Older adults with type 2 diabetes face a difficult trade-off: they are among the most vulnerable to medication-related harms yet are often underrepresented in the clinical trials that guide treatment decisions. A new study led by Yuan Lu, ScD, helps address this gap by providing large-scale, real-world evidence about the safety of commonly used diabetes medications.
Published in Nature Communications, the study analysed data from more than 1.8 million people aged 65 and older across the United States and Europe. The researchers compared four major classes of second-line antihyperglycaemic medications – typically prescribed when first-line therapy such as metformin is not sufficient – across 18 safety outcomes.
“Evidence from clinical trials often does not fully capture older adults,” says Lu, assistant professor of medicine (cardiovascular medicine) at Yale School of Medicine. “They are more likely to experience side effects due to frailty, multiple chronic conditions, and the use of several medications at the same time.”
Newer diabetes drugs show overall safety advantages
The study found a consistent pattern: newer classes of medications, including GLP-1 receptor agonists and SGLT2 inhibitors, were generally associated with lower risks of several important adverse outcomes compared to older drugs such as sulfonylureas and DPP-4 inhibitors.
Newer agents were linked to lower risks of hypoglycaemia, hyperkalaemia, and peripheral oedema – complications that can be especially dangerous in older adults. However, the findings also highlight important trade-offs. For example, SGLT2 inhibitors were associated with a higher risk of diabetic ketoacidosis, while GLP-1 receptor agonists were more likely to cause gastrointestinal side effects such as nausea and vomiting.
Rather than identifying a single “best” medication, Lu emphasises that the results support more informed, individualised decision-making. “Some patients may have a higher risk of hypoglycaemia, while others may be more susceptible to diabetic ketoacidosis,” she says. “These risks need to be considered together as part of an individual patient profile.”
Real-world data at a global scale
A key strength of the study is its scale and approach. The analysis drew on nine large databases and was conducted through the Observational Health Data Sciences and Informatics (OHDSI), an international research network that enables standardized analyses across diverse health care systems.
By using harmonised real-world data and consistent analytic methods, the researchers were able to evaluate a broad range of safety outcomes in routine clinical practice – offering insights that complement and extend findings from randomised trials.
Supporting safer prescribing for an aging population
As the population ages and the use of newer diabetes medications continues to grow, understanding their safety profiles in older adults is increasingly important. The findings reinforce current guideline recommendations that often favour newer agents, while also underscoring the need to tailor treatment decisions to each patient’s risks and preferences.
Like all observational studies, the analysis cannot fully rule out unmeasured differences between patients. Still, the large, multinational design gives a more complete picture of medication safety in a population often underrepresented in clinical research.
Looking ahead, Lu and her colleagues hope to expand this work to examine the comparative safety of individual medications and to evaluate the safety of newer GLP-1 receptor agonists across a wider range of outcomes, including among people with obesity. “By providing more evidence in populations that clinicians see every day, our goal is to support safer, more informed care,” she says.
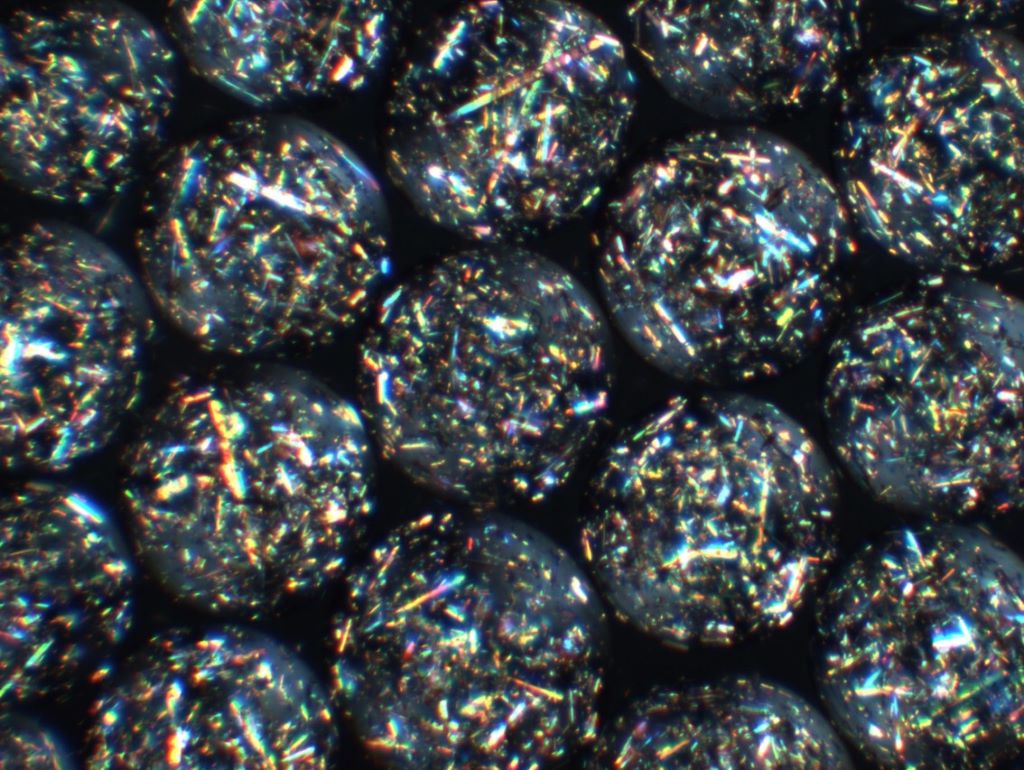
The development of a self-regulating, implantable living technology that could offer hope for millions with diabetes and other chronic diseases
The crystal capsules developed by the researchers. They made the cover of Science Translational Medicine.
A pioneering study marks a major step toward eliminating the need for daily insulin injections for people with diabetes. The research introduces a living, cell-based implant that can function as an autonomous artificial pancreas, essentially a living drug that is long-term, thanks to a novel crystalline shield technology.
Once implanted, the system operates entirely on its own: it continuously senses blood-glucose levels, produces insulin within the implant itself, and releases the exact amount needed – precisely when it is needed. In effect, the implant becomes a self-regulating, drug-manufacturing organ inside the body, requiring no external pumps, injections, or patient intervention.
One of the study’s most significant breakthroughs addresses the longstanding challenge of immune rejection, which has limited the success of cell-based therapies for decades. The researchers developed engineered therapeutic crystals that shield the implant from the immune system, preventing it from being recognised as a foreign object. This protective strategy enables the implant to function reliably and continuously for several years.
The technology has already been successfully tested in a mouse model for effective and long-term regulation of glucose levels and in non-human primates for cell viability and functionality. These results represent a critical milestone and strongly support the potential for future translation to human patients.
From Postdoctoral Insight to Global Collaboration
The study was led by Assistant Professor Shady Farah of the Faculty of Chemical Engineering at the Technion – Israel Institute of Technology, in co-correspondence with MIT, and in collaboration with Harvard University, Johns Hopkins University, and the University of Massachusetts. Asst Prof Farah began developing the concept with colleagues in 2018 during his postdoctoral fellowship at MIT and Boston Children’s Hospital/Harvard Medical School, under the supervision of Prof Daniel Anderson and Prof Robert (Bob) Langer, a world leader in tissue engineering and co-founder of Moderna.
Today, the research continues in Asst Prof Farah’s laboratory at the Technion, in close collaboration with leading US institutions, including MIT, Harvard, the University of Massachusetts, Boston Children’s Hospital, and the Johns Hopkins University School of Medicine.
A Platform with Far-Reaching Potential
While the immediate focus is diabetes, the researchers emphasise that this implantable, closed-loop platform could be adapted to treat a wide range of chronic conditions requiring continuous delivery of biological therapeutics – including haemophilia and other metabolic or genetic diseases.
If successfully translated to the clinic, this technology could redefine how chronic diseases are treated, shifting from repeated drug administration to living, self-regulating therapies that work seamlessly from within.
Spending too long sitting raises the risk of heart disease and diabetes in people over 60, warns a major global review. Published in the Journal of Physical Activity and Health, the review analysed data from 28 international studies involving 82 000 people aged 60 and older.
It flags strong links between sitting time and worsening markers for chronic disease including high blood sugar, cholesterol, waist size, and blood pressure. And that’s even for people who exercise regularly.
That means — whether watching TV, using a tablet or reading a book — the longer older people sit, the higher their risk of major health problems like heart disease, stroke, and type 2 diabetes.
“This is a link we can’t ignore,” said Dr Daniel Bailey, Reader in Sedentary Behaviour and Health at the Department of Life Sciences, Brunel University of London. “You can meet the weekly exercise target, but if you spend the rest of the day sitting, your health is still at risk.”
In the UK, where more than 12 million people are aged 65 or older, older adults can spend up to 80% of their waking hours sitting down and longer during winter or for people with mobility issues. That means millions may be unknowingly accumulating risks day after day — a concern for families, carers, and health professionals.
One of the most revealing findings was that the harmful effect of sitting for long periods showed up even in otherwise healthy older adults, not just those already diagnosed with illness. Waist measurement, a major predictor of health risk, had the strongest, most consistent link with sitting time.
“We’re seeing these impacts in people who don’t yet feel unwell,” said Dr Bailey. “That means we have a chance to intervene early and protect health before problems start.”
Importantly, the study found limited protective effect from exercise alone. After accounting for how active people were, the damage from long hours of sitting remains.
“The evidence is clear. We urgently need strategies that don’t just encourage exercise, but also help people sit less throughout the day,” said Dr Bailey. “Simple changes make a difference —standing during phone calls, replacing some TV time with gardening or a stroll, or light chores around the house.”
The study by Brunel University of London, the University of Lincoln, Federation University in Australia, and the University of Bedfordshire is the most comprehensive analysis to date linking sedentary behaviour to cardiometabolic risk in later life. As the NHS contends with rising rates of diabetes and heart disease, it spells out to policymakers that keeping moving throughout the day is as vital as structured exercise.
Dr Bailey stressed the shared role of public services, community groups and healthcare professionals to help older people avoid sitting for long stretches: “From GP advice to local councils and charities, there’s a role for everyone in changing the message.”
Cases of cardiovascular, leg/foot, kidney complications, and eye disease all higher in men Sex differences in complication rates persist regardless of disease duration
Photo by Photomix Company on Pexels
Men are at greater risk than women of the major health effects of diabetes (types 1 and 2), suggests a long term study published online in the Journal of Epidemiology & Community Health.
Rates of cardiovascular disease, leg, foot, and kidney complications, and the sight-threatening eye disease diabetic retinopathy are all higher in men, regardless of whether they had diabetes for more or less than 10 years, the findings show.
The global prevalence of diabetes is similar in men and women, and is projected to rise to 783 million by 2045, note the researchers.
But while cardiovascular disease is more common in men, overall, it’s not clear if this sex difference is apparent in the incidence of the complications associated with diabetes, say the researchers. Nor is it clear whether the length of time lived with diabetes might be influential, they add.
To explore this further, the researchers drew on survey responses from the 45 and Up Study, Australia, a large prospective study of 267 357 people over the age of 45 living in New South Wales (NSW).
These responses were linked to medical records for a total of 25 713 people, all of whom had either type 1 or type 2 diabetes, to monitor the development of any of the major health issues associated with diabetes
These include cardiovascular disease – ischaemic heart disease, mini stroke or TIA, stroke, heart failure, diabetic cardiomyopathy; eye problems – cataract, diabetic retinopathy; leg/foot problems – peripheral neuropathy (nerve damage), ulcers, cellulitis, osteomyelitis (bone inflammation), peripheral vascular disease (poor circulation), and minor or major amputation; and kidney problems – acute kidney failure, chronic kidney disease, chronic kidney failure, dialysis, and kidney transplant.
Almost half of the group were aged 60 to 74, and over half (57%; 14,697) were men, a higher proportion of whom were overweight (39% vs 29% of women) and had a history of heart disease.
Although a similar proportion of men and women were current smokers, a higher proportion of men were ex-smokers: 51% vs 29% of the women.
Of the 19 277 (75%) people with diabetes whose age was recorded at their diagnosis, 58% had been living with the disease for less than a decade and 42% had lived with it for 10 or more years.
Men had higher rates, and were at greater risk, of the complications associated with diabetes.
Over an average monitoring period of 10 years, and after factoring in age, 44% of the men experienced a cardiovascular disease complication while 57% had eye complications. Similarly, 25% of the men had leg/foot complications, and 35% kidney complications. The equivalent figures for women were, respectively, 31%, 61%, 18% and 25%.
Overall, men were 51% more likely to develop cardiovascular disease than women, 47% more likely to have leg and foot complications, and 55% more likely to have kidney complications.
Although there was little difference in the overall risk of eye complications between the sexes, men were at slightly higher risk (14%) of diabetic retinopathy.
While complication rates rose in tandem with the number of years lived with diabetes for both men and women, the sex difference in complication rates persisted.
By way of an explanation, the researchers point out that the men in the study were more likely to have well known risk factors. Men may also be less likely to make lifestyle changes, take preventive meds, or get health checks to lower their risks, they suggest.
This is an observational study, and as such, no firm conclusions can be drawn about causal factors, added to which people with a history of complications were excluded from the study. And information on potentially influential factors, such as diabetes medications, and glucose, blood fat, and blood pressure control wasn’t available.
But based on their findings, the researchers suggest: “For every 1000 people with diabetes, our findings suggest that an average of 37, 52, 21, and 32 people will develop cardiovascular disease, eye, lower limb, and kidney complications every year.”
While the risks of complications are lower in women with diabetes, they are still high, emphasise the researchers.
And they conclude: “Although men with diabetes are at greater risk of developing complications, in particular [cardiovascular disease], kidney and lower-limb complications, the rates of complications are high in both sexes.
“The similar sex difference for those with shorter compared with longer diabetes duration highlights the need for targeted complication screening and prevention strategies from the time of diabetes diagnosis.
“Further investigation into the underlying mechanisms for the observed sex differences in diabetes complications are needed to inform targeted interventions.”
A clinical trial from Wake Forest University School of Medicine shows that two widely available medications, the diabetes drug empagliflozin (Jardiance) and intranasal insulin, safely improve brain health in people with mild cognitive impairment and early Alzheimer’s disease. The study, published in Alzheimer’s & Dementia, marks the first time empagliflozin has been tested in non-diabetic patients with Alzheimer’s disease. The results show promising effects on memory, brain health and brain blood flow.
The research addresses a critical treatment gap for patients with Alzheimer’s disease. While recently approved anti-amyloid drugs represent progress, their benefits are modest, and they’re unavailable to many patients due to side effects and medical contraindications. They also don’t address the upstream metabolic and vascular problems that drive disease progression or help restore brain function after damage occurs.
“Our study suggests that targeting metabolism can change the course of Alzheimer’s disease,” said Suzanne Craft, PhD, lead investigator and professor of medicine and director of the Wake Forest Alzheimer’s Disease Research Center. “For the first time, we found that empagliflozin, an established diabetes and heart medication, reduced markers of brain injury while restoring blood flow in critical brain regions. We also confirmed that delivering insulin directly to the brain with a newly validated device enhances cognition, neurovascular health and immune function. Together, these findings highlight metabolism as a powerful new frontier in Alzheimer’s treatment.”
The four-week trial enrolled 47 older adults (average age 70) with mild cognitive impairment or early Alzheimer’s disease. Participants were randomly assigned to receive intranasal insulin alone, empagliflozin alone, both medications together or a placebo.
Both medications were safe and well-tolerated. Treatment-related side effects were mild and similar across all groups. Participants found the nasal insulin device highly feasible to use (4.6 out of 5.0), and compliance rates exceeded 97% for both medications throughout the study.
The results revealed different benefits for each medication. Intranasal insulin improved performance on sensitive cognitive tests that detect early memory and thinking changes. Brain imaging showed insulin treatment increased the structural integrity of white matter connections and changed blood flow patterns in memory-critical regions. The treatment also reduced plasma GFAP, a marker of astrocyte (support cells that maintain healthy connections between blood vessels and brain cells) dysfunction that’s elevated in Alzheimer’s disease.
Empagliflozin had different effects. The medication significantly lowered cerebrospinal fluid tau, a protein that forms toxic tangles in the brain in patients with Alzheimer’s disease. It also reduced neurogranin and vascular markers linked to disease progression and changed blood flow in key brain regions. Empagliflozin also increased HDL cholesterol, showing its beneficial metabolic effects work even in non-diabetic patients.
Both medications influenced multiple immune and inflammatory proteins in cerebrospinal fluid and blood. The changes suggest the drugs help activate protective immune responses while reducing harmful inflammation. Intranasal insulin particularly affected proteins involved in the nasal-olfactory plexus, a newly discovered pathway that connects the brain’s waste-clearance system to immune systems throughout the body.
The medications work differently but target overlapping problems. Empagliflozin, originally developed for diabetes, improves how the body processes glucose and sodium. That leads to better insulin sensitivity and vascular health throughout the body and brain. The drug also reduces oxidative stress and inflammation while improving how mitochondria produce energy in cells.
Intranasal insulin uses a precision delivery device to send insulin directly into the brain through the nose, bypassing the bloodstream. Once there, insulin activates receptors throughout the brain that keep synapses healthy, support blood vessel function, maintain white matter integrity, and regulate immune responses. Previous studies showed that lower doses of intranasal insulin preserved brain glucose metabolism and slowed white matter damage over 12 months.
The trial used higher insulin doses than previous studies (160 IU daily versus 40-80 IU) delivered through a cartridge pump system developed by Aptar Pharma and validated in earlier brain imaging studies. This device provides precise, reliable delivery to brain regions involved in memory and cognition. Empagliflozin was given at the standard 10 mg daily dose used for cardiovascular conditions in non-diabetic adults.
People with Alzheimer’s disease often have insulin resistance in the brain alongside vascular problems that reduce blood flow and nutrient delivery. These metabolic and vascular disruptions speed up the accumulation of amyloid plaques and tau tangles while preventing the brain from clearing these toxic proteins. Both medications tested in this trial target these upstream problems.
“We plan to build on these promising results with larger, longer studies in people with early and preclinical Alzheimer’s disease,” Craft said. “Because empagliflozin or intranasal insulin improved tau tangles, cognition, neurovascular health and immune function, we believe these treatments could offer real therapeutic potential, either on their own or in combination with other Alzheimer’s therapies.”
The complementary effects of the two medications could make them valuable additions to combination therapy approaches. Since both drugs are already FDA-approved for other conditions with well-established safety profiles, they could reach patients faster than entirely new medications would.
This new technology offers people with diabetes two-hour and overnight predictive notifications
The Accu-Chek SmartGuide® continuous glucose monitoring (CGM) solution provides 14 days accuratereal-time glucose values for adults living with diabetes1
Artificial intelligence (AI)-enabled algorithms can predict glucose levels up to two hours ahead and overnight, empowering users to take action before a glucose excursion occurs2 proactively
Over 4.2 million people living with diabetes were recorded in 2024, in South Africa people living with diabetes could benefit from the Accu-Chek SmartGuide® CGM solution 3
Johannesburg, 4 November 2025 – Roche (SIX: RO, ROG; OTCQX: RHHBY) announced today that its Accu-Chek® SmartGuide continuous glucose monitoring (CGM) solution is now available in South Africa. This significant milestone means that people living with diabetes over the age of 18 can now benefit from the solution’s enhanced glucose monitoring and artificial intelligence (AI)-enabled predictive insights1,2.
Diabetes is one of today’s most urgent healthcare challenges. In South Africa, 4.2 million people are living with the condition as of 2024 3. If left unmanaged, diabetes can lead to secondary complications including cardiovascular disease, kidney disease, nerve damage, blindness, lower limb amputation and mental health issues4. In a study conducted by GWI in partnership with Roche, 58% of people living with diabetes stated that they feel a mental burden associated with managing their diabetes.
Since it was introduced, CGM technology has significantly improved diabetes care5, yet a significant number of people still have difficulty keeping their glucose in the right range when using current systems.6 Hypoglycaemia is common amongst persons who have type 1 diabetes, with an annual incidence of severe hypoglycemia ranging from 3.3% to 13.5%.7
“The Accu-Chek SmartGuide CGM solution is a significant step towards providing greater peace of mind for people living with diabetes, due to the AI-enabled predictive capabilities it offers. This empowers patients to take action before undesired events occur,” said Merilynn Steenkamp, General Manager, Southern Africa, Roche Diagnostics.“Our new Accu-Chek SmartGuide® CGM solution puts the power of prediction into the hands of people living with diabetes with its integrated AI-enabled algorithms that predict glucose levels for the next 2 hours as well as imminent and nocturnal hypoglycaemia. People with diabetes should have the freedom to plan the day ahead and get a good night’s sleep at the end of it all.”
Nighttime hypoglycaemia can present a particular challenge for people with diabetes. Approximately 2-5% of deaths in people with type 1 diabetes under the age of 40 are due to episodes of very low glucose during the night8,9. The unpleasant symptoms and negative consequences of hypoglycaemia can result in actual fear of hypoglycaemia with possible significant implications for the diabetes management, metabolic control and subsequent health outcomes.10
The Accu-Chek SmartGuide® CGM solution uses AI-enabled algorithms to predict where an individual’s glucose levels are likely headed in the next 30 minutes, 2 hours, and even overnight. This means people with diabetes can move from a reactive to a proactive approach to their daily management, preparing for and managing potential episodes in advance, rather than waiting for alerts when they happen.
The Accu-Chek SmartGuide® CGM solution includes a wireless, water-resistant sensor, worn on the back of the upper arm, and the apps where the users can see their current glucose levels and their future glucose development through predictive analytics. Every five minutes, the sensor sends glucose values measured in real-time to the Accu-Chek SmartGuide app. The Accu-Chek SmartGuide® predict app then uses those glucose values and other optional information entered by the user such as food intake and insulin doses to detect patterns and predict future glucose levels. Supported by AI-trained algorithms, it provides key predictions of likely hypoglycaemia within 30 minutes as well as general estimated predictions of glucose levels within 2 hours and during a defined 7-hours nighttime period.11
Clinical studies have demonstrated the new Roche CGM solution’s high system accuracy, with an overall mean absolute relative difference (MARD) of 9.2% and 99.8% of measured glucose values falling within zones A and B on the Parkes Error Grid.1, 12 The evaluation of the predictive capabilities showed that all advanced predictive features exceeded high performance requirements as e.g. accuracy, sensitivity and specificity.13
Roche is committed to bringing improved and proactive relief to diabetes management across South Africa with the immediate availability of the Accu-Chek SmartGuide® CGM solution.
About the Accu-Chek SmartGuide® CGM solution
Accu-Chek SmartGuide® is a continuous glucose monitoring (CGM) solution developed by Roche providing accurate1 real-time glucose readings and AI-enabled predictions for different timeframes7. The solution includes three elements: the Accu-Chek SmartGuide® CGM sensor, the Accu-Chek SmartGuide® App and the Accu-Chek SmartGuide® Predict App. With an all-in-one applicator and 14-day wear time, Accu-Chek SmartGuide® is designed for people living with diabetes, 18 years of age and older. It aims at empowering people living with diabetes to be prepared for the future development of glucose levels and take preventive action by making the appropriate therapy adjustments in good time.
The Accu-Chek SmartGuide® CGM solution can be seamlessly integrated with the Accu-Chek® Care platform, offering healthcare professionals (HCPs) access to comprehensive and accurate1 therapy-relevant data provided by the CGM solution. This integration allows HCPs to analyse together with their patients how lifestyle and therapy impact their glucose levels and make more informed decisions.
About Roche
Founded in 1896 in Basel, Switzerland, as one of the first industrial manufacturers of branded medicines, Roche has grown into the world’s largest biotechnology company and the global leader in in-vitro diagnostics. The company pursues scientific excellence to discover and develop medicines and diagnostics for improving and saving the lives of people around the world. We are a pioneer in personalised healthcare and want to further transform how healthcare is delivered to have an even greater impact. To provide the best care for each person we partner with many stakeholders and combine our strengths in Diagnostics and Pharma with data insights from the clinical practice.
For over 125 years, sustainability has been an integral part of Roche’s business. As a science-driven company, our greatest contribution to society is developing innovative medicines and diagnostics that help people live healthier lives. Roche is committed to the Science Based Targets initiative and the Sustainable Markets Initiative to achieve net zero by 2045.
Genentech, in the United States, is a wholly owned member of the Roche Group. Roche is the majority shareholder in Chugai Pharmaceutical, Japan.
All trademarks used or mentioned in this release are protected by law.
References [1] Mader, J. K., Waldenmaier, D., Mueller-Hoffmann, W., Mueller, K., Angstmann, M., Vogt, G., Rieger, C. C., Eichenlaub, M., Forst, T., & Freckmann, G. (2024). Performance of a Novel Continuous Glucose Monitoring Device in People With Diabetes. Journal of diabetes science and technology, 18(5), 1044–1051. https://doi.org/10.1177/19322968241267774
[2] Simulation study, Data on file, Roche Diabetes Care GmbH, 2025.
[3] Ngassa Piotie P, Rheeder P. UP Expert Opinion: South Africa has more than 4 million people living with diabetes – many aren’t getting proper treatment. University of Pretoria Diabetes Research Centre News. 2024 Mar 11 [cited 2025 Oct 8]. Available from: https://www.up.ac.za/diabetes-research-centre/news/post_3214595-up-expert-opinion-south africa-has-more-than-4-million-people-living-with-diabetes-many-arent-getting-proper-treatment
[4] Tomic D, Shaw JE, Magliano DJ. The burden and risks of emerging complications of diabetes mellitus. Nat Rev Endocrinol. 2022 Sep;18(9):525-539. doi: 10.1038/s41574-022-00690-7. Epub 2022 Jun 6. PMID: 35668219; PMCID: PMC9169030.
[6] DeSalvo DJ, et al., Journal of Diabetes Science and Technology. 2023;17(2):322-328.
[7] Nakhleh A, Shehadeh N. Hypoglycemia in diabetes: An update on pathophysiology, treatment, and prevention. World J Diabetes. 2021 Dec 15;12(12):2036-2049. doi: 10.4239/wjd.v12.i12.2036. PMID: 35047118; PMCID: PMC8696639.
[8] Secrest AM et al. Characterizing sudden death and dead in bed syndrome in Type 1 diabetes: analysis from two childhood onset Type 1 diabetes registries. Diabet. Med. 2011. 28, 293–300.
[9] Jones J et al. Dead in bed – A systematic review of overnight deaths in type 1 diabetes. Diabetes Res Clin Pract. 2022. 191:110042.
[10] Wild, Diane et al. “A critical review of the literature on fear of hypoglycemia in diabetes: Implications for diabetes management and patient education.” Patient education and counseling vol. 68,1 (2007): 10-5. doi:10.1016/j.pec.2007.05.003
[12] Parkes Error Grid – a tool to evaluate the accuracy of glucose monitoring systems (BGM and CGM).
[13] Herrero, P., Andorrà, M., Babion, N., Bos, H., Koehler, M., Klopfenstein, Y., Leppäaho, E., Lustenberger, P., Peak, A., Ringemann, C., & Glatzer, T. (2024). Enhancing the Capabilities of Continuous Glucose Monitoring With a Predictive App. Journal of diabetes science and technology, 18(5), 1014–1026. https://doi.org/10.1177/19322968241267818.
New research in Diabetes, Obesity and Metabolism reveals that metformin, a medication traditionally prescribed to treat diabetes, is linked to lower risks of dementia and early death.
In the study by investigators at Taipei Medical University that included 452,777 adults with varying degrees of overweight and obesity, 35,784 cases of dementia and 76,048 deaths occurred over 10 years. Metformin users exhibited significantly lower risks of both dementia and all-cause death than nonusers.
The benefits of metformin were seen across all categories of overweight, obesity, and severe obesity, with 8–12% lower risks of dementia and 26–28% lower risks of death.
“Although our study results are promising for metformin’s effects on dementia and mortality, further research is required to explore the mechanisms involved,” said co-corresponding author Chiehfeng Chen, MD, PhD, MPH.
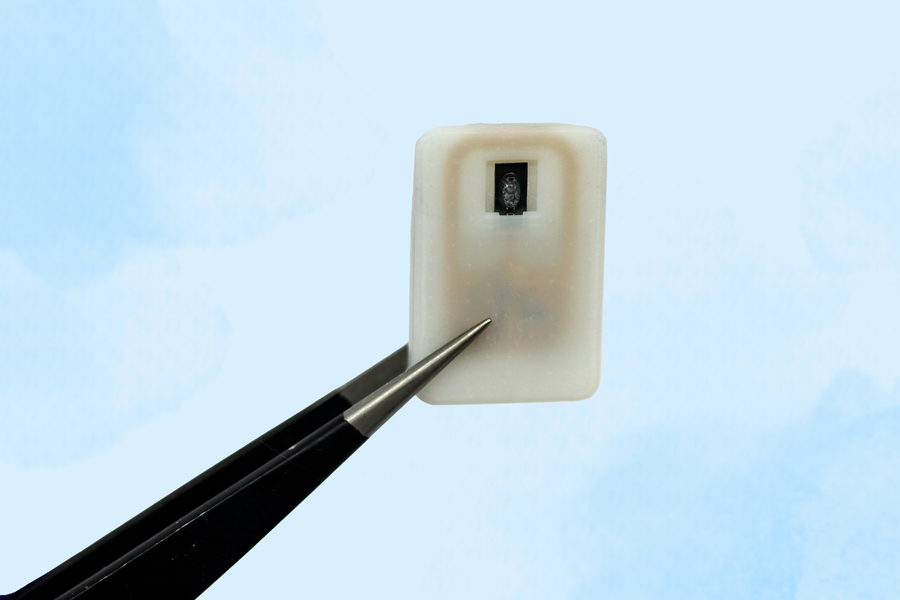
The new implant carries a reservoir of glucagon that can be stored under the skin and deployed during an emergency — with no injections needed.
Caption:A new implantable device carries a reservoir of glucagon that can be stored under the skin and could save diabetes patients from dangerously low blood sugar.
Image: Courtesy of the researchers
For people with Type 1 diabetes, developing hypoglycaemia, or low blood sugar, is an ever-present threat. When glucose levels become extremely low, it creates a life-threatening situation for which the standard treatment of care is injecting a hormone called glucagon.
As an emergency backup, for cases where patients may not realise that their blood sugar is dropping to dangerous levels, MIT engineers have designed an implantable reservoir that can remain under the skin and be triggered to release glucagon when blood sugar levels get too low.
This approach could also help in cases where hypoglycaemia occurs during sleep, or for diabetic children who are unable to administer injections on their own.
“This is a small, emergency-event device that can be placed under the skin, where it is ready to act if the patient’s blood sugar drops too low,” says Daniel Anderson, a professor in MIT’s Department of Chemical Engineering, a member of MIT’s Koch Institute for Integrative Cancer Research and Institute for Medical Engineering and Science (IMES), and the senior author of the study. “Our goal was to build a device that is always ready to protect patients from low blood sugar. We think this can also help relieve the fear of hypoglycaemia that many patients, and their parents, suffer from.”
The researchers showed that this device could also be used to deliver emergency doses of epinephrine, a drug that is used to treat heart attacks and can also prevent severe allergic reactions, including anaphylactic shock.
Siddharth Krishnan, a former MIT research scientist who is now an assistant professor of electrical engineering at Stanford University, is the lead author of the study, which appears today in Nature Biomedical Engineering.
Emergency response
Most patients with type 1 diabetes use daily insulin injections to help their body absorb sugar and prevent their blood sugar levels from getting too high. However, if their blood sugar levels get too low, they develop hypoglycaemia, which can lead to confusion and seizures, and may be fatal if it goes untreated.
To combat hypoglycaemia, some patients carry preloaded syringes of glucagon, a hormone that stimulates the liver to release glucose into the bloodstream. However, it isn’t always easy for people, especially children, to know when they are becoming hypoglycaemic.
“Some patients can sense when they’re getting low blood sugar, and go eat something or give themselves glucagon,” Anderson says. “But some are unaware that they’re hypoglycaemic, and they can just slip into confusion and coma. This is also a problem when patients sleep, as they are reliant on glucose sensor alarms to wake them when sugar drops dangerously low.”
To make it easier to counteract hypoglycaemia, the MIT team set out to design an emergency device that could be triggered either by the person using it, or automatically by a sensor.
The device, which is about the size of a quarter, contains a small drug reservoir made of a 3D-printed polymer. The reservoir is sealed with a special material known as a shape-memory alloy, which can be programmed to change its shape when heated. In this case, the researcher used a nickel-titanium alloy that is programmed to curl from a flat slab into a U-shape when heated to 40 degrees Celsius.
Like many other protein or peptide drugs, glucagon tends to break down quickly, so the liquid form can’t be stored long-term in the body. Instead, the MIT team created a powdered version of the drug, which remains stable for much longer and stays in the reservoir until released.
Each device can carry either one or four doses of glucagon, and it also includes an antenna tuned to respond to a specific frequency in the radiofrequency range. That allows it to be remotely triggered to turn on a small electrical current, which is used to heat the shape-memory alloy. When the temperature reaches the 40-degree threshold, the slab bends into a U shape, releasing the contents of the reservoir.
Because the device can receive wireless signals, it could also be designed so that drug release is triggered by a glucose monitor when the wearer’s blood sugar drops below a certain level.
“One of the key features of this type of digital drug delivery system is that you can have it talk to sensors,” Krishnan says. “In this case, the continuous glucose-monitoring technology that a lot of patients use is something that would be easy for these types of devices to interface with.”
Reversing hypoglycaemia
After implanting the device in diabetic mice, the researchers used it to trigger glucagon release as the animals’ blood sugar levels were dropping. Within less than 10 minutes of activating the drug release, blood sugar levels began to level off, allowing them to remain within the normal range and avert hypoglycaemia.
The researchers also tested the device with a powdered version of epinephrine. They found that within 10 minutes of drug release, epinephrine levels in the bloodstream became elevated and heart rate increased.
In this study, the researchers kept the devices implanted for up to four weeks, but they now plan to see if they can extend that time up to at least a year.
“The idea is you would have enough doses that can provide this therapeutic rescue event over a significant period of time. We don’t know exactly what that is — maybe a year, maybe a few years, and we’re currently working on establishing what the optimal lifetime is. But then after that, it would need to be replaced,” Krishnan says.
Typically, when a medical device is implanted in the body, scar tissue develops around the device, which can interfere with its function. However, in this study, the researchers showed that even after fibrotic tissue formed around the implant, they were able to successfully trigger the drug release.
The researchers are now planning for additional animal studies and hope to begin testing the device in clinical trials within the next three years.
“It’s really exciting to see our team accomplish this, which I hope will someday help diabetic patients and could more broadly provide a new paradigm for delivering any emergency medicine,” says Robert Langer, the David H. Koch Institute Professor at MIT and an author of the paper.
Other authors of the paper include Laura O’Keeffe, Arnab Rudra, Derin Gumustop, Nima Khatib, Claudia Liu, Jiawei Yang, Athena Wang, Matthew Bochenek, Yen-Chun Lu, Suman Bose, and Kaelan Reed.
The research was funded by the Leona M. and Harry B. Helmsley Charitable Trust, the National Institutes of Health, a JDRF postdoctoral fellowship, and the National Institute of Biomedical Imaging and Bioengineering.
The age of menarche can offer valuable clues about a woman’s long-term risk for conditions like obesity, diabetes, heart disease and reproductive health issues, according to a study being presented Sunday at ENDO 2025, the Endocrine Society’s annual meeting in San Francisco.
The Brazilian study found that both early and late menarche – the age when women first get their period– are linked to different health risks. Women who had their first period before age 10 were more likely to develop obesity, hypertension, diabetes, heart problems and reproductive issues like pre-eclampsia later in life. Women who started their period after age 15 were less likely to be obese but had a higher risk of menstrual irregularities and certain heart conditions.
“We now have evidence from a large Brazilian population that confirms how both early and late puberty can have different long-term health impacts,” said study author Flávia Rezende Tinano of the University of Sao Paulo in Sao Paulo, Brazil. “While early menarche increases the risk for multiple metabolic and heart problems, late menarche may protect against obesity but increase certain heart and menstrual issues. Most women can remember when they had their first period, but they might not realise that it could signal future health risks. Understanding these links can help women and their doctors be more proactive about preventing conditions like diabetes, high blood pressure and heart disease.”
Tinano said the study is one of the largest of its kind in a developing country, providing valuable data on a topic that has mostly been studied in wealthier countries. “It highlights how early and late puberty can affect a woman’s long-term health, especially in underrepresented populations like those in Latin America,” she said.
The study was part of the Brazilian Longitudinal Study of Adult Health (ELSA-Brazil) and evaluated data from 7623 women ages 35 to 74. The age of their first period was categorised as early (less than 10 years old), typical (ages 10 to 15) or late (older than 15). They assessed the women’s health through interviews, physical measurements, lab tests and ultrasound imaging.
“Our findings suggest that knowing a woman’s age at her first period can help doctors identify those at higher risk for certain diseases,” Tinano said. “This information could guide more personalised screening and prevention efforts. It also emphasises the importance of early health education for young girls and women, especially in developing countries.”
Despite clinicians recommending that many patients with diabetes take statins, nearly one in five opt to delay treatment. In a new study, researchers from Mass General Brigham found that patients who started statin therapy right away reduced the rate of heart attack and stroke by one third compared to those who chose to delay taking the medication. The results, which can help guide decision-making conversations between clinicians and their patients, are published in the Journal of the American Heart Association.
“I see patients with diabetes on a regular basis, and I recommend statin therapy to everyone who is eligible,” said senior author Alexander Turchin, MD, MS, of the Division of Endocrinology at Brigham and Women’s Hospital, a founding member of the Mass General Brigham healthcare system. “Some people refuse because they want to first try lifestyle interventions or other drugs. But other interventions are not as effective at lowering cholesterol as starting statin therapy as soon as possible. Time is of the essence for your heart and brain health.”
Heart attacks and strokes remain the leading cause of complications and mortality for patients with diabetes. Statin therapy reduces risk of these cardiovascular events by preventing plaque buildup in the blood vessels.
The researchers used an artificial intelligence method called Natural Language Processing to gather data from the electronic health records of 7239 patients at Mass General Brigham who ultimately started statin therapy during the nearly 20-year study period. The median patient age was 55, with 51% being women, 57% white, and a median HbA1c of 6.9.
Nearly one-fifth (17.7%) of the patients in the study declined statin therapy when it was first recommended by their clinicians, then later accepted the therapy (after a median of 1.5 years) upon repeated recommendation by their clinician. Of those who delayed, 8.5% had a heart attack or stroke. But for patients who started statins immediately, the rate of those cardiovascular events was just 6.4%.
“Clinicians should recognize the increased cardiovascular risk associated with delaying statin therapy for patients with diabetes and use this information to guide shared decision-making conversations with their patients,” said Turchin.