duration of control is not fully understood as most clinical trials only assess participants up to 24 weeks off of ART.
Lewin says a small study has also looked at using anti-PD1, an antibody that reverses immune system exhaustion and essentially “revs” up the immune system to keep fighting HIV. Early study findings were presented at the Conference on Retroviruses and Opportunistic Infections (CROI) this year. Participants stopped ART and were given four doses of the antibody, called Budigalimab, or placebo over 29 weeks. Six out of the nine people who received the antibody had delayed viral rebound and/or ART free control, and two people had viral control off ART for over 29 weeks. The antibody will now be evaluated in a larger study.
Additional approaches, according to Dr Daniel Douek, an expert in immunology and the Chief of the Human Immunology Section at the National Institute of Allergy and Infectious Diseases in the United States, include HIV vaccines, which so far have not generated a strong enough immune response to be considered successful. Douek was speaking on an IAS webinar on HIV cure research. Another promising approach is to start someone on ART as quickly as possible after infection in the hope of preventing the establishment of the latent reservoir.
Suppressing the immune system with a drug has also been tried, says Douek, and research so far in this area warrants further investigation. While it seems counterintuitive, the researchers wanted to see if suppressing immune system cells might stop or reduce HIV replication because the virus likes to replicate in activated immune cells. People living with HIV, even when on treatment have a lot of activated immune cells. The drug Ruxolitnib, which is used to treat graft-versus-host disease in transplant patients, was given to 60 people living with HIV alongside their HIV treatment. After five weeks, there was a decrease in markers of immune activation and cell survival. And between five and 12 weeks of using this combination, those with large viral reservoirs displayed signs that their reservoirs were reducing in size. However, Douek cautioned that much more work needs to be done before we can draw firm conclusions about the value of this approach .
What comes next?
Though we don’t yet have a viable cure for HIV, Lewin says a lot of progress has been made, especially over the decade and a half since Brown was cured. We now know a lot more than we did about the virus and how it hides away in cells. Today, she says, we have cure interventions that work well in monkeys and some interventions being investigated in human clinical trials have induced ART-free viral control in some participants. But she is also clear that it will probably be “a very long time” before you can go to your doctor and get an HIV cure.
In this #InTheSpotlight special briefing, we have focused on the science, but as we have learnt from the new hepatitis C cures and from HIV prevention injections, the journey from the lab to your local clinic can be a very long one and involves far more than just the science.
According to Lewin, a successful HIV cure will have to tick several boxes. She says one needs an intervention that is durable, so that it leads to ART-free viral load control over a prolonged period of time. At this point, an intervention that allows for control over two, three or five years, is seen as worthwhile. Although the ideal would be to give something once and have ART-free viral load control over a lifetime. The intervention also needs to be scalable, so it can be given to a lot of people. It also needs to be cheap.
And if there is one insight we’ve gained over our many years covering HIV, it is that affordability and sufficient supply are not things we can take for granted. Given that many of the potential cures involve treatments that are substantially more complicated to produce and administer than antiretrovirals, the challenges here might be more acute than what we’ve seen before.
That we will eventually get a cure is also by no means inevitable. This is why it is critically important that governments and philanthropies continue to invest in cure research and support programmes such as the International AIDS Society’s Toward an HIV Cure initiative. Among others, this initiative is helping to build the capacity needed to conduct cure research in low-and-middle income countries.
Right now, even under a best-case scenario, a world without a cure will mean that many millions of people will still be living with HIV until late in the 21st century. A successful cure could change this trajectory. Ultimately, Salzwedel is right when she says: “We can’t really end an epidemic without a cure”.
A University of Minnesota Medical School research team has found that giving iron supplements to children living with human immunodeficiency virus (HIV) in sub-Saharan Africa could be an important first step in optimising brain development.
The study, published in Lancet HIV, demonstrates that iron, while often withheld from children with HIV due to fear of increasing infection risk, is in fact beneficial. This finding paves the way for future research examining iron’s role in neurodevelopmental outcomes in children with HIV.
“With the success and widespread availability of antiretroviral therapy (ART), children with HIV in sub-Saharan Africa are living longer, and optimising their brain development is a new public health imperative,” said Sarah Cusick, PhD, associate professor at the U of M Medical School and a member of the Masonic Institute for the Developing Brain.
Between May 2018 and November 2019, researchers enrolled 200 children with HIV and anaemia who had received ART for at least six months. The study participants were randomly chosen to receive either iron supplements or a placebo for three months. Children who received iron had higher haemoglobin concentrations and better markers of iron nutrition than those who received the placebo. There also was no evidence of increased risk of infection.
According to Dr Cusick, further research is needed to assess brain development and infection risk over a longer period of time.
Photo by Miguel Á. Padriñán: https://www.pexels.com/photo/syringe-and-pills-on-blue-background-3936368/
By Nthusang Lefafa
Despite some improvement over the past three years, the North West province continues to experience medicine shortages, according to a survey by a community clinic monitoring initiative. We unpack the latest findings and ask why shortages persist in the province.
Some people in need of HIV or tuberculosis (TB) medicines were sent home empty handed after visiting clinics in the North West. This is according to the latest survey of public healthcare services in the province published by community-led clinic monitoring group Ritshidze. The survey data was collected in April and May this year.
Of the roughly 490 000 people living with HIV in North West, around 380 000 (77%) are on antiretroviral treatment, according to figures from Thembisa, the leading mathematical model of HIV in South Africa. Antiretroviral treatment is recommended for everyone living with the virus.
According to Ritshidze, besides HIV and TB medicines, other commonly reported stockouts at clinic-level include pain medicines (such as Paracetamol and Ibuprofen), cardiac medicines (such as Aspirin), contraceptives, dry stock (gauze, bandages, needles), maternal health medicines, psychiatric medicines, and different vaccines.
Out of the 72 facilities surveyed in the province, medicine stockouts lasting one to three months were reported at 20 and stockouts lasting three to six months were reported at six.
‘Failed to comply’
The North West health department, according to Ritshidze, has failed to comply with national guidelines recommending that people living with HIV should be provided with a three or more month supply of antiretrovirals at a time. They found that 71% of people surveyed in 2024 received antiretroviral refills of three to six months – in each of the previous three years this number was below 30%. There was large differences between districts, with 97% of people surveyed in Bojanala district reporting getting a 3 month supply of ARVs — compared to 37% in Dr Kenneth Kaunda.
Giving people longer antiretroviral refills like this means people do not have to visit health facilities as often to collect their medicines.
Various factors influence giving more people longer antiretroviral refills, Tebogo Lekgethwane, Director of Media and Communications in the province’s health department, told Spotlight.
A crucial factor, he said, is that patients must have a good track record of collecting their medication as well as a history of a documented undetectable viral load. “There’s therefore a criteria for multi-month supply which includes the fact that patients should have been on treatment for six months, they are compliant and clinically stable,” said Lekgethwane.
No “crisis” of medicine shortages
While the year-on-year comparisons should not be overinterpreted – Ritshidze themselves advise caution – the numbers nevertheless provide some indication that when it comes to medicines stockouts things are trending in the right direction. The total number of stockouts in the province reported to Ritshidze plunged from 895 in 2021 to 148 in 2024 – over the same period stockouts of HIV medicines went from 115 to 19 and stockouts of TB medicines from 28 to 7.
Lekgethwane was at pains to point out that Ritshidze’s findings do not necessarily represent the actual picture of the entire province. He said that the department believes that the Ritshidze report is subjective and relies on isolated incidents. These incidents, Lekgethwane said, are often quickly addressed.
“The current provincial medicine availability report shows that medicine availability has stabilised above 80%. As at the end of June 2024, ARV stock was at 89.5%, Expanded Programme on Immunisation and Contraceptives remained above 90%, TB treatment at 79%, Oncology treatment at 81.7% and Diabetes Mellitus at 85.8%. Therefore the province does not have a crisis of medicine shortages,” he said.
Asked what exactly these percentages mean, Lekgethwane said that it indicates the actual medicines stock available in the province in relation to what is required.
A pharmacy expert consulted by Spotlight further explained that the percentage indicates the percentage of medicines on a list or in a class that is available in the province.
The way these numbers are tracked is somewhat tricky. Firstly, if a clinic is supposed to have 10 different HIV medicines in stock, but they only have 8 in stock, then its HIV medicines availability would be at 80% (having a single pack of a medicine counts as having it in stock). When many facilities are considered together, as with an entire province like North West, the key indicator looks at what percentage of those facilities have medicines availability above 90%. We thus understand the figures shared by Lekgethwane to mean that 89.5% of facilities, depots and so on in the province have HIV medicines availability above 90%.
Catching up with payments
Past medicine shortages in the province were partly attributed to companies ceasing delivery of medicine due to non-payment of invoices. While the North West health department was under National Department of Health administration in 2020, the offices at the Mmabatho Medical Depot was raided. The search uncovered a number of unpaid invoices worth millions, some dating back to 2014. One unpaid invoice was for more than R16 million.
Bolstered by a Pharmaceutical Intervention Team to address medicine shortages, Lekgethwane said the department’s payments system is now in top shape.
“Payment of suppliers has remained a priority and the finance unit has assisted the team by making good progress on payments of supplier accounts. The unit continues to investigate and intervene when suppliers indicate their account status to the pharmacies.
“This has led to an increased number of deliveries from suppliers to the depot and increased direct deliveries to pharmacies from contracted companies as well as deliveries of main orders, allocation of orders and emergency orders from the depot to the pharmacies,” he said.
“The Department can confidently confirm that the financial management of pharmaceuticals has been improved resulting in 97% of 2024/2025 accruals being paid and remaining with only two accounts that are on hold. The two accounts that are on hold will only be paid once their compliance requirements are sorted,” said Lekgethwane.
He said that the intervention team has the capacity to assess and intervene, in among others, pharmaceutical supply chain issues, system effectiveness, distribution and delivery processes, storage capacity, human resource capacity and safety issues.
Lekgethwane said the team’s first priority was to assess the Mmabatho Medical Depot before moving onto pharmacies in hospitals and clinics across the province.
Getting medicines to rural areas
While Ritshidze also raised concern around transportation for the delivery of medicines, the department said transportation has never been a challenge.
“There are contracted service providers who deliver to the Mmabatho Medical Depot and the depot delivers to hospitals. Clinics receive their medicine from their referral hospital,” said Lekgethwane.
“However, the department is currently implementing the bulk pharmacies for districts to bring medicines closer to facilities”, he added. A bulk pharmacy is a medicine storage facility which serves as a medical depot. It is situated in the districts and helps with bringing medicines closer to rural areas so that medicines do not have to be transported from major towns.
In this regard, Lekgethwane said the Dr Kenneth District Bulk Pharmacy was recently opened and soon the General De la Rey Bulk Pharmacy will open.
He said the department is confident that the use of these bulk pharmacies will improve medicine storage and distribution capacity.
Shortage of pharmacists and pharmacy assistants
The Ritshidze report found that only 9% of surveyed facilities had a pharmacist and only 18% had a pharmacist assistant. Government regulations state that either pharmacists or pharmacy assistants should be responsible for stock receiving orders and updating the stock visibility system. However, Ritshidze found that enrolled nurses, enrolled nurse assistants, facility managers, and even cleaners acted in that capacity at some clinics.
The province has a 6% vacancy rate for pharmacists while 342 are currently employed, according to the 2024/2025 health department annual performance plan tabled in the North West Provincial Legislature earlier this month. The plan states that the department’s organisational structure makes provision for 10 pharmacists to be appointed in the province for every 100 000 uninsured individuals.
The DA’s Hendriette van Huyssteen says there is a challenge of pharmacists and pharmacy assistants where there are clusters of less than 10 000 uninsured individuals (where one pharmacist would be allocated for 10 000 uninsured individuals) and the clinics servicing them are far removed from one another.
“With the NHI [National Health Insurance] being signed into law, the number of pharmacists will become only a greater challenge. The cost per pharmacist employee stands at R765 000.00 per annum. It is unclear as to where the funding would come from for the remuneration of the additional pharmacists needed under the NHI, as even the NHI Act is unclear in this regard,” she said.
Notwithstanding the issue of budget constraints, the training of more pharmaceutical staff is integral to having fully functional health systems, said Professor Andrew Robinson. He is a deputy dean in the Faculty of Health Sciences at North West University (NWU). He was previously a deputy director general in the North West health department.
“To improve the pharmaceutical skills in the province, the NWU must ensure it aligns its pharmacy training to address the skill needs of the provincial health department to ensure equitable health service delivery to all, which is necessary for successful implementation of the NHI,” he said.