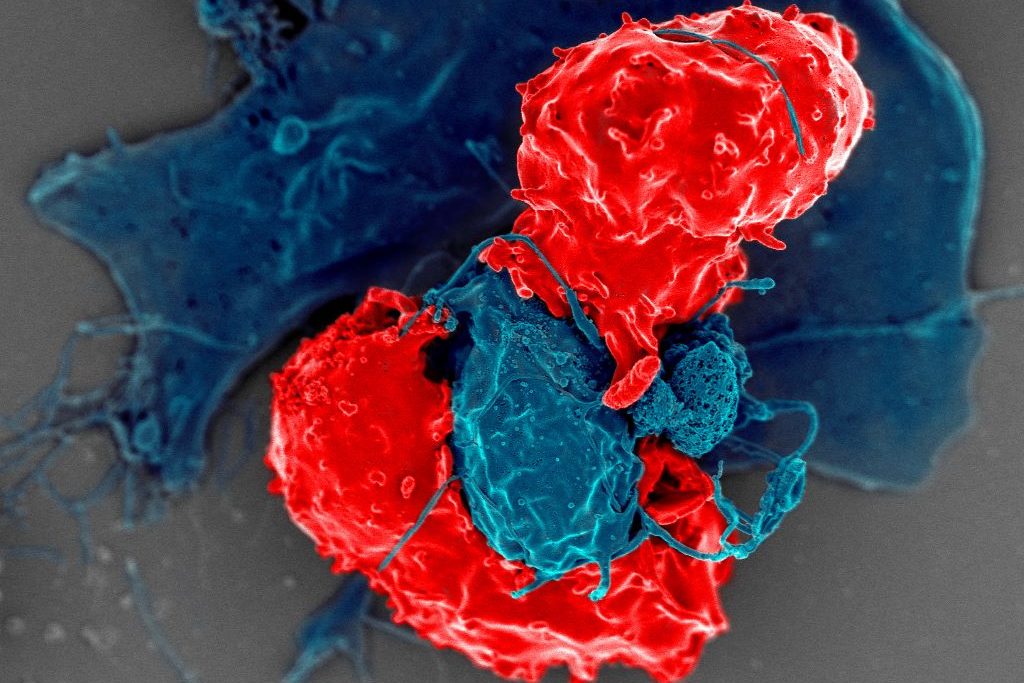
Scanning electron microscope image of T regulatory cells (red) interacting with antigen-presenting cells (blue). T regulatory cells can suppress responses by T cells to maintain homeostasis in the immune system. Credit: National Institute of Allergy and Infectious Diseases/NIH
Cedars-Sinai Health Sciences University investigators have identified for the first time a protein’s role as a “dimmer switch” that can calm an overactive immune system and restrain harmful inflammation. The protein, Butyrophilin 2A2 (BTN2A2), interacts with a key molecule that controls the strength of T-cell responses.
The findings, published inNature Communications, define a unique pathway that helps balance immune activity and could be harnessed to limit damage caused by a variety of autoimmune diseases.
In laboratory mice, loss of BTN2A2 led to exaggerated immune reactions and an increase in damaging kidney inflammation called glomerulonephritis. Treatment with BTN2A2 reduced disease severity by increasing immune-regulating T cells and lowering inflammation.
Supporting laboratory experiments in human T-cells demonstrated similar immune-calming effects.
“Glomerulonephritis remains a leading cause of chronic kidney disease and kidney failure worldwide, with limited treatment options,” said Ananth Karumanchi, MD, co-corresponding author of the study and director of the Renovascular Research Center at Cedars-Sinai. “Our findings provide a strong foundation for future studies aimed at modifying immune-driven kidney disease rather than simply managing its symptoms. The pathway could also be targeted in a range of autoimmune and inflammatory diseases including rheumatoid arthritis, multiple sclerosis, inflammatory bowel disease, and transplant rejections.”
Other Cedars-Sinai authors include Shafat Ali, Anders H. Berg, Michifumi Yamashita, Ambart E. Covarrubias, Jordan Mundell, Pranali N. Shah, Ruan Zhang, Vincent Dupont, Bong-Ha Shin, Shen Yang, Madhusudhanarao Katiki, Ramachandran Murali, Margareta D. Pisarska, Ravi Thadhani, Peter S. Heeger and Stanley C. Jordan
An international research group directed by UMC Utrecht have developed and characterised two first-in-class antibodies that specifically block the high-affinity IgG receptor FcγRI. Their findings open new perspectives for therapeutic modulation of FcγRI-driven inflammation in autoimmune diseases such as rheumatoid arthritis (RA), systemic lupus erythematosus (SLE) and immune thrombocytopenia (ITP).
FcγRI, also known as CD64, is a high-affinity receptor on myeloid cells that binds to the Fc region of immunoglobulin G (IgG) antibodies. It plays a key role in immune defence by triggering cellular functions such as phagocytosis and cytokine production. In a normal immune response, FcγRI is activated by immune complexes – clusters of antibodies bound to pathogens, which mark them for clearance. In autoimmune diseases, however, the immune system mistakenly targets the body’s own tissues (such as joint proteins in RA, nuclear antigens in SLE, or platelets in ITP), which results in the production of autoantibodies that form immune complexes. These misdirected complexes activate FcγRI unnecessarily, driving chronic inflammation and subsequent tissue damage.
The study, led by Prof Jeanette Leusen, PhD from the Antibody Therapy research group at the Center for Translational Immunology (UMC Utrecht) and carried out by PhD candidate Tosca Holtrop MSc, was a true team effort, in collaboration with experts from Kiel University (Germany), Leiden University Medical Center, Utrecht University, and Friedrich-Alexander University Erlangen-Nürnberg (Germany).
Discovery of first-in-class antibodies
For over 30 years, scientists have tried to generate antibodies against the IgG-binding domain of CD64, but the receptor’s extremely high affinity for IgG made this impossible with earlier technologies. Combining the UMAB unique immunisation method with novel phage display antibody libraries, the team bypassed this challenge by excluding the Fc region of the antibodies. This allowed them to discover two unique Fc-silent antibodies, C01 and C04, that bind purely via their Fab domains to FcγRI. Crystal structural analysis confirmed that C01 binds precisely within the IgG-binding site on EC2, making binding mutually exclusive.
High affinity for FcγRI
Quantitative binding studies revealed that both antibodies have higher affinity for FcγRI than human IgG, allowing them to efficiently displace IgG or pathogenic immune complexes up to 60 percent and block binding up to 90 percent. Importantly, neither antibody triggered FcγRI activation, a critical distinction from earlier anti-FcγRI antibodies, which could inadvertently trigger receptor clustering and cytokine release.
Subsequently. an in vitro model for immune thrombocytopenia was set-up, where C01 and C04 effectively inhibited opsonized platelets from binding to immune cells from ITP patients. In a preclinical in vivo ITP model, the antibodies significantly reduced IgG-dependent platelet depletion. The antibodies were also tested in an in vitro rheumatoid arthritis models, where they effectively inhibited patient-derived autoantibody–immune complex binding to monocytes, macrophages, and neutrophils from healthy donors.
Promising therapeutic candidate drugs
The study demonstrates that direct Fab-mediated inhibition of FcγRI is feasible and effective, opening a new avenue for treating autoimmune diseases characterised by IgG-autoantibody complexes. By preventing immune complex–driven activation without triggering the receptor, C01 and C04 represent a promising next step toward targeted, inflammation-sparing immunotherapy. “I think we found the needle in the haystack, after searching over a decade and thanks to a true team effort,” says Jeanette Leusen, principal investigator of the study. “Each research partner contributed a critical piece, from antibody discovery and structure determination to patient sample testing and preclinical models. Only together could we bring this to fruition. These antibodies not only provide a unique tool for studying FcγRI biology, but also hold promise as therapeutic candidates in autoimmune and infectious diseases.”
Korean children with early life exposure to antibiotics were not diagnosed with autoimmune diseases at higher rates
Photo by Chayene Rafaela on Unsplash
The global incidence of autoimmune diseases among children has increased over the past few decades. A study published August 21st in the open-access journal PLOS Medicine by Ju-Young Shin at Sungkyunkwan University, Republic of Korea, and colleagues suggests that early life antibiotic exposure is not associated with an increased risk of autoimmune diseases in children.
Previous research has suggested that exposure to antibiotics as a foetus or infant may contribute to the development of autoimmune diseases among children. However, confounding variables limit the validity of prior studies and the association of antibiotics to autoimmune disease remains poorly understood.
In order to investigate whether antibiotics may increase risk of autoimmune diseases, researchers conducted a retrospective cohort study comprised of over 4 million children born in the Republic of Korea between April 1, 2009, and December 31, 2020. They accessed a mother-child linked insurance claims database from the South Korea National Health Insurance Service-National Health Insurance Database (NHIS-NHID) to identify children whose mothers had received antibiotic prescriptions during pregnancy or while breastfeeding their infant. The researchers then retrospectively analysed the health outcomes of each cohort for a period of over 7 years, tracking all diagnoses of Type 1 diabetes, Juvenile idiopathic arthritis, Inflammatory bowel disease (ulcerative colitis, Crohn’s disease), Systemic lupus erythematosus, and Hashimoto’s thyroiditis.
The researchers found no relationship between antibiotic exposure during pregnancy or early infancy and the overall incidence of autoimmune diseases in children. Future research is needed, however, to replicate the outcomes in other populations and to further investigate potential effects on subgroups.
According to the authors, “Our findings suggest no association between antibiotic exposure during the prenatal period or early infancy and the development of autoimmune diseases in children. This observation contrasts with several previous studies reporting increased risks and underscores the importance of carefully considering the underlying indications for antibiotic use and genetic susceptibility when interpreting such associations. While the potential benefits of antibiotic treatment in managing infections during pregnancy or early infancy likely outweigh the minimal risk of autoimmune outcomes, our findings also highlight the need for cautious and clinically appropriate use of antibiotics during these critical developmental periods in specific subgroups.”
The authors note, “Exposure to antibiotics during pregnancy or early infancy was not associated with an increased risk of autoimmune diseases in children. Nevertheless, the importance of follow-up studies to confirm and extend these findings cannot be overstated.”
Many diseases affect men and women differently. Asthma tends to strike men earlier in life, yet more women develop asthma as they get older. Parkinson’s is more common in men, but Alzheimer’s is more common in women.
The differences are even more stark when it comes to autoimmune disease. Women are around two and a half times more likely than men to develop multiple sclerosis and nine times more likely to develop lupus.
Why would some diseases strike one sex more than another? And why do some tissues, such as the lungs and brain, seem especially vulnerable to these sex-based differences?
To answer these questions, scientists at La Jolla Institute for Immunology (LJI) are leading new research into how our immune cells defend specific parts of the body.
“In just the last two years, LJI scientists have uncovered a whole new body of information about how the immune systems of men and women are very different,” says Saphire. “We’re looking at what is genetically encoded in our XX or XY chromosomes, and how hormones like oestrogen and testosterone affect what is genetically programmed into our immune cells.”
In the paper, the researchers define biological sex (in an immunology context) as the presence of XX chromosomes in females and XY chromosomes in males. “Every cell in your body is either XX or XY,” says Saphire. “That X chromosome has many, many immune-related genes. Women have two copies of each. That gives them, in a sense, twice the palette of colours to paint from in formulating an immune response. It can also give them a stronger immune response for those genes that are doubly active – active in both copies simultaneously.
Sex hormones are important for much more than reproductive function. Immune cells can also sense hormones such as oestrogen and testosterone and use them to determine which genes to turn on or off and which ones to turn on more brightly or dim. This means similar immune cells can do different things, depending on whether that cell is from a male or a female.
Further, female cells vary in which of their two copies of X is “turned on.” As a result, women have organs with a collage, or mosaic, of immune cells that work differently in different tissues. This innate “variety” of immune cells appears to be an effective way to ward off infectious disease (women are better than men at fighting off pathogens such as SARS-CoV-2).
But scientists have also found that having more genes from X chromosomes may predispose women to autoimmune disease. This increased X chromosome “dosage” is closely linked to a higher risk for autoimmune diseases such as Sjögren’s syndrome and scleroderma.
New research into sex-based immune system differences is also critical for developing new cancer immunotherapies, Sharma explains.
“We’re increasingly understanding how sex-based differences affect disease outcomes. When it comes to medicine, one size doesn’t fit everybody,” says Sharma, who directs LJI’s Center for Sex-Based Differences in the Immune System. “This is leading to new research, particularly in the cancer field, toward precision medicine. We’re asking how a person’s individual immune system is contributing to controlling that cancer through immunotherapy.”
Saphire and Sharma also highlight environmental factors, such as nutrition and chemical exposures, that may add to the complex interplay of chromosomes and sex hormones. Men and women also appear to have some signature differences in their skin and gut microbiomes.
The researchers hope these foundational discoveries can lead to medical advances for all, and they’re working with collaborators across the country to move this research forward. “It takes a team to translate these findings,” says Sharma.
A woman with Systemic Lupus Erythematosus. Source: Wikimedia CC0
Researchers have found that certain antiviral genes become less active over time in lupus, revealing why some patients see their symptoms fade as they age.
It causes the immune system’s first-line viral defences, known as interferons, to attack the body. Nearly every organ is at risk, leading to conditions like kidney and heart disease.
But unlike many other autoimmune or chronic illnesses, lupus can improve as patients reach their 60s and 70s. University of California San Francisco researchers have now found a potential explanation.
“I see my younger lupus patients in their 20s, 30s, and 40s every few months, monitoring them closely for signs of severe disease, but many of my older patients just once a year to touch base,” said Sarah Patterson, MD, assistant professor of medicine in the division of rheumatology at UCSF. “If patients make it through those risky decades, they sometimes see a dramatic improvement.”
By analysing blood samples from patients across the age spectrum, the team discovered that aging turns down the activity of certain immune genes in people with lupus, leading to fewer interferons and other inflammatory proteins in the body.
The study found that in healthy adults, inflammation-related genes and proteins rose slowly over the years, a process that has been dubbed “inflammaging.” In patients with lupus, however, the expression of these genes and proteins were abnormally high in mid-life but decreased as the decades went by.
“Inflammaging seemed to be reversed in the lupus patients,” said Chaz Langelier, MD, PhD, associate professor of medicine at UCSF and senior author of the paper. “But it wasn’t fully reversed. The lupus patients still had a greater level of inflammatory signaling compared to healthy adults in older age.”
That reversal reflected what Patterson has seen in her patients — a return to something approaching healthy older age.
Next, the team intends to test whether drugs that block interferons are more or less effective in lupus patients at different ages. They also hope to extend the approach to understand other inflammation-related conditions, such as rheumatoid arthritis, COPD, and atherosclerosis.
A woman with Systemic Lupus Erythematosus. Source: Wikimedia CC0
Chronic inflammation occurs when the immune system is stuck in attack mode, sending cell after cell to defend and repair the body for months or even years. Diseases associated with chronic inflammation, like arthritis or cancer or autoimmune disorders, weigh heavily on human health – and their incidence is expected to rise. A new study by investigators from Mass General Brigham identified a protein called WSTF that could be targeted to block chronic inflammation. Crucially, this strategy would not interfere with acute inflammation, allowing the immune system to continue responding appropriately to short-term threats, such as infection by a pathogen. Results are published in Nature.
“Chronic inflammatory diseases cause a great deal of suffering and death, but we still have much to learn about what drives chronic inflammation and how to treat it,” said senior author Zhixun Dou, PhD, of the Center for Regenerative Medicine and Krantz Family Center for Cancer Research at Massachusetts General Hospital. “Our findings help us separate chronic and acute inflammation, as well as identify a new target for stopping chronic inflammation that results from aging and disease.”
Using chronically inflamed human cells, the researchers found that WSTF interacts with other proteins inside cell nuclei, which prompts its excretion and degradation. Since WSTF is responsible for concealing pro-inflammatory genes, this nucleus-eviction reveals those genes and, in turn, amplifies inflammation. They confirmed that WSTF loss could promote inflammation in mouse models of aging and cancer. They also found, using human cells, that WSTF loss only occurred in chronic inflammation, not acute. Using these findings, the researchers designed a WSTF-restoring therapeutic to suppress chronic inflammation and observed preliminary success in mouse models of aging, metabolic dysfunction-associated steatohepatitis (MASH), and osteoarthritis.
The researchers went further to examine tissue samples from patients with MASH or osteoarthritis. They found that WSTF is lost in the livers of patients with MASH, but not in the livers of healthy donors. Using cells from the knees of osteoarthritis patients undergoing joint replacement surgery, they showed that WSTF-restoring therapeutic reduces chronic inflammation from the inflamed knee cells. These findings highlight the potential of developing new treatments targeting WSTF to combat chronic inflammatory diseases.
Further research is needed to validate the therapeutic potential of WSTF restoration in broader settings and to develop specific strategies to target WSTF. Additionally, the findings suggest other similar proteins may be involved in chronic inflammation, opening a promising new avenue for studying and treating inflammation in the future.
Risks higher in women than in men with the same condition Chronic exposure to systemic inflammation may explain associations, say researchers
Photo by Sydney Sims on Unsplash
Living with an autoimmune disease is linked to a near doubling in the risk of persistent mental health issues, such as depression, generalised anxiety, and bipolar disorder, with these risks higher in women than in men, finds a large population-based UK study, published in the open access journal BMJ Mental Health.
Chronic exposure to the systemic inflammation caused by the autoimmune disease may explain the associations found, say the researchers.
A growing body of evidence suggests that inflammation is linked to mental ill health, but many of the published studies have relied on small sample sizes, limiting their statistical power, note the researchers.
In a bid to overcome this, they drew on data from 1.5 million participants in the recently established Our Future Health dataset from across the UK. Participants’ average age was 53; just over half (57%) were women; and 90% identified as White.
On recruitment to Our Future Health, participants completed a baseline questionnaire to provide personal, social, demographic, health and lifestyle information.
Health information included lifetime diagnoses–including for their biological parents–for a wide range of disorders, including autoimmune and psychiatric conditions.
Six autoimmune conditions were included in the study: rheumatoid arthritis; Graves’ syndrome (thyroid hormone disorder); inflammatory bowel disease; lupus, multiple sclerosis; and psoriasis.
The mental health conditions of interest were self-reported diagnoses of affective disorders, defined as depression, bipolar, or anxiety disorder.
In all, 37 808 participants reported autoimmune conditions and 1 525 347 didn’t. Those with autoimmune conditions were more likely to be women (74.5% vs 56.5%) and more likely to report lifetime diagnoses of affective disorders for their biological parents: 8% vs 5.5% for fathers; 15.5% vs 11% for mothers.
Chronic and pathogenic immune system activation—including the presence of markers of inflammation—is a hallmark of many autoimmune conditions. And in the absence of direct measurements of inflammatory biomarkers, an autoimmune condition was regarded as a proxy for chronic inflammation in this study.
The lifetime prevalence of any diagnosed affective disorder was significantly higher among people with an autoimmune disorder than it was among the general population: 29% vs 18%.
Similar associations in lifetime prevalence emerged for depression and anxiety: 25.5% vs just over 15% for depression; and just over 21% vs 12.5% for anxiety.
While the overall prevalence of bipolar disorder was much lower, it was still significantly higher among those with an autoimmune disorder than it was among the general population: just under 1% compared with 0.5%.
The prevalence of current depression and anxiety was also higher among people with autoimmune conditions.
And the prevalence of affective disorders was significantly and consistently higher among women than it was among men with the same physical health conditions: 32% compared to 21% among participants with any autoimmune disorder.
The reasons for this aren’t clear, say the researchers, but “theories suggest that sex hormones, chromosomal factors, and differences in circulating antibodies may partly explain these sex differences,” they write.
“Women (but not men) with depression exhibit increased concentrations of circulating cytokines and acute phase reactants compared with non-depressed counterparts. It is therefore possible that women may experience the compounding challenges of increased occurrence of autoimmunity and stronger effects of immune responses on mental health, resulting in the substantially higher prevalence of affective disorders observed in this study,” they add.
Overall, the risk for each of the affective disorders was nearly twice as high—87-97% higher—in people with autoimmune conditions, and remained high even after adjusting for potentially influential factors, including age, household income, and parental psychiatric history.
No information was available on the time or duration of illness, making it impossible to determine whether autoimmune conditions preceded, co-occurred with, or followed, affective disorders, note the researchers.
No direct measurements of inflammation were made either, and it was therefore impossible to establish the presence, nature, timing or severity of inflammation, they add.
“Although the observational design of this study does not allow for direct inference of causal mechanisms, this analysis of a large national dataset suggests that chronic exposure to systemic inflammation may be linked to a greater risk for affective disorder,” they conclude.
“Future studies should seek to determine whether putative biological, psychological, and social factors—for example, chronic pain, fatigue, sleep or circadian disruptions and social isolation—may represent potentially modifiable mechanisms linking autoimmune conditions and affective disorders.”
And they suggest that it may be worth regularly screening people diagnosed with autoimmune disease for mental health conditions, especially women, to provide them with tailored treatment early on.
Killer T cells about to destroy a cancer cell. Credit: NIH
Researchers have discovered a genomic ‘brake’ in a subset of immune cells that could help advance immunotherapy for cancer and autoimmune disease. The findings, led by a team at the Peter MacCallum Cancer Centre in collaboration with researchers at the Garvan Institute and Kirby Institute, provide new insights into how the body’s immune defence mechanisms can go awry in these diseases and open a new class of potential drug targets that could activate immune cells in tumour tissue.
The research was published in the journal Immunity.
Discovering an immune brake
Specialised killer T cells are released during an infection, trained to recognise and destroy the threat. When unchecked, these cells can cause autoimmune diseases such as type 1 diabetes or rheumatoid arthritis if they mistakenly attack the body’s own healthy tissues.
The immune system employs a mechanism to prevent autoimmune attacks called ‘tolerance’ – a process that can be exploited by cancer cells to shield them from the body’s natural defences.
“Until now, it was not fully understood how tolerance works at a molecular level. We used advanced sequencing techniques to identify a unique genomic signature in ‘tolerant’ T cells that differentiated them from killer T cells that were activated in response to viral infection,” says Dr Timothy Peters, co-first author from Garvan.
“These precise genome locations have never before been observed and allowed us to track precisely how killer T cells progress through the tolerance pathway, and how specific gene networks enable tolerance to be abused.”
Breakthrough for cancer and autoimmune disease
Dr Ian Parish, who led the research at the Peter MacCallum Cancer Centre said this breakthrough helps to understand why cancer treatments fail and opens the door to developing new treatments in the future.
“Current cancer immunotherapy treatments target the exhaustion phase of the immune response,” he said. “Our research suggests that a second, earlier ‘off-switch’ called tolerance may explain how many cancers resist current immunotherapies by blocking anti-cancer immunity from getting off the ground. We’re excited as these findings can be exploited for new treatments. Our next step is to understand if we can disrupt tolerance and engage the immune system to restart and attack those cancers resistant to treatment.”
Professor Chris Goodnow, Head of the Immunogenomics Lab at Garvan, says this new understanding of T cell tolerance opens up opportunities to develop new drugs that could selectively alter this pathway.
“The discovery of these gene locations provides us with a roadmap for developing future drugs, which could block the tolerance mechanisms to boost cancer-killing ability for immunotherapies. Conversely, for autoimmune diseases, enhancing tolerance could prevent harmful autoimmune attack,” he says.
In next steps, the researchers will focus on understanding how to disrupt the tolerance mechanism and engage the immune system to restart.
“These findings have revealed around 100 new potential targets for drugs to target the tolerance mechanism in T cells, which have until now been largely developed by trial and error,” says Professor Goodnow. “This could lead to a whole new class of treatments for autoimmunity and cancer.”
Professor Chris Goodnow is The Bill and Patricia Ritchie Foundation Chair and Director of the Cellular Genomics Futures Institute, UNSW Sydney. Dr Tim Peters is a Conjoint Lecturer at St Vincent’s Clinical School, UNSW Medicine and Health.
When the NKp46 receptor of the ILCs is blocked (right), the lupus nephritis recedes. Blue: cell nuclei. Credit: Charité | Frauke Schreiber
A Berlin-led research team has uncovered critical regulators of severe kidney damage in patients with the autoimmune disorder lupus. A small, specialised population of immune cells – called innate lymphoid cells (ILCs) – trigger an avalanche of effects that cause harmful kidney inflammation, also known as lupus nephritis.
The research, published this week in Nature, upends conventional wisdom that autoantibodies are primarily responsible for lupus nephritis.
“While autoantibodies are required for tissue damage, they are by themselves not sufficient. Our work reveals that ILCs are required to amplify the organ damage,” says Dr Masatoshi Kanda, a senior paper author who was a Humboldt Fellow at Max Delbrück Center and is now at the Department of Rheumatology and Clinical Immunology, Sapporo Medical University in Japan.
Lupus, or systemic lupus erythematosus, is most often diagnosed between the ages of 15 and 45. Symptoms can range from mild to severe. But what causes kidney damage in some patients – some to the point of requiring dialysis – has been unclear.
“The role of ILCs in lupus or lupus nephritis was entirely unknown,” says Professor Antigoni Triantafyllopoulou, a senior paper author at the German Rheumatology Research Center (DRFZ), an institute of the Leibniz Association, and at the Department of Rheumatology and Clinical Immunology at Charité – Universitätsmedizin Berlin. “We have now identified most of the circuit controlled by ILCs by looking at the whole kidney at single-cell resolution.”
Unusual immune cells
ILCs are a small group of immune cells that – unlike most other immune cells that circulate throughout the body – live in a specific tissue or organ.
“They are in the tissue all the time, from the time of embryonic development, which makes them very different from other immune cells,” says Professor Andreas Diefenbach, a senior paper author and director of the Institute of Microbiology, Infectious Diseases and Immunology at Charité – Universitätsmedizin Berlin.
Diefenbach’s lab was among those that discovered ILCs in the mid-2000s. Most of his research is focused on ILCs in the gut and how they modify tissue function. In this study, Triantafyllopoulou and Kanda teamed up with his group and Dr Mir-Farzin Mashreghi at the DRFZ to find out whether ILCs were present in the kidney and what role they might play in lupus nephritis.
The whole single-cell picture
To unravel this mystery, the team turned to single-cell RNA sequencing, which identifies genes that are active, or “switched on,” in individual cells and helps researchers understand the cell’s identity and function.
Kanda, a rheumatologist who was studying bioinformatics in Professor Norbert Hübner’s lab at the Max Delbrück Center at the time, developed a specialized protocol for single-cell RNA sequencing of mouse and human kidneys. “Masatoshi’s protocol was very good at pulling out and preserving multiple types of kidney cells, which gave us a much more complete overview of how lupus affects the whole kidney,” explains Triantafyllopoulou. The team sequenced nearly 100 000 individual kidney and immune cells of various types and functions.
The key receptor
Through experiments in mice, the team learned that a subgroup of ILCs with a receptor called NKp46 must be present and activated to cause lupus nephritis. When NKp46 is activated, this subgroup of cells ramped up production of a protein called GM-CSF, which stimulates invading macrophages to multiply. In the kidney, a flood of incoming macrophages caused severe tissue damage and fibrosis.
“These ILCs are really amplifiers in this system,” Diefenbach says. “They are small in population, but they seem to fertilise the whole process.”
When the team blocked NKp46 with antibodies or the receptor was genetically removed, kidney tissue damage was minimal. They also blocked GM-CSF with similar anti-inflammatory effects.
“Critically, autoantibody levels did not change when NKp46 was inhibited, but kidney tissue damage was reduced, which shows autoantibodies are not directly responsible for kidney inflammation,” Triantafyllopoulou explains.
The team also compared the results to sequencing data from tissue taken from human patients with lupus and found ILCs present, though more work is required to fully understand how to target ILCs in human kidneys. Nevertheless, the insights gained through these detailed studies point to new antibody therapies for patients with severe forms of lupus. The hope is to prevent the need for kidney dialysis in these patients.
New research published in Arthritis & Rheumatologyindicates that chronic exposure to air pollutants may increase the risk of developing lupus, an autoimmune disease that affects multiple organs.
For the study, investigators analysed data on 459 815 participants from the UK Biobank. A total of 399 lupus cases were identified during a median follow-up of 11.77 years. Air pollutant exposure was linked with a greater likelihood of developing lupus. Individuals with a high genetic risk and high air pollution exposure had the highest risk of developing lupus compared with those with low genetic risk and low air pollution exposure.
“Our study provides crucial insights into the air pollution contributing to autoimmune diseases. The findings can inform the development of stricter air quality regulations to mitigate exposure to harmful pollutants, thereby reducing the risk of lupus,” said co–corresponding author Yaohua Tian, PhD, of the Huazhong University of Science and Technology, in China.