
Vaccine and Immunotherapy Combo Halves Melanoma Recurrence

The combination of a vaccine and a drug, which both harness the immune system to attack cancer cells, has proven successful in cutting the risk of skin cancer recurrence by 49% , a new study shows. This reduction, which was calculated five years after patients had their tumours surgically removed, remains unchanged.
Led by researchers at NYU Langone Health and its Perlmutter Cancer Center, the study tested the vaccine, called intismeran, in combination with the mainstay immunotherapy pembrolizumab (Keytruda) in 107 patients who had been randomly chosen after melanoma surgery to determine whether the combination therapy prevented their cancer from recurring. Intismeran is a personalized immunotherapy strategy that is developed with information from a patient’s individual tumour. These results were compared with those from a randomly selected group of 50 melanoma patients who had only received pembrolizumab postoperatively, a current standard of care.
Results of the phase 2b trial, known formally as KEYNOTE-942, are being presented at the 2026 annual meeting of the American Society of Clinical Oncology on June 1 in Chicago and simultaneously published in the society’s Journal of Clinical Oncology.
After five years of follow-up, 68.8% of patients who took the combination therapy remained cancer-free, while 49.1% of the patients in the pembrolizumab-alone group had no signs of cancer. This means that adding intismeran to pembrolizumab reduced the risk for recurrence or death by 49%. The combination therapy also reduced the risk of distant metastasis by 59%. Overall survival, meaning no death from cancer or any other cause, was 92.2%for the vaccine with immunotherapy group, while for the immunotherapy-alone group it was 71.3%.
“Our study offers strong evidence to melanoma patients that intismeran vaccine therapy, when used in combination with immunotherapy, can demonstrably reduce their risk of having their cancer return and improve clinical outcomes,” said study senior investigator Janice Mehnert, MD, a professor in the Department of Medicine at NYU Grossman School of Medicine.
“Our findings also serve as encouragement to cancer researchers globally that mRNA vaccines like intismeran could work well in combination with immunotherapy for other cancers whose high rates of mutations have proven difficult to target,” said Dr Mehnert, who also serves as director of the melanoma medical oncology program and associate director of clinical research at Perlmutter Cancer Center.
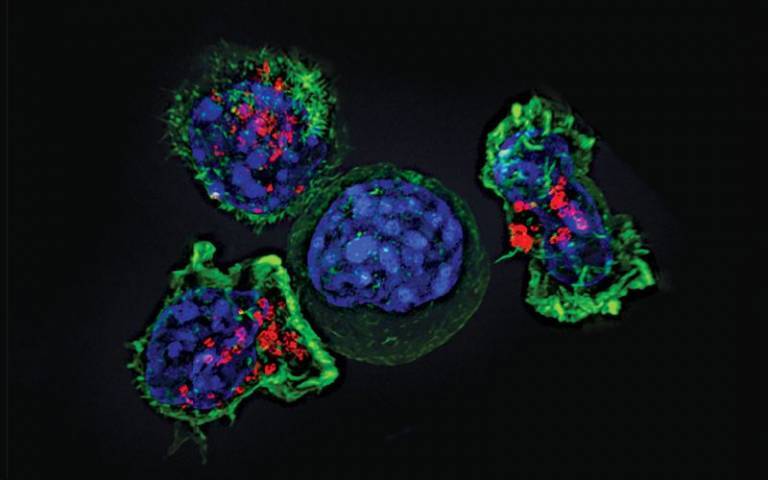
The study results highlight the role of T cells, which are capable of attacking viruses as well as cancers. To spare normal cells, the immune system uses checkpoint molecules on T cell surfaces to “turn off” their attack against viruses when they clear the infection. The body may recognide tumours as abnormal, but cancer cells hijack checkpoints to turn off and evade immune responses. Immunotherapies like pembrolizumab seek to block checkpoints, specifically the PD-1 protein receptor, making cancer cells more “visible” and vulnerable again to immune cells.
Immunotherapies, including PD-1 inhibitors like pembrolizumab, have become the mainstay for treating melanoma, although they do not work for all patients, because melanoma cells, known for their ability to evade the immune system, can become resistant to immunotherapy. For this reason, researchers have looked at adding vaccines.
The vaccine intismeran is based on messenger RNA, a chemical cousin of DNA that provides cells with instructions for making proteins. Intismeran and other mRNA cancer vaccines are meant to teach the immune system to recognize cancer cells as different from normal cells. In designing a vaccine against melanoma, researchers attempted to trigger an immune response to specific abnormal proteins, called neoantigens, made by cancer cells.
Because the study volunteers all had their tumours removed, researchers were able to analyse their cells for 34 neoantigens that were specific to each melanoma and create a personalised vaccine for each patient. As a result, T cells specific to the neoantigen proteins encoded by the mRNA were produced. Those T cells could then attack any melanoma cells trying to grow or spread.
Dr. Mehnert said that a phase 3, multicenter trial is already underway to determine if intismeran helps as a first-line therapy in combination with pembrolizumab for melanoma. Already, the vaccine is being tested to see if it also works to prevent recurrence of lung and other cancers.
For the KEYNOTE-942 trial, patients were enrolled at cancer centers in Australia and the United States from 2019 to 2021. All were men and women who had had surgery to remove their melanoma tumors. Seven patients in each treatment group died during follow-up, most from cancer. Side effects were considered manageable and included fatigue, pain at injection sites, and chills.
Source: NYU Langone Health






{kind=link}