Home-based hypertension care led to reductions in systolic blood pressure and improvements in hypertension control in South Africa, according to late-breaking research presented in a Hot Line session at ESC Congress 20251 and simultaneously published in the New England Journal of Medicine.
“Hypertension is the primary risk factor for stroke and heart disease, which are leading causes of death in South Africa. Despite the wide availability of low-cost, effective therapies, hypertension control remains extremely poor in resource-limited settings. Obstacles include a lack of patient confidence to manage their own hypertension care, overcrowded clinics with long wait times and the cost of transport to clinics,” explained the IMPACT-BP trial’s Co-Principal Investigator Doctor Thomas Gaziano from Mass General Brigham (MGB) and Harvard Medical School, Boston, USA. “Our trial aimed to assess the effectiveness and implementation of reliable, home-based, technology-supported interventions to improve blood pressure control in low-resourced rural South Africa.”
IMPACT-BP was an open-label, randomised controlled trial conducted at the Africa Health Research Institute (AHRI) in KwaZulu-Natal, South Africa, in which patients were recruited from two public-sector primary healthcare clinics. The implementation study was designed with Co-Principal Investigator, Doctor Mark Siedner of AHRI and MGH, Professor Nombulelo Magula of the University of KwaZulu-Natal, and the KwaZulu-Natal Provincial Department of Health.
Adult patients were eligible if they had evidence of uncontrolled hypertension as defined by South African Department of Health Guidelines: two measurements of systolic blood pressure (SBP) >140 mmHg and/or diastolic BP (DBP) >90 mmHg, taken a minimum of 6 months apart.
Patients were randomised to one of three strategies: 1) standard-of-care, clinic-based blood pressure (BP) management; 2) home-based BP self-monitoring supported by the provision of BP machines, community health workers (CHWs) who conducted home visits for data collection and medication delivery, and remote nurse-led care assisted by a mobile application with decision support; or 3) an enhanced CHW group in which BP machines included cellular technology to transmit BP readings automatically to the mobile application. The primary outcome was change in SBP from enrolment to 6 months.
In total, 774 patients were randomised. The mean age was 62 years, 76% were women, 14% had diabetes and 47% were living with HIV.
Compared with standard-of-care, mean SBP at 6 months was lower in the CHW group (−7.9mmHg; 95% confidence interval [CI] −10.5 to −5.3; p < 0.001) and the enhanced CHW group (−9.1mmHg; 95% CI −11.7 to −6.4; p < 0.001). In the standard-of-care group, hypertension control at 6 months was 57.6% compared with 76.9% in the CHW group and 82.8% in the enhanced CHW group. Improved BP with home-based care appeared to persist at 12 months.
Severe adverse events (2.7%) and deaths (1.0%) were uncommon overall and similar across groups. Retention in care remained more than 95% in both intervention groups, with patients reported to have enjoyed managing their own hypertension.
Summarising, Doctor Siedner said, “This study is an important example of how making models of chronic disease care more convenient – taking it from the clinic to patients’ homes and letting them play a major role in their own care – can substantially improve hypertension outcomes.”
Of particular value was that the programme was successful in a community that has historically had low access to care. Professor Magula concluded: “Achieving hypertension control in over 80% of people in a predominantly Black African community in rural South Africa is a clear example that equitable health care access can be achieved in disadvantaged communities. Similar models of care that address structural barriers could be considered to improve hypertension control in other remote and resource-limited settings. Expansion of the model to include the care of people with multiple comorbidities may also be valuable.”
Inkosi Albert Luthuli Central Hospital is KwaZulu-Natal’s only public hospital with a functioning cardiac unit. Photo by Hush Naidoo Jade Photography on Unsplash
By Chris Bateman
Doctors have blown the whistle about a crisis at one of KwaZulu-Natal’s most important public hospitals, saying it is functioning far under capacity due to a series of crippling cuts.
The Inkosi Albert Luthuli Central Hospital in Durban’s Cato Manor is operating at around 40% below surgical capacity, according to senior doctors there. As one of a small number of central hospitals in South Africa, it provides specialist services unavailable elsewhere in KwaZulu-Natal and serves as a critical hub for training healthcare workers.
Several doctors who work at Albert Luthuli, who asked to remain anonymous for fear of reprisals, told Spotlight that frozen posts, severely understaffed ICUs, shortages of surgical consumables, and delays in diagnostic tests have combined to drive an austerity-fuelled collapse they say is costing lives.
One doctor said theatre slates – daily surgery schedules – have been cut by as much as 60% compared to pre-pandemic levels. Some described the situation as worse than during COVID-19, when all elective surgeries were cancelled.
“Patients have to wait or be sent home when they can’t get on a theatre list. Then they’re either lost to follow-up or they present ‘in extremis’ later,” said one senior doctor. “Paediatric cases are among the worst. They should be referred on day one, but because of ICU nursing shortages they only get admitted on day four or five – if at all. Often, they’re too ill for our care to be effective.”
Spotlight put these allegations to the KwaZulu-Natal Department of Health, but the department had not responded by deadline despite several follow-ups.
Collapsing specialist services
Albert Luthuli is KwaZulu-Natal’s only public hospital with a functioning cardiac unit, according to one of the doctors who spoke to Spotlight. The doctor said the province has just one adult cardiologist in the public sector who sees over 60 patients per day and that cardiac surgeries have dropped from 600 per year to under 300 projected for 2025. By contrast, there are over 30 adult cardiologists working in the private sector in the province.
Anaesthesiology is among the hardest hit areas. According to Spotlight’s sources, eight anaesthetic consultants resigned in the past year, citing burnout and workload. Where nine or ten theatre slates once ran daily, there are now only four or five. Eleven anaesthetists remain to cover 19 theatres.
“I never thought I’d see the day when I wouldn’t want to come in. We are four ICU consultants covering nine beds. ICU needs one nurse per bed, but we’re usually staffed with six or seven nurses in total. Across six ICUs, we’ve got 25 nurses. We pull in ward staff or rely on overtime. You can’t have one nurse running between beds – it spreads infection, mistakes happen. It’s impossible,” one ICU doctor told Spotlight.
Doctors estimate a 45% shortage of qualified ICU nurses. “It’s like airplanes circling, running out of fuel, and crashing before they can land,” one senior doctor said. “Patients deteriorate while waiting for beds or for a theatre list to open.”
Specialist theatre nursing posts have also been cut, compounding the strain.
Registrars squeezed, training undermined
The hospital is meant to offer advanced procedures, experimental treatments, innovative research, and specialist training. Instead, registrars – these are doctors in specialist training – say they are losing out on irreplaceable experience.
Junior registrars are allegedly blocked from logging procedures they need to qualify, because seniors are prioritised to assist with the shrinking pool of operations.
Spotlight has seen a grievance letter from the Anaesthetics Department’s Registrar Representative, addressed to the hospital CEO, medical manager, the SA Society of Anaesthesiologists, and training stakeholders. It warns that the consultant exodus has left registrars running high-risk cases with inadequate supervision, “directly compromising both patient safety and registrar training.”
One senior doctor said theatre usage had more than halved in recent months compared to historical averages. With no new registrar intake and no appointments of departed registrars to consultant posts, it is projected only 10 or 12 permanent consultants will remain for the hospital’s 846 beds – there should be at least 21 consultants. (A registrar becomes a consultant, or qualified specialist, once their training is complete.)
“This is no longer a looming concern, but an active crisis,” the letter warned, threatening patient safety, staff wellbeing, and the integrity of training in KwaZulu-Natal.
“What they broke in six months will take years to fix,” said one registrar.
But some are more positive. Professor Dean Gopalan, Head of Anaesthesiology, Pain Medicine & Critical Care at UKZN’s School of Medicine, said austerity cuts had dented efforts to achieve excellence, but “we remain above required training norms”. He said he was awaiting feedback from the Health Professions Council (HPCSA), which inspected the hospital in July and raised concerns about specialist and nurse shortages. Spotlight followed up with the HPCSA, but had not received a response by the time of publication.
Not all departments are as fortunate. One doctor said it would be “almost impossible” to meet training accreditation standards for cardiology given the patient workload.
Human cost
Doctors say the crisis is most visible in paediatric congenital heart disease cases.
“These children could live normal lives if operated on early. Instead, they wait until they are drastically sick before making the theatre slate – often six months later,” said one doctor. “People forget surgery is also a primary healthcare intervention. Breadwinners sit at home unable to work, while their families suffer.”
In orthopaedics, doctors say the waiting list exceeds 1 300 patients, with the first elective surgery dates only available in March 2028. Before COVID-19, they say the waiting period was seven months.
“Many patients are unable to work due to their conditions and would be able to get back to work if they had their operations,” said one source. “We try prioritising them, but then you put them ahead of others also in severe pain. Complications are already coming in from other hospitals due to unavailable implants and delayed treatments.”
Procurement freeze
Several doctors trace the crisis to a “G77 notice” issued by the KZN Department of Health on 14 November 2024, freezing new purchase orders until April 2025 to “manage accruals” and reduce overspending. Exceptions required approval from head office.
While a less prescriptive circular has since replaced it, procurement remains “extremely difficult”, sources said.
Doctors said the freeze caused months-long delays in acquiring consumables, drugs, and equipment. “We’re almost at the point where we’re only doing emergencies,” said one doctor. “We prioritise cancer patients for chemo or radiation instead of urgently needed surgery. But in cardiac surgery, there’s definite mortality. You can’t avoid it when you can’t do bypasses or valve replacements. Waiting lists are years long.”
One anaesthetist recalled a patient being “closed” mid-operation because a critical consumable was unavailable.
A national problem?
The situation at Albert Luthuli hospital partly reflects a wider national crisis in specialist care. A 2019 government strategy paper noted only 16.5 specialists per 100 000 people overall, with just seven per 100 000 in the public sector, compared to 69 per 100 000 in private.
Professor Eric Buch, CEO of the Colleges of Medicine of SA, said austerity has worsened matters by reducing registrar posts and constricting the pipeline. “Specialist posts are being frozen, impeding access to specialist care and reducing the number of specialists available to train registrars. Even before austerity we had far too few specialists. Some registrars waited up to two years for a post.”
The Albert Luthuli hospital crisis is “not unique”, said Dr Reno Morar, COO of Nelson Mandela University’s Faculty of Health Sciences.
“Equity of access to specialised services simply does not exist,” he said. “Despite the mess, there are pockets of excellence, but there’s no strategic national vision for highly specialised services.”
Health Ombud Professor Taole Mokoena told Spotlight his office had not specifically investigated Albert Luthuli, but said that, “sadly, there are reports not dissimilar from many hospitals in the country,” citing Helen Joseph Hospital in Johannesburg and Robert Mangaliso Sobukwe Hospital in Kimberley.
Doctors at Albert Luthuli hospital have indicated to Spotlight they will lodge a formal complaint with the health Ombud.
Posts advertised
While the KZN Department of Health did not respond to Spotlight’s questions, there are signs of movement. Two days after we requested comment, a circular went out advertising dozens of specialist posts across provincial referral hospitals, including 12 anaesthetics posts, five of them at Albert Luthuli, plus 100 staff nurse and 50 registered nurse posts.
We also understand that an internal briefing of department heads was called for 27 August, 36 hours after Spotlight’s first request for comment.
Doctors, however, remain sceptical.
“Nothing will change for six months as we go through the interview, verification, and induction processes. Why did they take so long to listen? The damage is done. Relief is 18 to 24 months too late,” said one doctor.
Another senior doctor said that with each resignation over the past year, he lined up replacements and pleaded in vain for permission to advertise. “Since posts reopened this week, I know of just one applicant. Do they expect specialists to suddenly appear out of the woodwork?”
The job advertisements are for “far less than what has been lost and needed. And it’s far more than just numbers – it’s skills and experience”, noted another doctor. “It will take years to get back to where we were.”
Despair among staff
Several doctors expressed despair at what they see as a lack of urgency from government.
“It makes me wonder how resources are managed. Local cuts feel disproportionate compared to national ones. It’s disheartening. Some of us are here to make a difference, but we’re starting to lose hope,” one said.
Another added: “If you know there’s light at the end of the tunnel, you can keep going. But when it feels endless, it’s damn hard. We try to hide our disenchantment, but it’s becoming impossible.”
In the latest chapter of a long-running legal battle over the Gauteng Department of Health’s obligation to provide people in the province with radiation oncology services, the department has suffered another loss in the courts. Spotlight assesses the legal situation and asks what it means for people still waiting for the life-saving treatment.
With another court loss suffered this August, the Gauteng Department of Health has once again been ordered to urgently provide treatment for cancer patients who have been left in the lurch.
This ruling, handed down on August 5 by Judge Evette Dippenaar, follows urgent legal action brought by the Cancer Alliance. It was in response to the Gauteng health department’s appeal against a ruling handed down on March 27 by acting Judge Stephen van Nieuwenhuizen. That order compelled the department to clear its years-long backlogs in getting cancer treatment to patients.
In its March ruling, the South Gauteng High Court in Johannesburg found the department’s failure to deliver this critical treatment to be unconstitutional and unlawful. The decision follows the department’s failure to spend a R784 million allocation granted by the provincial Treasury in 2023 to reduce the treatment backlog by outsourcing services to the private sector over a three-year period. Due to severe delays, the department was forced to return the first R250 million tranche.
Van Nieuwenhuizen strongly criticised the department, stating: “The provincial health respondents have done nothing meaningful since the money was allocated in March 2023 to actually provide radiation oncology treatment to the cancer patients. Meanwhile, the health and general well-being of the patients has significantly deteriorated. There is clear, ongoing, and irreparable harm being suffered by those still waiting for treatment.”
He also condemned the department for its lack of accountability and poor management of public resources, finding that it had failed to uphold ethical standards, act transparently, or respond to patients’ needs fairly and effectively.
The court instructed the department to:
Take immediate action, including diversion to private facilities, to provide radiation oncology services to all patients on the backlog list,
Update the backlog list within 45 days,
Submit a detailed progress report on efforts to deliver treatment, and
Present a long-term plan for ongoing cancer treatment services within three months.
But Gauteng health MEC Nomantu Nkomo-Ralehoko and the health department challenged the judgment in May, just as their 45 days to act ran out. They chose instead to take the entire matter on appeal to the Supreme Court of Appeal (SCA).
In response, the Cancer Alliance, represented by SECTION27 (*see disclosure), went back to court for an interim order to make the March 27 ruling immediately enforceable, and not suspended until a ruling is made by the SCA. It is in response to this application that Judge Dippenaar ruled on August 5 that the March ruling is indeed immediately enforceable.
Two courts have now sent a clear message to the Gauteng health department, says attorney Khanyisa Mapipa, who heads health rights at SECTION27. She adds: “The Gauteng Department of Health’s action should be in the interest of the person who is seeking treatment. It should not be to deny, deny, deny and then to fight in the courts and not take any accountability.”
The waiting list
The estimated number of people on a waiting list for cancer treatment in 2022 was around 3 000 people. New data on this has not been made publicly available.
There are some signs of progress, although details are hard to pin down. In a statement released on August 24, which reiterates a July 20 statement, the Gauteng health department said it had introduced a strategic partnership with private service providers. “As the beginning of August 2025, 563 patients were receiving radiation oncology care through private partnerships, while 1 076 patients had completed treatment by end of July 2025,” it stated.
Both statements also noted that work was underway to complete new radiotherapy centres at Chris Hani Baragwanath and Dr George Mukhari Academic Hospitals.
But Mapipa says they still don’t have full details that comply with the court order. “What we’re asking for essentially is what the department should be doing anyway and that is for them to go through their patient files to establish who is still on the backlog list; who has passed away, who has received treatment, when patients were last assessed and what treatment they qualify for; and if it was a public facility or were they diverted to a private facility,” she says.
“As the judge pointed out in March, the department has to do this as a constitutional obligation, whether they fight this to the Constitutional Court or not, their obligation is to provide treatment for people who meet the criteria. Those on the backlog list meets the criteria,” she says.
Part of the March order also compelled the department to file progress reports with the court within three months on the measures taken to provide treatment and its long-term plans to resolve the ongoing cancer treatment crisis in Gauteng. Spotlight’s understanding is that these progress reports have not been submitted.
This is an important measure, Mapipa says, given the department’s poor track record. “The court rulings in both judgments found that because they have failed to be transparent throughout this process, the department is compelled to provide these reports to the courts,” she adds.
It is as yet unclear how the Gauteng health department plans to proceed. The department, in its three-paragraph statement following the August judgment, stated that it would review “the contents and implications” to determine and communicate its next steps. Their deadline to appeal the August 5 ruling was 26 August 2025. The department did not respond to questions from Spotlight.
Calls for accountability
Jack Bloom, Democratic Alliance shadow health MEC in Gauteng, says that without a proper audit and update of the backlog list of patients needing care, the “cancer treatment scandal has probably cost more lives than the 144 mental patients who died in the Life Esidimeni tragedy when they were sent to illegal NGOs”.
Bloom is calling for heads to roll, with Nkomo-Ralehoko and head of department Arnold Lesiba Malotana in his crosshairs.
“The DA condemns the department’s legal stalling tactics that harms patients who urgently require lifesaving treatment…Premier [Panyaza] Lesufi should not allow this cancer disaster to continue,” he says.
Salomé Meyer, spokesperson for Cancer Alliance, says that the legal proceedings are a distraction of the realities on the hospital floor. Charlotte Maxeke Johannesburg Academic Hospital for instance, she says, remains in “crisis”. She maintains there is a scarcity of sufficient and operational radiation oncology machinery, as well as extreme shortages in radiation oncology staff to operate the machines.
Meyer says the situation at Charlotte Maxeke Hospital dates back to 2017 when CEO Gladys Bagoshi was made aware of mounting challenges from a shortage of equipment and staffing.
“In 2021, Bagoshi turned down an equipment allocation, which Charlotte Maxeke Hospital desperately needed, so this allocation went to George Mukhari Hospital and Chris Hani Baragwanath Hospital instead. But the cobalt bunkers required to house the machines at these hospitals had not been built and are only expected to be completed in 2026 – so the machines remain in storage. In 2022, an order was finally placed for additional linacs [used for high energy beam radiation treatments] for the existing cobalt bunkers at Charlotte Maxeke Hospital, but that tender is still not finalised,” says Meyer.
She adds: “This is a failure of planning, governance, and accountability and we have to ask who is being held accountable when the same CEO has remained in place all these years.”
Neither Bagoshi nor the health department responded to questions on these assertions.
Disclosure: SECTION27 was involved in the court proceedings described in this article. Spotlight is published by SECTION27, but is editorially independent – an independence that the editors guard jealously. The Spotlight editors gave special attention to maintaining this editorial firewall in the production of this story.
In response to US funding cuts for South African health services and research projects, National Treasury has provided the National Department of Health with hundreds of millions of rands in emergency funds. Spotlight and GroundUp look at how precisely the government intends to spend this money.
Health Minister Dr Aaron Motsoaledi recently announced that National Treasury had released roughly R753 million to help plug the gap left by US funding cuts to South Africa’s health system. Another R268 million is also being released in the following two years for researchers that lost their US grants.
But this may only constitute the first round of emergency funds from government, according to sources we spoke to. The health department is planning on submitting a bid for an additional allocation later on, which will be considered by Treasury. But this will likely only be approved if the first tranche of funding is properly used.
So how is the money supposed to be used? To find out, we spoke with officials from the National Treasury, the National Department of Health and the South African Medical Research Council (SAMRC).
Money for provinces is for saving jobs at government clinics
The current tranche of money comes from Treasury’s contingency reserve, which exists partially to deal with unforeseen funding shortfalls. It was released in terms of Section 16 of the Public Finance Management Act.
Of the R753 million that’s been announced for this year, Motsoaledi stated that R590 million would be going to provincial health departments via the District Health Programme Grant – a conditional grant for funding the country’s public health efforts, particularly HIV, TB, and other communicable diseases. Such conditional grants typically give the health department more say over how provincial departments spend money than is the case with most other health funding in provinces.
To explain how government officials arrived at this figure, it’s worth recapping what services the US previously supported within provinces.
Prior to Donald Trump becoming US president on 20 January, the US Agency for International Development (USAID) had financed health programmes in specific districts with high rates of HIV. These districts were scattered across all South Africa’s provinces, save for the Northern Cape.
The funds were typically channelled by USAID to non-governmental organisations (NGOs), which used the money to assist the districts in two ways.
The first is that NGOs would hire and deploy health workers at government clinics. The second is that the NGOs would run independent mobile clinics and drop-in centres, which assisted so-called key populations, such as men who have sex with men, sex workers, transgender people, and people who inject drugs.
In response, the health department began negotiations with Treasury to get emergency funding to restore some of these services. As part of its application, the health department submitted proposals for each province, which specified how much money was needed and how it would be used. (Though this only took place after significant delay and confusion).
Since Treasury couldn’t afford to plug the entire gap left by the US funding cuts, the provincial-level proposals only requested money for some of the services that had been terminated. For instance, funding was not requested for the key populations health centres. Instead, the priority was to secure the jobs that had been lost at government health facilities.
As such, the total amount that was requested from Treasury for each province was largely calculated by taking the total number of health workers that NGOs had hired at clinics and working out how much it would cost to rehire them for 12 months.
Rather than paying the NGOs a grant to deploy these workers as was done by USAID, the health department proposed hiring them directly. This meant that they calculated their wages according to standard government pay scales, which is less than what these workers would have earned from the NGOs.
The total came to just under R1.2 billion for all the provinces combined.
Treasury awarded roughly half of this on the basis that the money would be used to finance these wages for six months, rather than 12. This amounts to the R590 million for provinces that was announced by Motsoaledi.
If all goes smoothly and this money is used effectively to hire these staff over the next six months, then a new tranche of Section 16 funding could be released in order to continue hiring them. Funds might also be released to fund the key populations health sites.
A concern, however, is that the money may just be used by provinces to augment their ordinary budgets. If the funds aren’t actually used to respond to the US cuts, then it is much less likely that more emergency funding will be released.
At this stage, it is too early to tell how provinces will use the money, particularly given that it appears that at least some of them haven’t gotten it yet.
Spotlight and GroundUp sent questions to several provincial health departments. Only the Western Cape responded. The province’s MEC for Health and Wellness, Mireille Wenger, said that the funds have not yet been received by her department, but that once they were, they would be directed to several key priority areas, including digitisation of health records, and the strengthening of the primary healthcare system.
It’s thus not clear whether the province will be using any of the funds to employ health staff axed by US-funded NGOs. In response to a question about this, Wenger stated that “further clarity is still required from the National Department of Health and National Treasury regarding the precise provincial allocations and conditions tied to the additional funding”.
What about research?
Of the R753 million that’s been released for this year, R132 million has been allocated to mitigate the funding cuts for research by US federal institutions, primarily the National Institutes for Health (NIH). Unlike USAID, the NIH is not an aid body. It provides grants to researchers who are testing new treatments and medical interventions that ultimately benefit everyone. These grants can be awarded to researchers in the US or abroad as part of a highly competitive application process.
Researchers in South Africa are awarded a few billion rands worth of grants from the NIH each year, largely due to their expertise in HIV and TB. But over the last few months, much of this funding has been terminated or left in limbo. (See a detailed explanation of the situation here).
The R132 million issued by Treasury is supposed to assist some of these researchers. It will be followed by another R268 million over the following two years. The Gates Foundation and Wellcome Trust are chipping in an additional R100 million each – though in their case, the funds are being provided upfront.
All of this money – R600 million in total – is being channelled to the SAMRC, which will release it to researchers via a competitive grant allocation system.
According to SAMRC spokesperson Tendani Tsedu, they have already received the R132 million from Treasury, though they are still “finalizing the processes with the Gates Foundation and Wellcome Trust for receipt of [their donations]”.
The SAMRC is also in negotiation with a French research body about securing more funds, though these talks are ongoing.
In the meantime, the SAMRC has sent out a request for grant applications from researchers who have lost their US money. The memo states: “Applicants may apply for funding support for up to 12 months to continue, wind down or complete critical research activities and sustain the projects until U.S. funding is resumed or alternative funds are sourced.”
“The plan,” Tsedu said, “is to award these grants as soon as possible this year.”
Professor Linda-Gail Bekker, CEO of the Desmond Tutu Health Foundation, told us that the hope is that the grants could fill some of the gaps. “This is a bridge and it is certainly going to save some people’s jobs, and some research,” she said, but “it isn’t going to completely fill the gap”.
Indeed, the SAMRC has made clear that its grants aren’t intended to replace the US funding awards entirely. This is unsurprising given that the money that’s being made available is a tiny fraction of the total grant funding awarded by the NIH.
It’s unlikely that research projects will continue to operate as before, and will instead be pared down, said Bekker.
“It’s going to be about getting the absolute minimum done so you either save the outcome, or get an outcome rather than no outcome,” she said.
In other cases, the funds may simply “allow you to more ethically close [the research project] down,” Bekker added.
For some, this funding may also have come too late. Many researchers have already had to lay off staff. Additionally, patients who had been on experimental treatments may have already been transitioned back into routine care. It’s unclear how such projects could be resumed months later.
In response, Tsedu stated: “For projects that have already closed as a result of the funding cuts, the principal investigator will need to motivate whether the study can be appropriately resurrected if new funds are secured.”
The SAMRC has established a steering committee which will adjudicate bids. They will be considering a range of criteria, Tsedu said, including how beneficial the research might be for the South African health system, and how heavily the project was impacted by the US funding cuts. They will also consider how an SAMRC grant could “be leveraged for future sustainability of the project, personnel or unit”, added Tsedu.
An endless back and forth
The job of the SAMRC steering committee will likely be made a lot more complicated by the erratic policy changes within the NIH. On 25 March, the body sent a memo to staff – leaked to Nature and Bhekisisa – instructing them to hold all funding awards to researchers in South Africa. After this, numerous researchers in the country said they couldn’t renew their grants.
However, last month, Science reported that a new memo had been sent to NIH staff which said that while South African researchers still couldn’t get new grants, active awards could be resumed.
Since then, some funds appear to be trickling back into the country, but certainly not all. For instance, Spotlight and GroundUp spoke to one researcher who had two active NIH awards before the cuts. He stated that one of these was resumed last month, while the other is still paused.
Bekker also told us that she had heard of one or two research grants being resumed in the last week, though she said the bulk of active awards to South Africa are still pending.
“Where people are the prime recipients [of an NIH grant] without a sub awardee, there seems to be a queue and backlog but some [of those awards] are coming through,” said Bekker. “But how long this is going to take and when it might come through, we’re waiting to hear.” She said a strategy might be to apply for the SAMRC bridging funding and “if by some miracle the [NIH funding is resumed]” then researchers could then presumably retract their SAMRC application.
In the meantime, health researchers will have to continue spending their time working out how to respond to the abrupt and increasingly confusing changes to funding guidelines that have dogged them since Trump assumed office.
“It’s such a dreadful waste of energy,” said Bekker. “If we were just getting on with the research, it would be so much better.”
Sanofi has reaffirmed its commitment to South African healthcare with the appointment of two senior leaders and a renewed focus on supporting healthcare professionals, expanding local partnerships, and improving access to essential treatments in key areas such as vaccines, immunology, and rare diseases.
“This is a new chapter for Sanofi in South Africa,” says Jean-Baptiste Bregeon, Sanofi South Africa’s Country Lead and Head of Vaccines. “We are focused on making a real impact through practical support for healthcare professionals, expanding access to important medicines and vaccines, and strengthening our ties with partners across the system.”
Focused leadership
Bregeon brings over 20 years of international experience, with senior roles in commercial and clinical operations across the Middle East, North Africa, and Eurasia. As former General Manager for North Africa at Sanofi Vaccines, he led efforts to improve vaccine access and build local capacity. He has also advised Sanofi’s global leadership on operational strategy and commercial planning.
Bregeon will oversee Sanofi’s overall strategy in the country and lead its vaccine division, which remains a core part of the company’s healthcare offering.
Lenisha Maharaj, newly appointed Head of Pharma for South Africa, Namibia and Botswana, is a seasoned Pharmaceutical Executive with over 20 years’ experience in the pharmaceutical and healthcare sectors. At Sanofi, she will oversee growth across the general medicines and specialty care portfolios, supporting both primary and specialist care.
“Sanofi understands the realities that healthcare professionals face,” says Maharaj. “Our goal is to support them with the right tools, training, and access to innovative treatments so they can keep delivering high-quality care.”
Strengthening partnerships and access
A key part of Sanofi’s long-term strategy is to build strong, lasting partnerships. Its collaboration with Biovac, a local vaccine manufacturer, is a core example. This will help to boost domestic vaccine production capacity and reduce reliance on global supply chains. Such public-private partnerships support healthcare resilience as well as local economic and scientific development.
Beyond vaccines, Sanofi is investing in other areas that have a direct impact on healthcare professionals and the patients they serve:
Clinical trials in South Africa: Expanding its local clinical research footprint to increase representation of African patients in global trials and ensure that treatment decisions are informed by local data.
Access to innovative medicines: Working to bring advanced treatments in rare diseases and immunology to South Africa, along with patient support programmes and diagnostic assistance, to help doctors and patients navigate access challenges.
Medical education and digital engagement: Offering CPD-accredited education, clinical webinars, and digital tools to help healthcare professionals stay updated on the latest treatment protocols and deliver more streamlined care.
Policy engagement and system support: Actively involved in discussions with policymakers and funders to help shape health policies that improve medicine access and promote fair, sustainable healthcare.
Supporting healthcare professionals
Sanofi says it recognises the ongoing pressures facing South African healthcare workers, from dealing with supply shortages and reimbursement hurdles to managing the growing burden of chronic and complex diseases.
“We see our role as being part of the solution,” says Bregeon. “We are here to support healthcare professionals, not only by ensuring a reliable supply of medicines, but by providing the training, tools, and partnerships they need to do their jobs effectively.”
The company is also prioritising engagement with healthcare professionals through regular updates, field team support, and opportunities for joint problem-solving around system-level challenges.
Sanofi says it is committed to staying in close conversation with the healthcare community and building a more resilient, inclusive, and patient-focused system.
“We want to work with doctors, nurses, pharmacists, policymakers and funders to build something long-term,” Bregeon adds. “We believe that by working together, we can improve outcomes for patients and strengthen the foundation of healthcare in this country.”
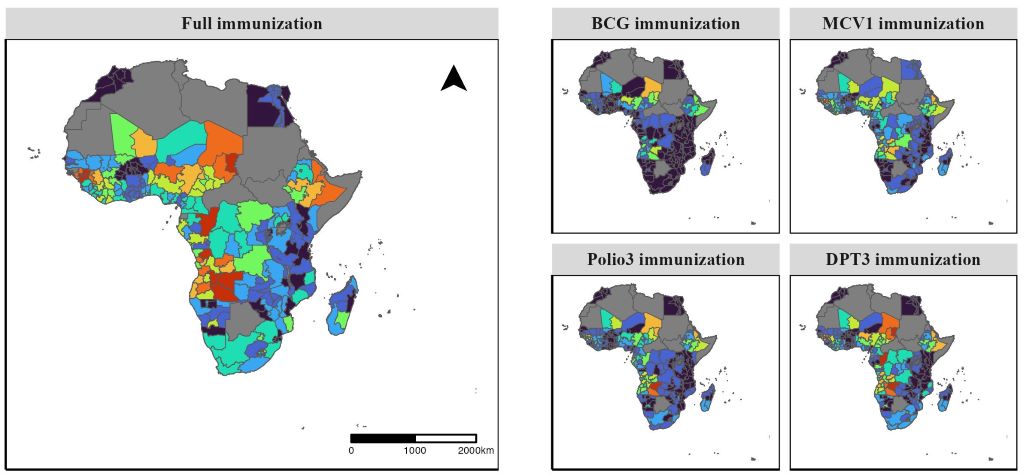
Researchers analysed 1 million records from national health surveys in 38 African countries and found progress in childhood immunisation coverage – but many countries, including South Africa, may still fall short of global targets
Maps of childhood immunisation coverage in African countries at regional level for 2020.
In the last two decades, childhood immunisation coverage improved significantly across most African countries. However, at least 12 countries, including South Africa, are unlikely to achieve global targets for full immunisation by 2030, according to a new study published July 29th in the open-access journal PLOS Medicineby Phuong The Nguyen of Hitotsubashi University, Japan, and colleagues.
Vaccines are one of the most effective ways to protect children from deadly diseases, yet immunisation coverage is still suboptimal in many African countries. Monitoring and progress in childhood immunisations at the national and local level is essential for refining health programmes and achieving global targets in these countries.
In the new study, researchers used childhood immunisation data contained in approximately 1 million records from 104 nationally representative Demographic and Health Surveys (DHS) conducted in 38 African countries between 2000 and 2019. Using modelling techniques, they estimated immunisation coverage trends through 2030 and assessed disparities across geographic regions and between socioeconomic groups.
The data showed overall improvements in immunisation coverage between 2000 and 2019. It forecast that, if current trends continue, most countries are projected to meet or exceed targets for achieving 80% or 90% coverage of vaccines against tuberculosis, measles, polio, diphtheria, pertussis (whooping cough), and tetanus. However, 12 of 38 countries are not on track to meet full immunisation goals, including high-development nations like South Africa, Egypt, and Congo Brazzaville. The study also pinpointed significant socioeconomic inequalities in coverage, with gaps in coverage of up to 58% between wealth quintiles. While these disparities were present across all countries, most are projected to shrink by 2030 –except in Nigeria and Angola, where inequalities are expected to persist or grow.
“These achievements are likely the result of sustained progress driven by decades of national and sub-national initiatives along with international support aimed at prioritising immunisation,” the authors say. “However, progress towards full immunisation coverage remains slow in 12 African countries examined. In most African nations, challenges related to vaccine affordability, accessibility, and availability remain major obstacles, driven by weak primary healthcare systems and limited resources.”
The authors add, “This study shows that while childhood immunisation coverage has improved in Africa, progress is uneven. Many countries and regions remain off track to meet global targets by 2030.”
The authors conclude, “Conducting this study reinforced how critical reliable sub-national data is for identifying communities being left behind. We hope the findings will help inform more equitable and targeted immunisation strategies.”
As healthcare reform gains momentum in South Africa, value-based care is becoming a hot topic – but meaningful progress has yet to take hold. The biggest hurdle? How care is purchased. Despite clear signs of stagnation, most funders remain committed to the same failed approach and have yet to drive the change that is needed.
“It’s encouraging to see a move away from fee-for-service thinking and a growing focus on value-based care. But to turn that interest into action will require real system reform – starting with strategic approaches to purchasing care that support system reengineering,” says Lungile Kasapato, CEO of PPO Serve, a healthcare management company that has been implementing value-based care in South Africa for more than a decade.
At its core, value-based care flips the script on how private healthcare is purchased in South Africa. Instead of rewarding volume, it prioritises prevention, puts patients at the centre, and ties payment to measurable outcomes. This stands in stark contrast to the dominant fee-for-service model, where doctors and hospitals are incentivised to provide more services rather than focus on delivering effective care.
A leading example of value-based care in practice is The Value Care Team, operationally supported by PPO Serve. This GP-led multidisciplinary programme broadens access while keeping costs in check. Teams are paid a risk-adjusted global fee to provide holistic patient care, along with substantial incentives tied to improved outcomes. The result is a model that aligns payment with patient outcomes – not the volume of services delivered.
To put it simply, Kasapato explains; “With value-based care, you don’t pay for every kilometre run, you pay to cross the finish line. And that finish line means improved health outcomes, prevention, and system efficiency.” For patients, primary healthcare under The Value Care Team looks and feels completely different. With no scheme benefit limits to navigate, patients are supported by a dedicated care coordinator who guides them through decisions made by their nominated GP and allied professionals. Each clinical team member has a complete picture of the patient’s health, working collaboratively rather than competitively to share accountability for delivering better outcomes.
This new approach to delivering primary care in the private sector isn’t just an isolated test run – it’s being developed and refined in real time. “We’re not just talking about value-based care, we’re implementing it,” says Kasapato. “At PPO Serve, we partner with practices to navigate day-to-day challenges, while working with medical schemes to design payment models that enable strategic purchasing. The Value Care Team is proof that value-based contracting isn’t just possible – it’s already happening in South Africa’s healthcare system.”
For this approach to take root and scale, medical schemes and state funders must take the lead by creating the market incentives that encourage providers and hospitals to adopt new ways of working. The Competition Commission’s 2019 Health Market Inquiry warned that without bold reform, South Africa’s private healthcare sector could face collapse – a warning that remains just as relevant today. But there is still an opportunity to change course. By embracing a strategic purchasing role, funders can help drive the system-wide transformation that’s urgently needed.
The Value Care Team is already leading by example, with a presence across Gauteng and KwaZulu-Natal, as well as in Bloemfontein and Gqeberha. Recognised by the World Health Organisation and featured in international peer-reviewed research as a breakthrough case study in emerging markets, the programme is actively driving real change – improving care coordination, cutting waste, and reducing unnecessary hospital admissions. Even so, Kasapato points out, the journey is far from over; “There is still a lot to learn from and with others as we move from talking about value to actually implementing it.”
The Nelson Mandela-Fidel Castro medical training programme has been controversial from the start. It’s had high points, low points and many say it should have an end point.
Almost 30 years since the Cuba-SA doctors’ training programme was launched, it still divides opinion.
This year only Gauteng and North West interviewed candidates for the bursary programme that sends students from South Africa to be trained in the island country.
Critics say the dwindling interest shows the Nelson Mandela-Fidel Castro (NMFC) medical training programme has passed its sell-by date. But supporters remain committed to its ideals and some beneficiaries of the programme still think of it as the opportunity of a lifetime.
Between the differing views, what can be glimpsed is a chequered story of three decades of trying to transform South Africa’s healthcare system. The programme has its origins in the ANC’s political fraternity with Cuba and the laudable ideal of boosting doctors numbers in under-serviced rural areas. But it is also a tale of political inertia arguably blurring over time into a blind spot as conditions changed. In the background is the stranglehold of corruption and maladministration in the health sector, shrinking provincial health budgets, transformation of doctors’ training, and changing curricula.
One concern is that little is actually known about the programme’s impact. There is a lack of clear data on the costs and the numbers of doctors produced. Shockingly, for such a long-running programme, no comprehensive evaluation reports have been published, as far as Spotlight has been able to establish.
A comprehensive evaluation would weigh the benefits of the programme against its costs, compare it to other options for training medical doctors, and contextualise it within the current reality of very tight health budgets in provincial health departments – as it is, not all the doctors we are training are being employed.
Given this context, it is not surprising that the National Department of Health recommended a scaling back of the programme a decade ago. While most provinces have taken this advice, the Gauteng and North West health departments have instead pushed ahead with the programme.
Old histories and old allegiances
The agreement that put in place the NMFC medical training programme was signed in 1996, with the first cohort of students leaving for Cuba a year later in 1997. It was a mere two years into democracy and South Africa urgently needed to address gaps in the provision of healthcare. Under apartheid, services prioritised a white minority mostly in urban settings and healthcare had a strong slant towards hospital or tertiary care. There was a shortage of doctors and those with the least access to healthcare services were rural communities made up mostly of black South Africans.
Medical schools mostly had curricula designed for the status quo and there were few academic pathways for underprivileged students who had good marks at school but were not top achievers, leaving them overlooked for scholarships and bursaries.
So the new government looked to Cuba.
With its focus on primary healthcare, preventative medicine, and community-based training, the Cuban approach to healthcare ticked many of the boxes for the South African government then led by President Nelson Mandela.
Since the communist revolution in Cuba in 1959, it has provided free healthcare to all its citizens. While there remains some scepticism over data collection and interpretation, politicisation of medicine, and limited freedom to criticise the state, Cuba’s healthcare system is also widely lauded.
According to the Primary Health Care Performance Initiative, the country registers average life expectancy at 78 years (South Africa is at around 66), infant mortality dropped from 80 deaths per 1000 live births in 1950 to just 5 deaths per 1000 by 2013, and it has one of the world’s highest doctor to patient ratios. In 2021, it was at 9.429 physicians per 1000 people, according to World Bank Open Data. In the same year, South Africa tracked at 0.8 per 1000.
Since the 1960s, Cuba has established itself as a hub for training international fee-paying students and sending them back to their mostly lower-income countries as graduate doctors. One of its biggest universities, the Latin American School of Medicine, graduated over 30 000 students from 118 countries in the 21 years since it was established.
Another tick was Cuba’s staunch support for the ANC. SA History Online emphasises the depth of solidarity. It notes: “Cuba was a state in alliance with provisional governments and independent states in the African continent. Cuba’s military engagement in Angola kept the apartheid state in check, foiling its geopolitical strategies and forcing it to concede defeat at Cuito Cuanavale, and ultimately forcing both PW Botha and FW de Klerk to the negotiating table.”
Costs and benefits
The political and historical bonds sealed the doctors’ training deal. But from the start, the bursary programme, funded from provincial budgets, came under fire. The estimated costs over nearly three decades are massive, but details remain fuzzy.
Spotlight’s questions to the national health department were “answered” in one paragraph by department spokesperson Foster Mohale. “More than 4 000 [lower numbers are quoted by government in other instances] doctors have been produced through this medical programme since its inception. The programme is still relevant today and complements the local medical schools to produce more doctors. Qualified doctors have options of joining either public or private health sector,” he wrote.
But discrepancies have been showed up in government’s own figures. In November 2022, Haseena Ismail, the then DA member on the portfolio committee of health raised concerns about the quality of government data.
Minister of Health at the time, Dr Joe Phaahla, said the preparatory year, including a stipend, cost US$4400 per student, and each of the following five years cost US$7400 per student. But a separate table from the health department listed higher figures – US$8400 for the preparatory year and up to US$15900 per student by the fifth year. Added to this, the department listed annual costs of US$6472 per student for food, accommodation, and medical insurance. There were also expenses for two return flights over six years, plus the cost of 18 months of tuition and accommodation for clinical training at a South African medical school.
Phaahla said that as of November 2022, 3369 students had been recruited into the programme, and 2617 had graduated. However, he noted there was no information on what happened to these doctors or where they were employed. Each bursary student is required to work for the state for the same number of years for which they received funding.
South Africa has 11 medical schools, with the most recent addition of the North West University.
The programme also faced criticism over selection criteria for bursary candidates and for requiring two extra years of training compared to local medical programmes. Students spend one year learning Spanish, five years training in Cuba, and then return to South Africa for an additional 18 months of clinical training at a local medical school.
Controversies have dogged the programme over the years. In 2013, the Afrikaans newspaper Beeld reported that by 2009, only half of the students enrolled in the programme during its first 12 years had completed their studies.
In 2012, government ramped up the numbers of students it sent abroad. In 2018, this backfired when about 700 fifth-year students returned home only to find they could not be accommodated at any of the then 10 medical schools in the country.
It was around this time that the national health department issued recommendations for the provinces to phase out the programme.
Gauteng and North West
Despite all of the above, the Gauteng Department of Health continues to fund students – around 20 last year and an expected 40 this year.
Spotlight’s questions on this to the Gauteng health department went unanswered.
Compounding the administrative and planning blunders for returning students is the impact of deepening corruption and mismanagement in Gauteng’s health department. It has been under routine Special Investigations Unit scrutiny as well as coming under fire for service delivery issues such as the ongoing backlog of cancer patients lingering on treatment waiting lists. In March, the South Gauteng High Court in Johannesburg ruled that the Gauteng health department failed in its constitutional obligation to make oncology services available.
The situation in the North West is also bleak. Its health facilities are routinely facing medicine stock-outs and understaffing. Its health department is regularly struggling with accruals and paying suppliers on time.
Given all these challenges, it is puzzling that these two provinces in particular are so committed to sending students to Cuba, we understand at higher cost than for training doctors locally.
‘Better investments’
Professor Lionel Green-Thompson, now the dean of the faculty of health sciences at the University of Cape Town, was involved in managing returning students from the Cuba-SA programme between the mid-2000s and 2016. At the time, he was a medical educator and clinician at Wits University where he oversaw the 18-month clinical training of more than 30 returning students.
“Some of these students were among the best doctors that I’ve trained and I remain a stalwart supporter of the ideals of the programme. But at this point, there are better investments to be made, including directly funding university training programmes in South Africa,” he tells Spotlight.
“A programme that’s rooted in our nostalgic connection with Cuba and its role in our change as a country is now out of step with many of the healthcare settings and realities we face in South Africa,” says Green-Thompson.
He says a proper evaluation of the programme needs to be done.
There are also lessons to learn, he says, including a review of admissions programmes. How some students who enter a programme at 20% below the normally accepted marks, exit the programme as excellent doctors, he says offers clues to rethink how great doctors can be made.
Green-Thompson also suggests we need to ask why specialisation has become a measure of success for many doctors in South Africa, often at the expense of family medicine. This, he says, takes away from the impact doctors make at community healthcare level as expert generalists.
But changing the perspectives of healthcare professionals requires early and sustained exposure to working in community healthcare settings, says Professor Richard Cooke, head of the department of family medicine and primary care at Wits. Cooke is also director of the Wits NMFC Collaboration since 2018 and serves on the NMFC Ministerial Task Team.
“I’m not in support of further students being sent to Cuba for the undergraduate programme, because these students are not being trained in our clinical settings,” he says, speaking in his Wits capacity.
“The Cuban system is far more primary healthcare based than South Africa’s, but that doesn’t necessarily translate into these students ending in primary healthcare,” says Cooke.
And curricula at Wits is shifting, for instance, towards placing students at district hospitals for longer periods of time, rather than weeks-long rotations, he says.
“When students become part of the furniture at a hospital, they become better at facilitating, at critical thinking, problem solving, teamwork and collaboration,” Cooke says.
But making this kind of transformation in local training takes government funding and commitment. Students and doctors need to be attracted to the programme and need reasons to stay. But the money and resources to make this happen are simply not there – even as the Cuba training programme continues.
Cooke adds: “There hasn’t been definitive data on the NMFC programme. But even if the programme over 30 years has done well and met its targets, it’s not been cost efficient. What’s needed now is to leverage expertise and established partnership in different, more cost-effective ways like in research, health systems science and health science education.”
Up to three times more expensive?
Professor Shabir Madhi, dean of the faculty of health sciences at Wits, says the NMFC programme costs an estimated three times more than it costs to train a student in South Africa. This, he says, should be enough reason for a beleaguered health department like Gauteng’s to stop sending students to Cuba.
He also says: “Government is aware that it simply can’t absorb the number of medical graduates being produced.” Madhi says some trainee doctors are sitting at home while others trying to finish specialisations are being derailed.
Broadly, he pins the blame on the mismanagement of resources, including the department underspending R590 million on the National Tertiary Service Grant meant to subsidise specialised medical treatment at tertiary hospitals.
Madhi says universities have worked hard to close the gaps identified by the NMFC programme 30 years ago, but now student doctors are being let down by government not playing its role.
“Across the universities, there’s been a complete overhaul of the curriculum to be focused on primary healthcare. Students are also getting community exposure as early as first-year training,” he says.
He says that when it comes to admissions, the majority of students entering medical schools across the country are now Black South Africans, and additional changes have been made to the selection process. “We used to have a race quota, but in further revisions, we have introduced criteria that focuses on the socio-economic component, with 40% of the admissions coming from students in quintile 1, 2 and 3 schools [no-fee public schools],” he adds.
South Africa has 11 medical schools, with the most recent addition of the North West University – specifically focussed on rural health – and the University of Johannesburg in the pipeline to join the list. So the number of doctors being trained and graduating is increasing. Madhi estimates the total number being trained is above 900 per year for Gauteng alone.
The bottleneck of getting doctors into clinics and hospitals, he maintains, is not a shortage of doctors, but government’s inability to pay doctors’ salaries or to create functioning, well-resourced workplace environments.
‘You can’t put a price on that’
For Dr Sanele Madela, the ongoing challenges cannot detract from the goal to get doctors into communities – including through the NMFC programme. Today, he’s the health attaché at the Havana Mission for the NMFC training programme. Madela was also at one time a schoolboy with a dream of becoming a doctor.
Growing up in Dundee in KwaZulu-Natal, he remembers almost never seeing a doctor in his community. “Then when we did see a doctor, it was a white person or an Indian person and they never spoke our language – a nurse would have to translate,” says Madela who was part of the 2002 NMFC intake.
The six years abroad, he says, exposed him to very different reasons for becoming a doctor.
“When people finish medical school, they say thank God it’s over, but in Cuba people say thank God for the knowledge and information so they can give back to their country,” he says.
When Madela got back to South Africa, his journey eventually led him to work in Dundee district hospital. It was the same hospital where his mother had worked as a cleaner.
The NMFC programme, Madela says, still plays a vital role because of its objective to get more doctors into rural and township areas – “and you can’t put a price on that”, he adds, responding to criticism over the programmes comparatively high costs.
“We are used to seeing the NMFC programme from the point of view of adding human resources, but it’s also about the impact it makes for a community,” he says. It’s the impact of a community finally getting their own doctor. His argument is that, thanks to the NMFC programme, he got to be that person for his community.
By Matimba Ngobeni, Country Head: Value & Access, Novartis South Africa
28 July 2025, Johannesburg South Africa – South Africa’s healthcare system stands at a crossroads. Despite the promise of progress outlined in the Budget Speech and the Presidential Health Compact, the reality on the ground reveals persistent and growing barriers to accessing innovative medicines.
Economic pressures, funding constraints, and infrastructure gaps continue to undermine equitable healthcare delivery, particularly for vulnerable communities. What’s more, recent international developments—such as U.S. President Donald Trump’s cuts to funding that supported healthcare initiatives in South Africa—threaten to exacerbate these challenges, potentially limiting access to life-saving advanced therapies.[1]
Economic pressures
The cost of advanced therapies remains out of reach, and the structural inequalities in our healthcare system persist. While top-tier medical plans still provide access to advanced medicines, we are seeing a shift. Patients are moving to lower-tier plans or into the public system, simply because they cannot afford more. And with that shift, their access to advanced therapies disappears. [2]This is not a uniquely South African problem.
Globally, we see the same story repeat: private healthcare becomes a fortress that only those who can pay the toll may enter. Everyone else is left to rely on an overburdened public system, strained by funding shortfalls, infrastructure gaps, and critical workforce shortages. The public healthcare system, already overburdened, struggles to absorb this increased demand. Rising healthcare costs combined with limited household budgets create a perfect storm where affordability becomes the biggest barrier to accessing cutting-edge treatments.
Funding constraints and infrastructure challenges
Both private and public sectors face severe funding constraints. Innovative medicines, especially advanced therapies, come with high price tags that strain budgets and limit availability. At the same time, infrastructure and skills gaps hinder the effective delivery of these treatments. Investments in healthcare infrastructure, workforce training, and data management are urgently needed to support the growing demand for advanced therapies.
While it may seem like all hope is lost, the Presidential Health Compact offers a promising framework aimed at transforming South Africa’s healthcare landscape through infrastructure development and improved data surveillance[3]. However, it stops short of directly addressing access to innovative medicines. This gap underscores the need for stronger collaboration between public and private stakeholders to ensure that patients do not bear the financial burden alone.
Towards equitable access: Collaboration is imperative
Another way forward is through a robust, transparent Health Technology Assessment (HTA) process, where medicines are evaluated not only on their cost but on their ability to save lives, improve quality of life, and reduce the long-term burden on the health system.
Inclusive HTAs, where payers and pharmaceutical companies work together, are essential for reimagining access to advanced therapies. If we only look at the upfront cost of innovation, we miss the bigger picture of societal value.
Globally, risk-sharing models and outcome-based pricing agreements are helping bridge the affordability gap[4]. South Africa could benefit from more flexible legislation to enable these models, ensuring that innovation doesn’t remain locked behind prohibitive price tags.
South Africa’s healthcare future depends on what we choose to prioritise: short-term financial gains or long-term societal wellbeing. Too often, systems have been designed around protecting profits rather than protecting lives. Healthcare should never be a luxury. Yet in South Africa, and across much of the world, the reality is stark: exclusion is the norm, not the exception.
If we want a future where access to life-saving medicines is a reality for all, we need to break down the barriers of affordability, infrastructure, and policy inertia. And we need to do it together — governments, healthcare companies, funders, and civil society — because lives are at stake.
All hope is not lost. But we cannot wait for crisis to be our catalyst. The time for bold, collaborative action is now.
**About Novartis:**
Novartis is an innovative medicines company. Every day, we work to reimagine medicine to improve and extend people’s lives so that patients, healthcare professionals and societies are empowered in the face of serious disease. Our medicines reach more than 250 million people worldwide.
Novartis South Africa (Pty) Ltd, Magwa Crescent West, Waterfall City, Jukskei View, 2090. Co. Reg. No. 1946/020671/07. Tel. No. +27 (0) 11 347 6600.
Disclaimer: The presentation may include data on formulations, products, indications, and dosages not yet approved by the South African Health Products Regulatory Authority. This information is not intended to be promoting nor recommending any formulation, indication, dosage, or other claim not covered in the approved Professional Information. Novartis South Africa (Pty) Ltd recommends the use of their products in accordance with the locally approved Professional Information. Views and opinions of speakers do not necessarily reflect those of Novartis.
#InsideTheBox is a column by Dr Andy Gray, a pharmaceutical sciences expert at the University of KwaZulu-Natal and Co-Director of the WHO Collaborating Centre on Pharmaceutical Policy and Evidence Based Practice. (Photo: Supplied)
By Andy Gray
For over 20 years, the law has required that the Minister of Health issues regulations to govern the advertising of medicines in South Africa, but as yet no such regulations are in place. In his latest #InsideTheBox column, Dr Andy Gray considers what this means for the marketing of medicines in the country.
Anyone who has travelled to the United States will have been struck by the extent to which medicines, both those requiring a prescription and those that can be bought by consumers without a prescription, are advertised on television.
The situation in South Africa is quite different. While there are many advertisements for medicines shown on local television stations, only some are specific about the proprietary (brand) name of the medicine and its indications. Other advertisements focus instead on the indication (the reason for using the medicine), but do not identify it by name. Instead, viewers are urged to approach their pharmacies or medical practitioners. At a different time, an advertisement may be flighted which identifies a medicine, its strength, pack size and perhaps price, but provides no information about what the indication for the medicine is.
To what extent does this represent meaningful and justified regulatory control over pharmaceutical marketing?
Only two countries with effective medicines regulatory systems allow prescription-only medicines to be advertised directly to the consumer, these being the United States and New Zealand. Other countries, including South Africa, restrict the advertising of prescription-only medicines to the health professionals who can prescribe or dispense them. One of the key justifications for this restriction on the ability of the pharmaceutical industry to market their products is that direct-to-consumer advertising may result in more inappropriate prescribing, when prescribers are under pressure from patients demanding medicines they have seen advertised. Short television advertisements are unlikely to be able to convey a balanced account of the potential benefits and harms of medicines, especially those that are new to the market.
South African law contains an interesting variant to regulation in this area. General Regulation 42 issued in terms of the Medicines and Related Substances Act, 1965, allows medicines containing substances in Schedules 0 and 1 to be advertised to the public, but requires that those containing substances in Schedules 2 to 6 to be advertised “only for the information of pharmacists, medical practitioners, dentists, veterinarians, practitioners, and other authorised prescribers” or “in a publication which is normally or only made available” to such persons. While Schedule 0 medicines can be bought in any retail outlet, Schedule 1 and 2 medicines can only be obtained from a pharmacy, but not self-selected from a shelf. The justification for that particular cut-off is difficult to trace in any policy document. An amendment to the regulation was published for comment in February 2023, but the final regulation has yet to be issued by the Minister of Health.
‘Failure to follow through’
The fundamental problem, however, lies in a failure to follow through on the legislation previously passed by Parliament. Section 18C of the current version of the Medicines and Related Substances Act, 1965, contains a prescriptive instruction to the Minister. “The Minister shall, after consultation with the relevant industries and other stakeholders, make regulations relating to the marketing of medicines, medical devices or IVDs and such regulations shall also provide for Codes of Practice for relevant industries,” it states. From 2003 to 2017, the section read: “The Minister shall, after consultation with the pharmaceutical industry and other stakeholders, make regulations relating to the marketing of medicines, and such regulations shall also provide for an enforceable Code of Practice.” The expansion of the remit, to include medical devices and in vitro diagnostics (IVDs) was added by Parliament in 2008, but only took effect in 2017.
The wording is peremptory – the Minister “shall” – which leaves no room for delay. While the word “enforceable” has been removed, the very intent of a regulation is that it should be enforced. That no regulations have been forthcoming in more than 20 years is an extraordinary failure of governance.
That failure is compounded by another act of omission. Section 18A of the Act states: “No person shall supply any medicine, medical device or IVD according to a bonus system, rebate system or any other incentive scheme.” The law also enables the Minister to “prescribe acceptable and prohibited acts” in this regard, in consultation with the Pricing Committee. No final regulations have been issued since 2017. The Pricing Committee is established to advise the Minister on matters relating to the pricing of medicines, such as the annual maximum increase and the dispensing fees charged by pharmacists and licensed dispensing practitioners.
It is already an offence, in terms of section 29 of the Act, for any person to make “any false or misleading statement in connection with any medicine, Scheduled substance, medical device or IVD”. Regulation 42 also states: “No advertisement for a medicine may contain a statement which deviates from, with or goes beyond the evidence submitted in the application for registration of such medicine with regard to its safety, quality or efficacy where such evidence has been accepted by the Authority in respect of such medicine and incorporated into the approved information of such medicine”.
While these two provisions may prevent false or misleading advertising, they are limited in their scope. In particular, since no complementary medicines are yet registered by the South African Health Products Regulatory Authority (SAHPRA), none have an approved professional information (previously known as a package insert) or a patient information leaflet.
Industry self-regulation
The pharmaceutical and medical devices industries have not been idle during this period of government inaction. A non-profit, self-regulatory body, the Marketing Code Authority (MCA), has developed a Code of Marketing Practice, drawing on international guidelines. This code provides for sanctions when rules are broken, following adjudication of a complaint. Fines of up to a maximum of R500 000 can be levied for severe or serious offences, which would, for example, pose “safety implications for patients”.
However, as a self-regulatory body, the MCA cannot require membership by any licensed manufacturer. It means that those manufacturers which are not members of the MCA are not bound by the Code and cannot be sanctioned. The MCA therefore advocates that compliance with a Code should be a condition to get a license to operate as a manufacturer. The MCA has also responded to draft regulations on perverse incentives.
At a time when deliberate disinformation is being disseminated from many quarters, including from government authorities previously considered to be reliable, a weakened regulatory system cannot simply be allowed to stagger along, in defiance of the express instructions of the legislature. Public safety demands an effective regulatory mechanism to proactively examine pharmaceutical marketing, across all media, the ability to take meaningful action where transgressions are identified, and an even playing field for all actors.
*Dr Gray is a Senior Lecturer at the University of KwaZulu-Natal and Co-Director of the WHO Collaborating Centre on Pharmaceutical Policy and Evidence Based Practice. This is part of a new series of #InsideTheBox columns he is writing for Spotlight.
Disclosure: Gray is a member of South Africa’s National Essential Medicines List Committee and co-chairs its Expert Review Committee.
Note: Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.