Anaemia detected in healthcare is associated with an increased risk of both cancer and higher mortality. This is shown in a new population-based study from Karolinska Institutet, published in BMJ Oncology. The findings may help guide clinical follow-up of patients with anaemia in routine care.
Anaemia is common among patients in healthcare and is defined by haemoglobin levels below the normal range. In this study, the researchers analysed the association between newly detected anaemia and the risk of cancer and mortality, and examined whether different types of anaemia, classified by the size of red blood cells, play a role.
The study is based on register data from the Stockholm Early Detection of Cancer Study (STEADY‑CAN) and includes almost the entire adult population of Stockholm County between 2011 and 2021. In total, just over 190 000 adults with newly detected anaemia were included, along with an equal number of age- and sex-matched individuals without anaemia. All participants were over 18 years of age and cancer-free at study entry.
The participants were followed for up to 18 months after anaemia was detected. During this period, 6.2 per cent of men and 2.8 per cent of women with anaemia developed cancer. The corresponding figures among individuals without anaemia were 2.4 per cent and 1.1 per cent, respectively. Mortality was also higher in the group with anaemia.
“We found that both the risk of cancer and the risk of death are highest during the first months after anaemia is detected, but that the increased risk persists later during follow-up as well,” says Elinor Nemlander, researcher at the Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, and first author of the study.
Type of anaemia matters
The study also shows that the type of anaemia is important. Individuals with small red blood cells, known as microcytosis, had a particularly high risk of cancer, especially cancers of the gastrointestinal tract and the haematopoietic system. By contrast, individuals with large red blood cells, macrocytosis, showed a stronger association with increased mortality, but not with cancer to the same extent. Red blood cell size is measured using the laboratory value MCV, which is included in routine blood tests.
“Our findings suggest that anaemia may be a sign of underlying disease rather than a condition in its own right. Blood tests that are already part of routine care can provide important information about which patients need closer follow-up,” says Elinor Nemlander.
People with long COVID are at increased risk of developing cardiovascular disease, according to a new study from Karolinska Institutet published in eClinicalMedicine. The results show that the risk of conditions such as cardiac arrhythmias and coronary artery disease is higher even among those who were not hospitalised during the acute infection.
Long COVID has become an increasingly significant health problem worldwide, and a growing number of studies suggest that the condition can lead to secondary cardiovascular diseases. To date, research has mainly focused on people who were hospitalised, whilst the risks for those who stayed at home or were treated at a GP are less well known. In the current study, the researchers investigated how often major cardiovascular events occur in these individuals compared with those without the diagnosis.
Of the just over 1.2 million people aged between 18 and 65 included in the study, around 9,000 had been diagnosed with long COVID, corresponding to 0.7 per cent. Two-thirds of them were women. People who had previously had cardiovascular disease or been hospitalised for COVID-19 were excluded from this group.
During the follow-up period of around four years, people with long COVID were more likely to suffer from cardiovascular disease: 18.2 per cent of women and 20.6 per cent of men experienced some form of cardiovascular event, compared with 8.4 per cent of women and 11.1 per cent of men in the group without long COVID.
When the researchers then adjusted the results for factors such as age, socio-economic status and other known risk factors, the differences remained. Women with long COVID had just over twice the risk of receiving a cardiovascular diagnosis compared with women without long COVID. Men had approximately a third higher risk.
“We found that cardiac arrhythmias and coronary artery disease were more common among both women and men with long COVID. In women, there was also an increased risk of heart failure and peripheral vascular disease. However, no clear association was found between long COVID and stroke,” says lead author Pia Lindberg, a nurse and PhD student at the Department of Medicine, Solna, Karolinska Institutet.
Need to be monitored more systematically
As many people with long COVID never required hospitalisation during their acute infection, there is a risk that secondary conditions may be missed, says Pia Lindberg, pointing out that the results suggest these patients may need to be monitored more systematically.
”Our results show that long COVID can be a risk factor for cardiovascular disease, even in younger people who were previously healthy. This underlines the need for structured follow-up that takes gender differences into account, particularly as cardiovascular disease in women often presents with more diffuse symptoms that can make diagnosis more difficult”, concludes Pia Lindberg.
By James White, Director: Sales and Marketing at Turnberry Management Risk Solutions
Many South Africans assume that belonging to a medical scheme means their hospital treatment will be fully covered. In practice, this is often not the case. Patients are increasingly encountering co-payments, specialist shortfalls and benefit sub-limits that leave them responsible for part of the bill. This happens because medical schemes pay according to their own tariff structures, while specialists often charge significantly more than those tariffs, sometimes as much as 500% of the scheme rate.
The difference between the scheme tariff and the provider’s invoice is then billed to the patient, and it can amount to tens of thousands of Rands. Gap cover exists specifically to address these shortfalls by covering the gap between what medical schemes pay and what healthcare providers charge, offering peace of mind and greater financial certainty.
Healthcare costs are rising faster than household incomes
Medical inflation in South Africa has consistently outpaced general inflation. While many employees receive annual increases of around four or five percent, healthcare costs often rise by nine or ten percent. Hospital tariffs, specialist fees and the cost of advanced medical technology continue to increase each year.
Medical schemes therefore face a difficult balancing act: keeping contributions affordable while managing rising provider costs. To do this, schemes increasingly rely on co-payments, tighter benefit limits and reimbursement based on scheme tariffs. For members, this means that belonging to a medical scheme does not always guarantee that every medical expense will be fully covered.
The shortfall between tariffs and specialist fees
One of the most common out-of-pocket expenses occurs when a healthcare provider charges more than the scheme rate. Medical schemes reimburse treatment according to their own tariffs, while specialists may charge several times that amount. This can create confusion for members, because policies often state that they pay “100% of the scheme rate”. In practice, this means the scheme pays up to its tariff limit, not the full amount charged by the provider.
From a gap cover perspective, this tariff shortfall accounts for the majority of claims. In many cases it represents roughly 78% to 80% of claims, making it one of the most common funding gaps patients experience.
Co-payments and sub-limits add further pressure
Shortfalls are not the only challenge patients face – medical schemes increasingly rely on co-payments and sub-limits to manage rising healthcare costs.
A co-payment is a fixed amount that the member must pay before treatment takes place. Depending on the procedure and scheme rules, these amounts can range from around R5,000 up to R30,000, and in some cases even higher. For many households, being asked to produce this amount upfront can create significant financial strain.
Sub-limits can create a similar problem. Even when a procedure is covered, schemes may limit how much they will pay for certain treatments, scans or specialist services. Once the limit is reached, the remaining cost falls to the patient.
Why adviser education matters
Because the system is complex, many clients only discover these gaps when they receive a bill after treatment. They assume their medical aid will cover the full cost of care, only to find that co-payments, benefit limits or specialist shortfalls still apply.
This is why it is important for advisers to explain clearly how medical schemes pay claims, particularly the difference between scheme tariffs and provider fees. When clients understand how these shortfalls arise, the role of gap cover becomes easier to understand. Rather than being seen as an optional extra, gap cover becomes part of the overall structure of healthcare cover alongside medical aid.
Understanding your healthcare cover before you need it
Healthcare funding in South Africa is unlikely to become less complex in the near future. As costs continue to rise, it is essential to understand how your medical scheme operates and where potential shortfalls may arise.
Many people only learn how their cover works when a claim is processed and an unexpected bill appears. Understanding the difference between scheme tariffs, provider fees, co-payments and benefit limits can help prevent these surprises.
Gap cover plays an important role in addressing these shortfalls by covering the difference between what medical schemes pay and what healthcare providers charge. Speak to a broker about what your medical aid covers, where shortfalls may occur, and how gap cover can help protect you from unexpected medical bills.
Turnberry Management Risk Solutions (Pty) Ltd is an authorised Financial Services Provider (FSP no. 36571). Underwritten by Lombard Insurance Company, an Authorised Financial Services Provider (FSP 1596) and Insurer conducting non-life insurance business.
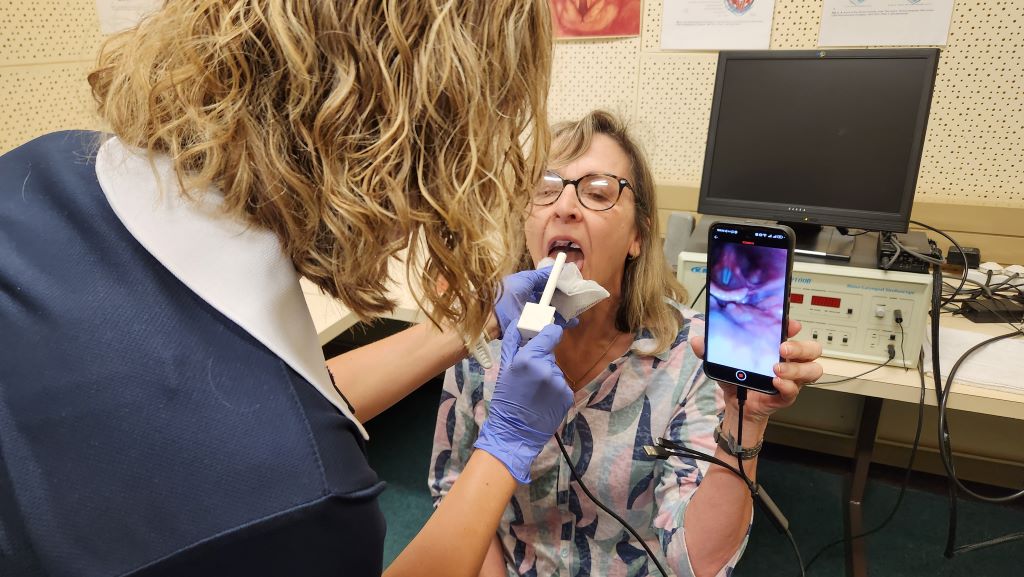
Dr Maria du Toit takes a close-up look at vocal cords, capturing high-resolution images and video using widely available mobile technology. Traditionally, this type of examination requires expensive equipment and specialist doctors, making it difficult to access in many parts of South Africa
Ahead of World Voice Day on 16 April, researchers at the University of Pretoria (UP) are inviting the public to take part in free voice checks using a new, locally developed device that could significantly expand access to vocal health services across South Africa.
The groundbreaking, low-cost, smartphone-compatible device, which is currently being tested as part of ongoing research, enables clinicians and trained users to take a close-up look at the voice user’s vocal cords by capturing high-resolution images and video using widely available mobile technology. Traditionally, this type of examination – known as laryngoscopy – requires expensive equipment and specialist doctors, making it difficult to access in many parts of South Africa.
“Your voice is something you use every day – whether for work, social interactions, or simply being heard. Yet many people ignore early warning signs of vocal problems,” says Professor Jeannie van der Linde, who is leading the research team and is Head of UP’s Department of Speech-Language Pathology and Audiology in the Faculty of Humanities.
Voice disorders are more common than many people realise. Prof Van der Linde adds: “International estimates suggest that up to one in five people will experience a voice problem at some point in their lives, with higher risk for those who rely heavily on their voices for work, such as teachers, healthcare workers and call centre agents. Despite this, access to specialised diagnostic services remains limited, particularly outside major urban centres.”
The research and device are part of a broader effort to rethink how vocal health services are delivered in South Africa. “Our aim was to develop a solution that is more portable, more affordable and easier to integrate into different healthcare contexts,” says Dr Maria du Toit, a Lecturer in Speech-Language Pathology and member of the research team.
“Many people ignore early signs like hoarseness or vocal fatigue, often because they don’t have easy access to assessment services,” Dr Du Toit says. “If we can identify these issues earlier, we can intervene sooner and potentially prevent more significant problems from developing.
The development of the device forms part of ongoing efforts within the department to explore how mobile anddigital technologies can be used to increase the availability of vocal health assessment and care.
Dr Roxanne Malan, a postdoctoral fellow, speech therapist and research team member, highlights the importance of designing technology that balances functionality with affordability and ease of use. “We wanted to ensure that the device is not only clinically useful but also practical in a range of settings, including those withlimited resources,” she says. “The goal is to make vocal health screening more widely available without compromising on quality.”
The technology, which has not been named yet, is being developed at UP and is currently undergoing testing to compare its performance with gold-standard laryngoscopy. “We started feasibility testing in June 2025 and preliminary tests have been very positive, demonstrating that the device is usable and produces high-quality images of the relevant structures,” Dr Malan says. “It consists of a low-cost, off-the-shelf borescope – typically used industrially – adapted with a 3D-printed handle to ensure optimal placement of the scope in the patient’s mouth, as well as the correct angle for visualisation. We have also assessed its safety for human use and its ability to be properly disinfected.”
In addition to testing the device, the World Voice Day initiative seeks to increase general awareness about theimportance of vocal health. “Your voice is central to how you communicate, work and engage with others,” Dr DuToit says. “Taking care of it should be seen as an essential part of overall health, not something to think aboutonly when there is a problem.”
Dr Malan says the team’s vision is for the scope to be readily available as a screening device in public hospitalsand clinics all over South Africa and other low- and middle-income countries. “But we still foresee numerousphases of testing to ensure that it can be used by a range of healthcare professionals, and that it makes asignificant difference in the target healthcare sectors. We will name and launch it at a stage when this has beendone.”
Dr Du Toit says members of the public can support the research by booking their free voice health check. “Byattending, you’re not only taking care of your own vocal health – you’re helping researchers develop solutionsthat could make voice care more easily available to thousands of people who currently don’t have access tothese services.”
Event details: Members of the public are invited to take part in free voice checks on World Voice Day, 16 April 2026, at the Department of Speech-Language Pathology and Audiology at the University of Pretoria’s Hatfield Campus.
Participants will have the opportunity to learn more about their vocal health and contribute to research that aims to make voice care more accessible across South Africa.
Who should consider a voice check?
This free check is especially recommended for:
● Teachers and lecturers
● Singers and performers
● Healthcare workers
● Clergy and public speakers
● Call centre workers
● Anyone who uses their voice extensively
You should also consider attending if you:
● frequently experience hoarseness or voice changes;
● feel your voice tires easily;
● have ongoing throat discomfort when speaking; and/or
● simply want reassurance that your voice is healthy.
Findings suggest lifelong beta-blockers may be unnecessary in some patients
Human heart. Credit: Scientific Animations CC4.0
Among stable, relatively low-risk patients who had previously suffered a heart attack, discontinuing beta-blockers after at least one year was found to be non-inferior, or comparable, to continuing beta-blockers in terms of death, another heart attack or hospitalisation for heart failure, according to a study presented at the American College of Cardiology’s Annual Scientific Session (ACC.26).
Beta-blockers, which lower heart rate and blood pressure by inhibiting adrenaline and other hormones, have long been a mainstay of treatment to reduce the likelihood of subsequent cardiac events following a heart attack. However, many studies confirming their benefits were conducted decades ago, when procedures and medications for secondary prevention were more limited than they are today. More recent studies suggest the benefits of beta-blockers may vary depending on the overall health of a patient’s heart.
“In appropriately selected patients who survived a heart attack and do not have heart failure or left ventricular systolic dysfunction, routine continuation of beta-blockers indefinitely may not be necessary,” said Joo-Yong Hahn, MD, a cardiologist at Samsung Medical Center in Seoul, South Korea, and the study’s senior author. “In practice, for stable patients who are several years out from a heart attack, discontinuation can be considered through shared decision-making and with monitoring of blood pressure and heart rate. For patients with beta-blocker-related side effects – fatigue, dizziness, bradycardia, hypotension – the case for discontinuation is even stronger.”
The study evaluated 2,540 patients at 26 sites in South Korea between 2021 and 2024 who had no subsequent cardiac events after taking beta-blockers for at least one year following a heart attack. Participants’ average age was 63 years and 87% were men. At a median of 3.5 years following randomisation, the primary endpoint – a composite of all-cause death, recurrent heart attack or heart failure hospitalisation – occurred in 7.2% of those who discontinued beta-blockers and 9% of those who continued taking the medication. The results met the threshold for non-inferiority because of a lower rate of this composite endpoint in the group that stopped taking beta-blockers.
Discontinuation of beta-blockers was also found to be similar for secondary endpoints, including each of the components of the primary composite endpoint, new-onset atrial fibrillation, unfavourable changes in left ventricular function, changes in quality of life and serious adverse events.
“In current practice – where revascularisation rates are high and secondary prevention is strong – we expected that the incremental benefit of continuing beta-blockers indefinitely in stable patients might be small,” Hahn said. “We found that discontinuation did not worsen major outcomes, cardiac function or quality of life in this selected stable population.”
Since most study participants had been taking beta-blockers for several years before discontinuing, Hahn said that the results may not apply to patients who have been taking beta-blockers for a shorter amount of time. The study also does not definitively establish the earliest timepoint at which it is safe to stop taking beta-blockers.
The results were generally consistent across prespecified subgroups. However, women and patients with mildly reduced left ventricular ejection fraction made up a small proportion of the trial population, limiting the interpretation of results for these subgroups. In addition, the study was conducted only in South Korea, potentially limiting its generalisability to other areas of the world.
Hahn said future studies could help to clarify whether and when it is safe to discontinue beta-blockers among higher-risk groups, women and those with mildly reduced left ventricular ejection fraction and to better define the optimal timing of discontinuation. Pooled analyses across contemporary randomised trials could provide additional insights and help guide practice decisions. The researchers also plan to conduct further analyses to assess potential differences in health care costs.
The study was funded by the Patient-Centered Clinical Research Coordinating Center in the Ministry of Health and Welfare of the Republic of Korea.