New Year’s Day saw the Gauteng Department of Health welcoming 112 babies into the world, the lion’s share of more than 400 births in total for the country. According to data released by Gauteng Health on X/Twitter, in the province’s public healthcare facilities, there were a total of 59 boys and 53 girls. Thelle Mogoerane Regional Hospital topped the table with 10 babies, followed by Chris Hani Baragwanath Academic Hospital (CHBAH) with 9 babies. But all of this was relatively quiet compared to Christmas Day, which saw more than three times the New Years’ Day number.
MEC Nkomo Nomantu together with MMC for Health Rina Marx joined the postpartum mothers at Dr George Mukhari Academic Hospital on the morning of New Year’s Day in welcoming their new arrivals. Gauteng’s academic hospitals recorded 19 births, while there were 10 births at the tertiary hospitals. Regional and district hospitals had 69 births and community healthcare centres had 14.
Christmas Day saw 387 babies born, 201 of them girls and 186 boys. CHBAH welcomed the most, with 46 births, followed by Tembisa Hospital with 38.
Like many countries, South Africa has a shortage of healthcare workers – particularly of doctors. One response to such shortages is task-shifting – in short, to let doctors focus on the things only they can do, and to shift some other less specialised tasks to other healthcare workers like nurses or pharmacists.
Task-shifting can take many forms. Earlier this year Spotlight reported on a court case that gave the green light to specially trained pharmacists to dispense antiretroviral treatment without a script (the judgement is being appealed). Similarly taking pressure off public sector clinics, the Department of Health has for several years now allowed some people to pick up their medicines at participating private sector pharmacies or other pickup points. Less well implemented, was the introduction of clinical associates in 2008 as a new type of mid-level healthcare worker that can take some of the pressure off of doctors and stand-in for them in some situations.
Probably the most impactful example of task-shifting in South Africa, however, was the introduction of Nurse Initiated and Managed Antiretroviral treatment (NIMART) in 2010.
What is NIMART?
Dr Silingene Ngcobo, a lecturer at the School of Nursing and Public Health at the University of KwaZulu-Natal and a Board Member of the Southern African HIV Clinicians Society, says NIMART is a clinical management program for people living with HIV which is driven by registered nurses. This means that registered nurses can independently manage a person living with HIV, starting from screening and diagnosis, all the way to treating, and monitoring throughout the HIV care continuum in the absence of a medical doctor.
As explained by Mmotsi Moloi, Training Programme Manager at the Aurum Institute (an NGO), prior to the introduction of NIMART in 2010 only doctors were authorised to prescribe antiretroviral therapy.
The rollout of antiretrovirals in South Africa technically started in 2004, but it only gathered momentum after the end of state-backed AIDS denialism in 2008. It soon after became clear that South Africa would not have enough doctors to handle the demand for HIV treatment and nurses would have to be roped in.
“The waiting lists became long, and the doctors could not meet the increasing demand of clients in need of antiretroviral treatment, this led to the death of clients while awaiting to be initiated,” says Moloi. “There was an urgent need to remedy the situation which was to decentralise management of HIV to Primary health care facilities and professional nurses to be trained and authorised to manage HIV infected clients.”
Ngcobo says nurses are often the only healthcare providers available to provide HIV prevention, care, and treatment services. She says the South African healthcare delivery system approach has changed from hospital-centred care to promotion of health and prevention of disease through primary healthcare and the introduction of NIMART fits this shift.
Hard to quantify
According to estimates from Thembisa, the leading mathematical model of HIV in the country, the number of people taking HIV treatment in South Africa increased from 1.2 million in 2010 to 5.7 million in 2022. How big a part NIMART played in this remarkable scale-up of treatment is hard to quantify, but that it played a pivotal role seems clear.
A review study published in 2021 that looked back at 10 years of NIMART in South Africa, found that adequate NIMART training “results in improved knowledge of HIV management, greater confidence and clinical competence, particularly if accompanied by mentoring”.
The review summarised results from several smaller studies conducted in different provinces on NIMART – which show, on a small scale at least, what potential impact NIMART has had. Among other things, the training of nurses to initiate and manage HIV treatment led to feelings of empowerment, and when coupled with appropriate training and support can “lead to increased quality of patient care, confidence and professional development”.
Studies conducted in Johannesburg cited by the review found that NIMART training increased access to HIV treatment, reduced workloads at referral facilities, and reduced referrals to tertiary hospitals. Nurses also saw an “improvement in the quality of life of their patients and the retention of patients in care, which they felt reflected the success of NIMART”.
When asked how many NIMART-qualified nurses we have in the country, Foster Mohale, spokesperson for the National Department of Health, says he can’t provide an exact number since they no longer collect data on NIMART since it has been incorporated in broader HIV training. He also says that provinces are the custodians of data for all trained healthcare workers and points out that the numbers change all the time due to attrition.
What NIMART nurses do
Ngcobo says NIMART nurses assess and screen people living with HIV for treatment eligibility, initiate antiretroviral therapy, provide adherence counselling and monitoring, screen for opportunistic infections, offer various preventative therapies, psychological support, as well as appropriate referrals to other members of the disciplinary team, and oversee repeat visits throughout the healthcare user’s life while managing any other health condition that the person might have.
Nurses also have to support people with tuberculosis and non-communicable diseases (such as diabetes and hypertension) to take treatment as prescribed.
“For effective management of other diseases, NIMART nurses should actually work with all other conditions because a person living with HIV still can gets various other conditions which still need to be managed. Therefore, the role of [the] NIMART nurse is to wholistically manage the patient and provide all the necessary healthcare services that the healthcare user in front of them will be requiring,” says Ngcobo.
Training requirements
The NIMART programme has changed somewhat since its launch back in 2010. Mohale says the programme now also covers the majority of healthcare professionals like medical doctors, pharmacists, registered or professional nurses, and other healthcare professionals who are authorised by their statutory bodies to assess, diagnose, prescribe, and dispense medications. He says in 2017 NIMART was changed to “Basic HIV for Health Care Professionals”, but the name NIMART is still in wide use.
The essence of the programme however remains that a professional nurse, or other qualifying healthcare professional, must complete special training (see this online course for example) before they are authorised to prescribe HIV treatment and manage the treatment and care of people living with HIV. Training typically requires both an exam and some practical work, ideally with the support of a mentor.
All prescribing by nurses in the public sector relies on section 56(6) of the Nursing Act, which allows an exception to the Medicines Act and other health-related laws, explains Andy Gray, Senior Lecturer in pharmaceutical sciences at the University of KwaZulu-Natal. “They therefore do not need section 22A(15) permits or section 22C(1)(a) dispensing licences in terms of the Medicines Act,” he says.
The legalities of how nurse prescribing works in South Africa is set out in a 2016 policy document issued by the National Department of Health. Amongst others, the document states that, “a nurse may only perform the functions authorised by Section 56(6) in public sector facilities in the district or municipality where the authorisation was granted to him/her”. In other words, nurses who move to jobs at other facilities or in other districts will often require new authorisation before they may prescribe medicines such as antiretrovirals.
Some concerns
But there are signs that training and mentorship is not functioning optimally across the board.
“There is non-standardised training and inadequate mentoring as the country doesn’t have enough trainers,” says Mohale. “There are human resource constraints for both trainers and nurses to be trained. Some districts rely on their district support partners to carry out trainings on their behalf.”
“Staff shortage from the facilities also leads to some nurses not being able to be trained due to demand for other health services at their service delivery points. Some challenges include failure to identify and manage drug-drug and drug-food interactions which are important in making sure that the patients are suppressing their viral loads,” he adds.
Mohale’s comments echo several barriers to the success of NIMART that were identified in the 2021 review study, including: “non-standardised training, inadequate mentoring, human resource constraints, health system challenges, lack of support and empowerment, and challenges with legislation, policy and guidelines”.
Mayo Clinic researchers mapped how the measles virus mutated and spread in the brain of a person who succumbed to a rare, lethal brain disease. New cases of this disease, which is a complication of the measles virus, may occur as measles re-emerges among the unvaccinated, say researchers.
Using the latest tools in genetic sequencing, researchers at Mayo Clinic reconstructed how a collective of viral genomes colonised a human brain.
The virus acquired distinct mutations that drove the spread of the virus from the frontal cortex outward.
The highly contagious measles virus infects the upper respiratory tract where it uses the trachea as a trampoline to launch and spread through droplets dispersed when an infected person coughs or sneezes.
Dr Cattaneo pioneered studies on how the measles virus spreads throughout the body. He first began to study the measles virus about 40 years ago and was fascinated by the rare, lethal brain disease called subacute sclerosing panencephalitis (SSPE), which occurs in about 1 in every 10 000 measles cases.
It can take about five to 10 years after the initial infection for the measles virus to mutate and spread throughout the brain.
Symptoms of this progressive neurological disease include memory loss, seizures and immobility.
Dr. Cattaneo studied SSPE for several years until the lethal disease nearly disappeared as more people were vaccinated against measles. But now, measles is resurging due to vaccine hesitancy and missed vaccinations.
During the COVID pandemic, millions of children missed receiving their measles vaccinations, which has resulted in an estimated 18% increase in measles cases and 43% increase in death from measles in 2021 compared to 2022 worldwide, according to a recent Centers for Disease Control and Prevention (CDC) report.
“We suspect SSPE cases will rise again as well. This is sad because this horrible disease can be prevented by vaccination. But now we are in the position to study SSPE with modern, genetic sequencing technology and learn more about it,” says Iris Yousaf, co-lead author of the study and a fifth-year Ph.D. candidate at Mayo Clinic Graduate School of Biomedical Sciences.
Dr Cattaneo and Yousaf had a unique research opportunity through a collaboration with the CDC. They studied the brain of a person who had contracted measles as a child and had succumbed to SSPE years later as an adult.
They investigated 15 specimens from different regions of the brain and conducted genetic sequencing on each region to piece together the puzzle of how the measles virus mutated and spread.
The researchers discovered that, after the measles virus entered the brain, its genome began to mutate in harmful ways over successive generations, creating a population of varied genomes.
“In this population, two specific genomes had a combination of characteristics that worked together to promote virus spread from the initial location of the infection – the frontal cortex of the brain – out to colonise the entire organ,” says Dr Cattaneo.
The next steps in this research are to understand how specific mutations favour virus spread in the brain. These studies will be done in cultivated brain cells brain organoids. This knowledge may help in creating effective antiviral drugs to combat virus spread in the brain. However, pharmacological intervention in advanced disease stages is challenging, and preventing SSPE through measles vaccination remains the best method.
It has long been known that people with diabetes are at a substantially increased risk of developing severe lung disease if they become infected with viruses such as influenza, as well as other pathogens. When the COVID-19 pandemic started in early 2020, it became even more important to understand this mysterious phenomenon. It became clear that people with diabetes were at a significantly higher risk of coming down with severe, even fatal, lung disease after developing severe COVID, but no one understood why. In fact, some 35% of the pandemic’s COVID mortalities had diabetes.
Now, research conducted at the Weizmann Institute of Science and published in Nature has revealed how, in diabetics, high levels of blood sugar disrupt the function of key cell subsets in the lungs that regulate the immune response. It also identifies a potential strategy for reversing this susceptibility and saving lives.
Prof. Eran Elinav‘s team in his lab at Weizmann, headed by Drs. Samuel Nobs, Aleksandra Kolodziejczyk and Suhaib K. Abdeen, subjected multiple mouse models of types 1 and 2 diabetes to a variety of viral lung infections. Just as in diabetic humans, in all these models the diabetic mice developed a severe, fatal lung infection following exposure to lung pathogens such as influenza. The immune reaction, which in nondiabetics eliminates the infection and drives tissue healing, was severely impaired in the diabetic mice, leading to uncontrolled infection, lung damage and eventual death.
Next, to decode the basis of this heightened risk, the team performed an evaluation of gene expression on the level of individual cells, in more than 150 000 single lung cells of infected diabetic and nondiabetic mice. The researchers also performed an extensive array of experiments involving immune and metabolic mechanisms, as well as an in-depth assessment of immune cell gene expression in infected diabetic mice. In the diabetic mice they identified a dysfunction of certain lung dendritic cells, the immune cells that orchestrate a targeted immune response against pathogenic infection. “High blood sugar levels severely disrupt certain subsets of dendritic cells in the lung, preventing these gatekeepers from sending the molecular messages that activate the critically important immune response,” says Nobs, postdoctoral fellow and study first author. “As a result, the infection rages on, uncontrolled.”
Next, they explored ways to prevent the harmful effects of hyperglycaemia in lung dendritic cells, as a means of lowering the infection’s risk in diabetic animals. Indeed, tight control of glycaemic levels by insulin supplementation prompted the dendritic cells to regain their capacity to generate a protective immune response that could prevent the cascade of events leading to a severe, life-threatening viral lung infection. Alternatively, administration of small molecules reversing the sugar-induced regulatory impairment corrected the dendritic cells’ dysfunction and enabled them to generate a protective immune response despite the presence of hyperglycaemia.
“Correcting blood sugar levels, or using drugs to reverse the gene regulatory impairment induced by high sugar, enabled our team to get the dendritic cells’ function back to normal,” says Abdeen, a senior intern who co-supervised the study. “This was very exciting because it means that it might be possible to block diabetes-induced susceptibility to viral lung infections and their devastating consequences.”
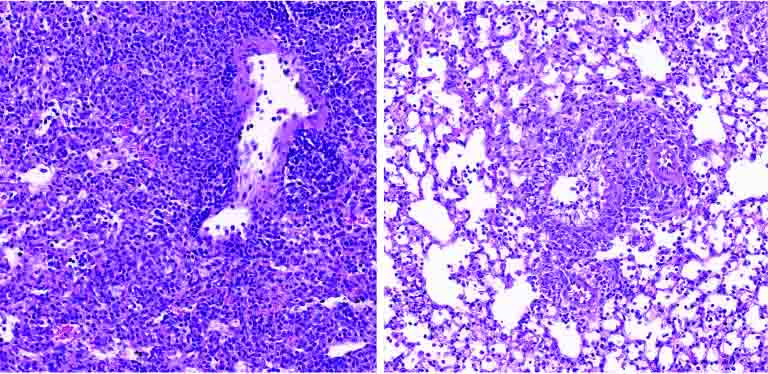
Lung tissue of a diabetic mouse (right) contains fewer immune cells (small purple dots) than that of a non-diabetic animal (left)
With over 500 million people around the world affected by diabetes, and with diabetes incidence expected to rise over the next decades, the new research has significant, promising clinical implications.
“Our findings provide, for the first time, an explanation as to why diabetics are more susceptible to respiratory infection,” Elinav says. “Controlling sugar levels may make it possible to reduce this pronounced diabetes-associated risk. In diabetic patients whose sugar levels are not easily normalized, small molecule drugs may correct the gene alterations caused by high sugar levels, potentially alleviating or even preventing severe lung infection. Local administration of such treatments by inhalation may minimize adverse effects while enhancing effectiveness, and merits future human clinical testing.”
The South African Health Products Regulatory Authority (SAHPRA) is aware of the product Lubri-A (Sterile Lubricating Jelly) manufactured by Electro-Spyres, classified as Class B medical device and currently being distributed across the country.
SAHPRA has been informed of multiple complaints received from health institutions, both public and private across the country. The complaints are as a result of a number of patients who became ill due to developing a fungal infection, caused by exposure to the fungal species, Wickerhamomyces anomalus (previously Candida pelliculosa) associated with use of Lubri-A (Sterile Lubricating Jelly).
Lubri-A is available in two presentations, the 2.5 g sachets and 50 g tubes.
Considering the wide usage of the product for lubricating purposes in medical and surgical procedures, the Regulator has taken a decision to urgently recall this product from the market as there are multiple contaminated batches, with the potential to cause serious and widespread nosocomial infections. SAHPRA is alerting healthcare professionals and the public to discontinue the use of the product, remove it from their inventory and return it through their normal distribution channel(s) with immediate effect.
As the source of the contamination of the product is still under investigation and not confirmed, all batches of Lubri-A are being recalled. Future manufacture and distribution of the product will be subject to review and authorisation by SAHPRA.
Classification of the recalls
The recall is being classified as a Class 1, Type A recall, which is associated with a serious product quality concern that may have severe consequences. This is a countrywide recall. The product is being recalled from hospitals, retail outlets, health care professionals, authorised prescribers and individual customers or patients.
What the public should know
Healthcare professionals that have used this product should contact their patients to determine any symptoms of infection after use of product.
The recall is limited to the product called LUBRI-A (2.5g and 50g sachets) and does not affect other lubricating gel products authorised for sale in South Africa.
The contact telephone numbers for Electro-Spyres are:
Landline: 011-608-3998 or 011-402-7208
WhatApp: +27-82-355-8862
“As a national regulatory authority, the recalling of medical products is a crucial measure to address safety concerns or quality issues so that we protect the health of the public. SAHPRA is recalling this product from the market as there are multiple suspected contaminated batches with the potential to cause serious and widespread nosocomial infections, ” indicates SAHPRA CEO, Dr Boitumelo Semete-Makokotlela.
An immune system protein that normally guards against fungal infections is also responsible for exacerbating certain autoimmune diseases such as irritable bowel disease (IBS), type 1 diabetes, eczema and other chronic disorders, new research from The Australian National University (ANU) has found.
The discovery, published in Science Advances, could pave the way for new and more effective drugs, without the nasty side effects of existing treatments.
In addition to helping to manage severe autoimmune conditions, the breakthrough could also help treat all types of cancer.
The scientists have discovered a previously unknown function of the protein, known as DECTIN-1, which in its mutated state limits the production of T regulatory cells.
These ‘guardian’ Treg cells are crucial to preventing autoimmune disease because they suppress the effects of a hyperactive immune system.
“Although the DECTIN-1 protein helps to fight fungal infections, in its mutated state it’s also responsible for exacerbating severe autoimmune disease,” lead author Dr Cynthia Turnbull, from ANU, said.
“Understanding how and why the mutated version of this protein causes autoimmunity in patients brings us a step closer to developing more effective drugs and offers new hope to more than one million Australians who suffer from some form of autoimmune disease.”
The scientists believe they can control the immune system by turning the DECTIN-1 protein on and off, like a light switch.
“Turning on the protein would lower the intensity of the immune system’s defensive response which would help to treat conditions such as autoimmune disease,” Professor Carola Vinuesa, from the Francis Crick Institute, said.
“On the other hand, turning off the protein could give the immune system a boost, sending its defensive mechanisms into overdrive and allowing the body to treat an entirely different set of diseases.
“The findings are exciting because there haven’t been many discoveries of so-called modifier proteins such as DECTIN-1, which can change the way the immune system behaves to the extent it can either cause a disease or prevent it.”
According to Dr Turnbull, this means DECTIN-1 could play a key role in treating cancer.
“Cancer cells can disguise themselves by releasing certain proteins and chemicals into the body that essentially render them invisible from the immune system’s natural defences,” she said.
“We think that by using drugs to turn off the DECTIN-1 protein, in combination with existing therapies, we can activate the immune system and help it identify and attack the cancerous cells.”
Current treatments for autoimmune?disease aren’t very effective and have a lot of damaging side effects.
This is because the majority of existing treatments suppress the entire immune system rather than targeting a specific area.
“That means it might not fix the exact problem behind the patient’s disease and could inadvertently make them vulnerable to infections. Many people on these kinds of treatments also get bacterial, fungal and viral infections which can make their autoimmunity worse,” Professor Vinuesa said.
Mutation found in family
By examining the DNA of a Spanish family, the researchers discovered the DECTIN-1 mutation was responsible for exacerbating the severity of a chronic autoimmune disease suffered by the family’s only child.
“We found the family was also carrying a mutated version of another immune system protein known as CTLA-4. The CTLA-4 mutation prevents guardian cells from working properly and is known to cause severe autoimmune disease in about 60 to 70 per cent of people who carry it in their DNA,” Dr Pablo Canete, from the University of Queensland, said.
“Strangely, the remaining 30 to 40 per cent of the population who carry this mutated protein don’t develop disease.
“We discovered the family’s only child had both the DECTIN-1 mutation and the CTLA4 mutation, while his parents had only one of each. This helped us identify why the child, who is now in his twenties, was the only person in the family to develop severe autoimmunity, ending a 20-year-long mystery behind the cause of his disease.
“By discovering the existence of mutated versions of modifier proteins such as DECTIN-1, we finally have an explanation for why some people develop severe autoimmune diseases while others don’t, even if they inherit gene mutations passed down from family members.”
Immunotherapy in combination with chemotherapy has become an important therapeutic treatment option in some patients with metastatic breast cancer. Which patients will benefit the most, however, remains unclear; current biomarkers such as PD-L1 that are used to predict response are mediocre at best. Vanderbilt researchers led a clinical trial combining atezolizumab, an immunotherapy, in combination with chemotherapy in patients with metastatic triple-negative breast cancer to both evaluate the efficacy of the treatment combination and to understand biomarkers of response to immunotherapy.
Atezolizumab became the first approved immunotherapy for breast cancer when the Food and Drug Administration granted it accelerated approval in 2019, but two years later, its maker voluntarily withdrew the indication after additional data from a follow-up clinical trial failed to corroborate its efficacy. Atezolizumab had been approved for metastatic PD-L1-positive triple-negative breast cancer in combination with the chemotherapy nab-paclitaxel. Results from Vanderbilt’s clinical trial, published in JAMA Oncology, indicate that this immunotherapy does have a clinically meaningful benefit with a different chemotherapy partner and the correlative analyses provide insight to which patients will respond.
The clinical trial combined atezolizumab with carboplatin – a chemotherapy that works differently than nab-paclitaxel. The new combination significantly improved progression-free and overall survival of patients with metastatic triple-negative breast cancer. Atezolizumab with carboplatin lengthened progression-free survival from a median of 2.2 months to 4.1 months. Overall survival increased from a median of 8.6 months for the control group, who received carboplatin alone, to 12.6 months for those who received the combination therapy.
The phase 2 randomized clinical trial was conducted at six cancer centers through the Translational Breast Cancer Research Consortium and involved 106 patients of diverse ethnicities.
“Triple-negative breast cancer is difficult to treat because we don’t have a clear target, and understanding the underlying factors that affect response to a treatment is key. This study is so important because we were able to collect biopsies in all of the participants and really understand factors that affect response,” said Vandana Abramson, MD, the Donna S. Hall Professor in Cancer Research and co-leader of the Breast Cancer Research Program at Vanderbilt-Ingram Cancer Center.
The researchers hypothesised that atezolizumab would have superior efficacy to carboplatin because the chemotherapy is a platinum agent, which causes structural DNA changes and generates neoantigens that may stimulate an immune response. Nab-paclitaxel chemotherapy works differently: it is a microtubule-stabilising agent that stops cancer cell division.
“The tremendous knowledge gained from our multidisciplinary analyses of the patients and their tumours will continue to be important for clinical decision-making. After our first description of the triple-negative breast cancer subtypes over 10 years ago, more recently, we refined the subtypes further into four, which were analysed in this study: two basal-like subtypes, a mesenchymal subtype and a lumen androgen receptor-expressing subtype. When we refined the triple-negative breast cancer subtypes, we revealed an immune-modulatory descriptor or correlation.
“This JAMA Oncology study and others continue to confirm that lymphocytes, as measured by the immune-modulatory correlation, have predictive value for better relapse-free survival for triple-negative patients. Further, this study provides evidence that the luminal androgen receptor subtype is more like oestrogen receptor-positive (or ER+) disease. Prior studies investigating immunotherapy in breast cancers have shown that patients with ER+ disease have less benefit from immunotherapy, and we found that to be the case with patients with luminal androgen-positive tumours in this trial,” said Jennifer Pietenpol, PhD, the study’s corresponding author.
Interestingly, patients with higher body mass indexes and uncontrolled blood glucose levels had greater benefit from atezolizumab with carboplatin. The researchers noted that these patients may have more immune cells upon which anti-PD1/PD-L1 therapies can act. A lower risk of disease progression was also associated with high mutation burden and increased tumour-infiltrating lymphocytes.
“In this study, we observed that patients received benefit with atezolizumab even if the tumours were PD-L1 negative. We also show that, like prior clinical trials in melanoma and renal and lung cancers, tumours with high mutation burdens and the presence of immune cells within or around the tumour receive greater benefit from immunotherapy. This makes sense because each mutation has the potential to be recognised as non-self by the immune system, increasing the probability of immune cells already positioned around the tumour to recognise and target the cancer,” said Brian Lehmann, PhD, Research Associate Professor of Medicine and lead correlative scientist on the study.
“One surprising finding was the trend toward greater benefit for patients with higher body mass indexes and patients with uncontrolled blood glucose at prediabetic and diabetic levels while on the study. Both obesity and diabetes are linked to systemic inflammation, and the increased benefit may be attributed to higher adipose tissue composition in the breast and augmented by metabolic syndrome conditions such as Type 2 diabetes. Further studies are necessary to validate these findings and delineate the effects of blood glucose and obesity on immunotherapy,”
The combination therapy was generally well-tolerated, and toxic effects were consistent with previous reports for atezolizumab. The most common drug complications on the combination arm of the clinical trial were low blood platelet counts, anaemia, lymphocytopenia, nausea, fatigue and increased liver enzymes. The participants identified as 69% white, 19% African American, 10% unknown and 1% Asian.
The holiday season is a time for joy and celebration but many Americans admit the endless flurry of activities make it difficult to eat healthy, exercise and get adequate rest, according to a new survey from The Ohio State University Wexner Medical Center.
Two-thirds of those surveyed said they overindulge in food, nearly 45% said they take a break from exercise and more than half report feeling tired and have less time for themselves. Plus, a third admit they drink more alcohol during the holidays.
“Holiday travel, activities with friends and family, and trying to get a bunch of things done can cause people to lose track of their healthy habits,” said Barbara Bawer, MD, family medicine physician at Ohio State Wexner Medical Center and clinical assistant professor of family and community medicine at The Ohio State University College of Medicine.
“If one healthy habit drops off, it can affect other areas very quickly.”
To make it through the holiday season with healthy habits intact, Bawer suggests trying to stick to a normal routine as much as possible while giving yourself some grace.
“Once you’re out of a routine, which typically happens around the holidays, it’s really hard to get back on track partly because the motivation is no longer there,” said Bawer.
When the invitations start to pile up and decadent menus feels tempting, Bawer offers this advice, “Remember that it’s OK to say no.”
To keep healthy habits in check, try the following:
Diet: When it comes to sustaining healthy eating habits, it’s important to plan ahead. If you have an evening event, don’t starve yourself all day. Eat a high protein, low carb meal earlier in the day so you don’t overeat.
You can indulge with a favorite dish or dessert but it’s OK to say no to sampling every entrée or treat so you’re not eating excess calories at each event.
Exercise: Try to keep the same exercise schedule. If an obligation prevents you from going to a fitness centre or going for a run, be flexible. It’s OK to say no to the gym and consider doing an activity with family and friends that keeps you moving like going for a walk or playing a game of basketball.
Sleep: Go to sleep and wake up at your normal times, even when travelling. Limit the use of supplements like melatonin, as long-term use can disrupt healthy sleep-wake cycles. It’s OK to say no to some invitations if you feel like you’re going to overextend yourself.
Alcohol: People may drink more during the holidays but binge drinking is never a healthy choice. Binge drinking is when a man consumes five drinks or a woman consume four drinks in one setting. It’s OK to say no to excessive drinking. If you do drink, try to stick to the recommended two drinks for men or one drink for women. Avoid drinking on an empty stomach and drink plenty of water.
“Small, consistent changes and slowly adding to them can help you reach your health goals,” Bawer said.
Survey results and methodology This survey was conducted on behalf of The Ohio State University Wexner Medical Center by SSRS on its Opinion Panel Omnibus platform. The SSRS Opinion Panel Omnibus is a national, twice-per-month, probability-based survey. Data collection was conducted from Oct. 20-23 among a sample of 1 007 respondents. The survey was conducted via web (n = 977) and telephone (n = 30) and administered in English. The margin of error for total respondents is +/-3.6 percentage points at the 95% confidence level. All SSRS Opinion Panel Omnibus data are weighted to represent the target population of U.S. adults ages 18 or older.
HFA outlines presidential petition to prevent decimation of the SA healthcare system
The NHI Bill presented to President Cyril Ramaphosa cannot be permitted, as in its current form, it will infringe the rights of all South Africans by destroying the South African healthcare system. The Health Funders Association (HFA) has petitioned the President to withhold assent of the Bill on constitutional and procedural grounds and intends to take the matter as far as necessary and to the Constitutional Court if need be.
“We have taken a strong stand by respectfully urging the President to withhold assent of the Bill, citing constitutional and procedural concerns that pose a significant threat to the integrity of the country’s healthcare system,” remarks HFA Chairperson Craig Comrie.
“Should the need arise, the HFA is prepared to escalate the matter to the courts. Our goal is to meticulously align the legislation with the authentic objectives of Universal Health Coverage and the principles enshrined in the South African Constitution.
“Our action in opposing the NHI Bill being signed into law protects the interests of ALL South Africans who will require healthcare in future, including the people we are duty-bound to safeguard through the medical schemes and healthcare administrators we represent,” Comrie says.
While expressing unwavering support for achieving Universal Health Coverage (UHC) in South Africa, the HFA questions Parliament’s endorsement of a bill that raises significant constitutional and procedural concerns and fundamentally cannot achieve a sustainable system of UHC.
Some of the primary concerns outlined in the letter include:
Constitutional concerns: The NHI Bill’s clear infringement on constitutional rights, particularly the right to access healthcare and freedom of choice for South Africans, and by implication, the right to life. The Bill is seriously flawed in that regard, undermining the rule of law.
Procedural concerns: Questioning the extent and effectiveness of public consultation during the drafting and review of the NHI Bill, where thousands of submissions resulted in no meaningful changes to the Bill, the HFA advocates for a more inclusive and consultative approach.
The letter implores President Ramaphosa to exercise the powers granted by the Constitution to refer the NHI Bill back to Parliament for review.
“In addition to petitioning the President directly as guardian of the Constitution, the HFA will oppose the NHI Bill in its current form through every possible avenue, including approaching the courts to set aside the Bill on constitutional and procedural grounds.
“The HFA will also seek a High Court interdict against implementation of the NHI Act until the merits of our case have been heard and ruled upon by the High Court.
Craig Comrie concludes, “It is with a heavy heart that we make this plea, urging the President to secure the rights and wellbeing of our people. We will persist to ensure that what is right triumphs in our nation. South Africa deserves leadership that prioritises the welfare of all of its citizens, above all.”
A study published in Nature Communications has revealed that the time at which we eat could influence our risk of developing cardiovascular disease. This study, suggests that eating a late first or last meal is associated with a higher risk of cardiovascular disease. It also appears that a longer night-time fasting duration is associated with a reduced risk of cerebrovascular disease such as stroke. The findings, suggest the importance of daily meal timing and rhythm in reducing cardiovascular disease risk.
The study was led by scientists from INRAE, the Barcelona Institute for Global Health, Inserm, and the Université Sorbonne Paris Nord.
Diet plays a major role in the development and progression of cardiovascular diseases. The modern lifestyle of Western societies has led to specific eating habits such as eating dinner late or skipping breakfast. In addition to light, the daily cycle of food intake (meals, snacks, etc) alternating with periods of fasting synchronizes the peripheral clocks, or circadian rhythms, of the body’s various organs, thus influencing cardiometabolic functions such as blood pressure regulation. Chrononutrition is emerging as an important new field for understanding the relationship between the timing of food intake, circadian rhythms and health.
Scientists used data from 103,389 participants in the NutriNet-Santé cohort (79% of whom were women, with an average age of 42) to study the associations between food intake patterns and cardiovascular disease. To reduce the risk of possible bias, the researchers accounted for a large number of confounding factors, especially sociodemographic factors (age, sex, family situation, etc.), diet nutritional quality, lifestyle and sleep cycle.
The results show that having a first meal later in the day (such as when skipping breakfast), is associated with a higher risk of cardiovascular disease, with a 6% increase in risk per hour delay. For example, a person who eats for the first time at 9 am is 6% more likely to develop cardiovascular disease than someone who eats at 8 am When it comes to the last meal of the day, eating late (after 9 pm) is associated with a 28% increase in the risk of cerebrovascular disease such as stroke compared with eating before 8 pm, particularly in women. Finally, a longer duration of night-time fasting – the time between the last meal of the day and the first meal of the following day – is associated with a reduced risk of cerebrovascular disease, supporting the idea of eating one’s first and last meals earlier in the day.
These findings, which need to be replicated in other cohorts and through additional scientific studies with different designs, highlight a potential role for meal timing in preventing cardiovascular disease. They suggest that adopting the habit of eating earlier first and last meals with a longer period of night-time fasting could help to prevent the risk of cardiovascular disease.