View of the spinal cord. Credit: Scientific Animations CC4.0
Mechanoreceptors are present in the spinal cord from birth, are sensitive to mechanical stimuli, and play an important role in triggering the pathological events that follow trauma. What happens if they are blocked? The extent of the damage decreases. This is the finding of a new study published inThe Journal of Physiology and conducted by a team at Scuola Internazionale Superiore di Studi Avanzati (SISSA), led by Professor Giuliano Taccola, with Atiyeh Mohammadshirazi as first author.
Everything happens within the very first milliseconds after the trauma, the scientists explained. It is during this brief time window that these spinal mechanoreceptors become active, triggering an impairment of the electrical signals that underlies normal neural communication. This initial event sets off a cascade of neurotoxic factors known as secondary damage, which amplifies and spreads the original traumatic lesion over the following hours and days.
Understanding the role of these receptors, according to the authors, is important not only for clarifying what happens during spinal shock. As demonstrated in the experiments, when their activity is blocked, the functional damage is also reduced. For this reason, spinal mechanoreceptors may represent a potential target for strategies aimed at reducing the disabling consequences of spinal cord injury.
Physical trauma disrupts electrical signaling
“It is well known that physical trauma to the spinal cord disrupts the flow of electrical signals that underlie the functioning of our nerve fibers. This phenomenon is known as DIP (Depolarizing Injury Potential). It begins almost immediately after trauma and continues propagating the primary damage over the following weeks, progressively worsening the lesion,” explain Atiyeh Mohammadshirazi and Giuliano Taccola. “However, the origins of this phenomenon are not yet fully understood.”
Mechanoreceptors and their role in the spread of damage
Receptors are cellular structures that respond to specific signals. Among them are mechanoreceptors, specialized proteins located on the cell membrane of sensitive cells that act as sensors for mechanical forces such as compression. Mechanoreceptors are found throughout the body, including around the spinal cord and within its central canal. In this environment, according to the SISSA research, they appear to play an important role in the propagation of injury.
The two authors explain, “In the progression of damage, depolarization precedes other well-known events such as the release of neurotoxic agents, and the inflammatory response that ultimately leads to cell death, the transient spinal hypoxia, and the rapid cell neuronal loss in the area of the primary lesion.” In this context, mechanoreceptors seem to contribute to initiating the depolarization process.
Mohammadshirazi and Taccola confirm: “When we blocked their activity in our experiments, we observed that the functional damage was significantly contained and limited.”
A possible avenue for reducing trauma-induced damage
“Our work,” conclude Giuliano Taccola and Carmen Falcone, who contributed to the histological analysis of the study, “explored what happens at the cellular level immediately after spinal trauma. As we explained, these injuries do not only involve the initial mechanical damage; they also trigger a cascade of complex neurotoxic events that amplify and worsen cellular damage and disrupt communication between neurons.”
They conclude: “With our laboratory model experiments, we demonstrated that blocking mechanosensitive receptors can effectively reduce the immediate pathological effects of spinal trauma. Our research is basic research, of course, and practical applications are still far away. Nevertheless, it may open a promising path to explore in the future to reduce spinal shock and the damage that follows trauma.”
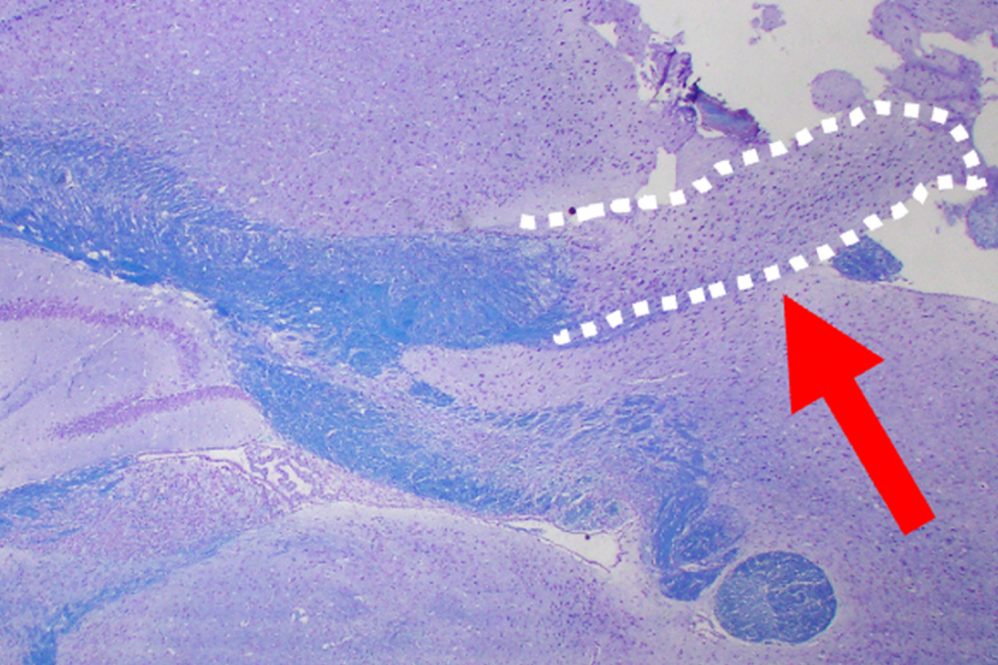
Part of the brain disappears in mice treated with dasatinib and quercetin
The image shows a section of the brain of a mouse treated with dasatinib and quercetin. The bluish area is the corpus collosum. The dotted outline shows the part of the corpus collosum that is affected by the medication. (Image courtesy of Crocker Lab/UConn School of Medicine)
A two-drug combination frequently used in anti-ageing research causes brain damage in mice, University of Connecticut researchers report in the March 16 issue of PNAS. The findings should make doctors cautious about prescribing the drug combo prophylactically, but also suggest new ways to understand multiple sclerosis.
“When you administer this cocktail to an animal, young or old, the myelin is damaged, which makes it disappear. Even worse in the young animals” than in the aged ones, says UConn School of Medicine immunologist Stephen Crocker.
Myelin is the insulation around the nerves. When it disappears, nerves don’t work as well, and people can develop numbness, pain, and lose the ability to walk. They can also have problems thinking and remembering. Missing myelin is the primary cause of multiple sclerosis. And Crocker and his colleagues saw it happen to mice when treated with dasatinib+quercetin (D+Q) at doses often used to treat ageing-related inflammation and metabolic disorders.
D+Q is a popular combination of medicines in anti-ageing research. Many studies have shown it works to eliminate aged cells that contribute to inflammation and other age-related symptoms. It is being tested for a range of diseases, from type II diabetes to Alzheimer’s. People in the anti-ageing scene sometimes even use it off-label, though the medical community discourages this. Very few studies have looked at its effect on the brain.
Evan Lombardo ’23 (CLAS), currently a Dartmouth neuroscience graduate student, and Robert Pijewski ’21 PhD, now at Anna Maria College, were working in Crocker’s lab when they wondered if it was possible to rejuvenate the brains of people with multiple sclerosis, and potentially heal their symptoms, using D+Q. They tried it on mice, both young (6 to 9 months) and old (22 months), as well as on brain cells cultured in a dish in the lab. The brain cells were oligodendrocytes, the cells that are supposed to grow and maintain myelin.
The results were dramatic. Healthy mice have myelin surrounding the axons (nerve cells) in the brain. It looks like dark rings around the lighter axon (see figure 1, the left panel.) But the mice treated with D+Q had much less myelin around their axons after the treatment, and the damage was worse in the younger mice. The corpus callosum, a region that connects the cerebral cortex to other parts of the brain and is associated with a range of important functions, also disappeared in mice treated with D+Q. This is known to happen sometimes to people who received chemotherapy, and causes the symptoms sometimes referred to as “chemo brain.”
When the researchers looked closely at the damaged brain tissue, they found clues as to why the myelin had disappeared. The myelinating cells – oligodendrocytes – hadn’t died. They’d regressed into a juvenile form of themselves. And the metabolism of the cells was abnormal, too.
“We suspect the drugs are choking off energy the cells need, and the cells respond by reducing complexity, reverting to a younger state, but less functional,” Crocker says.
Interestingly, these cells that have reverted look very much like a distinct population of cells found in people with multiple sclerosis. It suggests that in multiple sclerosis, myelinating cells might come under stress and revert to a younger stage. It also means those cells might be able to recover. And that is what the researchers are working on now.
“If we can mimic this, we have an amazing opportunity to see if the cells can recover and repair the brain,” Crocker says.
Findings published by The BMJ reinforce previous research linking use of the antiseizure drug valproate during pregnancy to neurodevelopmental disorders such as ADHD and autism in children, and indicate no substantial risk for several other antiseizure drugs including levetiracetam and lamotrigine.
However, the researchers say continued monitoring of the few signals – possible associations between a medicine and an unintended side effect – that emerged (eg, for zonisamide) will be important.
Antiseizure drugs are commonly and increasingly used by women of childbearing age for conditions like epilepsy, bipolar disorders, and migraine prevention. Women with epilepsy are advised to continue taking these during pregnancy, as uncontrolled seizures pose risks to both mother and child.
Yet, while valproate use during pregnancy has been linked to impaired neurodevelopment in children, information on other antiseizure drugs is limited.
To address this gap, researchers analysed claims data for pregnancies with diagnosed epilepsy from two large US public and commercial insurance databases, spanning the period from 2000 to 2021.
They compared 14,993 children exposed to at least one antiseizure medication during the second half of pregnancy with 8,887 unexposed children. Of these, 5,505 were followed for at least 5 years and 2,516 for at least 8 years after birth.
Potentially influential factors including mother’s age, ethnicity, mental health, substance use, other medication use and underlying conditions were also taken into account.
Valproate and zonisamide showed associations with several neurodevelopmental disorders, whereas levetiracetam and phenytoin were not associated with an increased risk of any of the studied outcomes.
Although no meaningful associations were found for topiramate and lamotrigine across most outcomes, there was a potential signal for intellectual disability (both drugs) and learning difficulty (topiramate only). However, the authors note that these findings are based on small numbers and require confirmation in follow-up studies.
Several other drugs were also associated with a risk increase for intellectual disability. However, the authors note that these estimates are based on small numbers and therefore should be interpreted with caution.
Carbamazepine and oxcarbazepine also showed a modest risk increase for ADHD and behavioral disorders.
This is an observational study, so no definitive conclusions can be drawn about cause and effect, and the authors point to several limitations including relying on insurance claims data and the potential influence of other unmeasured factors such as underlying epilepsy type and severity.
However, the use of two large nationwide databases of insured pregnant women linked to their children enhanced the generalisability of their findings and enabled them to assess the risk of specific neurodevelopmental disorders associated with individual antiseizure medications. Results were also consistent after additional analyses, suggesting that they are robust.
As such, they conclude: “Our study reinforces the substantial risks of neurodevelopmental disorders associated with prenatal valproate exposure and suggests the need to further evaluate the safety of zonisamide during pregnancy.”
“Continued monitoring of newer antiseizure drugs and the few potential signals that emerged (ie, the moderate increased risk of ADHD and behavioural disorder after carbamazepine and oxcarbazepine exposure, and the association of several antiseizure drugs with intellectual disability) will be important,” they add.
Researchers at King’s College London have shown that a widely used cardiac arrest risk score can be applied before patients reach hospital, enabling paramedics to assess the risk of brain injury at an earlier stage of care.
Results from the RAPID-MIRACLE trial have found, for the first time, that the widely used MIRACLE2 risk score can be applied outside a hospital setting to accurately predict brain injury following a cardiac arrest. This could inform the type of immediate care patients receive, helping to ensure they have the best treatment available while saving crucial resources.
An out of hospital cardiac arrest (OHCA) carries a high risk of death, with fewer than 10% of patients surviving. Even when a patient’s heart is successfully restarted through CPR and circulation is restored, known as return of spontaneous circulation (ROSC), clinicians often face uncertainty about the extent of brain injury.
Despite current UK and European guidelines recommending that patients who experience an out of hospital cardiac arrest are sent to a specialist cardiac centre, the majority of patients are still conveyed to local emergency departments. The MIRACLE2 score, when applied in the pre-hospital setting, may now open up the possibility of identifying patients earlier and enabling direct transfer to specialist centres, allowing faster access to expert care and advanced treatments for patients who might otherwise have been conveyed to a local hospital.
Created by Dr Nilesh Pareek, Adjunct Senior Lecturer and Consultant Interventional Cardiologist, the MIRACLE2 score accurately predicts the extent of brain damage after 30 days following an OHCA. Until now, it has only been applied once a patient reaches hospital.
Dr Pareek and his team worked with the London Ambulance Service and Heart Research UK to evaluate whether the score could be calculated immediately after ROSC in the community.
The study followed patients from paramedic care through to hospital treatment across multiple London sites, providing real-world evidence of how the score performs outside a hospital environment.
The researchers tested two new versions of the score – one which included a blood test and one which didn’t. While the version with the blood test was highly accurate, paramedics frequently found it impractical due to technical failures and time pressure. The version without the blood test, known as Pre-MIRACLE2, was almost identical in terms of accuracy.
While MIRACLE² has supported early in-hospital risk stratification following out-of-hospital cardiac arrest, RAPID-MIRACLE extends this work into the pre-hospital setting, enabling paramedics to assess risk earlier in a patient’s care pathway. By validating the model in the field, we have taken an important step towards integrating earlier risk assessment into routine emergency care.”Dr Nilesh Pareek, senior author of the study and Adjunct Senior Lecturer, King’s College London and Consultant Interventional Cardiologist, King’s College Hospital
Alongside the study, the MIRACLE² app, led by Dr Pareek, has been updated to incorporate the newly validated pre-hospital model. The app, developed by Ensono Digital, uses the MIRACLE2 algorithm and is designed as a practical tool to help clinicians calculate the score quickly and accurately, without needing to recall each variable from memory.
By entering patient information such as age, initial heart rhythm and other markers, paramedics and hospital clinicians can generate an immediate estimate of a patient’s risk of poor neurological outcome following out-of-hospital cardiac arrest.
The research team is now in discussion with emergency medical services regarding a potential service evaluation to explore how the updated tool could be implemented in routine practice.
Heart Research UK were delighted to fund the RAPID-MIRACLE trial with the aim of improving outcomes for this poorly served patient group. The promising results from the trial suggest that better outcomes can be delivered, and we hope the risk score can be adopted nationally for all patients.”Dr Kate Langton, Director of Research at Heart Research UK
The research findings were presented in Washington at the CRT 2026 conference and the full study was published in European Heart Journal – Acute Cardiovascular Care.
Even with highly extensive training, the human brain is not really capable of performing two tasks simultaneously. Moreover, even the smallest deviations from trained routines can have a significant impact on how quickly and successfully people complete tasks simultaneously. This is shown by a new study conducted by Martin Luther University Halle-Wittenberg (MLU), the FernUniversität in Hagen and the Medical School Hamburg. It was recently published in the Quarterly Journal of Experimental Psychology.
In three experiments, the researchers investigated how people perform two tasks simultaneously that involve different senses: participants were asked to indicate the size of a circle that was briefly displayed with their right hand and simultaneously to say whether a sound played at the same time was high, medium or low. The speed at which the participants completed the tasks and the number of mistakes they made were measured. The tasks were repeated over a period of up to twelve days. The results showed that the more often the test subjects completed the test, the faster they solved both tasks without errors.
Earlier studies with similar findings had therefore suggested that so-called dual-task costs, ie, performance losses when working on two tasks simultaneously, could almost completely disappear after extensive practice. “This phenomenon, known as virtually perfect time sharing, has long been considered evidence of true parallel processing in the brain and proof that our brain is capable of unlimited multitasking. The results of our study clearly contradict this assumption,” says psychologist Professor Torsten Schubert from MLU.
The new study shows that the underlying cognitive processes still do not run completely in parallel. What’s more, even the smallest changes to the tasks caused the error rate to rise and the participants to take longer to complete the tasks. “Our brain is very adept at sequencing processes so that they no longer interfere with each other. However, this optimisation has its limits. In particularly challenging situations, our cognitive apparatus therefore tires very quickly and becomes error prone,” Schubert continues.
The study also provides new impetus for safety research. “Our results show why multitasking can often be risky in everyday life, despite routine, for example when driving and talking on the phone at the same time. This is also relevant for professions with complex activities where several tasks have to be performed in parallel, such as air traffic controllers or simultaneous translators,” says Professor Tilo Strobach from the Medical School Hamburg. Professor Roman Liepelt from the FernUniversität in Hagen adds: “Our study sheds new light on the limits of human information processing. Understanding such cognitive bottlenecks is crucial for improving work processes, learning environments and safety measures in everyday life.”
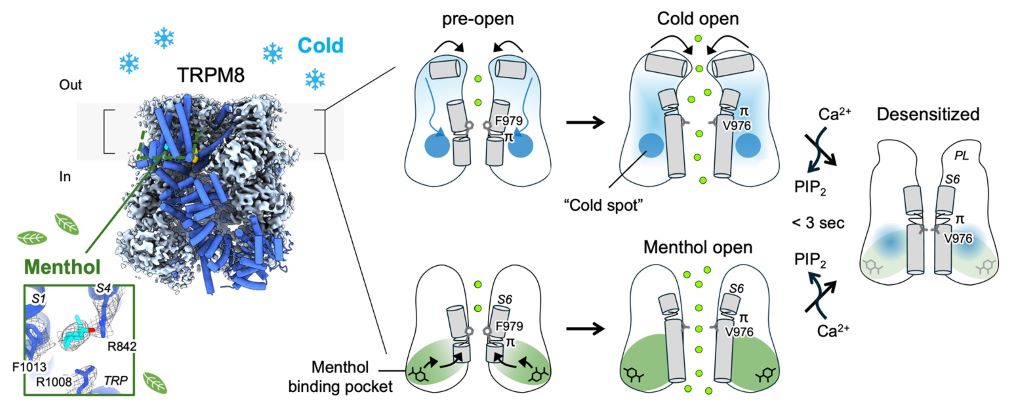
First-ever molecular snapshots show the body’s “cold sensor” in action, with implications for treating pain, migraines, and dry eye
Using cryo-electron microscopy, researchers captured multiple conformational snapshots of the cold sensing channel, TRPM8, as it transitions from closed to open.
When you step outside on a winter morning or pop a mint into your mouth, a tiny molecular sensor in your body springs into action, alerting your brain to the sensation of cold. Scientists have now captured the first detailed images of this sensor at work, revealing exactly how it detects both actual cold and the perceived cool of menthol, a compound derived from mint plants. The research was presented at the 70th Biophysical Society Annual Meeting in San Francisco from February 21–25, 2026.
The study focused on a protein channel called TRPM8. “Imagine TRPM8 as a microscopic thermometer inside your body,” said Hyuk-Joon Lee, a postdoctoral fellow from Seok-Yong Lee’s laboratory at Duke University. “It’s the primary sensor that tells your brain when it’s cold. We’ve known for a long time that this happens, but we didn’t know how. Now we can see it.”
TRPM8 sits in the membranes of sensory neurons innervating the skin, oral cavity, and eyes. It responds to cold temperatures – roughly between 8°C and 28°C – by opening up and allowing ions to flow into the cell, which triggers a nerve signal to the brain. It’s also the reason menthol, eucalyptus, and certain other compounds produce that characteristic cooling sensation.
“Menthol is like a trick,” Lee explained. “It attaches to a specific part of the channel and triggers it to open, just like cold temperature would. So even though menthol isn’t actually freezing anything, your body gets the same signal as if it were touching ice.”
Using cryo-electron microscopy – a technique that images flash-frozen proteins with an electron beam – Lee and colleagues captured multiple conformational snapshots of TRPM8 as it transitions from closed to open. They discovered that cold and menthol activate the channel through shared yet distinct allosteric networks: cold primarily triggers changes in the pore region (the part that actually opens to let ions through), while menthol binds a different part of the protein and induces shape changes that propagate to the pore.
“When cold is combined with menthol, the response is enhanced synergistically,” Lee said. “We used this combination to capture the channel in its open state – something that hadn’t been achieved with cold by itself.”
The findings have medical implications. When TRPM8 doesn’t function properly, it has been linked to conditions including chronic pain, migraines, dry eye and certain cancers. Acoltremon, a drug that activates TRPM8, is an FDA-approved eye drop for dry eye disease. As a menthol analogue, it works by activating the cooling pathway to stimulate tear production and soothe irritated eyes.
The researchers also identified what they call a “cold spot” – a specific region of the protein that is uniquely important for sensing temperature and helps prevent the channel from becoming desensitised during prolonged cold exposure.
“Previously, it was unclear how cold activates this channel at the structural level,” Lee said. “Now we can see that cold triggers specific structural changes in the pore region. This gives us a foundation for developing new treatments that target this pathway.”
The work offers the first molecular definition of how cold and chemical stimuli are integrated to create the sensation of coolness – answering a fundamental question in sensory biology that has puzzled scientists for decades.
Stimulating two brain areas, nudging them to collectively fire in the same way, increased a person’s ability to behave altruistically, according to a study published February 10th in the open-access journal PLOS Biology by Jie Hu from East China Normal University in China and colleagues from University of Zurich in Switzerland.
As parents raise their kids, they often work to teach them to be kind and to share, to think about other people and their needs – to be altruistic. This unselfish attitude is critical if a society is going to function. And yet, while some people grow up to devote themselves to others, other people still manage to grow up selfish.
To understand what brain areas and connections might underlie individual differences in altruism, the researchers asked 44 participants to complete 540 decisions in a Dictator Game – offering to split an amount of money with someone else, which they then got to keep. Each time, the participant could make more or less money than their partner, but the amounts varied. As the participants played the game, the researchers stimulated their brains with transcranial alternating current stimulation over the frontal and parietal lobes of the brain. The stimulation was set up to make the brain cells in those areas fire together in repetitive patterns, training them all to either gamma or alpha oscillation rhythms.
The authors found that during the alternating current stimulation designed to enhance the synchrony of gamma oscillations in the frontal and parietal lobes, the participants were slightly more likely to make an altruistic choice and offer more money to someone else – even when they stood to make less money than their partner. Using a computational model, the researchers showed that the stimulation nudged the participants’ unselfish preferences, making them consider their partner more when they weighed each monetary offer. The authors note that they did not directly record brain activity during the trials, and so future studies should combine brain stimulation with electroencephalography to show the direct effect of the stimulation on neural activity. But the results suggest that altruistic choices could have a basis in the synchronized activity of the frontal and parietal lobes of the brain.
Coauthor Christian Ruff states, “We identified a pattern of communication between brain regions that is tied to altruistic choices. This improves our basic understanding of how the brain supports social decisions, and it sets the stage for future research on cooperation – especially in situations where success depends on people working together.”
Coauthor Jie Hu notes, “What’s new here is evidence of cause and effect: when we altered communication in a specific brain network using targeted, non-invasive stimulation, people’s sharing decisions changed in a consistent way – shifting how they balanced their own interests against others’.”
Coauthor Marius Moisa concludes, “We were struck by how boosting coordination between two brain areas led to more altruistic choices. When we increased synchrony between frontal and parietal regions, participants were more likely to help others, even when it came at a personal cost.”
Researchers at the University of Missouri may have uncovered a clue explaining why young adults with autism are roughly six times more likely to develop Parkinson’s disease later in life.
In a recent study, the researchers found that some young adults with autism show abnormalities in dopamine transporters, tiny molecules in the brain that recycle unused dopamine, on brain scans that are typically used to diagnose older adults with Parkinson’s disease.
Future research could help determine whether the health of dopamine transporters could be an early warning sign of Parkinson’s disease developing later in life.
“While the loss of these dopamine transporters can be biomarkers for Parkinson’s disease, no one had ever thought to look at them in the context of young adults with autism, so hopefully this work can help us explore if there is a potential link going forward,” David Beversdorf, a professor in the School of Medicine and College of Arts and Science, said. “There has been previous work looking into the total amount of dopamine in the brains of people with autism, but we took a new approach by looking at abnormalities in terms of how dopamine is processed in a specific part of the brain called the basal ganglia via these dopamine transporters.”
Dopamine under the spotlight
Dopamine is a neurotransmitter involved in numerous body functions, such as memory, pleasure, motivation, behaviour and attention. Of particular interest to Beversdorf, a clinician at the Thompson Center for Autism and Neurodevelopment, is that dopamine also helps control muscle movement as well as cognition.
Beversdorf, who collaborated with lead author Nanan Nuraini on the study, originally wanted to know whether certain repetitive behaviors common in some young adults with autism, such as hand-flapping or rocking back and forth, were linked with abnormalities in dopamine transporters.
While he did not notice patterns in that regard, what he found surprised him.
Beversdorf looked at Dopamine Transporter (DaT) brain scans of 12 young adults with autism.
Four different nuclear medicine specialists examined the scans. All of them agreed that two of the 12 young adults had abnormal dopamine transporters and that eight appeared normal. They disagreed on the remaining two.
“Since these DaT scans are typically used to diagnose or evaluate older adults with Parkinson’s disease, the appearance of abnormalities in some young adults with autism was very surprising, so we should look into this topic more going forward,” Beversdorf said. “While it’s too early to jump to conclusions, hopefully our work raises awareness about the importance of monitoring the brain health of young adults with autism as they age.”
Next, Beversdorf hopes to study a broader range of people with autism by conducting more DaT scans across different age groups.
“The earlier we can identify those who might be at greater risk for getting Parkinson’s disease down the road, the sooner we can discuss preventative measures, including whether certain medications could potentially slow down the progression of disease,” Beversdorf said.
If someone living with HIV is not on antiretroviral therapy, the virus can cause inflammation in, among other places, the brain. Photo by Anna Shvets
By Biénne Huisman
Antiretroviral therapy has shifted HIV from a fatal to a chronic condition. But neuropsychiatrists say it is imperative for people living with the virus to start treatment immediately as the “duration of untreated exposure” may cause irreversible brain damage and impact long-term cognitive health.
It has been recognised for decades that cognitive impairment is a potential complication of HIV infection. Questions over how likely and how serious this potential complication is have become more urgent over time as the population of people living with HIV ages – ageing after all also increases the risk of cognitive decline.
There were around 1.75 million people over the age of 50 living with HIV in South Africa in 2024, according to Thembisa, the leading mathematical model of HIV in the country. This is just over 20% of the estimated eight million HIV positive people in the country. A study published in the Lancet medical journal also has the number at around 20% in sub-Saharan Africa.
This is a delicate field of enquiry as researchers walk a tightrope to avoid “the burden of double stigma”, while conceptualising the necessary tools to best diagnose brain problems and suitable interventions.
Within as little as two weeks
At Groote Schuur Hospital’s Neuroscience Institute, Professor John Joska, director of the University of Cape Town’s (UCT’s) HIV Mental Health Research Unit, explains that HIV can enter the brain within as little as two weeks after the initial infection – primarily through infected white blood cells, such as lymphocytes. If a person is not on antiretroviral therapy, the virus can cause inflammation in the brain and possibly also tissue damage.
“The brain is a protected compartment,” says Joska. “A theory as to how the virus, which is a protein particle, gets into the brain is through infected lymphocytes. This doesn’t directly infect nerve cells, what we call neurons. It infects other supporting tissues and cells in the brain, causing an inflammation which damages typically the white matter of the brain. Over time, that inflammation can cause loss of neurons, but indirectly.”
While antiretroviral therapy is crucial for clearing and suppressing HIV in all body compartments, including in the brain, he says that it does not reverse damage that occurred before the treatment was started.
“Today, people with HIV are living near normal lifespans,” he says. “The question is, will the fact that they’ve had HIV, with some duration of untreated exposure and potential loss of brain tissue, cause them to be at higher risk than the average person for developing dementias of old age – which really are mainly Alzheimer’s disease or vascular dementia.” It is these longer-term effects that are the main concern when it comes to the impact of HIV on the brain.
Part of the problem is that South Africa not only has an ageing population of people living with HIV, but many of these people would only have started treatment quite long after they contracted the virus. One key reason for this is the South African government’s reluctance to make antiretroviral treatment available in the early 2000s. It has been estimated that those delays resulted in over 300 000 avoidable deaths – they may also be contributing to brain health issues now and in the future.
From efavirenz to dolutegravir
Apart from HIV itself, some of the medicines used to treat the infection have also had an impact on the brain.
In 2019, the standard HIV treatment in South Africa changed from a three-drug combination containing an antiretroviral drug called efavirenz, to a combination containing the drug dolutegravir. This shift had mental health benefits, as evidenced in research lead by Joska’s fellow UCT Neuro-HIV researcher, Associate Professor Sam Nightingale.
Joska says: “The study looked at the period from 2017 to 2020 and the switch from efavirenz to dolutegravir based treatment. It was well known that efavirenz caused, certainly for the first two months, a bunch of psychotropic or psychological issues like nightmares or anxiety, even psychosis for some people. But our findings showed people who switched to dolutegravir actually do very well. They look more like people without HIV after eight months. So dolutegravir has been a huge advantage, not only because it’s robust, but because it’s neuro-protective.”
New models for HIV and cognitive impairment
A shift is underway in how experts are thinking about cognitive impairment in people with HIV. Some neuropsychiatrists, including Joska, are recommending a shift away from the 2007 HIV-Associated Neurocognitive Disorders model, arguing that its cognitive test scores do not adequately account for variables such as education and socioeconomic background, and that it can overdiagnose impairment. The argument is set out in an article, lead-authored by Nightingale, that was published in the journal Nature Reviews Neurology in 2023.
The authors argue that a label of cognitive impairment might cause a “double burden of stigma” for people living with HIV – affecting self-esteem, inciting fear and prompting further discrimination against persons already subject to stigma as it stands. To illustrate the point, they point out how, up until recently, people with HIV in the United Kingdom could not become airline pilots due to concerns over cognitive impairment. However, following a campaign by a pilot living with HIV, the United Kingdom’s Civil Aviation Authority removed the ban in 2022.
Nightingale and his colleagues argue that traditional test scores be used in conjunction with real-life symptoms and medical evidence of brain problems. It introduces the conceptual model of HIV-Associated Brain Injury, which refers specifically to damage caused by the virus. This distinguishes it from other causes of cognitive impairment such as depression, substance abuse, diabetes and cardiovascular disease. As Spotlight previously reported, HIV is also associated with an increased risk of depression, though this is at least partially driven by social factors.
Lower cognitive function associated with late diagnosis
At the 2026 Conference on Retroviruses and Opportunistic Infections hosted in Denver in the United States in late February, these issues were tabled at a discussion titled “When I’m 64: Neurodegeneration, Epigenetic Aging, and Cognition in Older People With HIV.”
Professor John Joska is the director of the University of Cape Town’s HIV Mental Health Research Unit. (Photo: Biénne Huisman/Spotlight)
In his presentation, Professor Alan Winston of Imperial College London, also a member of the International HIV-Cognition Working Group, and a frequent co-author alongside Joska and Nightingale, relayed existing research findings that on average, people living with HIV have lower cognitive function – including memory, attention span and executive function like planning – compared to people who don’t have HIV of the same age. He said that this manifests as an increased risk of lower grade early dementia.
Like Joska, Winston stressed that the most deteriorated cognitive function in people living with HIV is associated with untreated HIV and late HIV diagnosis. He reiterated that starting HIV treatment soon after diagnosis is protective, and that viral suppression is associated with better cognition. In groups of patients with HIV well controlled on dolutegravir-based HIV treatment, cognition appears similar to HIV negative groups, he said.
HIV clinicians need to pay better attention to the brain
In an impassioned presentation, Dr Shibani Mukerji, Associate Professor of Neurology at Harvard Medical School, argued that protecting the brain is an overlooked frontier in effective HIV treatment, and that clinicians need to pay more attention to it.
“By the time patients and clinicians notice cognitive decline – generally and in HIV – the damage to the brain is done and lives are affected negatively. People don’t raise cognitive concerns early enough due to stigma, fear, [and] lack of recognition of the issues. It is seen as ‘just getting old’,” she said.
Mukerji emphasised the need to prioritise brain health. “HIV doctors and treatment programmes are focused, almost exclusively, on viral load as the marker of successful treatment. They may be thinking laterally and consider TB and other infections, maybe cardiovascular disease – but they are definitely not paying enough attention to brain health. HIV doctors aren’t aware enough of brain health issues in people living with HIV, and even when they are, they often don’t feel comfortable diagnosing or managing it, so it is under recognised and under diagnosed.”
The perception that there is no way to manage or treat cognitive decline –generally and in people living with HIV – is wrong, she said, adding that optimising physical, mental and social health is critical for brain health.
“Almost half of dementia risk [in people in general] is linked to preventable causes,” she told conference delegates, along with a slide listing preventable causes including loss of hearing, social isolation, cardiovascular disease and depression.
She explained: “If someone has cognitive decline and for example you improve their hearing – if they have hearing issues – and you work on their social isolation, and treat their vascular disease, and treat their depression, you can see a marked improvement in their cognition.”
Ending her presentation with a twist of humour, Mukerji’s last slide referred to the session’s title, a reference to the Beatles song on aging “When I am 64”. She printed the song’s lyrics: “When I get older, losing my hair, many years from now…”, closing her talk by saying: “It’s okay to stand up and sing, in fact your doctor might prescribe it.”
Houston Methodist researchers find antibiotics aid recovery from traumatic brain injury
Source: CC0
What if healing the brain after traumatic injury starts in the gut? In a new study published in Nature Communications Biology, Houston Methodist researchers led by Sonia Villapol, PhD, found that short-term antibiotic treatment significantly reduced neuroinflammation and neurodegeneration following traumatic brain injury (TBI) by altering the gut microbiome in animal models.
“We found that antibiotic treatment following TBI can reduce harmful gut bacteria, decrease lesion size and limit cell death,” said Villapol, an associate professor in the Department of Neurosurgery at Houston Methodist. “Our results support a gut–brain mechanism in which microbiome changes influence peripheral immunity and, in turn, neuroinflammation after TBI.¨
Administering antibiotics cleans the gut of harmful bacteria, allowing beneficial bacteria to flourish. The study found that two helpful bacteria, Parasutterella excrementihominis and Lactobacillus johnsonii, are key to driving cell repair. According to Villapol, they could also be major regulators for peripheral inflammation in the body.
Notably, 70% of immune system regulation is generated by the gut microbiome. During gut imbalance, the bidirectional nature of the brain-gut axis can wreak havoc throughout the entire body.
“Our brains are constantly sending signals to the rest of our bodies. Following a traumatic brain event, those signals can get scrambled and disrupt other organs, including our digestive system,” Villapol said. “If the gut stays out of balance, the brain may have a harder time healing.”
Recent studies indicate that TBI-induced gut microbiome imbalance may even contribute to the development of neurodegenerative diseases like Parkinson’s, Alzheimer’s and dementia.
Villapol’s lab is focused on investigating and developing new neuroprotective treatments to fight inflammation linked with neurodegenerative disease. “If we can break neuroinflammation in the acute or chronic stage, we can reduce the risk of developing Alzheimer’s or dementia,” said Villapol.
The next phase of the research will focus on bioengineering P. excrementihominis and L. johnsonii to further develop precision therapies to reduce neuroinflammation.