A recent analysis reveals that older adults with prior incarceration report worse physical and mental health than their peers, even if they were incarcerated in the distant past. The findings are published in theJournal of the American Geriatrics Society.
Among the 1318 US adults aged 50 years and older who responded to the Family History of Incarceration Survey, 21% had been incarcerated. Formerly incarcerated older adults were more likely to be men, non-Hispanic Black or “other” race/ethnicity, meet criteria for disability, be unmarried, and have lower income and education compared with those never incarcerated.
After adjusting for potentially confounding factors like demographics and socioeconomics, prior incarceration was associated with an approximately 90% higher odds of reporting “fair” or “poor” physical health. Length of time since incarceration did not moderate the association, meaning that even those incarcerated more than 10 years ago had equally poor self-reported health. The association with mental health was explained in part by income and employment.
The findings suggest that clinicians could consider screening for incarceration history and connecting formerly incarcerated patients to services and organisations that serve this community.
“Mass incarceration began in 1973, so older adults have spent most of their adult lives in this era and millions have been incarcerated in the past. It is critical to understand how incarceration – even in the distant past – may affect the health of older adults and what we can do to improve their health,” said corresponding author Louisa W. Holaday, MD, MHS, of the Icahn School of Medicine at Mount Sinai.
Researchers have adapted a rapid diagnostic technology that is able to identify undetected cases of malaria, helping tackle the spread of disease.
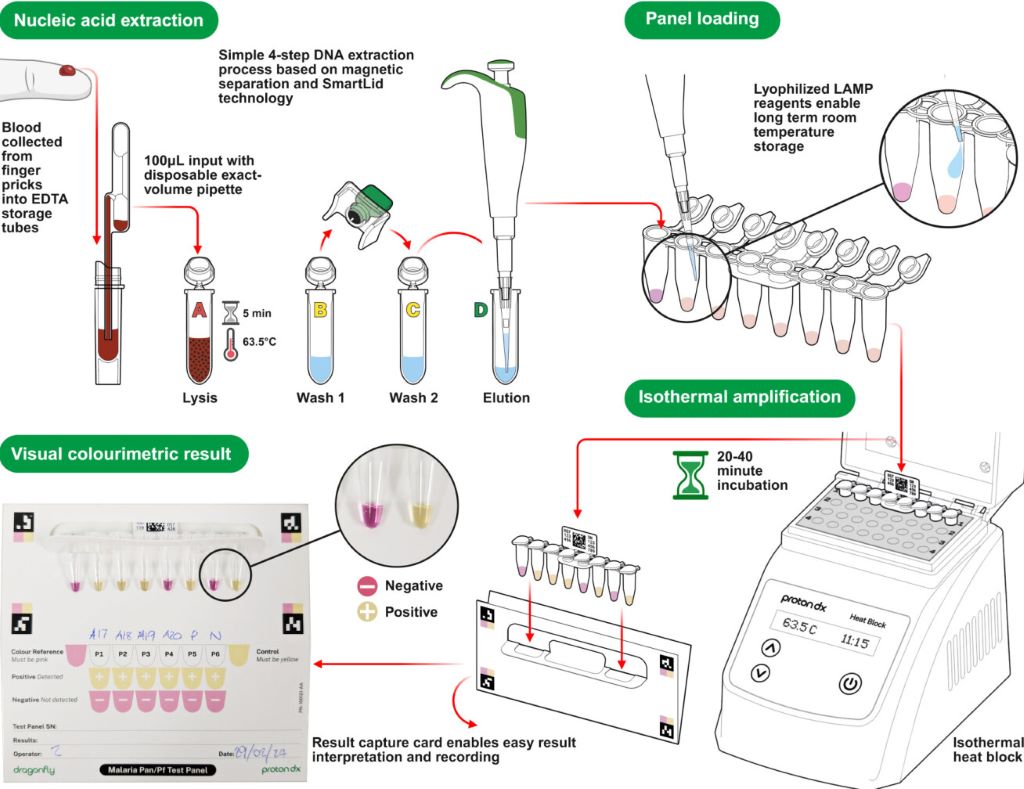
A diagram showing how the Dragonfly technology works (Credit: ProtonDx)
A team of scientists from Imperial College London, the MRC Unit The Gambia, the Clinical Research Unit of Nanoro in Burkina Faso, ProtonDx Ltd, and the NIHR Global Health Research Group have developed and validated a low-cost, point-of-care diagnostic that can rapidly detect low levels of malaria from a finger prick.
The test, called Dragonfly, relies on technology originally created at Imperial and its spinout ProtonDx. The technology allows users to diagnose malaria with high accuracy, without the need for extensive laboratory equipment or infrastructure. Results can be delivered in as little as 45 minutes, and the test is sensitive enough to detect even the lowest levels of malaria parasites in the blood – meaning that people without symptoms of malaria can still be identified.
Malaria is one of the leading causes of preventable deaths worldwide, with around 95% of all deaths occurring in Africa. Asymptomatic infections are a major driver of ongoing transmission, as individuals who carry the disease without showing symptoms do not seek medical treatment. Mosquitos feeding on blood from people without malaria symptoms can still deliver the malaria parasite to other people when they take their next blood meal. The new technology offers hope for combatting this potential spread of infection, by offering a way to identify previously undetectable malaria cases rapidly and on the ground in countries which are most affected by malaria.
The findings, published in Nature Communications, have significant global health implications as this field-deployable molecular diagnostic method offers a sensitive, scalable solution to support test-and-treat strategies for malaria elimination across Africa.
Professor Aubrey Cunnington, from Imperial’s Department of Infectious Disease and Co-Lead of the NIHR Global Health Research Group with Professor Halidou Tinto (from IRSS, Burkina Faso), said: “This is the first time that a diagnostic test for use outside of a laboratory setting has proven sensitive enough to detect low level malaria parasite infections in people who don’t have any symptoms.
“These people are the main source of malaria transmission, and in countries trying to eliminate malaria, there has long been interest in trying to detect these asymptomatically infected people with a screening test performed in their communities, and then giving treatment to those who are positive.
“Until now, no test has been able to detect enough of these infected people to make this a viable proposition, but the Dragonfly test now makes this possible.”
Detecting the undetectable
By collaboratively working as part of the NIHR Global Health Research Group, scientists were able to develop and test this new technology with the help of researchers in the regions affected most by malaria.
Almost 700 blood samples were collected from the community in The Gambia and Burkina Faso to assess the Dragonfly test’s accuracy against gold standard PCR testing and other common methods of testing, including expert microscopy and rapid diagnostic test (e.g., lateral flow immunoassay).
It was found that the Dragonfly tool could detect >95% of all malaria parasite infections, including 95% detection of those where the numbers of parasites were too low to be detected by looking at blood under a microscope.
Although Dragonfly is currently used as a research-used-only device, important progress is being made to understand the potential cost of a final manufactured version – especially when deployed at scale – a critical factor for effective deployment in sub-Saharan Africa. The team is already working closely with the Africa Centres for Disease Control and Prevention to explore opportunities with local manufacturers in the region, ensuring that production and scale-up can be rooted in local capacity. Future studies will also need to assess the robustness of the tool in community settings which are less connected to laboratory facilities.
Dr Jesus Rodriguez-Manzano, last author and technology development lead, from the Department of Infectious Disease, said “This research would not have been possible without the collaborative nature and all the organisations who took part in this study. The technology delivered through this work represents a game changer for malaria control efforts.”
The testing equipment
In the Dragonfly testing process, a capillary blood sample obtained from a simple finger prick is processed in around 10 minutes, without the need for specialised laboratory equipment, to extract high-purity nucleic acids from malaria parasites. The prepared sample is then placed into a detection panel, which is inserted into a portable heater.
After a 30-minute incubation at a constant temperature, results can be read visually using a colour chart: a pink reaction indicates a negative result, while a yellow reaction confirms malaria infection.
The Dragonfly can be manufactured at a fraction of the cost of other platforms, is compact enough to fit into a backpack, and can operate on batteries, an important feature for bringing the tool directly to communities without requiring additional specialised equipment. Testing can be carried out by most people without extensive training, meaning that healthcare providers or scientists do not need to be present for its use.
A common but often undiagnosed genetic condition may be causing delays in type 2 diabetes diagnoses and increasing the risk of serious complications for thousands of Black and South Asian men in the UK – and potentially millions worldwide.
The new study is conducted by the University of Exeter, in collaboration with Queen Mary University of London (QMUL). The findings, published in Diabetes Care, show that around one in seven Black and one in 63 South Asian men in the UK carry a genetic variant known as G6PD deficiency. Men with G6PD deficiency are, on average, diagnosed with type 2 diabetes four years later than those without the gene variant. But despite this, fewer than one in 50 have been diagnosed with the condition
G6PD deficiency does not cause diabetes, but it makes the widely used HbA1c blood test – which diagnoses and monitors diabetes – appear artificially low. This can mislead doctors and patients, resulting in delayed diabetes diagnosis and treatment.
Professor Inês Barroso from the University of Exeter said: “Our findings highlight the urgent need for changes to testing practices to tackle health inequalities. Doctors and health policy makers need to be aware that the HbA1c test may not be accurate for people with G6PD deficiency and routine G6PD screening could help identify those at risk. Addressing this issue is not only crucial for medicine, but for health equity.”
G6PD deficiency is a genetic condition that affects more than 400 million people worldwide, and is especially prevalent among those with African, Asian, Middle Eastern, and Mediterranean backgrounds. It is more common in men and usually goes undetected because it rarely causes symptoms. The World Health Organization recommends routine screening for G6PD deficiency in populations where it is common, but this is not widely implemented in the UK or many other countries.
This new study, supported by the National Institute for Health and Care Research Exeter Biomedical Research Centre, has found men with G6PD deficiency are at a 37% higher risk of developing diabetes-related microvascular complications, such as eye, kidney, and nerve damage, compared to other men with diabetes.
The HbA1c blood test is the international standard for managing type 2 diabetes and is used in 136 countries worldwide to diagnose diabetes, including being the routine test for diagnosis in the UK. However, for people with G6PD deficiency, this test may underestimate their blood sugar levels, causing significant medical delays and increasing their risk of serious complications.
Dr Veline L’Esperance, a GP and Senior Clinical Research Fellow at QMUL, said: “These findings are deeply concerning because they show how a widely used diagnostic tool may be failing communities that are already disproportionately affected by type 2 diabetes. Too many people are being left undiagnosed until it is too late to prevent serious complications. We need greater awareness among healthcare professionals and stronger policies to ensure equitable screening and diagnosis. That is why we are launching ‘Black Health Legacy’, which aims to be the largest health research programme focused on tackling diseases that disproportionately affect people from Black backgrounds. This is about saving lives and tackling long-standing inequalities in our healthcare system.”
The findings are based on genetic and health data from over half a million people in UK Biobank and Genes & Health studies. The research was conducted by a multidisciplinary team of clinicians and scientists, with the support of community partners, who linked the genetic data from each participant to their medical information. By doing this the team found men with the G6PD deficiency genetic variant were diagnosed at an older age compared to those without the condition. In addition, those with G6PD deficiency and diabetes also had more diabetes related complications. Researchers say further studies in more diverse populations are now needed to confirm these findings globally.
Next step is testing ‘holy grail’ therapy’s safety and effectiveness in patients
Squamous cancer cell being attacked by cytotoxic T cells. Image by National Cancer Institute on Unsplash
A new, highly potent class of immunotherapeutics with unique Velcro-like binding properties can kill diverse cancer types without harming normal tissue, University of California, Irvine cancer researchers have demonstrated.
A team led by Michael Demetriou, MD, PhD, reported that by targeting cancer-associated complex carbohydrate chains called glycans with binding proteins, they could penetrate the protective shields of tumor cells and trigger their death without toxicity to surrounding tissue.
Their biologically engineered immunotherapies – glycan-dependent T cell recruiter (GlyTR, pronounced ‘glitter’) compounds, GlyTR1 and GlyTR 2 – proved safe and effective in models for a spectrum of cancers, including those of the breast, colon, lung, ovaries, pancreas and prostate, the researchers reported in the journal Cell.
“It’s the holy grail – one treatment to kill virtually all cancers,” said Demetriou, a professor of neurology, microbiology and molecular genetics at the UC Irvine School of Medicine and the paper’s corresponding author. “GlyTR’s velcro-like sugar-binding technology addresses the two major issues limiting current cancer immunotherapies: distinguishing cancer from normal tissue and cancer’s ability to suppress the immune system.”
The researchers were awarded a Cancer Moonshot Initiative grant from the National Cancer Institute in 2018 for this study.
Landmark research
The study’s publication, the culmination of a decade of research, is a watershed moment and source of pride for UC Irvine and the UCI Health Chao Family Comprehensive Cancer Center.
“This landmark study is a paradigm shift with the very real potential to change how we treat cancer patients,” said Marian Waterman, PhD, former deputy director of research at the cancer centre and champion of the project since Demetriou and his then-postdoctoral fellow, Raymond W. Zhou, the study’s first author, began working on the concept in 2015.
Added Richard A. Van Etten, MD, PhD, director of the cancer centre and also an early supporter of the GlyTR project, “This novel technology may, for the first time, allow the widespread application of targeted T-cell therapy to solid tumours, which is the ‘holy grail’ in the immuno-oncology field.”
Current treatments, such as chimeric antigen receptor (CAR) T therapy, use the body’s white blood cells to attack cancer. They have largely worked only for blood cancers, such as leukaemia. The GlyTR technology also proved effective in targeting leukaemia, the study shows.
Unorthodox approach
While many cancer researchers have sought protein biomarkers for specific cancers, Demetriou and Zhou aimed at a more abundant target, the unique coating of glycans that surround cancer cells but are found in very low density in normal cells.
These complex sugar chains are the most widespread cancer antigens known, but were generally ignored by researchers because they are inert to the immune system.
To solve this problem, Demetriou and Zhou engineered the GlyTR compounds to attach themselves, Velcro-like, to glycan-dense cancer cells while ignoring low-glycan-density normal cells. Once attached, the GlyTR compounds identify the cancer cells as targets for killing by the body’s immune system.
In contrast, current cancer immunotherapies attack cells based on specific proteins regardless of their glycan density and thereby fail to distinguish tumour cells from healthy tissue.
A second impediment to developing broadly active cancer immunotherapies is the shield glycans form around solid tumours.
By targeting glycans and blanketing the tumour cells with the Velcro-like compounds, the GlyTR technology overcomes both obstacles.
Human trials
The next step will be testing the therapy’s safety and effectiveness in humans. Clinical grade GlyTR1 protein manufacturing is already being developed at the NCI Experimental Therapeutics program labs in Maryland, Demetriou said.
That will enable the launch of a phase 1 clinical trial, which could begin within about two years. It will test the therapy in patients with a range of metastatic solid cancers. The highest glycan density is typically seen in patients with refractory/metastatic disease, a population that also has the greatest unmet need for treatment.
Preterm infants born before 32 weeks who received more skin-to-skin contact while in the hospital showed stronger brain development in areas tied to emotion and stress regulation than babies who received less skin-to-skin care, according to a study published in Neurology®, the medical journal of the American Academy of Neurology. The study can only show an association and cannot establish causation.
“Skin-to-skin contact in preterm infants has been shown to have many benefits, with previous studies linking it to improved bonding, sleep, heart and lung function and growth, as well as reduced pain and stress,” said study author Katherine E. Travis, PhD, of Burke Neurological Institute in White Plains, New York. “Our findings in infants born very preterm suggest skin-to-skin care may also play a role in shaping early brain development, highlighting the potential importance of caregiving experiences during the earliest weeks of a preemie’s life.”
he study included 88 preterm infants with an average gestational age of 29 weeks who weighed an average of 2.65 pounds. The average stay in the hospital was two months. The goal was to find out whether skin-to-skin holding, also called kangaroo care, was linked to brain development in areas that help regulate emotions and stress. Researchers tracked skin-to-skin care with family members throughout each infant’s hospitalisation, including how long each session lasted and the total minutes per day. Families visited an average of once per day. When they provided skin-to-skin care, the average session was around 70 minutes with 73% of sessions provided by mothers. For the entire hospital stay, the average amount of skin-to-skin care per day was 24 minutes.
Each infant received a brain scan before going home from the hospital – around the time they would have reached full-term age of around 40 weeks. The brain scans measured how water moves through brain tissue. This movement helps reveal how white matter – the brain’s communication network – is developing. Researchers then compared the markers of white matter with the amount of time the preemies received skin-to-skin care per session and per day.
For skin-to-skin duration per session, researchers found longer sessions were linked to higher mean diffusivity – how freely water moves through the brain – in two key brain regions: the cingulum, which supports attention and emotion regulation; and the anterior thalamic radiations, which connects areas involved in emotional processing and memory.
Longer sessions were also linked to lower fractional anisotropy – how water movement is influenced by developing cellular tissues – in the anterior thalamic radiations. For daily total minutes of skin-to-skin care, researchers found higher amounts were linked to higher mean diffusivity in the anterior thalamic radiations. They were also linked to lower fractional anisotropy in the anterior thalamic radiations. These associations remained significant even after researchers accounted for factors that could influence brain development, including gestational age at birth, age at time of scan, socioeconomic status and how often family visited.
“Our findings add to growing evidence that white matter development is sensitive to a preterm infant’s experience while in the hospital,” said Travis. “Skin-to-skin care not only provides preterm infants with family connections through bonding, it may also be encouraging new connections within the brain itself, improving a baby’s brain health overall.”
A limitation of the study is that it was conducted at a single hospital and researchers reviewed existing medical records. The authors note that future research should explore how early caregiving experiences – like skin-to-skin care – might shape brain development and support later behavioural outcomes as preterm infants grow.
For many South African parents, few things are more stressful than watching their baby’s delicate skin flare up with redness, dryness, or tiny itchy patches. Baby eczema, also called atopic dermatitis, affects up to 1 in 5 children worldwide – and while it’s common, it can leave parents feeling worried and overwhelmed.
But the good news is, with the right skincare routine, baby eczema is manageable. And no, it doesn’t mean your little one will always struggle with sensitive skin.
“Parents are often surprised to learn that baby eczema is not a sign that they’re doing something wrong,” says Karen Van Rensburg, spokesperson for Sanosan South Africa. “It’s a common skin condition linked to an underdeveloped skin barrier, and the key is to protect and strengthen that barrier with gentle care.”
Baby eczema usually shows up between two and six months of age. It can appear on the face, behind the ears, on the arms, legs, or even the chest. The skin becomes dry, red, itchy and, in some cases, scaly.
“Triggers vary,” explains Van Rensburg. “It could be heat, dry air, soaps with harsh ingredients, or even certain fabrics. Understanding what sparks your baby’s flare-ups is an important step in managing the condition.”
So what can parents do at home? Here are some dermatologist-approved tips:
1. Keep baths short and sweet Stick to lukewarm water and limit bath time to 5–10 minutes. Avoid bubble baths and fragranced soaps.
2. Moisturise immediately after bathing Lock in hydration by applying a fragrance-free, gentle moisturiser while your baby’s skin is still slightly damp.
3. Choose your products wisely Opt for creams specifically designed for sensitive baby skin. Look for formulas enriched with natural oils, chamomile, or panthenol – like those found in Sanosan’s baby skincare range.
4. Watch the wardrobe Dress your baby in soft, breathable cotton and avoid scratchy fabrics like wool. Always wash new clothes before wearing.
5. Spot and soothe flare-ups early At the first sign of redness or irritation, apply a gentle, protective cream to calm the skin.
6. Don’t overheat the room Babies with eczema are often sensitive to heat. Keep the nursery cool and use a humidifier if the air feels very dry.
7. See a healthcare professional when needed If the rash is severe, infected, or your baby seems very uncomfortable, always seek medical advice.
“Parents sometimes think stronger products will ‘fix’ eczema faster,” says Van Rensburg. “But baby skin is incredibly delicate. Harsh ingredients strip away natural oils and make things worse. Gentle, consistent care is far more effective in the long run.”
Baby eczema can feel daunting, but with the right care and patience, most little ones outgrow it as their skin barrier matures. In the meantime, gentle skincare, lots of cuddles, and a watchful eye on triggers can make the world of difference.
“Think of it as supporting your baby’s skin while it learns to protect itself,” Van Rensburg adds. “You’re not just treating eczema – you’re helping build a healthy foundation for life.”
Sanosan focuses on natural ingredients and gentle formulas for healthy skin. Using active ingredients specially tailored to your baby’s skin, natural milk protein is the central ingredient in Sanosan and is especially nourishing. More than 90 % of the ingredients are of natural origin such as organic olive oil, and the formulations are biodegradable.
Safety first: all products are clinically tested and are free from parabens, silicones, paraffins, SLS / SLES and phenoxyethanol. For more info visit sanosan.co.za
Research in the Journal of Hepatology demonstrates that genetically engineered porcine livers can support key hepatic functions in humans
A landmark study in the Journal of Hepatology reports the world’s first auxiliary liver xenotransplant from a genetically engineered pig to a living human recipient. (Credit: Journal of Hepatology / Zhang et al.)
An important new study in the Journal of Hepatology, published by Elsevier, reports the world’s first auxiliary liver xenotransplant from a genetically engineered pig to a living human recipient. The patient survived for 171 days, offering proof-of-concept that genetically modified porcine livers can support key metabolic and synthetic functions in humans, while also underscoring the complications that currently limit long-term outcomes.
According to the World Health Organization, thousands of patients die every year while waiting for organ transplants due to the limited supply of human organs. In China alone, hundreds of thousands experience liver failure annually, yet only around 6000 people received a liver transplant in 2022. This pioneering case offers a potential new avenue to bridge the gap between organ demand and availability.
The case involved a 71-year-old man with hepatitis B-related cirrhosis and hepatocellular carcinoma who was not eligible for resection or human liver transplantation. Surgeons implanted an auxiliary graft from a genetically modified Diannan miniature pig with 10 gene edits, including xenoantigen knockouts and human transgenes to enhance immune and coagulation compatibility.
For the first month after surgery, the graft functioned effectively, producing bile and synthesising coagulation factors, with no evidence of hyperacute or acute rejection. However, on day 38, the graft was removed following the development of xenotransplantation-associated thrombotic microangiopathy (xTMA), a serious complication related to complement activation and endothelial injury. Treatment with the complement inhibitor eculizumab and plasma exchange successfully resolved the xTMA. Despite this, the patient later experienced repeated episodes of upper gastrointestinal haemorrhage and passed away on day 171.
“This case proves that a genetically engineered pig liver can function in a human for an extended period,” explained lead investigator Beicheng Sun, MD, PhD, Department of Hepatobiliary Surgery, and President of the First Affiliated Hospital of Anhui Medical University, Hefei, Anhui Province, China. “It is a pivotal step forward, demonstrating both the promise and the remaining hurdles, particularly regarding coagulation dysregulation and immune complications, that must be overcome.”
“This report is a landmark in hepatology,” commented Heiner Wedemeyer, MD, Co-Editor, Journal of Hepatology, and Department. of Gastroenterology, Hepatology, Infectious Diseases and Endocrinology, Hannover Medical School, Hannover, Germany, in an accompanying editorial. “It shows that a genetically modified porcine liver can engraft and deliver key hepatic functions in a human recipient. At the same time, it highlights the biological and ethical challenges that remain before such approaches can be translated into wider clinical use. Xenotransplantation may open completely new paths for patients with acute liver failure, acute-on-chronic liver failure, and hepatocellular carcinoma. A new era of transplant hepatology has started.”
“The publication of this case reaffirms the Journal of Hepatology as the world’s leading liver journal. We are committed to presenting cutting-edge translational discoveries that redefine what is possible in hepatology,” added Vlad Ratziu, MD, PhD, Editor in Chief, Journal of Hepatology, and Institute for Cardiometabolism and Nutrition, Sorbonne Université and Hospital Pitié Salpêtrière, Paris, France.
Study links blood levels of inflammatory markers with different aspects of cancer-related fatigue.
Photo by Karolina Grabowska on Pexels
New research reveals that inflammatory responses may play a role in different types of fatigue experienced by many people with cancer. The findings are published by Wiley online in CANCER, a peer-reviewed journal of the American Cancer Society.
Cancer-related fatigue can be a distressing and persistent burden that causes patients to feel physical, emotional, and/or cognitive tiredness or exhaustion. Activation of inflammatory responses by the tumour itself and/or by cancer treatment is thought to be a key biological driver of this symptom, but inflammatory activity across the cancer continuum has not been thoroughly examined.
To investigate, researchers at the University of California, Los Angeles (UCLA) analysed protein markers of inflammation in 192 women with early-stage breast cancer who were examined before radiation or chemotherapy and throughout the 18 months after treatment. At each assessment, women reported on different dimensions of fatigue (general, physical, mental, and emotional) and provided blood that was tested for protein markers of inflammation. These included two pro-inflammatory cytokines (TNF-α and IL-6) and two downstream markers of their activity (sTNF-RII and CRP).
Higher levels of TNF-α, sTNF-RII, and IL-6 were linked with greater general fatigue, which involves feelings of tiredness and exhaustion. These effects remained even after accounting for age, race, education, body mass index, and cancer stage. Similarly, there was a positive association between physical fatigue, which involves feelings of physical weakness and heaviness, and TNF-α, sTNF-RII, and CRP. Conversely, higher levels of TNF-α and sTNF-RII were associated with lower levels of emotional fatigue. No significant associations between mental (or cognitive) fatigue and inflammatory markers were found.
“Our findings indicate that inflammation plays a role in some aspects of cancer-related fatigue, but not others, and that these effects persist well after treatment,” said lead author Julienne E. Bower, PhD, of UCLA. “This is critical for developing targeted treatments for this common and disabling symptom.”
Neurons in the brain of an Alzheimer’s patient, with plaques caused by tau proteins. Credit: NIH
It has been known that brain lithium (Li) levels are depleted in individuals with mild cognitive impairment, a precursor for Alzheimer’s disease. For years, there have been attempts to restore Li levels to prevent Alzheimer’s disease by administering lithium carbonate. But now, it has been shown that the Li from this compound has been sequestered and not actually restoring the endogenous Li levels. Now, scientists have tried using lithium oxide (LiO) salts instead – and the treatment appears to be effective in prevention and even reversal of a mouse model of Alzheimer’s.
Join our QuickNews podcast as the arguments for and against this lithium-based approach are unpacked and debated.
UCLA researchers have uncovered a link between “morning sickness” symptoms and the body’s natural, but complex, inflammatory response to biological and bodily changes during pregnancy.
According to the National Institutes of Health, up to 80% of early-stage pregnant mothers experience some nausea, vomiting and aversions to certain foods and smells. While uncomfortable, these symptoms are not typically a sign that anything is wrong with the health of the mother or the developing fetus, but rather an indication of a delicate balance unique to pregnant women.
“During pregnancy, a mother’s immune system faces a tricky challenge: it has to protect both her and the foetus from infection, but without accidentally attacking the foetus, whose genetic identity is half-foreign because it is half derived from the father. Normally, the immune system attacks anything that seems foreign, so in pregnancy, it has to carefully adjust to keep the foetus safe while still defending against infection,” said UCLA anthropology professor Molly Fox, corresponding author of the study published in Evolution, Medicine and Public Health.
The researchers believe that this delicate balance, which protects mother and foetus, is achieved by a unique mix of inflammatory responses. They function to prevent the mother’s body from rejecting the foetus, alongside adaptive behavioural mechanisms, like nausea, that encourage the mother to avoid foods that are potentially harmful, especially in the first and second trimesters when the foetus is most vulnerable.
“Nausea, vomiting or aversions to foods or smells are not indications that something is going wrong for the mother or the foetus. It’s likely an indication that everything is moving along normally, and a reflection of the body’s healthy and helpful immune response,” said UCLA anthropology professor and paper co-author Daniel Fessler.
Methodology and findings
For the study, the UCLA-led team of anthropologists and epidemiologists collected and analysed blood samples to measure immune system molecules called cytokines. Cytokines are proteins that send signals to help the body launch a quick defence against sickness and regulate inflammation. Participants also filled out questionnaires that asked about morning sickness-related symptoms and food and smell aversions during the early stages of pregnancy. The participants were 58 Latina women in Southern California who were followed beginning in early pregnancy through the postpartum.
Sixty-four percent of study participants experienced odour or food aversions, primarily to tobacco smoke and meat. Sixty-seven percent reported nausea and 66% experienced vomiting.
The study team measured pro-inflammatory cytokines as well as anti-inflammatory cytokines. They found that women who experienced an aversion to tobacco smoke showed a noticeable shift toward a more inflammatory response. Food aversions, nausea and vomiting were also associated with a more pro-inflammatory immune balance.
An evolutionary process?
The correlation is consistent with researchers’ theory that these symptoms may be part of an evolutionary adaptation that helps pregnant mothers’ bodies minimize exposure to harmful substances, though the study’s authors caution that the evidence is not definitive and more research is needed.
They emphasised that the study allowed the team to look at both human biological and behavioural responses during pregnancy.
“In many mammals, the foetal compartment has barriers separating it from the mother’s blood supply, where her immune cells are. But in humans, we have a unique setup – foetal cells are bathed in maternal blood. Humans have the most invasive of all placentas, burrowing deep into maternal tissue. So humans need unique strategies to prevent the mother’s immune system from attacking the foetus,” said Fox.
These immunological changes may induce nausea, which in turn encourages food avoidance that might act as an additional layer of protection, according to the researchers
“Nowadays, you will see labels on packages of ground beef or soft cheese that warn pregnant women to be cautious about these products because of the risks of foodborne illness during pregnancy. Aversions to certain odours and foods, and nausea and even vomiting, appear to be evolution’s way of achieving that same objective,” said Fessler.
Practical implications
The researchers, including first author Dayoon Kwon, who just completed her PhD in epidemiology at UCLA (and is now a postdoctoral fellow at Stanford), said that the study could help bolster recognition that nausea and vomiting are normal symptoms with biological underpinnings associated with healthy pregnancies. The study’s results could help in paving the way for common-sense workplace accommodations, such as more efficient deployment of health care benefits and other helpful resources to reduce stigma, excessive absences and lost productivity.
They also encourage other researchers to continue to look into the questions raised by the study, to not only explore the evolutionary questions, but to work toward providing clinicians with non- or low-invasive measures of prognoses.