Schizophrenia and bipolar disorder are serious mental illnesses that affect both males and females, but research in Acta Psychiatrica Scandinavica indicates that sex may influence the characteristics and course of these conditions.
The research included 1516 individuals from the multicentre PsyCourse Study: 543 with bipolar disorder, 517 with schizophrenia, and 456 healthy controls.
Several differences between groups and sexes were identified in age at diagnosis, age at treatment, illness duration, illicit drug use, and smoking. For example, females in the schizophrenia group were older than males at first outpatient treatment compared with females in the bipolar disorder group. Moreover, those who were older at first outpatient treatment presented a longer duration of illness. Regarding substance use, the highest rates were observed in males with schizophrenia. People with bipolar disorder showed better functioning and neurocognitive performance than those with schizophrenia. Among individuals with bipolar disorder, females reported better performance in verbal memory and psychomotor speed than males. Both females and males with serious mental illnesses showed higher rates of thyroid alterations than healthy controls.
“Our findings reveal a clear message: sex-sensitive treatment is essential for improving clinical outcomes, promoting healthy habits, and managing comorbidities,” said corresponding author Anabel Martinez-Arán, PhD, of the Hospital Clinic of Barcelona.
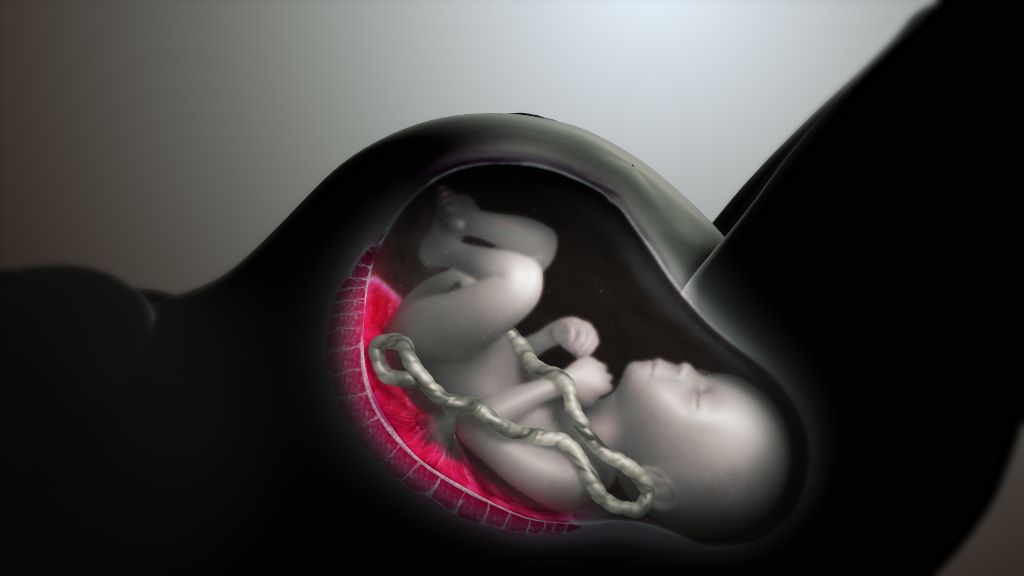
The placenta has long been thought to produce serotonin during pregnancy. But in a new study, Yale researchers shatter the deep-rooted hypothesis – and show that the placenta doesn’t produce serotonin but instead regulates its delivery to the embryo and foetus. They found that serotonin comes from the pregnant parent, with the placenta acting as a “serotonin shield” that controls how much reaches the embryo and foetus.
The findings, published in the journal Endocrinology, could offer critical insights into how a parent’s serotonin levels might affect the development of their baby’s body and brain, the researchers say.
“The placenta is in essence the ‘serotonin shield’ that regulates how much serotonin is ultimately delivered to the embryo and foetus, not the source of serotonin,” said Harvey Kliman, a research scientist in the Department of Obstetrics, Gynecology, and Reproductive Sciences at Yale School of Medicine and corresponding author of the study. “Why does this matter? Because now we correctly know where this delivery is regulated.”
Often called a “happiness hormone,” serotonin regulates mood, so it’s often associated with the brain. In reality, less than 5% of serotonin is made in the brain, with 95% of it made in the gut. But serotonin does more than just regulate mood. It’s also a growth hormone. In the gut, it gets taken up by platelets and is delivered to parts of the body that need to grow, including in wound healing.
During pregnancy, serotonin also helps with growth: It travels into the placenta through a special protein known as the serotonin transporter (SERT) where it plays a critical role in the development of the embryo and foetus.
Serotonin from the mother is taken up by the foetal placenta, which then produces a myriad of hormones, growth factors, and regulators that are delivered to the foetus.
For the new study, researchers sought to better understand these relationships by using a pure source of placenta cells, unlike in previous studies that looked at either whole animals or isolated mouse placentas. To do so, they first purified human cytotrophoblasts, which are the stem cells that make all the cells of the placenta. They then added serotonin to those cells to see where it would go and discovered it concentrated in the nucleus. Next, they used a selective serotonin reuptake inhibitor (SSRI) that blocked SERT, escitalopram, to show that the normal growth, function, and differentiation of these cells was completely blocked.
They also used another inhibitor called cystamine to block serotonylation, or the process by which serotonin is added to proteins like histone 3, which turns genes “on” and “off.” Again, that completely blocked the normal growth of the cells.
Blocking either SERT or serotonylation led to significant changes in gene expression of RNAs in the cytotrophoblasts, they found. Some genes, including ones involved in making, moving, and growing cells, became downregulated, or less active, when serotonin couldn’t enter the cell. Other gene, including ones that help cells stay alive and protect them, became upregulated, or more active. According to the researchers, these findings show that serotonin is critical for the growth of the cytotrophoblasts, the placenta, and by extension, the foetus.
Additionally, researchers discovered that the cytotrophoblasts don’t contain tryptophan hydroxylase (TPH-1), or the enzyme that makes serotonin, indicating the cells within the placenta can’t produce serotonin on their own.
“This suggests that factors that either inhibit serotonin transport through the placenta, or increase it, may have a significant impact on the placenta, embryo, foetus, and ultimately, the newborn and its brain,” Kliman said.
For example, Kliman says this explains why taking SSRIs, which decrease the levels of serotonin into the placenta, leads to smaller babies, and why, conversely, increased levels of serotonin may lead to bigger babies, with bigger brains, who may be at increased risk for developmental disabilities like autism.
Kliman and his lab have long investigated the link between placentas and children with autism, specifically the number of trophoblast inclusions (TIs) in the placenta. TIs are like wrinkles or folds in the placenta, caused by cells multiplying more than they should, typically only seen in pregnancies where there are genetic problems with the foetus.
This new study is the culmination of research first published in 2006 that found significantly more TIs in the placentas from children with autism, and later in 2021, that the genetics of the foetus, and not the parent’s uterine environment, determine how many TIs are in the placenta.
“This puts a big nail into the theory that vaccines cause autism,” suggested Kliman. “Autism, in essence, starts in the womb, not after delivery, and is most likely due to the genetics of the placenta and to a lesser extent, the maternal environment the placenta finds itself in.”
People who take medication for ADHD have a lower risk of suicide attempts, substance abuse, traffic accidents, and criminality than people with ADHD who do not take medication. This is shown in a new study by researchers from Karolinska Institutet and University of Southampton, published in the journal BMJ.
ADHD, which affects about 5% of children and 2.5% of adults globally, is associated with an increased risk of suicide attempts, substance abuse, accidents, and crime, among other things.
The researchers behind the study wanted to investigate whether ADHD medication reduces the risk of these outcomes by analysing Swedish national registry data between 2007 and 2020.
A total of nearly 150 000 individuals between the ages of 6 and 64 with newly diagnosed ADHD were included. The average age in the group was 17, and 41% were women. Of these, 57% started medication, with methylphenidate being the most common drug.
The researchers compared people who had started medication within three months of diagnosis with those who had not, and assessed the outcomes over two years after diagnosis.
Reduction in the risk of serious outcomes
The results showed that ADHD medication was associated with a significant reduction in the risk of several serious outcomes: suicide attempts decreased by 17%, substance abuse by 15%, traffic accidents by 12%, and criminality by 13%. The effects were even more pronounced in certain subgroups – for example, a 25% reduction in substance abuse and criminality was noted in individuals who had had recurring problems with these issues.
One possible explanation is that the medication leads to reduced impulsivity, which can reduce the risk of crime by curbing aggressive behaviour, as well as improved attention, which can reduce the risk of traffic accidents by reducing distractions,” says the study’s last author, Zheng Chang, a researcher at the Department of Medical Epidemiology and Biostatistics, Karolinska Institutet. He continues:
“These results provide evidence that ADHD medication can affect important health and societal outcomes, which should be taken into account both in clinical practice and in the public debate on drug treatment.”
The study is a collaboration between Karolinska Institutet and the University of Southampton. The study was funded by the Swedish Research Council and the Swedish Research Council for Health, Working Life and Welfare, Forte, among others. Some researchers have received fees from pharmaceutical companies, but for work outside the current study.
New research from the Institute of Psychiatry, Psychology & Neuroscience (IoPPN) at King’s College London, in partnership with the University of Bath, has found that the reasons why a person chooses to use cannabis can increase their risk of developing paranoia.
Photo by Thought Catalog on Unsplash
The use and potency of cannabis is increasing worldwide, and dependence and cannabis-induced psychosis are also greatly increasing as a result, especially in North America. Two new research papers, both using data from Cannabis & Me – the largest survey of its kind – have identified key risk factors associated with the more severe forms of paranoia in cannabis users.
The first study, published in BMJ Mental Health, explored the relationship between why people first started using cannabis, and how this affected their subsequent use.
3389 former and current cannabis users aged 18 and over responded to a survey examining their reasons for first and continued use, their weekly consumption of cannabis in THC units, and their mental health.
Researchers established several key findings. Respondents who first started using cannabis to self-medicate an illness, including physical pain, anxiety, depression, or because they were experiencing minor psychotic symptoms, all demonstrated higher paranoia scores.
This was in contrast to those respondents who tried cannabis for fun or curiosity, or with their friends, who reported the lowest average paranoia and anxiety scores.
Dr Edoardo Spinazzola, a Research Assistant at King’s IoPPN and the study’s first author said, “This research suggests that using cannabis as a mean to self-medicate physical or mental discomfort can have a negative impact on the levels of paranoia, anxiety, and depression. Most of these subgroups had average scores of depression and anxiety which were above the threshold for referral to counselling.”
Respondents were also asked to provide data on the frequency and strength of the cannabis they were using so that researchers could track their average weekly consumption of Tetrahydrocannabinol (THC) – the principle psychoactive component of cannabis.
The researchers found that the average respondent consumed 206 units of THC a week. This might equate to roughly 10-17 ‘joints’ per week, if the user was consuming an expected 20% THC content that is standard for the most common types of cannabis available in London.
However, respondents who started using cannabis to help with their anxiety, depression, or in cases where they started due to others in their household who were already using cannabis, reported on average 248, 254.7, and 286.9 average weekly THC units respectively.
Professor Tom Freeman, Director of the Addiction and Mental Health Group at the University of Bath and one of the study’s authors said, “A key finding of our study is that people who first used cannabis to manage anxiety or depression, or because a family member was using it, showed higher levels of cannabis use overall.
“In future, standard THC units could be used in a similar way to alcohol units – for example, to help people to track their cannabis consumption and better manage its effects on their health.”
In a separate study, published in Psychological Medicine, researchers explored the relationship between childhood trauma, paranoia and cannabis use.
Researchers used the same data set from the Cannabis & Me survey, with just over half of respondents (52 per cent) reporting experience of some form of trauma.
Analysis established that respondents who had been exposed to trauma as children reported higher average levels of paranoia compared to those who hadn’t, with physical and emotional abuse emerging as the strongest predictors.
Researchers also explored the relationship between childhood trauma and weekly THC consumption. Respondents who reported experience of sexual abuse had a markedly higher weekly intake of THC, closely followed by those who reported experiencing emotional and physical abuse.
Finally, the researchers confirmed that the strong association between childhood trauma and paranoia is further exacerbated by cannabis use, but is affected by the different types of trauma experienced. Respondents who said they had experienced emotional abuse or household discord were strongly associated with increased THC consumption and paranoia scores. Respondents reporting bullying, physical abuse, sexual abuse, physical neglect and emotional neglect on the other hand did not show the same effects.
Dr Giulia Trotta, a Consultant Psychiatrist and Researcher at King’s IoPPN and the study’s first author said,
“We have not only established a clear association between trauma and future paranoia, but also that cannabis use can further exacerbate the effects of this, depending on what form the trauma takes.
“Our findings will have clear implications for clinical practice as they highlight the importance of early screening for trauma exposure in individuals presenting with paranoia.”
Professor Marta Di Forti, Professor of Drug use, Genetics and Psychosis at King’s IoPPN, Clinical Lead at the South London and Maudsley NHS Foundation Trust’s Cannabis Clinic for Patients with Psychosis, and the senior author on both studies said, “There is extensive national and international debate about the legality and safety of cannabis use.
“My experience in clinic tells me that there are groups of people who start to use cannabis as a means of coping with physical and emotional pain. My research has confirmed that this is not without significant further risk to their health and wellbeing, and policy makers across the world should be mindful of the impact that legalisation , without adequate public education and health support, could have on both the individual, as well as on healthcare systems more broadly.”
Every 34 seconds, someone in the United States dies from heart disease. As nearly half of the country suffers from some form of cardiovascular disease (CVD), another 1 in 4 adults experience a mental health disorder in their lifetime, signalling an inevitable overlap.
Now, a new report from Emory University shows that certain mental health conditions escalate the risk of developing heart disease by 50–100% – and adverse outcomes from existing heart conditions by 60–170%.
The report, published in The Lancet Regional Health-Europe, summarises cardiovascular health disparities among those diagnosed with depression, anxiety, schizophrenia, bipolar and post-traumatic stress disorders (PTSD). The article is part of a series aiming to raise awareness around disparities in CVD health in four populations: women, the elderly, racial minorities and those with mental health conditions.
Emory University professor Viola Vaccarino, MD, PhD, led this metareview linking mental health conditions to CVD, along with co-authors Amit Shah, MD, and Douglas Bremner, MD, also Emory professors.
The report associated the following conditions and their corresponding risks of developing CVD:
Major depression, 72%
PTSD, 57%
Bipolar disorder, 61%
Panic disorder, 50%
Phobic anxiety, 70%
Schizophrenia, nearly 100%
The research also shows that these conditions are associated with a poorer prognosis, greater risk for readmission and higher mortality from existing heart conditions. For example, major depression more than doubles the mortality rate in those with existing CVD.
Additionally, the report emphasises a bidirectional relationship. “More than 40 percent of those with cardiovascular disease also have a mental health condition,” adds Vaccarino.
The physiology of stress
According to the report, a well-documented relationship exists among depression, schizophrenia, PTSD, and abnormal stress responses in the autonomic nervous system (ANS) and hypothalamic-pituitary adrenal axis (HPA).
The former allows the brain to manage involuntary responses, such as functions of the liver, heart, sweat glands, and eye muscles. ANS also manages both acceleration and deceleration of these functions, regulating inflammatory responses. Since most major organs have ANS nerve endings, this system impacts most bodily functions.
The hypothalamic-pituitary adrenal axis (HPA) also influences immune response and metabolism, which can impact cardiovascular function.
According to the report, dysregulation of these systems creates “adverse downstream effects that can affect cardiovascular risk chronically, including increased inflammation, metabolic abnormalities, high blood pressure, enhanced systemic vascular resistance and autonomic inflexibility.” Inflammation has also been implicated in both the development of heart disease and mental health conditions.
Social determinants and quality of care
The role of social determinants of health in CVD disparities is critical. Those with mental health conditions may face disruptions and barriers in the continuum of care, such as affordability and accessibility. Compromised health literacy or communication can also impede access to health screenings and treatment.
Clinicians could also be challenged to care for patients with certain mental conditions, which can be compounded by stigma and existing models that fragment mental and physical health care. Stigmas are also present in the field of clinical research, where having a mental health condition is often an exclusionary criterion in randomised trials.
Moreover, according to the report, current prediction models don’t account for mental health disorders when forecasting the risk of developing heart disease.
Next steps toward a healthier future
To address the disparities of CVD among people with mental health disorders, the authors recommend an integrated approach with interdisciplinary care encompassing behavioural, mental and cardiovascular health.
“The tight connection between cardiovascular and psychological health warrants changes in the health care system that are more amenable to patients with comorbidities,” says Vaccarino. “A clinical team would be ideal for the care of these patients – a team of specialists, social workers, and nursing staff who work in collaboration to provide multidisciplinary care and resources.”
The report concludes that closing the health disparity gap upholds the rights of those living with a mental health condition to achieve the highest level of health and fully participate in society.
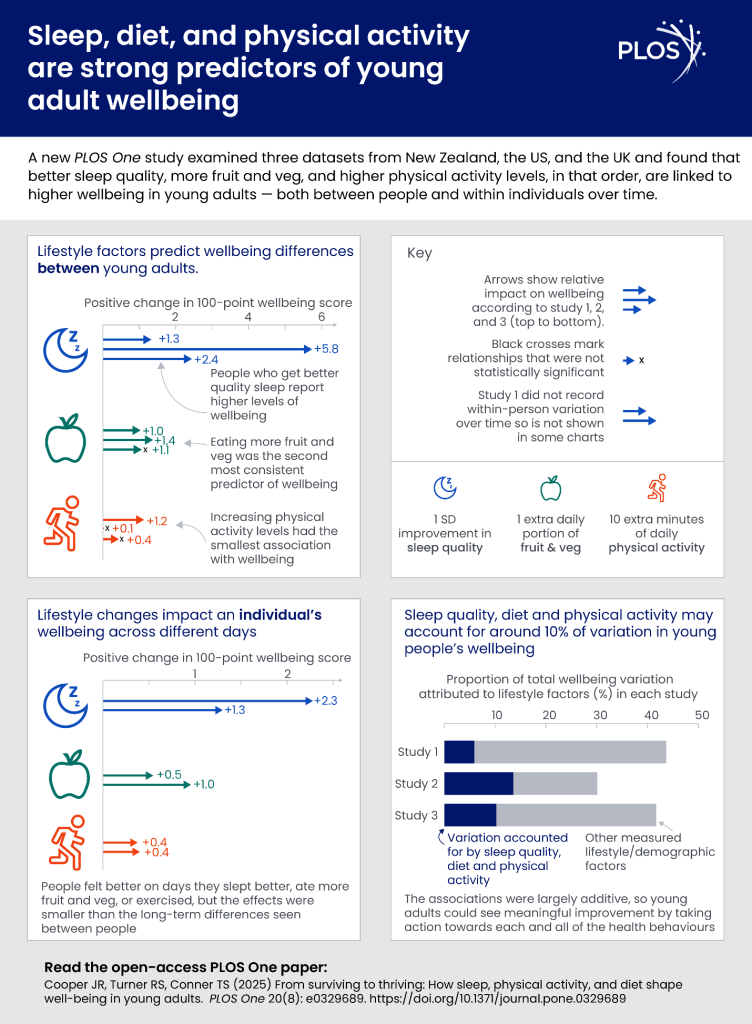
Study also suggests eating fruit and vegetables and exercising are linked with strong benefits – and fruit and vegetable consumption might compensate for poor sleep
A new study of young adults has strongly linked better sleep quality with better mental wellbeing, with fruit and vegetable consumption and physical activity also strongly associated with psychological wellbeing. Perhaps surprisingly, the findings also suggest that boosting fruit and vegetable intake could potentially help mitigate the effects on wellbeing of a poor night’s sleep. Dr Jack Cooper, previously from the University of Otago, New Zealand, and colleagues present these findings in the open-access journal PLOS One on August 27, 2025.
Prior research has linked better health behaviours—actions that people can adjust in their lives—to better physical health. Evidence also suggests that health behaviours may be linked to mental wellbeing. However, research on this topic has been limited. For example, studies have typically focused only on mental illness, a separate measure from positive psychological wellbeing, and they typically neglect to consider how different health behaviours might interact to affect wellbeing.
To address these and other gaps, Cooper and colleagues analysed relationships between three health behaviours – sleep quality, eating fruits and vegetables, and physical activity – and psychological wellbeing in adults aged 17 to 25. They used data from three studies: a survey study of 1032 adults in New Zealand, the UK, and the US; a 13-day study of 818 New Zealand adults who were asked to keep a daily diary; and an 8-day diary study of 236 New Zealand adults who also wore Fitbits tracking physical activity.
Across all three studies, better sleep quality was most strongly associated with better mental wellbeing, with fruit and vegetable consumption coming in second. Both behaviours showed benefits even when comparing between different days for the same person – so eating more fruit and vegetables one day was associated with a real-time wellbeing boost. Physical activity – whether measured by FitBits or diaries, which aligned – was also linked to better wellbeing, but mostly when comparing between days for an individual rather than when comparing across individuals.
Links between each of the three behaviors and wellbeing appeared to be independent and additive – which might mean that the more of them you do, the bigger the wellbeing benefit. The only exception: above-average intake of fruits and vegetables appeared to mitigate the effects of a poor night’s sleep, and a good night’s sleep appeared to protect against lower fruit and vegetable intake.
This study used samples of young adults from three countries—the U.K., U.S., and New Zealand—and samples sizes were relatively homogeneous. Future research could address some of these limitations by including participants from additional countries and increasing the sample size to improve generalizability. Although this study could not prove a causative link between these behaviors and mental wellbeing, the authors hope that their findings could inform efforts to improve psychological wellbeing of young adults.
Lead author Dr. Jack Cooper adds: “Young adults don’t have to reach some objective benchmark of healthiness to see wellbeing improvement. Sleeping a little better, eating a little healthier, or exercising even for 10 minutes longer than you normally do was associated with improvements to how you feel that day.”
Senior author Professor Tamlin Conner, of the University of Otago Psychology Department, adds: “Understanding what lifestyle factors support wellbeing can help young adults not just ‘get by’ but thrive during this critical life stage.”
“Of these healthy habits, sleep quality stood out as the strongest and most consistent predictor of next-day wellbeing, but eating fruit and vegetables and being active also helped boost wellbeing”.
“This age group faces unique pressures – such as leaving home, financial stress, educational pressures and social stressors – that can lower happiness. Understanding what lifestyle factors support wellbeing can help young adults not just ‘get by’ but thrive during this critical life stage.
Patients reported better sleep as well as decreased anxiety and pain over 18 months of treatment
Insomnia patients taking cannabis-based medical products reported better quality sleep after up to 18 months of treatment, according to a study published August 27 in the open-access journal PLOS Mental Health by Arushika Aggarwal from Imperial College London, U.K., and colleagues.
About one out of every three people has some trouble getting a good night’s rest, and 10% of adults meet the criteria for an insomnia disorder. But current treatments can be difficult to obtain, and the drugs approved for insomnia run the risk of dependence. To understand how cannabis-based medical products might affect insomnia symptoms, the authors of this study analysed a set of 124 insomnia patients taking medical cannabis products. They examined the patient’s reports of their sleep quality, anxiety/depression, and quality of life changes between one and 18 months of treatment.
The patients reported improved sleep quality that lasted over the 18 months of treatment. They also showed significant improvements in anxiety/depression as well as reporting less pain. About 9% of the patients reported adverse effects such as fatigue, insomnia, or dry mouth, but none of the side effects were life-threatening. While randomised controlled trials will be needed to prove that the products are safe and effective, the authors suggest that cannabis-based medical products could improve sleep quality in insomnia patients.
Co-author Dr Simon Erridge, Research Director at Curaleaf Clinic, summarises: “Over an 18-month period, our study showed that treatment for insomnia with cannabis-based medicinal products was associated with sustained improvements in subjective sleep quality and anxiety symptoms. These findings support the potential role of medical cannabis as a medical option where conventional treatments have proven ineffective, though further randomised trials are needed to confirm long-term efficacy.”
He adds: “Conducting this long-term study provided valuable real-world evidence on patient outcomes that go beyond what we typically see in short-term trials. It was particularly interesting to observe signs of potential tolerance over time, which highlights the importance of continued monitoring and individualised treatment plans.”
New research, led by Queen Mary University of London and published in Clinical Psychological Science, has revealed that highly sensitive people (HSP) are more likely to experience mental health problems compared to individuals who are less sensitive.
The meta-analysis of 33 studies, the first of its kind, looked at the relationship between sensitivity and common mental health problems such as depression and anxiety. Researchers found there was a significant, positive relationship between the two, concluding that highly sensitive people are more likely to experience depression and anxiety compared to those who are less sensitive.
In the study, sensitivity was defined as a personality trait that reflects people’s capacity to perceive and process environmental stimuli such as bright lights, subtle changes in the environment and other peoples’ moods. Often overlooked in mental health studies and clinical practice, which tend to focus on neuroticism and its association with mental health conditions, this research shows that understanding a person’s sensitivity level is important and can have therapeutic implications.
People with sensitive personality traits may benefit from different treatment plans
For example, people with more sensitive personality traits may be more likely to benefit from treatment plans which involve techniques such as applied relaxation and mindfulness, which can also prevent relapse.
Tom Falkenstein, a psychotherapist and a PhD student at Queen Mary University of London, said: “This is the most extensive systematic review on sensitivity and mental health in adolescents and adults to date, and is the first ever meta-analysis on the topic to estimate the impact of this relationship. We found positive and moderate correlations between sensitivity and various mental health problems such as depression, anxiety, post-traumatic stress disorder, agoraphobia and avoidant personality disorder. Our findings suggest that sensitivity should be considered more in clinical practice which could be used to improve diagnosis of conditions.”
“In addition, our findings could help improve treatment for these individuals. Around 31% of the general population are considered highly sensitive, and, as our findings show, are more likely to respond better to some psychological interventions than less sensitive individuals. Therefore, sensitivity should be considered when thinking about treatment plans for mental health conditions. Our work shows it is crucial that the awareness of sensitivity is improved among mental health care professionals, so clinicians and practitioners can recognise the trait in their patients, and tailor treatment to their sensitivity.”
Michael Pluess, Professor in Developmental Psychology at University of Surrey and Visiting Professor at Queen Mary University of London said: “This is the first meta-analysis providing robust evidence that highly sensitive people are more prone to common mental health problems. However, it is important to remember that highly sensitive people are also more responsive to positive experiences, including psychological treatment. Our results provide further evidence that sensitive people are more affected by both negative and positive experiences and that the quality of their environment is particularly important for their well-being.”
The systematic review and meta analysis of 33 studies was carried out by an academic team from several universities including Queen Mary University and the University of Surrey.
A new article published in the Canadian Medical Association Journal warns of the mental health dangers stemming from the increasing potency of cannabis. In Ontario, there has been a more than 14-fold increase in risk for visiting the emergency department for cannabis-related schizophrenic disorders. After a cannabis-induced psychotic episode, cessation of cannabis use is necessary to reduce the risk of relapse, and in severe cases, antipsychotics may be needed.
“Cannabis from the 2000s is not the same as in 2025,” said coauthor Dr Nicholas Fabiano, MD, resident and researcher with the Department of Psychiatry, University of Ottawa, Ottawa, Ontario. “THC content has increased by 5 times. This is likely a significant driver in the increasing link between cannabis use and schizophrenia.”
Cannabis potency is increasing — The concentration of tetrahydrocannabinol (THC) has increased fivefold in the last 20 years in Canada from about 4% to 20% in most legal dried cannabis.
High-potency and regular cannabis use is linked to increased risk of psychosis — The risk of psychosis is increased in people using high-potency THC (more than 10% THC), people using it frequently, and those who are younger and male. A history of mental disorders (depression, anxiety, etc) also appears to increase the risk.
Cannabis-induced psychosis and cannabis use disorder increase the risk of schizophrenia — A recent study of 9.8 million people in Ontario found a 14.3-fold higher risk of developing a schizophrenia-spectrum disorder in people visiting the emergency department for cannabis use and a 241.6-fold higher risk from visits for cannabis-induced psychosis.
Treatment requires stopping cannabis and taking medication — Continued use of cannabis after a first episode of cannabis-induced psychosis is linked to greater risk of returning symptoms. Antipsychotic medication can help people with severe and prolonged symptoms.
Behavioural options may help with cannabis cessation — Motivational interviewing or cognitive behavioural therapy by a physician or psychologist can help build skills to resist cravings and follow treatment recommendations.
In Brazil, belief in reincarnation is common, with up to a third of people believing it is possible. Some claim to have memories of their past lives. Researchers analysed the profile of adults who claim to have past-life memories, the features of these memories, and their associations with mental health, happiness, and religiosity/spirituality. The results indicated a high prevalence of mental disorder symptoms, with religiosity and spirituality being protective factors.
Most religious and spiritual traditions worldwide share a belief in a transcendental realm and/or the continuity of life after physical death. This belief is common among the adult population of 35 countries across six continents, with percentages ranging from 38% in Sweden to 85% in Indonesia.
A recent survey, involving nationally representative samples in 22 countries across all continents, concluded that there are no countries where most of the population said they did not believe in life after death, with the majority answering “yes” or “unsure” to this question.
While there are studies of claims of past-life memories (PLM) in children, there is still little knowledge about cases in adults and the impact of PLM on claimers. To fill this gap, Sandra Maciel de Carvalho and her team analysed the profile of adults who claim to have PLM, including sociodemographic data, the features of these memories, and their associations with mental health, happiness, and religiosity/spirituality.
With support from the BIAL Foundation, researchers from the Federal University of Juiz de Fora (Brazil) and the University of Virginia (USA) performed an online survey for the first time among a sample of 402 adults living in Brazil who reported having memories of past lives. In this country, 66% of citizens say that there is probably, or definitely, life after death, and 33% believe that people will be reborn in this world.
Most of the sample participants were middle age 41.6 years, female (79%), with higher education (68%), Spiritists (54.5%), and very/moderately spiritual (91%). PLM started spontaneously in 82%, on average, at 19.9 years old. Birthmark/defect (54%), unusual philia (intense and unusual attractions or interests; 30%), and phobia in childhood (71%), and persistent phobia (71%) were commonly associated features.
In this sample, childhood philias and phobias were associated with lower happiness and more symptoms of mental disorders (46%), which may indicate a lasting psychological impact associated with PLM. Post-traumatic stress disorder (36%) was associated with phobias. Religion/spirituality was associated with greater happiness and lower mental disorder outcomes, potentially acting as a protective factor.
According to Sandra Maciel de Carvalho, “this study demonstrated that PLM in adults may be more prevalent than previously thought and may be associated with significant suffering and distress”. PLM may constitute a “relevant issue in mental health, and further studies are needed on its prevalence, impact, and proper clinical management”, the researcher emphasises.
Learn more about the project “89/18 – National survey of “Cases of Reincarnation Type” in Brazil” here.