
How an Anti-inflammatory Helps the Heart After a Heart Attack

Every day, thousands of people worldwide suffer a heart attack, often leading to lasting damage to the heart muscle. New research from the University of Oslo suggests that targeting inflammation in the body helps protect the heart and improve recovery after a heart attack.
“In a small country like Norway alone, we see around 11 000 heart attacks every year,” says postdoctoral fellow Camilla Huse at the Research Institute for Internal Medicine, at University of Oslo and Oslo University Hospital. “Forty heart attacks every day is a lot.”
Fortunately, modern treatments are so effective that most patients survive a heart attack.
Inflammation damages the heart
However, a heart attack triggers a strong inflammatory reaction in the body. While this inflammation is part of the body’s natural response, it also causes damage to the heart muscle during a heart attack.
Such injury can lead to poorer health, a reduced quality of life and fewer working years for those affected. It also increases the risk of developing new heart diseases later in life.
So, how can we protect the heart during a heart attack?
Can anti-inflammatory medication improve heart attack treatment?
For some time, the researchers at the University of Oslo and Oslo University Hospital have been studying a medicine that blocks the effect of a substance that stimulates inflammation, a substance called IL-6. Previously, they have shown that administering this medicine in addition to established treatment for heart attacks has promising results: the patients suffered less damage to their hearts.
“This could be a new way of treating patients,” senior researcher Tuva Børresdatter Dahl says, and continues:
“To move forward with treatment, we need to understand what happens in the body when we block inflammation. Which processes inside the cells are affected by the medicine being tested? Which are not? And how does this relate to damage to the heart and to the improved recovery of the patient?”
How to investigate the effect of the treatment
The researchers conducted a study in which they examined the immune cells of 200 patients with STEMI. STEMI is a type of heart attack where the risk of serious complications is high.
The patients were randomly divided into two groups. Half of them received the anti-inflammatory medication, blocking the IL-6 signal, while the other half received a placebo, i.e. a treatment without any active ingredient.
The researchers then monitored how the treatment affected the immune cells in the blood. They also measured how much of the heart muscle was damaged.
Monocytes at the front line of our immune system
The researchers found that the treatment affects a type of immune cell called monocytes, which play an important role in all forms of inflammation.
“The monocytes are right at the front line of our immune system. They are among the first immune cells to arrive to the heart when a heart attack occurs,” Huse says.
Shortly after a heart attack, a strong inflammatory mobilisation occurs in the body, and monocytes flow to the heart muscle.
“The monocytes help to repair and clean up after a heart attack. But they can often get a little too eager. Thus, they also contribute to worsening the damage to the heart muscle after the heart attack,” she explains.
Reduced inflammation linked to better heart attack recovery
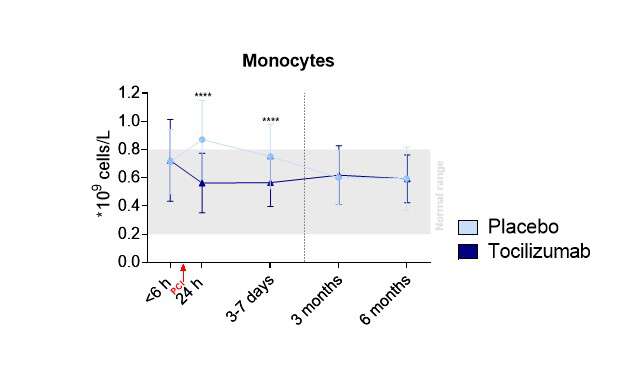
The study showed that the patients who received the anti-inflammatory medication had fewer monocytes in their blood shortly after the heart attack.
Normally, having high levels of these immune cells soon after a heart attack are linked to more heart damage and worse outcomes for the patients. Lower levels, on the other hand, are associated with less damage to the heart and better healing.
The researchers also found that the medicine made the cells in the heart muscle more resistant to damage, so that more heart cells survived the heart attack.
Changing immune cell behaviour to protective
As a result of the treatment, the way the monocytes behave was also changed.
“The function of the monocytes changed, from being more harmful to becoming more protective. The “good” functions of the immune cells were strengthened,” Huse says.
“We believe that those functions are the reason why patients suffer less damage after the heart attack. The heart is helped towards recovery,” she adds.
The study also showed another important effect: mechanisms that normally draw inflammatory cells into the damaged area were prevented in the patients who received the medicine.
What could this mean for heart attack patients in the future?
The research provides new insight into how inflammation affects the heart during a heart attack, and how this treatment can protect the heart from damage following STEMI.
This creates an opportunity for anti-inflammatory drugs to become part of a standard treatment for heart attacks and give patients a better life afterwards.
“The study shows that monocytes play an important role in the development of heart attacks. We believe that affecting these cells, which the blocking of IL-6 does, is beneficial. It could be a new and important additional treatment for these patients,” Dahl points out.
Why mechanism-focused research matters
The researcher believes that more such in-depth studies are needed when new medicines are tested.
“They provide a better understanding of the mechanisms behind illness and how the medicine affects the body. It doesn’t just tell us whether a treatment has worked, but also why or why not.
“Such knowledge can make new treatment options possible. This type of research should therefore be prioritised in future clinical studies,” Dahl says.
Reference
Huse C, Murphy SL, Yang K, Balzer NR, Stokke MK, Anstensrud AK, et al. The effects of interleukin-6-receptor inhibition on monocytes in STEMI: a substudy of the ASSAIL-MI trial. EBioMedicine. 2025. doi:10.1016/j.ebiom. 2025.105960
By Julie Nybakk Kvaal, Institute of Clinical Medicine
Source: University of Oslo




