Groundbreaking research from the University of Houston shows that a single low-dose atropine eye drop can produce daylong effects in managing myopia, or nearsightedness.
Professor of Optometry Lisa Ostrin and postdoctoral researcher Barsha Lal are reporting that even one drop in the eye of low-dose atropine (0.01%–0.1%) produces clear changes in pupil size and focusing ability that persist for at least 24 hours. Importantly, they also found that the drop shows no short-term structural effects on the eye, with only temporary changes in blood flow inside the retina.
Ostrin’s latest research is published in the journal Eye and Vision. It adds to a growing body of vision research from David Berntsen, Golden-Golden Professor of Optometry at the University of Houston, who is co-leading a clinical trial to delay the development of myopia in children by using the atropine drops.
Low concentration atropine is widely prescribed to slow myopia progression in children, yet its short-term retinal and choroidal effects remain incompletely understood. Ostrin’s new study evaluated short-term effects of a range of low atropine concentrations on the length of the eye, the blood vessels in the retina and the thickness of the retina and choroid, which sits just behind the retina. These are important measurements because longer eye length is associated with myopia and as it gets longer, the retina and choroid are stretched.
“These findings indicate that a single instillation of atropine does not alter axial length or retinal or choroidal thickness over 24 hours but may transiently affect superficial retinal perfusion in a time-dependent manner,” said Ostrin.
In the double-masked, randomised study, twenty healthy adults received a single instillation of either a placebo or atropine in the right eye during five separate sessions. Researchers then checked the eye structure, thickness, and length in the central retina both one-hour and 24-hours later.
“Characterising these short-term effects is important for a better understanding of the physiological responses to atropine in clinical and research settings,” said Ostrin who previously published research results of a study investigating the short-term effects of a range of low-dose atropine concentrations on the pupils of young adults. In that study, she found similar results with a single drop of atropine inducing significant changes in the pupils.
Together, the studies indicate that atropine induces early functional and vascular effects in the eye, in the absence of structural change.
“By linking objective ocular responses with subjective visual experience, this work advances our understanding of how atropine works and supports more precise, evidence-based, and individualised approaches to myopia management,” said Ostrin.
South Africa is facing an alarming increase in non-communicable diseases and related mortality. According to Statistics South Africa, deaths due to non-communicable diseases such as type 2 diabetes and hypertension increased by over 58% between 1997 and 2018.
The crisis of overweight and obesity in the country adds to the risk of these diseases. Nearly 40% of the adult population is overweight. Although physical activity can help prevent and manage many non-communicable diseases, 47% of adults do not engage in any physical activity. Most people struggle to meet the World Health Organization’s recommended 150-300 minutes of moderate-intensity aerobic physical activity per week.
A significant part of the challenge is that people have adopted an “all or nothing” approach to physical activity. The perception is that one has to participate in structured workouts, such as gym sessions, running, or cycling.
Instead, research has shown that even brief, low-intensity movements can yield measurable physical and mental health benefits. Even everyday tasks count. New evidence shows that short movement bouts of less than five minutes can have positive health implications.
As researchers in exercise science and sports medicine we have observed that physical activity is particularly low in South Africa. Only 19.8% of adults meet the WHO’s guideline, against the global average of 73%.
Our study of 62 office-based workers at the University of the Witwatersrand also showed the short-term health impact of height-adjustable, sit-to-stand desks. Our intervention reduced prolonged sitting and slightly improved indicators such as body mass index and blood pressure. Given South Africa’s high burden of obesity and sedentary lifestyles among office workers, these improvements are encouraging and support global health messaging that even modest increases in daily movement can positively influence health.
These findings were the springboard for the “Mzansi, what’s your move?” campaign at the university. We want to encourage staff and students to move more by showing how simple actions add up to physical activity. The campaign is supported by a series of comics and murals on campuses.
Here, we highlight some of the actions that we used in our campaign to encourage everyone to get moving. These are daily tasks that may seem mundane but count as physical activity, while reflecting people’s realities.
Housework
Many people do not consider housework a form of physical activity. But tasks like sweeping, mopping or vacuuming require sustained movement and engage multiple muscle groups.
Scrubbing floors, washing windows and cleaning bathrooms involve movements such as squatting and stretching. Working in the garden can strengthen muscles too.
As part of our campaign, we’ve developed comic strips that highlight movements that can be done at home and in the community. We emphasise how all family members can move in ways that fit their lifestyles and physical abilities.
Active commuting
Walking or cycling to work or school contribute significantly to daily physical activity. Studies have shown that active commuting is associated with lower body fat, reduced blood pressure, and improved mental well-being.
Including movement into daily travel routines is a practical way to accumulate physical activity without setting time aside. Walking briskly to a train station, cycling a few kilometres to work, or taking a longer walking route to drop off children at school accumulates over time. Even seemingly small changes, such as getting off the bus one stop early or taking the stairs instead of the elevator, produce measurable health benefits over weeks and months.
However, achieving the full benefits of active commuting is complex and it relies on cities building and maintaining road infrastructure. In South Africa, safety is a legitimate concern for all road users. A 2024 Statistics South Africa report shows that more pedestrians than car occupants died in road crashes in 2007, 2013, and 2019. Another safety concern relates to the country’s high crime rates. People may be reluctant to walk, even in their own neighbourhoods.
These challenges are not insurmountable. For starters, people should consider people moving in groups, joining walking and running clubs.
Beyond what individuals can do, municipalities can do something about green spaces. This includes ensuring that parks are safe to walk in and are clean. Broken pavements and bicycle lanes need to be maintained in all neighbourhoods.
Incidental movements
Incidental movements refer to small bouts of activity that occur throughout the day. Integrating these movements into everyday life can yield significant health benefits, especially in office contexts, where many people sit for extended periods. Employers can try nudging staff, for example to use the stairs instead of elevators, with simple posters or painted footprints. Another way to encourage physical activity is to centralise shared equipment (printers, bins, water stations) so that staff walk short distances.
Micro-breaks also provide opportunities for informal movements. Stretching during meetings or after long sitting periods, standing discussions instead of seated ones, and walking meetings for small groups all contribute to the physical activity of employees.
In 2024, we investigated the short-term impact of physical activity interventions such as high-intensity interval training and moderate-intensity continuous training on 43 labourers at the University of the Witwatersrand. The number of participants in this study was small, but the findings show that our intervention reduced indicators such as waist circumference, body mass index, blood glucose and blood pressure, and improved physical fitness.
Way forward
People don’t need a gym membership or a strict workout schedule to get moving. Simple, everyday activities all add up to meaningful physical activity. Small movements help to reduce the risks of chronic diseases, strengthen muscles, boost mental wellbeing, and counteract the harmful effects of prolonged sitting.
These “movement snacks” make exercise accessible, manageable and sustainable, particularly for people who find structured workouts intimidating or time-consuming.
Researchers at Karolinska Institutet and KTH Royal Institute of Technology have developed an improved method for creating insulin-producing cells from human stem cells. The results, published in Stem Cell Reports, demonstrate that these cells effectively regulate blood sugar levels in laboratory tests and can reverse diabetes in mice.
Type 1 diabetes occurs when the immune system destroys insulin-producing cells in the pancreas, meaning the body can no longer absorb glucose from the blood and regulate blood sugar levels. One possible treatment is to replace these cells with new ones. However, previous methods of producing such cells from stem cells have often yielded mixed results.
“We have developed a method that reliably produces high-quality insulin-producing cells from multiple human stem cell lines. This opens up opportunities for future patient-specific cell therapies, which could reduce immune rejection,” says Per-Olof Berggren, professor at the Department of Molecular Medicine and Surgery, Karolinska Institutet, and corresponding author alongside Siqin Wu, researcher at Spiber Technologies AB (formerly at Karolinska Institutet).
Optimised cell production
The optimised production process yields more mature and purer insulin-producing cells than previous methods. In a laboratory setting, the cells were able to secrete insulin and responded strongly to glucose. When the researchers transplanted these cells into diabetic mice, the animals gradually regained the ability to regulate their blood sugar. The transplantation was performed in the anterior chamber of the eye.
“This is a technique we use to monitor the development and function of the cells over time in a minimally invasive way,” explains Per-Olof Berggren. “We observed that the cells gradually matured after transplantation, retaining their ability to regulate blood sugar for several months, which demonstrates their potential for future treatments.”
Stem cell therapy for type 1 diabetes is already being tested in several clinical trials. However, a challenge with previous methods is that the stem cells often develop into a combination of the desired and undesired cell types, increasing the risk of complications. Another challenge is that the insulin-producing cells created are often not mature enough to respond well to glucose.
Solving previous problems
By adjusting the culture steps and allowing the cells to form three-dimensional clusters themselves, many unwanted cell types are eliminated and the cells gain a better ability to respond to glucose, according to the researchers.
“This could solve several of the problems that have previously hindered the development of stem cell-based treatments for type 1 diabetes. Building on this, we will work towards clinical translation aiming at treating type 1 diabetes,” says Fredrik Lanner, professor at the Department of Clinical Science, Intervention and Technology, Karolinska Institutet, and last author of the paper.
Non-concussive head impacts correlated with changes to the gut microbiome on following days, in pilot study tracking six US collegiate football players over one season
Non-concussive head impacts – hits to the head that don’t cause clinically detectable symptoms – are correlated with subsequent changes to the gut microbiome in a small sample of US collegiate football players, according to a new study published May 6, 2026, in the open-access journal PLOS One by Ahmet Ay and Kenneth Douglas Belanger of Colgate University, USA, and colleagues.
Non-concussive head impacts are common in American football, with players experiencing between 100 and 1000 across a season. While research has shown that full concussions can disrupt the gut microbiome – which regulates inflammation and the neuroimmune system – whether sub-concussive hits might produce similar effects had not been investigated.
In the new study, researchers tracked six NCAA Division I American football players across a competition season, beginning during preseason training. Their on-field activity profiles were monitored using GPS units and head impacts were tracked using a helmet-based sensor system; 226 faecal samples were analysed for their microbiome composition; and participants completed lifestyle questionnaires after each sample collection.
The researchers found that microbial diversity changed within two to three days after a substantial head impact. Specifically, certain bacteria – including the order Coriobacteriales, the family Prevotellaceae, and the genus Prevotella – tended to decrease in abundance while the genus Ruminococcus increased. In previous studies, these changes have correlated with brain injury and inflammation.
The athletes’ gut microbiomes also changed significantly over the course of the season, with mathematical modelling suggesting that the cumulative effects of non-concussive head impacts was likely associated with this shift, even after accounting for 15 potentially confounding factors including diet changes, exercise intensity, sleep, and stress.
The study is limited by its small sample size and lack of a control group, with its design meaning findings could only establish correlation but not causation. However, the authors conclude that even sub-symptomatic head impacts might affect the gut microbiome, both in the immediate aftermath of injury and over a longer time course in athletes who experience multiple impacts.
Ken Belanger adds: “As far as we are aware, this is the first study to examine connections between head impacts and the composition of the gut microbiome – the complex community of bacteria and other organisms within the digestive system.”
“Our results provide evidence that even head impacts that do not result in a concussion or other reported symptoms may influence the microbes present within the gut, both in the short- and longer-term. Determining what causes these changes and whether they have a positive or negative influence on recovery from head injury will require further investigation.”
“Our research highlights the importance of thinking integratively about the interactions between the gut and the brain. We are only beginning to scratch the surface in our understanding of how these complex organs and organ systems communicate with and affect each other.”
Aziz Zafar adds: “After having only heard of the complicated interplay between neuronal inflammation and the gut microbiome, I found it to be such an exciting scientific experience to explore that interplay in the context of head impacts.”
Zachary Pelland adds: “It has been an amazing privilege to work so deeply on a personally and scientifically meaningful project which could not have happened without immeasurable support across academic departments, athletics, administration, and alumni at Colgate University.”
Older adults with type 2 diabetes face a difficult trade-off: they are among the most vulnerable to medication-related harms yet are often underrepresented in the clinical trials that guide treatment decisions. A new study led by Yuan Lu, ScD, helps address this gap by providing large-scale, real-world evidence about the safety of commonly used diabetes medications.
Published in Nature Communications, the study analysed data from more than 1.8 million people aged 65 and older across the United States and Europe. The researchers compared four major classes of second-line antihyperglycaemic medications – typically prescribed when first-line therapy such as metformin is not sufficient – across 18 safety outcomes.
“Evidence from clinical trials often does not fully capture older adults,” says Lu, assistant professor of medicine (cardiovascular medicine) at Yale School of Medicine. “They are more likely to experience side effects due to frailty, multiple chronic conditions, and the use of several medications at the same time.”
Newer diabetes drugs show overall safety advantages
The study found a consistent pattern: newer classes of medications, including GLP-1 receptor agonists and SGLT2 inhibitors, were generally associated with lower risks of several important adverse outcomes compared to older drugs such as sulfonylureas and DPP-4 inhibitors.
Newer agents were linked to lower risks of hypoglycaemia, hyperkalaemia, and peripheral oedema – complications that can be especially dangerous in older adults. However, the findings also highlight important trade-offs. For example, SGLT2 inhibitors were associated with a higher risk of diabetic ketoacidosis, while GLP-1 receptor agonists were more likely to cause gastrointestinal side effects such as nausea and vomiting.
Rather than identifying a single “best” medication, Lu emphasises that the results support more informed, individualised decision-making. “Some patients may have a higher risk of hypoglycaemia, while others may be more susceptible to diabetic ketoacidosis,” she says. “These risks need to be considered together as part of an individual patient profile.”
Real-world data at a global scale
A key strength of the study is its scale and approach. The analysis drew on nine large databases and was conducted through the Observational Health Data Sciences and Informatics (OHDSI), an international research network that enables standardized analyses across diverse health care systems.
By using harmonised real-world data and consistent analytic methods, the researchers were able to evaluate a broad range of safety outcomes in routine clinical practice – offering insights that complement and extend findings from randomised trials.
Supporting safer prescribing for an aging population
As the population ages and the use of newer diabetes medications continues to grow, understanding their safety profiles in older adults is increasingly important. The findings reinforce current guideline recommendations that often favour newer agents, while also underscoring the need to tailor treatment decisions to each patient’s risks and preferences.
Like all observational studies, the analysis cannot fully rule out unmeasured differences between patients. Still, the large, multinational design gives a more complete picture of medication safety in a population often underrepresented in clinical research.
Looking ahead, Lu and her colleagues hope to expand this work to examine the comparative safety of individual medications and to evaluate the safety of newer GLP-1 receptor agonists across a wider range of outcomes, including among people with obesity. “By providing more evidence in populations that clinicians see every day, our goal is to support safer, more informed care,” she says.
Few medications can target disordered proteins, but new research outlines an enhanced approach that could lead to treatments for prostate cancer and other diseases
Photo by Louis Reed on Unsplash
Researchers at the University of British Columbia and BC Cancer have developed a new way to target proteins long considered ‘undruggable’, opening the door to new treatments for prostate cancer and other serious diseases.
Known as intrinsically disordered proteins, these molecular shapeshifters are extremely difficult to target with medication due to their flexible and ever-changing structure. They play a central role in a wide range of diseases, including cancer, neurodegenerative disorders, heart disease and autoimmune conditions, yet only a handful of medications currently exist that can target them.
In a study published today in Nature Signal Transduction and Targeted Therapy, the researchers demonstrate a new approach for designing drugs that bind more strongly to these proteins and block their disease-causing activity. In some cases, the compounds they developed bound up to a million times more tightly than any previously reported.
“This study shows that proteins previously thought to be undruggable can be drugged with remarkable efficacy,” said principal investigator Dr Marianne D. Sadar, professor of pathology and laboratory medicine at the UBC faculty of medicine and distinguished scientist at BC Cancer. “The findings could have profound implications for the treatment of cancer and other diseases, providing a roadmap for the development of new treatments.”
A long-standing challenge in drug discovery
Unlike most proteins, which fold into stable three-dimensional shapes, disordered proteins contain flexible regions that change as they interact with molecules inside cells. Because they lack fixed binding sites, they are extremely difficult to target with traditional drugs.
“Most drug discovery is like designing a key for a very specific lock,” said Dr Sadar. “But disordered proteins don’t behave like locks at all, they’re more like moving strands of spaghetti.”
Dr Sadar and her team have spent decades studying how to target these proteins. In 2008, they developed the first compound capable of binding to them, and have since advanced two such drugs into clinical trials – another world-first milestone for the field.
Despite these advances, achieving strong and consistent binding has remained a central challenge.
A new strategy against prostate cancer
The new study focused on a specific protein, the androgen receptor, which fuels the growth of most prostate cancers.
Rather than fitting into a single fixed spot, the researchers developed compounds that interact with the moving region of the protein, freeze it in an inactive state, and prevent it from turning on genes that drive cancer growth.
“It’s a major achievement. Our target drugs had binding affinity a million times greater than existing drugs targeting these regions,” said Dr Natalie Strynadka, professor of biochemistry and molecular biology at the UBC faculty of medicine.
By systematically modifying the compounds at the molecular level, the researchers identified several promising candidates that effectively shut down the receptor. In animal studies, several compounds slowed prostate cancer growth more effectively than a commonly used prostate cancer treatment.
“What surprised us was how effectively these molecules could attach to a protein that doesn’t have a fixed structure,” said Dr Raymond Andersen, professor in UBC’s department of chemistry. “We were able to shut down the androgen receptor even in situations where current prostate cancer drugs stop working.”
The researchers now aim to advance the most promising candidates toward clinical trials, with the goal of developing prostate cancer drugs that can be used earlier in treatment and with fewer side-effects. Because disordered proteins are involved in many diseases, they say the approach could have a much broader impact.
“If the approach continues to prove successful, it could dramatically expand the number of proteins that scientists can target with medicines – turning what was once considered a dead end into a promising new frontier for drug discovery,” said Dr Sadar.
Colourised transmission electron micrograph of an HIV-1 virus particle (yellow/gold) budding from the plasma membrane of an infected H9 T cell (purple/green).
Researchers at Karolinska Institutet, in collaboration with colleagues at The Scripps Research Institute and Emory University, have developed a new vaccine strategy that has generated antibodies capable of neutralising highly divergent HIV variants. The study, published in the journal Nature, provides new insights into how the immune system can be guided towards a particularly protected part of the virus.
HIV mutates rapidly, making it difficult to develop an effective vaccine. One major challenge has been to stimulate the immune system to produce so‑called broadly neutralising antibodies that recognise parts of the virus shared by many HIV variants.
In the study, the researchers focused on a small structure located at the very top of the virus’s surface protein, known as the apex, which is important for the protein’s three-dimensional structure. The apex is similar across many HIV variants but is shielded by dense layers of sugar molecules, making such binding difficult to achieve.
“We developed a strategy in which specially designed HIV proteins were attached to tiny fat particles, known as liposomes. This enabled multiple copies of the virus’s surface protein to be presented to the immune system simultaneously, thereby strengthening the immune response”, says Mónika Ádori, researcher at Department of Microbiology, Tumor and Cell Biology, Karolinska Institutet.
The vaccine strategy was tested in an animal model in which macaques were immunised with liposomes linked to a selected HIV protein and then given booster doses in which the protein was gradually altered. The aim was to train the immune system to recognise features that are shared across different HIV variants.
Resembles antibodies that develop in humans
With this strategy, all vaccinated animals developed antibodies that neutralised a wide range of HIV variants. When the researchers analysed the antibodies in more detail, they found that they bind to the virus’s apex in a way similar to antibodies that sometimes develop in humans after long‑term HIV infection.
“The study shows that it is possible, through vaccination, to steer the immune system towards this specific part of the HIV surface protein,” says Gunilla Karlsson Hedestam, professor at the Department of Microbiology, Tumour and Cell Biology at Karolinska Institutet and a shared senior author of the study.
“This is an important step towards understanding how an HIV vaccine could be designed. Discussions are now underway about how the strategy could be taken forward into clinical studies,” she continues.
The study was funded by the US National Institutes of Health (NIH). The researchers report no conflicts of interest.
Publication
”Vaccine generates broadly cross-neautralizing antibodies to the HIV Env apex“, Javier Guenaga, Monika Adori, Shridhar Bale, Swastik Phulera, Ioannis Zygouras, Fabian-Alexander Schleich, Xaquin Castro Dopico, Sashank Agrawal, Miyo Ota, Richard Wilson, Jocelyn Cluff, Tamar Dzvelaia, Marco Mandolesi, Wen-Hsin Lee, Agnes A. Walsh, Mariane B. Melo, Laurent Verkoczy, Darrell J. Irvine, Martin Corcoran, Ian A. Wilson, Diane Carnathan, Guido Silvestri, Andrew B. Ward, Gabriel Ozorowski, Gunilla B. Karlsson Hedestam, Richard T. Wyatt, Nature, online 29 April, doi: 10.1038/s41586-026-10429-3
Study from Japan finds rising rates, especially after breast cancer treatment
Photo by Tima Miroshnichenko on Pexels
Some therapies used to treat cancer may increase the risk of later developing cancers that affect the blood. A population-based study in Japan has revealed a gradual increase in the rates of therapy-related acute myeloid leukaemia (tAML) in recent years, especially after breast cancer treatment. The findings are published by Wiley online in CANCER, a peer-reviewed journal of the American Cancer Society.
tAML is an aggressive cancer of the blood and bone marrow that develops after prior chemotherapy or radiation for an earlier, primary cancer, likely arising in part due to DNA damage from these treatments. To assess whether tAML is increasing as a post-cancer therapy complication as the number of cancer survivors increases, investigators analysed data from the Osaka Cancer Registry pertaining to patients in Japan who were diagnosed with AML between 1990 and 2020.
Among 9,841 patients with AML, 636 (6.5%) had tAML. The annual tAML incidence increased from 0.13 per 100,000 population in 1990 to 0.36 per 100,000 population in 2020. The proportion of tAML cases in overall AML cases almost doubled.
The most common primary cancer that was treated before tAML developed was another form of blood cancer (23.1%), followed by breast cancer (14.6%), colorectal cancer (11.5%), and gastric cancer (8.7%). The distribution of primary cancers changed over time, with a prominent increase in breast cancer and a decrease in gastric cancer.
“The study provides an important step towards better understanding how the nature of tAML is changing with the increasing number of cancer survivors,” said lead author Kenji Kishimoto, MD, PhD, of the Osaka International Cancer Institute.
Anxiety itself is not a mental illness. It’s a normal, adaptive emotion that helps us respond to perceived threats.
Anxiety is the automatic reaction that makes you jump back when you think you’ve seen a snake while bushwalking – before realising it’s a stick.
It’s also (inconveniently) the sweaty palms and shaky voice you notice before a presentation or a first date, or the circling thoughts that keep you awake at 3am.
Most of us have ways to cope with anxious thoughts and feelings that can give us more of a sense of control. This could be checking and double-checking we’ve got the room right for our presentation, or seeking reassurance from someone we love.
But when might these behaviours fit a diagnosis of an anxiety disorder? And when could they actually be a sign of obsessive compulsive disorder (OCD)?
As clinical psychologists, we find these questions come up a lot, perhaps spurred by a recent surge of interest in OCD on social media. So what’s the difference between anxiety and OCD? And how are they treated?
Social media is full of content ‘diagnosing’ OCD and explaining how it’s different to anxiety. TikTok
When is anxiety something more serious?
“Normal” anxiety can become an anxiety disorder when fears or worry are persistent, intense and start interfering with everyday life.
About one in three people will experience an anxiety disorder at some point in their lifetime.
These disorders have slightly different symptoms. But all share excessive and persistent fear or worry that causes distress or leads people to avoid important parts of life including work, study or social activities.
So, what about OCD?
Although OCD involves anxiety, it is actually considered a separate disorder in the diagnostic manual used by mental health professionals.
It is possible to have both – around half to three-quarters of individuals with OCD also meet criteria for one or more anxiety disorders as well.
OCD involves obsessions, compulsions, or both. These cause significant distress or interfere with daily functioning.
Obsessions are intrusive, unwanted thoughts, images or urges. This could mean an intense fear your food is contaminated, suddenly visualising hurting someone, or a feeling that keeps entering your mind that you’ve made a serious mistake.
Compulsions are the repetitive behaviours (or mental rituals) people feel driven to perform to ease that distress, such as checking, repeating phrases, excessive hand-washing or seeking reassurance.
Many of us will occasionally experience unwanted thoughts or go back to check the oven is actually off. Keeping things tidy or being particular about routines can simply be habits that don’t cause distress.
But what makes OCD different is its severity and impact.
If obsessions or compulsions take up large amounts of time, cause you significant distress, or interfere with daily life, it may be a sign of OCD.
You can’t “spot” OCD from behaviour alone. OCD can also be invisible because many compulsions happen mentally, such as repeating phrases or counting. People with OCD may also try to hide their symptoms out of shame.
Are OCD and anxiety treated differently?
While anxiety disorders and OCD share some similarities, including repetitive distressing thoughts, the patterns and beliefs driving them are different. This means the way they’re treated will also differ.
Cognitive behavioural therapy (CBT) is one of the most effective treatments for both anxiety disorders and OCD.
For OCD, treatment often involves a specialised form of CBT called exposure and response prevention (ERP). It involves gradually facing situations that trigger distressing thoughts while resisting the urge to perform compulsions.
For example, someone with contamination fears might gradually reduce the number of times they wash their hands before eating. Over time, people learn the feared outcome does not occur, that they can tolerate their discomfort without the ritual, and that the anxiety passes on its own.
Treatment for anxiety disorders focuses on the specific fear. For generalised anxiety, for example, it involves understanding patterns of worry, challenging beliefs that keep worries going, and developing more helpful ways to respond to problems, such as brainstorming solutions and taking small actions.
Antidepressant medication (particularly selective serotonin re-uptake inhibitors, or SSRIs) can be an effective component of treatment for both anxiety disorders and OCD. A combined treatment approach of medication (SSRIs) and therapy (CBT) often leads to the best treatment outcomes, especially for severe OCD.
A final note
While it’s great mental health is being discussed more openly online and stigma is reducing, social media can also blur the line between personal experience and evidence-based information.
If something you’ve seen online has sparked curiosity about your mental health, the best next step is to talk with a qualified professional who can help you understand what you’re experiencing and what support might help.
There are lots of evidence-based online treatment programs for anxiety disorders and OCD you can access for free or low-cost, such as This Way Up, MyNewWay or Mindspot.
There are also online treatments for kids and teens with OCD and anxiety.
You can also ask your GP about a Mental Health Care Plan for Medicare-rebated psychology sessions.
Poorer mental health was associated with worse reported care and less trust in the healthcare system
Photo by Alex Green on Pexels
People with self-reported poorer mental health also report worse quality of care and lower confidence in healthcare systems, according to a study published May 5th in the open-access journal PLOS Medicine by Margaret E. Kruk from Washington University in St. Louis, U.S., and colleagues.
Rates of depression and anxiety have increased worldwide since the COVID-19 pandemic, and more people are pursuing mental health treatment as a result. However, there is limited up-to-date data describing how these individuals seek out and receive care. Detailed, population-level information can help healthcare systems meet this growing population’s needs.
To make a start on gathering this data, Kruk and her colleagues surveyed 32 419 adults in 18 high-, low-, and medium-income countries. More than 1000 people from each country responded. Participants self-reported data via the People’s Voice Survey in 2022 and 2023.
First, survey respondents self-assessed their physical and mental health (the latter including “poor,” “fair,” “good,” “very good,” and “excellent”). Then, they quantified their overall confidence in the healthcare system, their own use of healthcare services, the typical quality of care received, and their ability to manage their own mental health (a metric called patient activation).
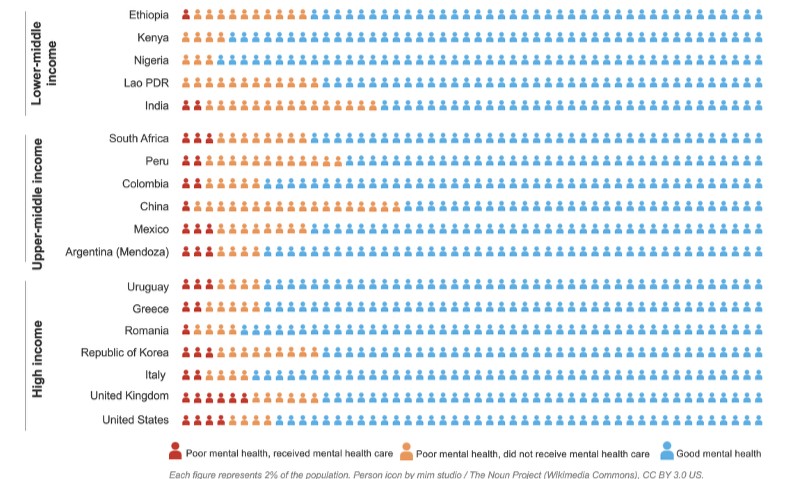
Mental healthcare receipt among people with poor mental health. Infographic displaying the weighted distribution of mental health status and care receipt. Each figure icon represents 2% of the population. Dark orange = respondents with poor/fair mental health who received mental healthcare in the past 12 months; light orange = those with poor/fair mental health who did not receive care; blue = those with good/very good/excellent mental health.
Across all countries, respondents reporting poor mental health were more likely to report chronic illness, poorer overall health, lower patient activation, worse care quality and lower confidence in the healthcare system. Between 0.9% (Lao PDR) and 52.4% (UK) of these respondents reported receiving mental health care in the last year. Respondents in Nigeria reported the best overall mental health (4.7% people reported the lowest proportion of “poor” or “fair” mental health (4.7%), while respondents in China had the highest proportion (39.6%).
The researchers hope these results can help the countries in question – and individual healthcare systems – better serve the needs of those with poor mental health. While this is a descriptive study, the researchers posit patient activation as a potential target for elevating overall health and wellness.
The authors acknowledge that big-picture data doesn’t describe individuals’ specific experiences within the healthcare system. They suggest comparison across similar health systems and tracking system performance over time to continuously improve health services.
The authors add, “What stands out from this study is that poor mental health doesn’t exist in isolation. People reporting poor mental health were nearly twice as likely to have a chronic illness and far less likely to feel empowered to manage their own health. Health systems need to stop treating mental health in a silo and recognise that these patients are showing up across all areas of care – and often with more complex needs.”
Kruk adds, “As a research consortium working across very different health systems, we expected to find variation, and we did, in treatment access. But the experience gap was remarkably consistent: people with poor mental health had worse care, more unmet needs, and less trust in the system, regardless of where they lived. Health systems globally need to rethink how they serve this growing group, not just whether they can reach them.”