In the analysis of data from the Health and Retirement Study, a nationally representative sample of older US adults, optimism was assessed using the validated Life Orientation Test-Revised in 9071 cognitively healthy individuals within 2 years of obtaining each person’s first measure of cognitive function. Dementia was assessed during up to 14 years of follow-up.
A 1-standard deviation increase in optimism was associated with a 15% lower risk of developing dementia, after adjusting for age, sex, race/ethnicity, education, depression, and major health conditions.
“Identifying optimism as a protective psychosocial factor highlights the potential value of optimism in supporting healthy aging,” the authors wrote.
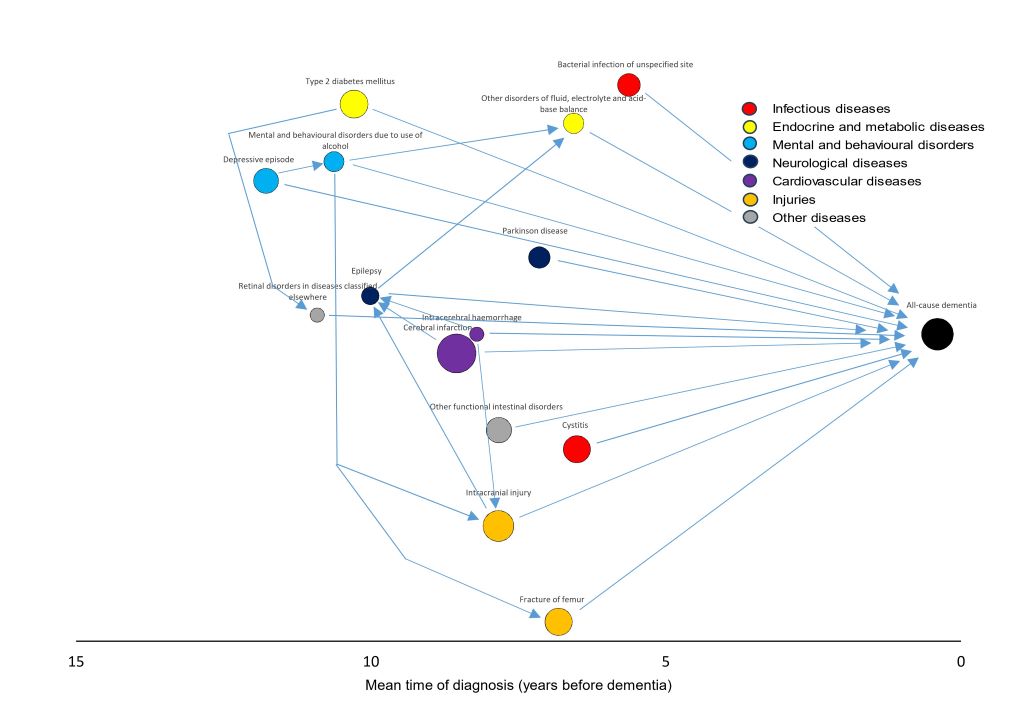
Finnish registry study finds that infections like cystitis and bacterial disease are linked to higher dementia risk independently of other coexisting conditions
Source: CC0
Severe infections increase the risk of dementia independently of other coexisting illnesses, according to a new study published March 24th in the open-access journal PLOS Medicine by Pyry Sipilä of the University of Helsinki, Finland, and colleagues.
Severe infections have been linked to an increased risk of dementia. However, it has been unclear whether this association is explained by other coexisting, non-infectious diseases that predispose people to both infections and dementia.
In the new study, researchers used nationwide Finnish health registry data covering more than 62 000 individuals aged 65 or older who were diagnosed with late-onset dementia between 2017 and 2020, along with more than 312 000 matched dementia-free controls. Taking a broad approach, they examined all hospital-treated diseases recorded during the previous twenty years, identifying 29 diseases that were robustly associated with increased dementia risk. Nearly half (47%) of dementia cases had at least one of the 29 identified diseases before their diagnosis.
Of those diseases, two were infections: cystitis (a urinary tract infection) and bacterial infection of an unspecified site. Among the non-infectious diseases, the strongest associations with dementia were seen for mental disorders due to brain damage or physical disease, Parkinson’s disease, and alcohol-related mental and behavioural disorders.
When the researchers then adjusted for all 27 non-infectious dementia-related diseases identified, the association between both infections and dementia remained largely intact. Less than one-seventh of the excess dementia risk among individuals with hospital-treated cystitis or bacterial infections was attributable to pre-existing conditions. The link between infections and dementia was even stronger for early-onset dementia (diagnosed before age 65), where five types of infection – including pneumonia and dental caries – were associated with elevated risk.
The study was limited by the lack of baseline cognitive assessments and clinical examination data before dementia diagnoses, as well as a lack of data on infection treatments.
“Overall, our findings support the possibility that severe infections increase dementia risk; however, intervention studies are required to establish whether preventing or effectively treating infections yields benefits for dementia prevention,” the authors say.
The authors add, “We found 27 diverse severe, hospital-treated diseases that were robustly associated with an increased risk of dementia. Two of these diseases were infections, namely urinary tract infections and unspecified bacterial infections.”
“In our study, dementia-related infections occurred on average 5 to 6 years before dementia diagnosis. Given that the development of dementia often takes years or even decades, these findings suggest that severe infections might accelerate underlying cognitive decline. However, as these findings were observational, we cannot exclude the possibility that some unmeasured confounding factors might also have affected our findings. Thus, we cannot prove cause and effect.”
“Ideally, intervention trials should examine whether better infection prevention helps reduce dementia occurrence or delay the onset of this disease.”
A new prospective cohort study by investigators from Mass General Brigham and colleagues analysed 131 821 participants from the Nurses’ Health Study (NHS) and Health Professionals Follow-Up Study (HPFS), finding that moderate consumption of caffeinated coffee (2-3 cups a day) or tea (1-2 cups a day) reduced dementia risk, slowed cognitive decline, and preserved cognitive function. Their results are published in JAMA.
“When searching for possible dementia prevention tools, we thought something as prevalent as coffee may be a promising dietary intervention – and our unique access to high quality data through studies that has been going on for more than 40 years allowed us to follow through on that idea,” said senior author Daniel Wang, MD, ScD, associate scientist with the Channing Division of Network Medicine in the Mass General Brigham Department of Medicine and assistant professor at Harvard Medical School. Wang is also an assistant professor in the Department of Nutrition at Harvard Chan School and an associate member at the Broad Institute. “While our results are encouraging, it’s important to remember that the effect size is small and there are lots of important ways to protect cognitive function as we age. Our study suggests that caffeinated coffee or tea consumption can be one piece of that puzzle.”
Early prevention is especially crucial for dementia, since current treatments are limited and typically offer only modest benefit once symptoms appear. Focus on prevention has led researchers to investigate the influences of lifestyle factors like diet on dementia development.
Coffee and tea contain bioactive ingredients like polyphenols and caffeine, which have emerged as possible neuroprotective factors that reduce inflammation and cellular damage while protecting against cognitive decline. Though promising, findings about the relationship between coffee and dementia have been inconsistent, as studies have had limited follow-up and insufficient detail to capture long-term intake patterns, differences by beverage type, or the full continuum of outcomes—from early subjective cognitive decline to clinically diagnosed dementia.
Data from the NHS and HPFS help to overcome these challenges. Participants repeated assessments of diet, dementia, subjective cognitive decline, and objective cognitive function and were followed for up to 43 years. Researchers compared how caffeinated coffee, tea, and decaffeinated coffee influenced dementia risk and cognitive health of each participant.
Of the more than 130 000 participants, 11 033 developed dementia. Both male and female participants with the highest intake of caffeinated coffee had an 18% lower risk of dementia compared with those who reported little or no caffeinated coffee consumption. Caffeinated coffee drinkers also had lower prevalence of subjective cognitive decline (7.8% versus 9.5%). By some measurements, those who drank caffeinated coffee also showed better performance on objective tests of overall cognitive function.
Higher tea intake showed similar results, while decaffeinated coffee did not – suggesting that caffeine may be the active factor producing these neuroprotective results, though further research is needed to validate the responsible factors and mechanisms.
The cognitive benefits were most pronounced in participants who consumed 2–3 cups of caffeinated coffee or 1–2 cups of tea daily. Contrary to several previous studies, higher caffeine intake did not yield negative effects – instead, it provided similar neuroprotective benefits to the optimal dosage.
“We also compared people with different genetic predispositions to developing dementia and saw the same results – meaning coffee or caffeine is likely equally beneficial for people with high and low genetic risk of developing dementia,” said lead author Yu Zhang, MBBS, MS, PhD student at Harvard Chan School and a research trainee at Mass General Brigham.
Eating cheese and cream with a high fat content may be linked to a lower risk of developing dementia. This is shown by a new large-scale study from Lund University. The researchers analysed the dietary habits of more than 27 000 people and linked these to the occurrence of dementia over a follow-up period of up to 25 years.
The debate about low-fat diets has long shaped our health advice and influenced how we view food and health. For several decades, fear of saturated fat and its link to cardiovascular disease has dominated. The MIND diet1 is a diet developed with the aim of reducing the risk of dementia. The diet includes protective foods such as vegetables, nuts, fruits, berries, whole grains, and fish, while cheese is one of the foods that should be limited.
Emily Sonestedt, researcher in nutritional epidemiology at Lund University in Sweden, and her colleagues, therefore wanted to investigate whether there was any link between dairy products and dementia. They collected dietary data from 27,670 people using the Malmö Diet Cancer population study, in which the participants respond about their dietary and cooking habits. The average age at the start of the study was 58, and the participants were followed for an average of 25 years, during which time 3,208 people developed dementia. The dementia diagnoses were obtained from the Swedish patient registry. For cases diagnosed up to 2014, additional validation studies were conducted in which dementia specialists reviewed medical records, brain scans, and cognitive test results.
After adjusting for lifestyle factors such as physical activity, diet, smoking, and alcohol consumption, the researchers found that people who ate 50 grams of cheese (with more than 20 percent fat) daily had a 13 percent lower risk of developing dementia than those who ate less than 15 grams daily. 50 grams is equivalent to about five regular slices of cheese. In total, about a quarter of the participants ate more than 50 grams or more daily.
”When we went on to look at specific types of dementia, we found that there was a 29 percent lower risk of vascular dementia in people who ate more full-fat cheese. We also saw a lower risk of Alzheimer’s disease, but only among those who did not carry the APOE e4 gene variant—a genetic risk factor for Alzheimer’s disease.”
The researchers also investigated the link between high-fat cream (30-40 percent fat) and dementia. People who consumed 20 grams or more daily had a 16 percent lower risk of dementia than those who did not consume any at all.
The results of the cheese studies support the link between vascular health and brain health.
”The updated dietary guidelines in Sweden from this year say that we can eat dairy products every day, preferably fermented varieties such as yogurt or kefir. Both we and other researchers have found in observational studies that fermented dairy products in particular may be linked to a slightly reduced risk of cardiovascular disease 2,” says Emily Sonestedt.
In previous studies3, the research team has seen links to vascular health, with cheese and fermented dairy products in particular protecting against cardiovascular disease.
”Although higher-fat cheese and cream were associated with a reduced risk of dementia, other dairy products and low-fat alternatives did not show the same effect. Therefore, not all dairy products are equal when it comes to brain health. The few studies that have investigated this have found a correlation with cheese, so more research is needed to confirm our results and investigate whether certain high-fat dairy products really do provide some protection for the brain.”
The MIND diet stands for Mediterranean–DASH Intervention for Neurodegenerative Delay – a combination of the Mediterranean diet and the DASH diet. DASH (Dietary Approaches to Stop Hypertension) is a diet developed primarily to lower high blood pressure and improve cardiovascular health.
The time to carry out diagnostic MRI scans for dementia can be cut to one third of their standard length, according to a new study led by UCL researchers.
The findings, published in Alzheimer’s & Dementia, have been described as a step towards ending ‘the postcode lottery in dementia diagnosis’. Shorter scans would be easier and more comfortable for patients and also enable more people to be scanned at a lower cost. The team behind the study say this could at least double the number of dementia scans able to be done in one day.
Senior author Professor Nick Fox, Director of the UCL Dementia Research Centre at the UCL Queen Square Institute of Neurology, said: “As more treatments that can slow or change the course of dementia are being developed, it’s important to make sure MRI scans are available to everyone. This is because people living with dementia often need an MRI scan as part of their diagnosis before they can access these treatments.
“To help make this possible, our team carried out the first study looking at how new imaging techniques – called parallel imaging – could speed up MRI scans in clinics. Their goal is to move closer to a future where every person with dementia can get a diagnosis through a scan.”
MRI scans often play a key role in an accurate dementia diagnosis, including ruling out other causes of symptoms and assisting in diagnosing the type of dementia. Emerging disease-modifying treatments such as lecanemab and donanemab also require an MRI scan before starting treatment and for safety monitoring during the course of treatment. Reducing the cost of scanning would contribute to lowering the total cost of delivering for such treatments.
The ADMIRA study (Accelerated Magnetic Resonance Imaging for Alzheimer’s disease), part funded by Alzheimer’s Society’s Heather Corrie Impact Fund, aimed to understand the reliability of fast MRI scans compared to standard-of-care clinical scans. The neurologists on the study were joined by co-authors from the UCL Hawkes Institute and the UCL Advanced Research Computing Centre in the faculty of Engineering.
The research team scanned 92 people in an outpatient setting where an MRI brain scan was planned as part of their routine clinical assessment. The accelerated scans were carried out and enhanced to increase the quality of the image using new scanning methods. Three neuroradiologists examined these scans, and weren’t aware if they were looking at fast or standard-of-care scans.
Co-author Professor Geoff Parker (UCL Hawkes Institute and UCL Medical Physics and Biomedical Engineering) said: “Our research has taken advantage of recent breakthroughs in scanner technology. Our task was to work out just how fast we could scan while maintaining image quality good enough for diagnosis.”
The team found that the quicker scans reduced time in the scanner by 63% and they were as reliable as the standard-of-care scans for diagnosis and visual ratings.
First author Dr Miguel Rosa-Grilo (UCL Queen Square Institute of Neurology) said: “We were confident that the new scan would prove non-inferior to the standard scan, given the high image quality – but it was remarkable how well it performed.”
Richard Oakley, Associate Director of Research and Innovation at Alzheimer’s Society, said: “Dementia is the UK’s biggest killer, but one in three people living with the condition haven’t had a diagnosis. An early and accurate diagnosis isn’t just a label, it’s the first step to getting vital care, support and treatment.
“While MRIs aren’t the only way to diagnosis dementia, very few people with concerns about their cognitive health are offered one as part of the diagnosis process, mainly because they are expensive and not widely available. These faster MRIs, which take less than half the time of standard scans, could help end this postcode lottery in dementia diagnosis, cut costs and potentially give more people access to them.
“MRI scans can be an uncomfortable and daunting experience for patients, so anything we can do to make it an easier process is really positive.
“So far, this shortened MRI scan has been tested at one specialist centre with one type of MRI scanner, so more research is needed to make sure this works across different types of scanners and a diverse range of people. We’re hugely encouraged by this progress and eager to see how it continues.”
The team will now build on their early results by making sure the approach works across different types of MRI machines, so it can benefit as many hospitals and clinics as possible.
Photo by Kampus Production: https://www.pexels.com/photo/a-man-in-blue-sweater-sitting-beside-man-in-white-long-sleeves-7551646/
Low cholesterol can reduce the risk of dementia, a new University of Bristol-led study with more than a million participants has shown.
The research, led by Dr Liv Tybjærg Nordestgaard while at the University of Bristol and the Department of Clinical Biochemistry at Copenhagen University Hospital – Herlev and Gentofte, found that people with certain genetic variants that naturally lower cholesterol have a lower risk of developing dementia.
Some people are born with genetic variants that naturally affect the same proteins targeted by cholesterol-lowering drugs, such as statins and ezetimibe. To test the effect of cholesterol-lowering medication on the risk of dementia, the researchers used a method called Mendelian Randomisation – this genetic analysis technique allowed them to mimic the effects of these drugs to investigate how they influence the risk of dementia, while minimising the influence of confounding factors like weight, diet, and other lifestyle habits.
By comparing these individuals to individuals without these genetic variants, the researchers were able to measure differences in the risk of dementia. They found reducing the amount of cholesterol in the blood by a small amount (one millimole per litre) to be associated with up to 80% reduction in risk of developing dementia for certain drug targets.
“What our study indicates is that if you have these variants that lower your cholesterol, it looks like you have a significantly lower risk of developing dementia,” said Dr Nordestgaard, who now works in the Department of Clinical Biochemistry at Copenhagen University Hospital – Bispebjerg and Frederiksberg hospital.
The results suggest that having low cholesterol, whether due to genes or medical treatment, can help reduce the risk of dementia. However, the study does not say anything definitive about the effect of the medicine itself.
One of the challenges is that dementia typically does not appear until late in life, and therefore research in the area typically requires a very long period of follow-up.
It is still not known exactly why high cholesterol can increase the risk of dementia, but one possible explanation proposed by Dr Nordestgaard is that high cholesterol can lead to atherosclerosis.
“Atherosclerosis is a result of the accumulation of cholesterol in your blood vessels,” Dr Nordestgaard said. “It can be in both the body and the brain and increases the risk of forming small blood clots – one of the causes of dementia.
“It would be a really good next step to carry out randomised clinical trials over 10 or 30 years, for example, where you give the participants cholesterol-lowering medication and then look at the risk of developing dementia,” Dr Nordestgaard added.
The study used data from the UK Biobank, the Copenhagen General Population Study, the Copenhagen City Heart Study, the FinnGen study, and the Global Lipids Genetics Consortium.
Any amount of alcohol consumption may increase risk of dementia, according to the most comprehensive study of alcohol consumption and dementia risk to date.
Led by the University of Oxford, Yale University, and the University of Cambridge, the research challenges previous suggestions that light-to-moderate drinking may have a protective effect against dementia. The study is published in BMJ Evidence-Based Medicine.
Alcohol consumption is widespread and is linked with an increased risk of many diseases. Heavy drinking has previously been linked to higher risk of dementia. The connection between moderate levels of drinking and higher risk of dementia was uncertain with some studies suggesting that moderate drinking may even reduce dementia risk. However, recent studies involving brain scans have shown that drinking alcohol even at low levels may increase the risk of dementia.
This study combined observational data from more than half a million participants in two large and diverse population studies: the US Million Veteran Program and UK Biobank to assess whether self-reported alcohol use was linked with risk of developing a broad range of types of dementia.
The researchers also investigated links between genetically-predicted likelihood of drinking alcohol and alcohol use disorder for more than 2.4 million participants in 45 individual studies. This approach helped the researchers overcome some of the difficulties in distinguishing correlation from causation.
Key findings:
Observational analyses seemed to support previous findings that current low and moderate drinking is associated with lower risk of dementia when compared with non-drinking and heavy drinking; however, some current non-drinkers were previously heavy drinkers, which could account for their increased dementia risk compared to consistently low drinkers;
Genetic analyses, however, revealed a continuously increasing trend of higher dementia risk with greater alcohol intakes, suggesting that any level of alcohol consumption increases the risk of dementia, with no evidence that drinking alcohol may have a protective effect;
A doubled increase in a person’s genetically-predicted risk of alcohol use disorder was associated with a 16% higher risk of dementia, while a three times higher increase in number of alcoholic drinks per week increased the risk of dementia risk by 15%;
The study also showed that people who later developed dementia reduced their alcohol intake before diagnosis, another explanation for prior findings of protective effects of alcohol, rather than true benefit.
Dr Anya Topiwala, Senior Clinical Researcher at Oxford Population Health, Consultant Psychiatrist, and lead author of the study, said ‘Our findings challenge the common belief that low levels of alcohol are beneficial for brain health. Genetic evidence offers no support for a protective effect – in fact, it suggests the opposite. Even light or moderate drinking may increase the risk of dementia, indicating that reducing alcohol consumption across the population could play a significant role in dementia prevention.’
Dr Stephen Burgess, Statistician at the University of Cambridge, said ‘The random nature of genetic inheritance allows us to compare groups with higher and lower levels of alcohol drinking in a way that allows us to make conclusions that untangle the confusion between correlation and causation. Our findings do not only hold for those who have a particular genetic predisposition, but for anyone who chooses to drink, our study suggests that greater alcohol consumption leads to higher risk of dementia.’
Dr Joel Gelernter, Professor at Yale University and senior author of the study, said ‘These results, which add to our understanding of the relationship between alcohol and dementia, have clinical implications – there was a time when medical knowledge seemed to support that light drinking would be beneficial to brain health, and this work adds to the evidence that this is not correct’.
This study adds to growing evidence that alcohol use, even at moderate levels, may have no safe threshold when it comes to brain health, reinforcing the case for preventive strategies that reduce alcohol consumption in the general population.
A new study suggests that physical frailty may contribute to the development of dementia. The study was published on September 17, 2025, in Neurology®, the medical journal of the American Academy of Neurology.
Physical frailty is defined as having three or more of these five symptoms: often feeling tired; little or no physical activity; slow walking speed; low grip strength; and unintentional weight loss.
“We’ve known that frailty is associated with a higher risk of dementia, but our study provides evidence that frailty may be an actual cause of dementia,” said study author Yacong Bo, PhD, of Zhengzhou University in China. “On the other hand, despite this new evidence, we can’t rule out the possibility that frailty is instead a marker of the early changes in the disease process.”
The study involved 489 573 people with an average age of 57 who were followed for an average of 14 years. A total of 4.6% of the participants met the definition for frailty, with three or more of the symptoms. Another 43.9% who had one or two symptoms were categorised as pre-frailty and 51.5% had no symptoms and were categorised as not frail.
During the study, 8900 people developed dementia. A total of 4.6% of those with frailty developed dementia, compared to 2.2% of those with pre-frailty and 1.3% of those without frailty. After researchers adjusted for other factors that could affect the risk of dementia, such as age, education level and physical activity, they found that the people who met the definition for frailty were nearly three times more likely to develop dementia than those who had no symptoms of frailty.
Those categorised as pre-frailty were 50% more likely to develop dementia. People with frailty who also had genes linked to dementia were nearly four times more likely to develop dementia than those without frailty or the genetic risk. The researchers also analysed the data and found evidence suggesting that frailty may potentially be a factor in causing dementia.
“These findings reinforce the importance of identifying and managing frailty as a strategy for preventing dementia,” Bo said.
Looking at the data from the other direction, the researchers found that dementia is unlikely to increase the risk of frailty. The researchers also looked at brain imaging and biological biomarkers and found that people with frailty were more likely to have changes in their brain structure related to dementia.
“These biomarkers may be a mechanism underlying the pathway from frailty to dementia,” said Bo. A limitation of the study was that four of the five symptoms of frailty were reported by the participants, so they may not have provided accurate information.
The brain has its own waste disposal system – known as the glymphatic system – that’s thought to be more active when we sleep.
But disrupted sleep might hinder this waste disposal system and slow the clearance of waste products or toxins from the brain. And researchers are proposing a build-up of these toxins due to lost sleep could increase someone’s risk of dementia.
There is still some debate about how this glymphatic system works in humans, with most research so far in mice.
But it raises the possibility that better sleep might boost clearance of these toxins from the human brain and so reduce the risk of dementia.
Here’s what we know so far about this emerging area of research.
Why waste matters
All cells in the body create waste. Outside the brain, the lymphatic system carries this waste from the spaces between cells to the blood via a network of lymphatic vessels.
But the brain has no lymphatic vessels. And until about 12 years ago, how the brain clears its waste was a mystery. That’s when scientists discovered the “glymphatic system” and described how it “flushes out” brain toxins.
Let’s start with cerebrospinal fluid, the fluid that surrounds the brain and spinal cord. This fluid flows in the areas surrounding the brain’s blood vessels. It then enters the spaces between the brain cells, collecting waste, then carries it out of the brain via large draining veins.
Scientists then showed in mice that this glymphatic system was most active – with increased flushing of waste products – during sleep.
One such waste product is amyloid beta (Aβ) protein. Aβ that accumulates in the brain can form clumps called plaques. These, along with tangles of tau protein found in neurons (brain cells), are a hallmark of Alzheimer’s disease, the most common type of dementia.
In humans and mice, studies have shown that levels of Aβ detected in the cerebrospinal fluid increase when awake and then rapidly fall during sleep.
But more recently, another study (in mice) showed pretty much the opposite – suggesting the glymphatic system is more active in the daytime. Researchers are debating what might explain the findings.
So we still have some way to go before we can say exactly how the glymphatic system works – in mice or humans – to clear the brain of toxins that might otherwise increase the risk of dementia.
In one experiment, a single night of complete sleep deprivation in healthy adults increased the amount of Aβ in the hippocampus, an area of the brain implicated in Alzheimer’s disease. This suggests sleep can influence the clearance of Aβ from the human brain, supporting the idea that the human glymphatic system is more active while we sleep.
This also raises the question of whether good sleep might lead to better clearance of toxins such as Aβ from the brain, and so be a potential target to prevent dementia.
How about sleep apnoea or insomnia?
What is less clear is what long-term disrupted sleep, for instance if someone has a sleep disorder, means for the body’s ability to clear Aβ from the brain.
Sleep apnoea is a common sleep disorder when someone’s breathing stops multiple times as they sleep. This can lead to chronic (long-term) sleep deprivation, and reduced oxygen in the blood. Both may be implicated in the accumulation of toxins in the brain.
Insomnia is when someone has difficulty falling asleep and/or staying asleep. When this happens in the long term, there’s also an increased risk of dementia. However, we don’t know the effect of treating insomnia on toxins associated with dementia.
So again, it’s still too early to say for sure that treating a sleep disorder reduces your risk of dementia because of reduced levels of toxins in the brain.
So where does this leave us?
Collectively, these studies suggest enough good quality sleep is important for a healthy brain, and in particular for clearing toxins associated with dementia from the brain.
But we still don’t know if treating a sleep disorder or improving sleep more broadly affects the brain’s ability to remove toxins, and whether this reduces the risk of dementia. It’s an area researchers, including us, are actively working on.
For instance, we’re investigating the concentration of Aβ and tau measured in blood across the 24-hour sleep-wake cycle in people with sleep apnoea, on and off treatment, to better understand how sleep apnoea affects brain cleaning.
This is an emerging field and we don’t yet have all the answers about the link between disrupted sleep and dementia, or whether better sleep can boost the glymphatic system and so prevent cognitive decline.
So if you are concerned about your sleep or cognition, please see your doctor.
New research in Diabetes, Obesity and Metabolism reveals that metformin, a medication traditionally prescribed to treat diabetes, is linked to lower risks of dementia and early death.
In the study by investigators at Taipei Medical University that included 452,777 adults with varying degrees of overweight and obesity, 35,784 cases of dementia and 76,048 deaths occurred over 10 years. Metformin users exhibited significantly lower risks of both dementia and all-cause death than nonusers.
The benefits of metformin were seen across all categories of overweight, obesity, and severe obesity, with 8–12% lower risks of dementia and 26–28% lower risks of death.
“Although our study results are promising for metformin’s effects on dementia and mortality, further research is required to explore the mechanisms involved,” said co-corresponding author Chiehfeng Chen, MD, PhD, MPH.