Houston Methodist researchers find antibiotics aid recovery from traumatic brain injury
Coup and contrecoup brain injury. Credit: Scientific Animations CC4.0
In a new study published in Nature Communications Biology, Houston Methodist researchers led by Sonia Villapol, PhD, found that short-term antibiotic treatment significantly reduced neuroinflammation and neurodegeneration following traumatic brain injury (TBI) by altering the gut microbiome in animal models.
“We found that antibiotic treatment following TBI can reduce harmful gut bacteria, decrease lesion size and limit cell death,” said Villapol, an associate professor in the Department of Neurosurgery at Houston Methodist. “Our results support a gut–brain mechanism in which microbiome changes influence peripheral immunity and, in turn, neuroinflammation after TBI.”
Administering antibiotics cleans the gut of harmful bacteria, allowing beneficial bacteria to flourish. The study found that two helpful bacteria, Parasutterella excrementihominis and Lactobacillus johnsonii, are key to driving cell repair. According to Villapol, they could also be major regulators for peripheral inflammation in the body.
Notably, 70% of immune system regulation is generated by the gut microbiome. During gut imbalance, the bidirectional nature of the brain-gut axis can wreak havoc throughout the entire body.
“Our brains are constantly sending signals to the rest of our bodies. Following a traumatic brain event, those signals can get scrambled and disrupt other organs, including our digestive system,” Villapol said. “If the gut stays out of balance, the brain may have a harder time healing.”
There are an estimated 4 million traumatic brain injuries a year in the U.S. Recent studies indicate that TBI-induced gut microbiome imbalance may even contribute to the development of neurodegenerative diseases like Parkinson’s, Alzheimer’s and dementia.
Villapol’s lab is focused on investigating and developing new neuroprotective treatments to fight inflammation linked with neurodegenerative disease. “If we can break neuroinflammation in the acute or chronic stage, we can reduce the risk of developing Alzheimer’s or dementia,” said Villapol.
The next phase of the research will focus on bioengineering Parasutterella excrementihominis and Lactobacillus johnsonii to further develop precision therapies to reduce neuroinflammation.
Houston Methodist researchers find antibiotics aid recovery from traumatic brain injury
Source: CC0
What if healing the brain after traumatic injury starts in the gut? In a new study published in Nature Communications Biology, Houston Methodist researchers led by Sonia Villapol, PhD, found that short-term antibiotic treatment significantly reduced neuroinflammation and neurodegeneration following traumatic brain injury (TBI) by altering the gut microbiome in animal models.
“We found that antibiotic treatment following TBI can reduce harmful gut bacteria, decrease lesion size and limit cell death,” said Villapol, an associate professor in the Department of Neurosurgery at Houston Methodist. “Our results support a gut–brain mechanism in which microbiome changes influence peripheral immunity and, in turn, neuroinflammation after TBI.¨
Administering antibiotics cleans the gut of harmful bacteria, allowing beneficial bacteria to flourish. The study found that two helpful bacteria, Parasutterella excrementihominis and Lactobacillus johnsonii, are key to driving cell repair. According to Villapol, they could also be major regulators for peripheral inflammation in the body.
Notably, 70% of immune system regulation is generated by the gut microbiome. During gut imbalance, the bidirectional nature of the brain-gut axis can wreak havoc throughout the entire body.
“Our brains are constantly sending signals to the rest of our bodies. Following a traumatic brain event, those signals can get scrambled and disrupt other organs, including our digestive system,” Villapol said. “If the gut stays out of balance, the brain may have a harder time healing.”
Recent studies indicate that TBI-induced gut microbiome imbalance may even contribute to the development of neurodegenerative diseases like Parkinson’s, Alzheimer’s and dementia.
Villapol’s lab is focused on investigating and developing new neuroprotective treatments to fight inflammation linked with neurodegenerative disease. “If we can break neuroinflammation in the acute or chronic stage, we can reduce the risk of developing Alzheimer’s or dementia,” said Villapol.
The next phase of the research will focus on bioengineering P. excrementihominis and L. johnsonii to further develop precision therapies to reduce neuroinflammation.
Taking certain antidepressants at the time of a traumatic brain injury (TBI) is not associated with an increased risk of death, brain surgery or longer hospital stays, according to a study published on January 28, 2026, in Neurology®, the medical journal of the American Academy of Neurology.
For the study, researchers looked at serotonergic antidepressants, which treat anxiety and depression by increasing serotonin activity in the brain. These included selective serotonin reuptake inhibitors (SSRIs), serotonin and norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs).
“Concerns have previously been raised that serotonergic antidepressants might increase the risk of bleeding in the brain or complicate early recovery after traumatic brain injury,” said study author Jussi P. Posti, MD, PhD, of the University of Turku in Finland. “However, our study found no evidence to support those concerns.” The study included 54 876 people in Finland who were 16 or older when hospitalised with a TBI. A total of 14% used serotonergic antidepressants at the time of the TBI.
Researchers reviewed national prescription records for preinjury antidepressant use and medical records to determine how many people died within a month, whether they needed emergency brain surgery, and how long they stayed in the hospital. A total of 4105 people died within a month. This included 7.6% of those taking antidepressants and 7.5% of people who did not. After adjusting for factors such as age, sex and other health conditions, researchers found people taking antidepressants before injury were no more likely to die within a month than those not taking them.
Antidepressant users were slightly less likely to require emergency brain surgery to relieve pressure or bleeding in the brain and prevent further damage. Of the total participants, 6.8% of the antidepressant users and 8.6% of those who did not use antidepressants needed emergency brain surgery. After adjustments, antidepressant users had an 11% lower risk. The amount of time in the hospital was the same for both groups.
“These findings provide reassurance for people who take antidepressants that antidepressant use does not appear to worsen early recovery after traumatic brain injury,” said Posti. “Future studies should examine whether these results hold true for long-term recovery and across different health care settings.”
A limitation of the study was that it was conducted only at hospitals and health care centres in Finland, so results may vary in other areas. The study was supported by the Finnish government, the Paulo Foundation, Paavo Nurmi Foundation, Research Council of Finland, Sigrid Jusélius Foundation and Finnish Foundation for Cardiovascular Research.
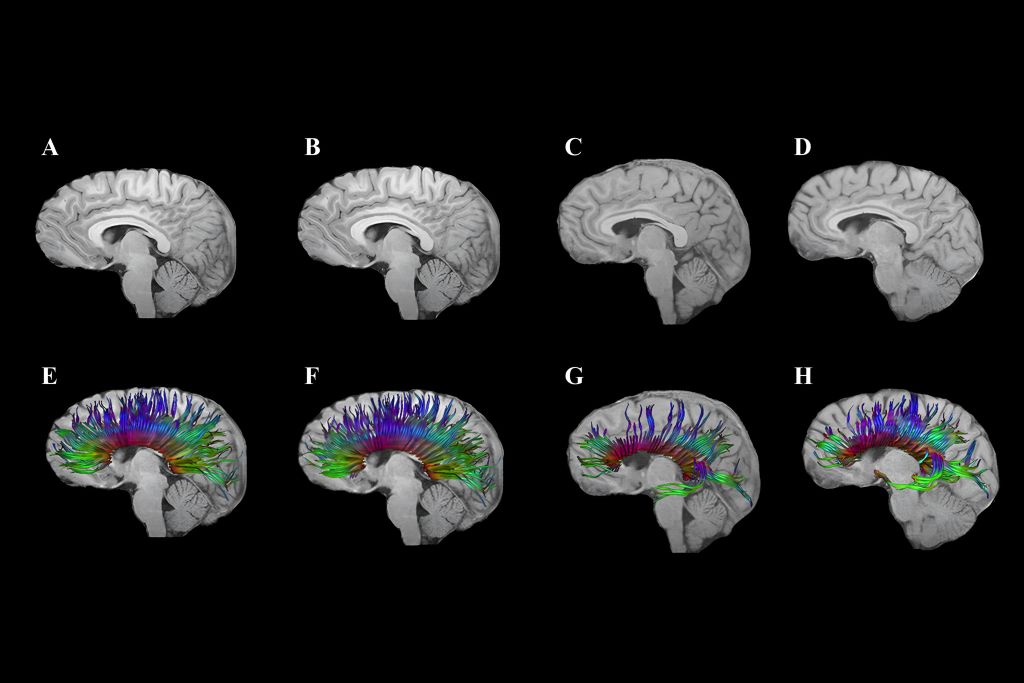
Diffusion tensor imaging shows corpus callosum fibre tracts in two adolescents: One with traumatic brain injury (TBI; G and H) and one with an orthopaedic injury (E and F). At 3 months post-injury (E, G), early degeneration and loss of fibre tracts are visible, especially in the TBI case. At 18 months (F, H), some recovery or reorganisation occurs, but persistent loss and thinning of tracts remain, particularly in the frontal regions, indicating lasting white matter damage after TBI.
By Kathy Malherbe
A silent but devastating brain disease is casting a shadow over contact and collision sports, particularly rugby. Traumatic Brain injuries (TBIs) as a result of an impact to the head, cause a disruption in the normal function of the brain. Repeated TBIs are linked to an increased risk of neurodegenerative diseases like early-onset dementia which has the highest prevalence and is the most concerning. Others include Parkinson’s disease, Alzheimer’s and Chronic Traumatic Encephalopathy, better known as CTE.
How head injuries happen
Dr Hofmeyr Viljoen, radiologist at SCP Radiology, says that there are several types of head injuries common in rugby. ‘The most frequent being TBIs which occur when the impact and sudden movement results in the brain shifting rotationally, sideways or backwards and forwards within the skull. This stretching and elongation causes damage to nerve fibres as well as blood vessels. Surprisingly, a direct blow isn’t always necessary. Rapid acceleration and deceleration, such as during a tackle or fall, can also result in an injury. More severe head injuries may include skull fractures, bruising or bleeding around the brain, all of which require urgent diagnosis and intervention.’
Riaan van Tonder, a sports physician with a special interest in sports-related concussion and radiology registrar at Stellenbosch University, explains that concussions and, even more so, repetitive sub-concussive impacts, result in a cascade of changes at a cellular level, gradually damaging the nervous system.
Although rugby is notorious for heavy tackles and collisions, it took a lawsuit to prompt more widespread awareness. A class-action suit filed in the High Court in London, by former union and league players, accused World Rugby of failing to implement adequate rules to assess, diagnose and manage concussions. Steve Thompson’s, the legendary English hookers, early onset dementia has been one of the sports’ biggest talking points. He was diagnosed in 2020 with this neurodegenerative disease, purportedly as a result of repeated trauma to the brain. The claimants argue that the governing bodies were negligent and that their neurological problems stem from years of unmanaged head injuries. The outcome of this case to be heard in 2025, could significantly reshape the legal and medical responsibilities of sports organisations globally.
What is Chronic Traumatic Encephalopathy (CTE)
CTE is a progressive neurodegenerative condition strongly linked to repeated head impacts. It has been implicated in memory loss, mood disturbances, psychosis and, in many cases, premature death. It can only be diagnosed after death at autopsy, where researchers examine brain tissue for abnormal protein deposits and signs of widespread degeneration. Despite this limitation, mounting evidence is forcing sports organisations, including rugby authorities, to confront uncomfortable truths about how repeated head trauma can alter lives permanently.
Uncovering the extent of the problem
In 2023, the Boston University CTE Centre released updated autopsy findings from its brain bank. Of 376 former NFL player’s brains studied post-mortem, 345 had been diagnosed with CTE, a staggering 91.7%. While brain banks are inherently subject to selection bias, the results remain alarming. For comparison, a 2018 study of 164 randomly selected brains revealed just one case of CTE.
This brain disease isn’t new. Its earliest descriptions date back to Dr Harrison Martland in 1928, who studied post-mortem findings in boxers and coined the term ‘punch drunk’ to describe their confusion, tremors and cognitive decline. What was once confined to boxing is now known to affect athletes in rugby, football, ice hockey and even military personnel exposed to repeated blast injuries.
Radiology’s role in determining head injuries
Although Computed Tomography (CT) scans are not designed to specifically diagnose concussions, they are crucial to imaging patients with severe concussion or atypical symptoms. ‘CT scans rapidly detect serious issues like fractures, brain swelling and bleeding, providing crucial information for urgent treatment decisions,’ explains Dr Viljoen.
‘Magnetic Resonance Imaging (MRI) is used particularly when concussion symptoms persist or worsen. It excels in identifying subtle injuries, such as microbleeds and brain swelling that may have been missed by CT scans,’ he says.
‘CTE is challenging because currently, it can only be definitively diagnosed after death,’ he explains. ‘However, ongoing research aims to develop methods to detect CTE in living patients, potentially using advanced imaging techniques like Positron Emission Tomography (PET).’ Most research is focused on advancing non-invasive methods to see what is happening inside the brain of a living person and to track it over time.
Advanced imaging methods
Emerging imaging techniques, such as Diffusion Tensor Imaging (DTI), show promise for better understanding and management of head injuries, especially the subtle effects of concussions. ‘DTI helps identify damage to the brain’s white matter, potentially guiding return-to-play decisions and treatment strategies,’ notes Dr Viljoen.
The biomechanics of brain trauma
Former NFL player and biomechanical engineer, David Camarillo, explains in a TED talk that helmets, although effective at preventing skull fractures, do little to stop biomechanical forces from affecting the brain inside the skull.
Camarillo highlights that concussions and the stretching of nerve fibres are more likely to affect the middle of the brain, the corpus callosum, the thick band that facilitates communication between the left and right brain hemispheres. ’It’s not just bruising,’ he says, ‘we’re talking about dying brain tissue.’
Smart mouthguard technology in rugby
‘Presently,’ says Van Tonder, ‘smart mouthguards are mandatory at elite level. These custom-fitted mouthguards contain accelerometers and gyroscopes that detect straight and rotational forces on the head. Data is transmitted live to medical teams at a rate of 1 000 samples per second.
‘If a threshold is exceeded, an alert is triggered, prompting an immediate Head Injury Assessment (HIA1). Crucially, the system can identify dangerous impacts, even when no symptoms or video evidence is apparent. This is an essential shift in concussion management,’ says van Tonder. ‘It allows proactive assessments rather than waiting for visible signs.’ World Rugby has committed €2 million to assist teams in adopting this technology and integrating it into HIA1.
Brain Health Service
The really good news is that in March this year, World Rugby and SA Rugby launched a new Brain Health Service to support former elite South African players. It’s the first of its kind in the world and South Africa is the fourth nation to establish this system that supports players to understand how they can optimise management of their long-term brain health. It includes an awareness and education component, an online questionnaire and tele-health delivered cognitive assessment with a trained brain health practitioner. This service assesses players for any brain health warning signs, provides a baseline result, advice on managing risk factors and signposts anyone in need of specialist care.
Super Rugby and smart mouthguards
Super Rugby has revised its smart mouthguard policy, no longer requiring players to leave the field immediately for a HIA when an alert is triggered. The change follows criticism from players and coaches, including Crusaders captain Scott Barrett, who argued the rule could unfairly affect match outcomes. Players must still wear the devices but on-field doctors will assess them first; full HIAs will be conducted at half-time or full-time, if necessary. Further trials are planned to improve the system before reinstating immediate alerts.
Where to from here?
Researchers continue to explore ways to reduce brain movement inside the skull during collisions. One innovative idea includes an airbag neck collar for cyclists, which inflates around the head upon impact. It’s closer to the goal of reducing the brain’s movement – and therefore the risk of concussion. However, regulatory hesitation remains a barrier, with no formal cycling helmet approval process currently in place.
The evidence linking repetitive head impacts to long-term brain degeneration is too compelling to ignore. Rugby, like other contact sports, must continue evolving its protocols, technology and player education to protect athletes at all levels … starting at schools.
While innovations such as smart mouthguards mark significant progress, much remains to be done: From regulatory reform to changing the sporting culture that once downplayed the severity of concussion. Van Tonder notes, ‘We’re behind, but it’s not too late to catch up.’
In rugby, the HIA protocol now consists of three stages:
HIA1: Immediate, sideline assessment during the match.
HIA2: Same-day evaluation within three hours post-match.
HIA3: A more detailed follow-up, typically done 36-48 hours later.
Trauma centres in the United States will begin to test a new approach for assessing traumatic brain injury (TBI) that is expected to lead to more accurate diagnoses and more appropriate treatment and follow-up for patients.
The new framework, which was developed by a coalition of experts and patients from 14 countries and spearheaded by the National Institutes of Health (NIH), expands the assessment beyond immediate clinical symptoms. Added criteria would include biomarkers, CT and MRI scans, and factors such as other medical conditions and how the trauma occurred.
For 51 years, trauma centres have used the Glasgow Coma Scale to assess patients with TBI, roughly dividing them into mild, moderate, and severe categories, based solely on their level of consciousness and a handful of other clinical symptoms.
That diagnosis determined the level of care patients received in the emergency department and afterward. For severe cases, it also influenced the guidance doctors gave the patients’ families, including recommendations around the removal of life support. Yet, doctors have long understood that those tests did not tell the whole story.
“There are patients diagnosed with concussion whose symptoms are dismissed and receive no follow-up because it’s ‘only’ concussion, and they go on to live with debilitating symptoms that destroy their quality of life,” said corresponding author Geoffrey Manley, MD, PhD, professor of neurosurgery at UC San Francisco and a member of the UCSF Weill Institute for Neurosciences. “On the other hand, there are patients diagnosed with ‘severe TBI’ who were eventually able to live full lives after their families were asked to consider removing life-sustaining treatment.”
In the US, TBI resulted in approximately 70 000 deaths in 2021 and accounts for about half-a-million permanent disabilities each year. Motor vehicle accidents, falls, and assault are the most common causes.
New system will better match patients to treatments
Known as CBI-M, the framework comprises four pillars – clinical, biomarker, imaging, and modifiers – that were developed by working groups of federal partners, TBI experts, scientists, and patients.
“The proposed framework marks a major step forward,” said co-senior author Michael McCrea, PhD, professor of neurosurgery and co-director of the Center for Neurotrauma Research at the Medical College of Wisconsin in Milwaukee. “We will be much better equipped to match patients to treatments that give them the best chance of survival, recovery, and return to normal life function.”
The framework was led by the NIH National Institute of Neurological Disorders and Stroke (NIH-NINDS), for which Manley, McCrea, and their co-first and co-senior authors are members of the steering committee on improving TBI characterisation.
The clinical pillar retains the Glasgow Coma Scale’s total score as a central element of the assessment, measuring consciousness and pupil reactivity as an indication of brain function. The framework recommends including the scale’s responses to eye, verbal, and motor commands or stimuli, presence of amnesia, and symptoms like headache, dizziness, and noise sensitivity.
“This pillar should be assessed as first priority in all patients,” said co-senior author Andrew Maas, MD, PhD, emeritus professor of neurosurgery at the Antwerp University Hospital and University of Antwerp, Belgium. “Research has shown that the elements of this pillar are highly predictive of injury severity and patient outcome.”
Biomarkers, imaging, modifiers offer critical clues to recovery
The second pillar uses biomarkers identified in blood tests to provide objective indicators of tissue damage, overcoming the limitations of clinical assessment that may inadvertently include symptoms unrelated to TBI.
Significantly, low levels of these biomarkers determine which patients do not require CT scans, reducing unnecessary radiation exposure and health care costs. These patients can then be discharged. In those with more severe injuries, CT and MRI imaging – the framework’s third pillar – are important in identifying blood clots, bleeding, and lesions that point to present and future symptoms.
In sports, the connection between head injuries and neurodegenerative diseases such as chronic traumatic encephalopathy, Alzheimer’s disease, and Parkinson’s disease is now well recognised.
Researchers at Tufts University and Oxford University have now uncovered mechanisms that may connect the dots between trauma events and the emergence of disease. They point to latent viruses lurking in most of our brains that may be activated by the jolt, leading to inflammation and accumulating damage that can occur over the ensuing months and years.
The results suggest the use of antiviral drugs as potential early preventive treatments post-head injury. The findings are published in a study in Science Signaling.
The microbiome aids in digestion, immune system development, and protection against harmful pathogens.
But the microbiome also includes dozens of viruses that swarm within our bodies at any given time. Some of these can be potentially harmful, but simply lie dormant within our cells. Herpes simplex virus 1 (HSV-1), found in over 80% of people, and varicella-zoster virus, found in 95% of people, are known to make their way into the brain and sleep within our neurons and glial cells.
Dana Cairns, GBS12, research associate in the Department of Biomedical Engineering and lead author of the study, had found evidence in earlier studies suggesting that activation of HSV-1 from its dormant state triggers the signature symptoms of Alzheimer’s disease in lab models of brain tissue: amyloid plaques, neuronal loss, inflammations, and diminished neural network functionality.
“In that study, another virus – varicella – created the inflammatory conditions that activated HSV-1,” said Cairns. “We thought, what would happen if we subjected the brain tissue model to a physical disruption, something akin to a concussion? Would HSV-1 wake up and start the process of neurodegeneration?”
The link between HSV-1 and Alzheimer’s disease was first suggested by co-author Ruth Itzhaki, visiting professorial fellow at Oxford University, who more than 30 years ago identified the virus in a high proportion of brains from the elderly population. Her subsequent studies suggested that the virus can be reactivated in the brain from a latent state by events such as stress or immunosuppression, ultimately leading to neuronal damage.
Blows to Brain-like Tissue
In the current study, the researchers used a lab model that reconstructs the environment of the brain to better understand how concussions may set off the first stages of virus reactivation and neurodegeneration.
The brain tissue model consists of a 6mm-wide donut-shaped sponge-like material made of silk protein and collagen suffused with neural stem cells, which are then coaxed into mature neurons, growing axons and dendrite extensions and forming a network. Glial cells also emerge from the stem cells to help mimic the brain environment and nurture the neurons.
The neurons communicate with each other through their extensions similarly to how they would communicate in a brain. And just like cells in the brain, they can carry within them the DNA of dormant HSV-1 virus.
After enclosing the brain-like tissue in a cylinder and giving it a sudden jolt atop a piston, mimicking a concussion, Cairns examined the tissue under the microscope over time. Some of the tissue models had neurons with HSV-1, and some were virus-free.
Following the controlled blows, she observed that the infected cells showed re-activation of the virus, and shortly after that the signature markers of Alzheimer’s disease, including amyloid plaques, p-tau (a protein that creates fiber-like “tangles” in the brain), inflammation, dying neurons, and a proliferation of glial cells called gliosis.
More strikes with the pistons on the tissue models mimicking repetitive head injuries led to the same reactions, which were even more severe. Meanwhile, the cells without HSV-1 showed some gliosis, but none of the other markers of Alzheimer’s disease.
The results were a strong indicator that athletes suffering concussions could be triggering reactivation of latent infections in the brain that can lead to Alzheimer’s disease. Epidemiological studies have shown that multiple blows to the head can lead to doubling or even greater chances of having a neurodegenerative condition months or years down the line.
“This opens the question as to whether antiviral drugs or anti-inflammatory agents might be useful as early preventive treatments after head trauma to stop HSV-1 activation in its tracks, and lower the risk of Alzheimer’s disease,” said Cairns.
The problem goes far beyond the concerns for athletes. Traumatic brain injury is one of the most common causes of disability and death in adults, affecting about 69 million people worldwide each year, at an economic cost estimated at $400 billion annually.
“The brain tissue model takes us to another level in investigating these connections between injury, infection, and Alzheimer’s disease,” said David Kaplan, Stern Family Endowed Professor of Engineering at Tufts.
“We can re-create normal tissue environments that look like the inside of a brain, track viruses, plaques, proteins, genetic activity, inflammation and even measure the level of signalling between neurons,” he said. “There is a lot of epidemiological evidence about environmental and other links to the risk of Alzheimer’s. The tissue model will help us put that information on a mechanistic footing and provide a starting point for testing new drugs.”
The rugby season is kicking off in schools across South Africa and players, parents, coaches and referees are preparing for exciting, yet physically demanding matches. In many sports, injuries are an unfortunate, common occurrence. Rugby, inherently a contact sport, also carries the inevitable risk of head injuries, ranging from minor concussions to severe Traumatic Brain Injuries (TBIs).
The importance of early detection
The early detection of head injuries is essential for effective treatment and preventing further complications. In many cases, the symptoms of a concussion or TBIs may not be immediately apparent and athletes may continue playing which can lead to further damage.
Accurate diagnosis and management of head injuries require a combination of clinical evaluation and advanced imaging techniques. Dr Hofmeyr Viljoen, radiologist at SCP Radiology talks about the nature of these injuries, the critical role radiology plays in diagnosing and managing them and what preventative measures can be taken.
Understanding head injuries in rugby
Dr Viljoen explains that there are several types of head injuries common in rugby. ‘The most frequent is concussion, a mild traumatic brain injury occurring when the brain is jolted inside the skull from an impact or violent movement. Concussions can be mild or lead to significant short and long-term issues. Occasionally, with more severe injuries we see skull fractures, contusions and haemorrhage surrounding the brain. These require urgent diagnosis and management.’
Recognising the symptoms
He emphasises awareness of concussion symptoms, including headaches, dizziness, nausea, confusion, memory problems, sensitivity to light and difficulty concentrating. ‘Immediate recognition is vital,’ he explains. ‘A player with any of these symptoms must be removed from play immediately to prevent further injury.’
The role of radiology
Radiology plays an essential part in accurately diagnosing the extent of head injuries. According to Dr Viljoen, Computed Tomography (CT) scans are always the first imaging method used in emergency settings. Although patients with concussion typically do not have significant imaging findings, it is crucial to image those patients with severe concussion or atypical symptoms. ‘CT scans rapidly detect serious issues like fractures, brain swelling and bleeding, providing crucial information for urgent treatment decisions,’ he explains.
Magnetic Resonance Imaging (MRI) is used in situations requiring more detailed evaluation, particularly when concussion symptoms persist or worsen. ‘MRI excels in identifying subtle injuries, such as microbleeds and brain swelling, often missed by CT scans,’ says Dr Viljoen. Unlike CT scans, MRI does not use radiation, making it a safer option for repeated assessments over time.
Advanced imaging methods
Emerging imaging techniques, such as Diffusion Tensor Imaging (DTI), show promise for better understanding and management of head injuries, especially the subtle effects of concussions. ‘DTI helps identify damage to the brain’s white matter, potentially guiding return-to-play decisions and treatment strategies,’ notes Dr Viljoen.
Understanding possible complications – Second Impact Syndrome (SIS)
SIS is a rare but extremely serious condition that occurs when a person sustains a second concussion before fully recovering from an initial concussion. This second injury doesn’t have to be severe to trigger SIS – it can even be minor – but it causes rapid and severe brain swelling (cerebral oedema).
The brain’s ability to regulate its blood flow and pressure is compromised following the initial concussion, making it vulnerable to catastrophic swelling after a subsequent impact. Symptoms can escalate quickly, often within minutes, including loss of consciousness, severe headache, dilated pupils, respiratory failure and even death. Young athletes are especially vulnerable to SIS. Due to its rapid progression and severity, SIS is considered a medical emergency requiring immediate intervention.
Preventing SIS involves strictly adhering to concussion management protocols, ensuring full recovery after any head injury and carefully monitoring symptoms before returning to sports or high-risk activities.
Addressing Chronic Traumatic Encephalopathy (CTE)
Dr Viljoen says CTE is a long-term degenerative brain condition linked to repeated head impacts. ‘CTE is challenging because currently, it can only be definitively diagnosed after death. However, ongoing research aims to develop methods to detect CTE in living patients, potentially using advanced imaging techniques like Positron Emission Tomography (PET).’ Most research is focused on advancing non-invasive methods to see what is happening inside the brain of a living person and to track it over time.
Common causes of head injuries in rugby
These primarily arise from the high-impact nature of the sport, with tackling identified as a significant risk factor. Tackling, particularly when performed incorrectly or at a dangerous height, frequently leads to head trauma. Young players are especially vulnerable as their tackling techniques may not yet be fully developed, increasing the likelihood of injury. Teaching safe and correct tackling methods early is a way to mitigate these risks
Rugby’s dynamic gameplay often results in players being brought down forcefully or falling awkwardly. Even with protective gear, the impact of the head striking the playing surface can lead to concussions or more severe trauma
Due to the speed and intensity of the game, unintended impacts between players are inevitable. These include clashes of heads or impacts from knees and elbows, which can result in injuries ranging from mild concussions to more severe brain injuries. Preventative strategies and safer playing practices can reduce these risks
Prevention remains critical
Dr Viljoen emphasises the importance of proper training: ‘Educating young players on safe tackling techniques and enforcing protective protocols significantly reduces injury risks. Protective gear like headguards can minimise superficial injuries, though it does not prevent concussions.’
He also stresses the importance of concussion protocols. ‘Coaches at schools and clubs must rigorously apply concussion management strategies, ensuring players are adequately assessed and cleared by medical professionals before returning to the field.’ Under-reporting in schoolboy ruby often occurs because the player either wants to stay in the game and/or doesn’t recognise the symptoms of concussion.
Dr Viljoen concludes, ‘Rugby is a fantastic sport for building teamwork and resilience but player safety must always come first. Through awareness, timely medical intervention and proper preventative strategies, we can significantly reduce the risk and severity of head injuries, allowing young athletes to safely enjoy the game they love.’
A new study led by researchers at Mass General Brigham suggests a nasal spray developed to target neuroinflammation could one day be an effective treatment for traumatic brain injury (TBI). By studying the effects of the nasal anti-CD3 in a mouse model of TBI, researchers found the spray could reduce damage to the central nervous system and behavioural deficits, suggesting a potential therapeutic approach for TBI and other acute forms of brain injury. The results are published in Nature Neuroscience.
“Traumatic brain injury is a leading cause of death and disability – including cognitive decline – and chronic inflammation is one of the key reasons,” said lead author Saef Izzy, MD, FNCS, FAAN, a neurologist and head of the Immunology of Brain Injury Program at Brigham and Women’s Hospital, a founding member of the Mass General Brigham healthcare system. “Currently, there is no treatment to prevent the long-term effects of traumatic brain injury.”
The study examines the monoclonal antibody Foralumab, made by Tiziana, which has been tested in clinical trials for patients with multiple sclerosis, Alzheimer’s disease, and other conditions.
“This opens up a whole new area of research and treatment in traumatic brain injury, something that’s almost impossible to treat,” said senior author Howard Weiner, MD, co-director of the Ann Romney Center for Neurologic Diseases at Brigham and Women’s Hospital. “It also means this could work in intracerebral hemorrhage and other stroke patients with brain injury.”
Multiple experiments were done in mouse models with moderate-to-severe traumatic brain injury to explore the communication between regulatory cells induced by the nasal treatment and the microglial immune cells in the brain. Over time, researchers were able to identify how they modulate immune response.
“Modulating the neuroinflammatory response correlated with improved neurological outcomes, including less anxiety, cognitive decline, and improved motor skills,” Izzy said.
In addition to assessing the effects of the treatment, the research team was able to learn about immune response over time and compare the immune responses and effects of TBI in the mice.
The next step in the research is to translate the findings from preclinical models to human patients.
“Our patients with traumatic brain injury still don’t have an effective therapeutic to improve their outcomes, so this is a very promising and exciting time to move forward with something that’s backed up with solid science and get it to patients’ bedsides,” said Izzy.
Once in the clinical setting, Weiner said the hope is this treatment could be used on a variety of traumatic brain injury patients, including football players with repetitive concussions.
“We envision giving a nasal spray right there on the sidelines,” said Weiner. “It isn’t something we can do yet, but we see the potential.”
A new analysis of mortality data reveals the disproportionate impact of traumatic brain injuries (TBI) on older adults, males and certain racial and ethnic groups. The study, published in the peer-reviewed journal Brain Injury, provides a comprehensive analysis of TBI-related deaths across different population groups across the US in 2021.
The findings indicate that suicides remain the most common cause of TBI-related deaths, followed by unintentional falls, and specific groups are disproportionately affected by these tragedies.
Men, in particular, were found to be most likely to die from a TBI – more than three times the rate of women (30.5 versus 9.4). The reasons observed were multifactorial and could reflect differences in injury severity following a fall or motor vehicle crash, to the interaction of sex and age – with TBI outcomes in men worsening with age, while postmenopausal women fare better than men of similar age.
“While anyone is at risk for getting a TBI, some groups have a higher chance than others of dying from one. We identified specific populations who are most affected. In addition to men, older adults are especially at risk, with unintentional falls being a major cause of TBI-related death. American Indian or Alaska Native people also have higher rates of these fatal injuries,” says lead author Alexis Peterson PhD, of the National Center for Injury Prevention and Control at the Centers for Disease Control and Prevention.
“These findings highlight the importance of tailored prevention strategies to reach groups who may be at higher risk and the role healthcare providers can play in reducing TBI-related deaths through early intervention and culturally sensitive care.”
TBI remains a leading cause of injury-related death in the US In 2020, TBIs were associated with around a quarter of all injury-related deaths.
Using data from the National Vital Statistics System, the new analysis identified 69 473 TBI-related deaths among US residents during 2021. The age-adjusted TBI-related mortality rate was 19.5 per 100 000, representing an 8.8% increase from 2020.
Through statistical modeling, the researchers examined the simultaneous effect of multiple factors such as geographic region, sex, race and ethnicity, and age, on TBI-related mortality.
Key findings include:
Older adults (75+) had the highest rates of TBI-related deaths, with unintentional falls being the most common cause in this age group.
Non-Hispanic American Indian/Alaska Native individuals experienced the highest TBI-related death rate (31.5) compared to other racial and ethnic groups.
There were 37,635 TBI-related deaths categorised as unintentional injuries (ie, motor vehicle crashes, unintentional falls, unintentionally struck by or against an object, other).
30,801 were categorized as intentional injuries (ie, all mechanisms of suicide and homicide).
Children aged from birth to 17 years accounted for around 4% of TBI-related deaths (2,977).
The authors emphasise the critical role of healthcare providers in preventing TBI-related deaths, particularly with groups at higher risk. “By assessing patients who may be at higher risk for TBI, especially due to falls or mental health challenges, healthcare providers can make timely referrals and recommend culturally tailored interventions to prevent further injury or death,” says Dr Peterson.
Public health efforts should focus on addressing the underlying causes of TBI-related deaths, such as unintentional falls and mental health crises, to help prevent further loss of life. “TBIs remain a significant public health concern, especially among older adults, men, and certain racial and ethnic groups,” says Peterson. “CDC has proven resources that healthcare providers can use to not only reduce health disparities that increase the risk for TBI but also improve care for anyone affected by a TBI.”
The authors note the COVID-19 pandemic could have influenced TBI-related death trends in 2021. They also acknowledge several limitations of this analysis, including potential misclassification or incomplete documentation of causes on death certificates, which may lead to inaccuracies in estimating TBI-related deaths.
Coup and contrecoup brain injury. Credit: Scientific Animations CC4.0
Birmingham scientists have shown light therapy delivered transcranially can aid tissue repair after mild traumatic brain injury (mTBI). Their research, published in Bioengineering & Translational Medicine, indicates that this novel method could result in a new treatment option in an area of medicine that currently has few, if any, treatment options.
Traumatic brain injury (mTBI) results when the initial trauma of head injury is magnified by a complex set of inflammatory changes that occur in the brain. These secondary processes, which take place from minutes to hours after head injury, can dramatically worsen outcomes for patients.
The method invented by scientists at the University of Birmingham, UK and patented by University of Birmingham Enterprise aims to protect against this secondary damage, and stimulate faster, and better recovery for patients.
We want to develop this method into a medical device that can be used to enhance recovery for patients with traumatic brain or spinal cord injury, with the aim of improving outcomes for patients.
Professor Zubair Ahmed, College of Medicine & Health
In the study, the Birmingham team, comprising researchers Professor Zubair Ahmed, Professor Will Palin, Dr Mohammed Hadis and surgeons Mr Andrew Stevens and Mr David Davies, examined the effect of two wavelengths of near infrared light (660nm and 810nm) on recovery following injury.
The study in preclinical models used daily two-minute bursts of infrared light, delivered by a laser, for three days post-injury.
The findings showed significant reductions in the activation of astrocytes and microglial cells, which are heavily implicated in the inflammatory processes in the brain that follow head trauma, and significant reductions in biochemical markers of apoptosis (cell death).
At four weeks, there were significant improvements in performance in functional tests involving balance and cognitive function. The red light therapy also accelerated recovery compared to controls, with superior outcomes for light with a wavelength of 810nm.
The study builds on research published earlier this year which showed near infrared light delivered directly to the site of spinal cord injury both improves survival of nerve cells and stimulates new nerve cell growth.
Professor Ahmed, who led the study, said: “We want to develop this method into a medical device that can be used to enhance recovery for patients with traumatic brain or spinal cord injury, with the aim of improving outcomes for patients.”
The researchers are seeking commercial partners to co-develop the device and take it to market.