Respiratory syncytial virus (RSV), a common infection in children and older adults, can also infect nerve cells and trigger inflammation leading to nerve damage, according to a new Tulane University study.
RSV can cause mild symptoms such as coughing, sneezing and fever or lead to more severe conditions such as pneumonia or bronchiolitis. But since the disease was first discovered in 1956, it has been thought to only infect the respiratory tract.
This study, published in The Journal of Infectious Diseases, is the first to prove that RSV can penetrate nerve cells and may provide the clearest link between RSV and reported neurological symptoms in children.
RSV has been previously detected in the spinal fluid of children with seizures. Additionally, 40% of RSV-positive children under the age of 2 have shown acute encephalopathy, brain damage that can result in confusion, memory loss or cognitive difficulties.
The findings underscore the potential long-term impacts of the disease, as well as the importance of preventative measures such as the two RSV vaccines approved by the FDA in 2023.
“This is the most common respiratory virus in the first years of life as well as an impactful virus among the elderly,” said Dr Giovanni Piedimonte, Tulane University vice president for research and professor of pediatrics, biochemistry and molecular biology.
“This adds a new dimension to the importance of RSV vaccines for both the elderly and mothers to protect their babies.”
Researchers studied the virus using 3D peripheral nerve cultures grown from stem cells and rat embryos.
After finding they can be infected by RSV, researchers found RSV induced the release of chemokines – proteins that fight infections by controlling immune cells – and caused significant inflammation.
With low levels of RSV infection, the nerves became hyperreactive to stimulation. At higher levels, they observed a progressive degeneration of the nerve and increased neurotoxicity due to excess inflammation.
“Until this study, the theory was that the inflammatory response was indirectly activating the nerves,” Piedimonte said.
“This study shows that not only does that happen, but the virus can penetrate directly into the nerves.”
The nerve hyperreactivity could explain why children who get RSV are later more likely to have asthmatic symptoms, Piedimonte said.
The study also found that RSV could enter the spinal cord via peripheral nerves despite not having the ability to enter the spinal neurons directly.
More research is needed to explore that mechanism, but Piedimonte theorises that by using the peripheral nerves to enter the spinal cord, RSV can bypass the blood-brain barrier, enter the central nervous system and infect the brain.
If confirmed, it could signal a connection between RSV and other neurological or developmental disorders, Piedimonte said.
“If indeed it’s confirmed in future studies that viruses like this are able to access the central nervous system, that opens a huge Pandora’s box,” Piedimonte said.
Hypnotisability appears to be a stable trait that changes little throughout adulthood, much like personality and IQ. But now, for the first time, Stanford Medicine researchers have demonstrated a way to temporarily heighten hypnotisablity, potentially allowing more people to access the benefits of hypnosis-based therapy.
In the new study, published in Nature Mental Health, the researchers found that less than two minutes of electrical stimulation targeting a precise area of the brain could boost participants’ hypnotisability for about one hour.
“We know hypnosis is an effective treatment for many different symptoms and disorders, in particular pain,” said lead author Afik Faerman, PhD, a postdoctoral scholar in psychiatry. “But we also know that not everyone benefits equally from hypnosis.”
Focused attention
Approximately two-thirds of adults are at least somewhat hypnotisable, and 15% are considered highly hypnotisable, meaning they score 9 or 10 on a standard 10-point measure of hypnotisability.
“Hypnosis is a state of highly focused attention, and higher hypnotisability improves the odds of your doing better with techniques using hypnosis,” said David Spiegel, MD, a professor of psychiatry and behavioural sciences and a senior author of the study.
Spiegel has devoted decades to studying hypnotherapy and using it to help patients control pain, lower stress, stop smoking and more. Several years ago, Spiegel led a team that used brain imaging to uncover the neurobiological basis of the practice. They found that highly hypnotisable people had stronger functional connectivity between the left dorsolateral prefrontal cortex, which is involved in information processing and decision making; and the dorsal anterior cingulate cortex, involved in detecting stimuli.
“It made sense that people who naturally coordinate activity between these two regions would be able to concentrate more intently,” Spiegel said. “It’s because you’re coordinating what you are focusing on with the system that distracts you.”
Shifting a stable trait
With these insights, Spiegel teamed up with Nolan Williams, MD, associate professor of psychiatry and behavioural sciences, who has pioneered non-invasive neurostimulation techniques to treat conditions such as depression, obsessive-compulsive disorder and suicidal ideation.
The hope was that neurostimulation could alter even a stable trait like hypnotisability.
In the new study, the researchers recruited 80 participants with fibromyalgia, a chronic pain condition that can be treated with hypnotherapy. They excluded those who were already highly hypnotisable.
Half of the participants received transcranial magnetic stimulation, in which paddles applied to the scalp deliver electrical pulses to the brain. Specifically, they received two 46-second applications that delivered 800 pulses of electricity to a precise location in the left dorsolateral prefrontal cortex. The exact locations depended on the unique structure and activity of each person’s brain.
“A novel aspect of this trial is that we used the person’s own brain networks, based on brain imaging, to target the right spot,” said Williams, also a senior author of the study.
The other half of participants received a sham treatment with the same look and feel, but without electrical stimulation. Hypnotisability was assessed by clinicians immediately before and after the treatments, with neither patients nor clinicians knowing who was in which group.
The researchers found that participants who received the neurostimulation showed a statistically significant increase in hypnotisability, scoring roughly one point higher. The sham group experienced no effect.
When the participants were assessed again one hour later, the effect had worn off and there was no longer a statistically significant difference between the two groups.
“We were pleasantly surprised that we were able to, with 92 seconds of stimulation, change a stable brain trait that people have been trying to change for 100 years,” Williams said. “We finally cracked the code on how to do it.”
The researchers plan to test whether different dosages of neurostimulation could enhance hypnotisability even more.
“It’s unusual to be able to change hypnotisability,” Spiegel said. A study of Stanford University students that began in the 1950s, for example, found that the trait remained relatively consistent when the students were tested 25 years later, as consistent as IQ over that time period. Recent research by Spiegel’s lab also suggests that hypnotisability may have a genetic basis.
Bigger implications
Clinically, a transient bump in hypnotisability may be enough to allow more people living with chronic pain to choose hypnosis as an alternative to long-term opioid use. Spiegel will follow up with the study participants to see how they fare in hypnotherapy.
The new results could have implications beyond hypnosis. Faerman noted that neurostimulation may be able to temporarily shift other stable traits or enhance people’s response to other forms of psychotherapy.
“As a clinical psychologist, my personal vision is that, in the future, patients come in, they go into a quick, non-invasive brain stimulation session, then they go in to see their psychologist,” he said. “Their benefit from treatment could be much higher.”
Researchers at the University of Tsukuba in Japan have discovered that oestrogen receptor (ER) β, expressed in the lateral septum of the limbic system, plays a crucial role in suppressing anxiety-like behaviour by male mice in social situations. Publishing their findings in Neuroscience, they also reported that the distribution and expression region of ERβ differs from that of ERα.
Oestradiol, a sex steroid hormone, plays an essential role in social behaviour, including regulating social anxiety, which is anxiety experienced when unknown individuals are encountered.
In males, testosterone secreted by the testes is converted to oestradiol in the brain, and the oestradiol binds to two types of oestrogen receptors (ERs), ERα and ERβ, to regulate social behaviour. However, its neuroendocrine basis has not been understood. In this study, the role of ERα and ERβ expressed in the lateral septum (LS), which regulates social anxiety, was investigated using male mice.
The researchers first investigated the expression of ERα and ERβ in the LS using genetically modified male mice. ERβ-expressing cells in the mice were labelled with red fluorescent protein, which revealed that the distributions of ERα and ERβ are different.
Furthermore, the researchers investigated the knockdown effects of ERα or ERβ gene expression in the LS of male mice during situations of social and nonsocial anxiety. The results show that social anxiety increases with the inhibition of ERβ expression.
Additionally, ERα- and ERβ-positive cells in the LS projected into different regions of the hypothalamus.
Thus, the researchers concluded that ERα- and ERβ-expressing cells in LS are distinct cell populations with different localisations and neuronal projections, and the ERβ population plays a crucial role in neural circuitry that regulates anxiety-like behaviour in social situations.
Ischaemic and haemorrhagic stroke. Credit: Scientific Animations CC4.0
Early neurological deterioration (END) within the first 48 hours after acute ischaemic stroke (AIS) onset is relatively common, and is a predictor of poor outcomes. Treatment options are limited and unproven, but but a clinical trial has shown that the anticoagulant argatroban was safe and effective in improving outcomes. The results were published in JAMA Neurology.
Apart from straightforward causes, such as intracerebral haemorrhage and malignant oedema, the mechanism of END remains mostly unclear. Interventions for unexplained END can include plasma volume expansion, induced hypertension, and intensified antithrombotic therapy, but none has been formally proved so far.
The direct thrombin inhibitor argatroban is rapid acting, short acting, and has low bleeding rates, which could help prevent thrombus propagation and provide additional benefit after stroke/TIA. Argatroban has been associated with a reduction in ischaemic stroke damage but the safety and efficacy of argatroban is not well established for AIS treatment, and evidence is lacking for the effect of argatroban in patients with AIS and END.
Researchers conducted a randomised clinical trial that initially included 628 patients, average age 65 and 400 (63.7%) male. Eligible patients were adults with AIS who experienced END, which was defined as an increase of 2 or more points on the National Institutes of Health Stroke Scale within 48 hours from symptom onset.
Patients were randomly assigned to the argatroban group and control group within 48 hours of symptom onset. Both groups received standard therapy based on guidelines, including oral mono or dual antiplatelet therapy. The argatroban group received intravenous argatroban for 7 days (continuous infusion at a dose of 60mg per day for 2 days, followed by 20mg per day for 5 days) in addition to standard therapy.
The results showed that good neurological function at 90 days in those randomised to receive argatroban plus antiplatelet compared with antiplatelet alone was observed in 80.5% vs 73.7%)of participants, a statistically significant difference.
The authors concluded that the trial “shows that the combination of argatroban and antiplatelet therapy resulted in a significantly greater likelihood of good functional outcome at 90 days in patients with END after AIS, with no additional risk of major intracranial or extracranial haemorrhage.”
When 67-year-old Larry Christian suffered a sudden loss of balance, he was diagnosed with a haemorrhagic stroke, and referred to the University of Delaware’s Physical Therapy Clinic for rehabilitation.
“Initially, I had a lot of balance problems that we worked pretty intensely to correct,” Christian said.
He enrolled in a clinical trial at UD, led by co-investigator Darcy Reisman, professor and chair of the Department of Physical Therapy, that sought to explore whether high-intensity interval training (HIIT) aids in improved gait post-stroke. UD was one of three sites selected for the clinical trial led by primary investigator and associate professor Pierce Boyne of the University of Cincinnati. Sandra Billinger, professor and vice chair of stroke translation research at the University of Kansas Medical Center, is also a co-investigator and represents the third site involved in the clinical trial.
Now, seven years later, Christian is walking better.
“Participating in this study got me to a point where I could walk better and even take a walk outside,” Christian said. “I’ve been pretty healthy all my life, and while I can’t play volleyball anymore, walking again made me feel great.”
Christian is among the lucky ones. Among 7 million stroke survivors in the US, fewer than 10% have adequate walking speed and endurance to complete normal daily activities like grocery shopping.
Reisman said the results of the multi-million-dollar, five-year clinical trial showed HIIT helped more people than just Christian. The results, published in JAMA Neurology, show that chronic stroke survivors who engaged in high-intensity exercise with bursts of maximum-speed walking alternated with recovery periods saw a significant difference in their walking capacity over 12 weeks. The improvements were so dramatic Boyne and Reisman have secured a clinical trial grant renewal to triple the size of their study to 165 participants.
She added HIIT looks different for each stroke survivor, and the optimal exercise program for each person with stroke remains unknown.
“We want them to train at the fastest possible speed, which varies from person to person,” Reisman said. “But we don’t want them running.”
For those already walking at a reasonably fast pace, research associate Henry Wright in Reisman’s lab will add an incline or a weighted vest or wrap a bungee cord around their waist to create resistance.
“It’s self-reported data, but participants tell me they have more energy, or they’re able to do more around the house, or they’re not winded when they go shopping,” Wright said. “By the end of the training, I can see their walking is smoother, they’re getting farther on clinical testing, and it’s rewarding to see their gains.”
The results from the initial clinical trial showed Reisman and collaborators that HIIT was feasible and safe in a small group of stroke survivors, who saw sustained gains in walking capacity, more so than patients engaged in moderate-intensity exercise.
However, further study of the intervention in larger populations is crucial to change the standard of care.
“Many physical therapists were trained during a time when patients with neurologic conditions, particularly stroke, were treated with kid gloves, partly because they say stroke is the heart attack of the brain,” Reisman said. “It’s common they also have cardiovascular conditions, so people tend to be extra careful with those patients in terms of pushing them.
“But what we know now is at least moderate-intensity, and likely high-intensity interval training, is essential not only for stroke survivors’ cardiovascular system but also for their brain,” Reisman said. “The evidence shows that intensity is linked to the release of neurotrophins in the brain that help the brain remodel after a stroke.”
Kiersten McCartney, a physical therapist obtaining her doctorate in biomechanics and movement science, worked on the clinical trial with Reisman. She spent the 2022 Winter Session at Magee Rehabilitation Hospital in Philadelphia, helping them implement moderate-to-high-intensity exercise and saw the benefits first-hand.
“I’ll never be able to say there’s no risk of heart attack. Even the fittest people can have a heart attack when exercising,” McCartney said. “Still, the data points to the idea that you’re doing more harm than good by not engaging your patients with stroke in high-intensity exercise when we talk about those longer-term outcomes.”
The HIIT-Stroke Trial 2 will continue to examine dosing to confirm whether a full 12 weeks of vigorous exercise is needed to see significant improvements in walking. Reisman and collaborators will identify whether differences in sex and other factors played a role in rehabilitation. If the five-year study results are similar and show significant gains from high-intensity interval exercise in a larger population, investigators would next work with NIH Strokenet to launch a nationwide clinical trial in people with stroke.
“We’ve known about the value of moderate-intensity exercise for more than a decade, and it’s still not the standard of care,” Reisman said. “If we find that HIIT is the optimal intervention, the next phase would be the knowledge translation phase, where we’d systematically develop a methodology to get HIIT into clinics.”
For HIIT to work as an intervention, Reisman said therapists will need the proper tools. She’s been pushing for commercially available heart rate monitors, placed around the chest during exercise, to be the standard of care in clinics for years.
“They’re already a standard of care for people in the community,” Reisman said. “Getting them into clinics is imperative so PTs can monitor patients’ heart rate the entire time they exercise. That constant monitoring gives therapists data on how a person is responding beyond visible signs and symptoms, and in turn, more peace of mind.”
But beyond tools and training, Reisman said, it comes down to evidence and education.
“If we have hundreds and hundreds of stroke survivors who’ve gone through our high-intensity exercise intervention, and we’ve seen no major adverse events – that will help,” Reisman said. “The more data we have to show therapists, the better we can implement this intervention that will change lives.”
People who have more disrupted sleep in their 30s and 40s may be more likely to have memory and thinking problems a decade later, according to new research published in Neurology. The study does not however prove that sleep quality causes cognitive decline, it only shows an association.
“Given that signs of Alzheimer’s disease start to accumulate in the brain several decades before symptoms begin, understanding the connection between sleep and cognition earlier in life is critical for understanding the role of sleep problems as a risk factor for the disease,” said study author Yue Leng, PhD, of the University of California, San Francisco.
“Our findings indicate that the quality rather than the quantity of sleep matters most for cognitive health in middle age.”
The study involved 526 people, average age of 40, who were followed for 11 years. Researchers looked at participants’ sleep duration and quality, and had them perform cognitive tests.
Participants wore a wrist activity monitor for three consecutive days on two occasions approximately one year apart to calculate their averages. Participants slept for an average of six hours.
Participants also reported bedtimes and wake times in a sleep diary and completed a sleep quality survey with scores ranging from zero to 21, with higher scores indicating poorer sleep quality. A total of 239 people, or 46%, reported poor sleep with a score greater than five. Participants also completed a series of memory and thinking tests.
Researchers also looked at sleep fragmentation, which measures repetitive short interruptions of sleep. They looked at both the percentage of time spent moving and the percentage of time spent not moving for one minute or less during sleep. Added together, participants had an average sleep fragmentation of 19%.
Researchers then divided participants into three groups based on their sleep fragmentation score. Of the 175 people with the most disrupted sleep, 44 had poor cognitive performance 10 years later, compared to 10 of the 176 people with the least disrupted sleep.
After adjusting for age, gender, race, and education, people who had the most disrupted sleep had more than twice the odds of having poor cognitive performance when compared to those with the least disrupted sleep.
There was no difference in cognitive performance at midlife for those in the middle group compared to the group with the least disrupted sleep.
“More research is needed to assess the link between sleep disturbances and cognition at different stages of life and to identify if critical life periods exist when sleep is more strongly associated with cognition,” Leng said.
“Future studies could open up new opportunities for the prevention of Alzheimer’s disease later in life.”
The amount of time people slept and their own reports of the quality of their sleep were not associated with cognition in middle age.
Microglia, the brain’s immune cells, can trigger cognitive deficits after radiation exposure and may be a key target for preventing these symptoms, University of Rochester researchers have found. Their work, published in the International Journal of Radiation Oncology Biology Biophysics, builds on previous research showing that after radiation exposure microglia damage synapses, the connections between neurons that are important for cognitive behaviour and memory.
“Cognitive deficits after radiation treatment are a major problem for cancer survivors,” M. Kerry O’Banion, MD, PhD, professor of Neuroscience, member of the Wilmot Cancer Institute, and senior author of the study said.
“This research gives us a possible target to develop therapies to prevent or mitigate against such deficits in people who need brain radiotherapy.”
Using several behavioural tests, researchers investigated the cognitive function of mice before and after radiation exposure.
Female mice performed the same throughout, indicating a resistance to radiation injury but Male mice could not remember or perform certain tasks after radiation exposure.
This cognitive decline correlates with the loss of synapses and evidence of potentially damaging microglial over-reactivity following the treatment.
Researchers then targeted the pathway in microglia important to synapse removal. Mice with these mutant microglia had no cognitive decline following radiation. And others that were given the drug, Leukadherin-1, which is known to block this same pathway, during radiation treatment, also had no cognitive decline.
“This could be the first step in substantially improving a patient’s quality of life and need for greater care,” said O’Banion. “Moving forward, we are particularly interested in understanding the signals that target synapses for removal and the fundamental signaling mechanisms that drive microglia to remove these synapses. We believe that both avenues of research offer additional targets for developing therapies to help individuals receiving brain radiotherapy.”
O’Banion also believes this work may have broader implications because some of these mechanisms are connected to Alzheimer’s and other neurodegenerative diseases.
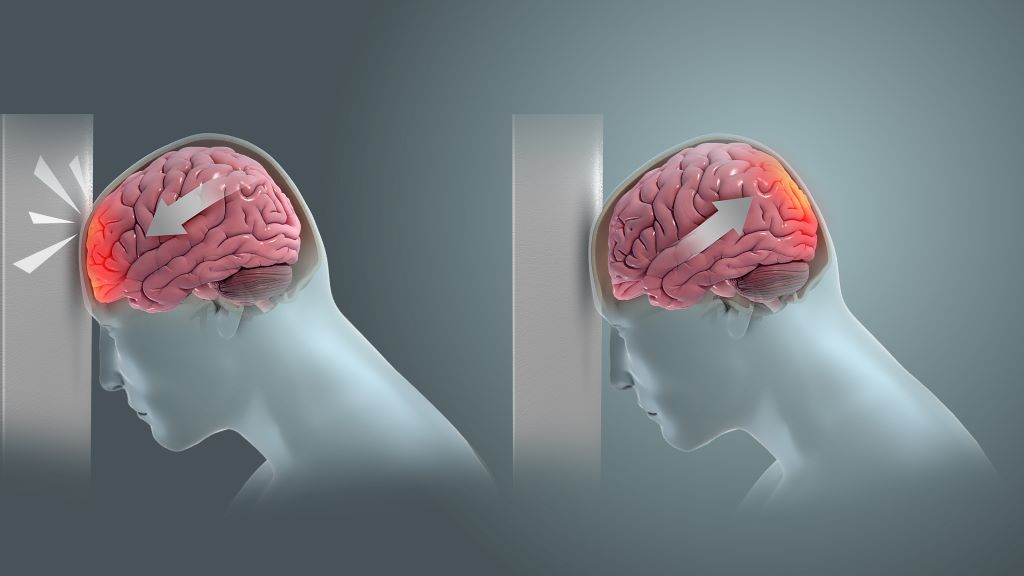
Coup and contrecoup brain injury. Credit: Scientific Animations CC4.0
Researchers have created a new brain imaging method that allows to be diagnosed, even when existing imaging techniques like magnetic resonance imaging (MRI) The technique involves loading gadolinium, a standard MRI contrast agent, into ‘backpacks’ that are attached macrophages. mTBIs cause inflammation, attracting macrophages there. Coupling the gadolinium contrast agent to these cells enables MRI to reveal brain inflammation and increase the number of correctly diagnosed mTBI cases, improving patient care. The method is described in a new paper in Science Translational Medicine.
“70-90% of reported TBI cases are categorised as ‘mild,’ yet as many as 90% of mTBI cases go undiagnosed, even though their effects can last for years and they are known to increase the risk of a host of neurological disorders including depression, dementia, and Parkinson’s disease,” said senior author Samir Mitragotri, PhD, in whose lab the research was performed. “Our cell-based imaging approach exploits immune cells’ innate ability to travel into the brain in response to inflammation, enabling us to identify mTBIs that standard MRI imaging would miss.”
Using immune cells to identify inflammation
Most of us know someone who has had a concussion (another name for an mTBI), sometimes even more than one. But the vast majority of people who experience an mTBI are never properly diagnosed. Without that diagnosis, they can exacerbate their injuries by returning to normal activity before they’re fully recovered, which can lead to further damage. Some studies even suggest that repeated mTBIs can lead to chronic traumatic encephalopathy (CTE), the neurodegenerative disease that has been found to afflict more than 90% of professional American football players.
Because the effects of mTBI are believed to be caused by “invisible” brain inflammation, members of the Mitragotri lab decided to leverage their experience with immune cells to create a better diagnostic. “Our previous projects have focused on controlling the behaviour of immune cells or using them to deliver drugs to a specific tissue. We wanted to exploit another innate ability of immune cells – homing to sites of inflammation in the body – to carry imaging agents into the brain, where they can provide a visible detection signal for mTBI,” said first author Lily Li-Wen Wang, Ph.D.. Wang is a former Research Fellow in the Mitragotri Lab at the Wyss Institute and SEAS who is now a scientist at Landmark Bio.
Gadolinium needs water to show up on MRI
The team planned to use their cellular backpack technology to attach gadolinium molecules to macrophages, known to infiltrate the brain in response to inflammation. But right away, they ran into a problem: in order to function as a contrast agent for MRI scans, gadolinium needs to interact with water. Their original backpack microparticles are made of a hydrophobic polymer called PLGA. So Wang and her co-authors started developing a new backpack made out of a hydrogel material that could be manufactured at a large scale in the lab.
After years of hard work, they finally created a new hydrogel backpack that could produce a strong gadolinium-mediated MRI signal, attach stably to both mouse and pig macrophages, and maintain their cargo for a sustained period of time in vitro. They named their new microparticles M-GLAMs, short for “macrophage-hitchhiking Gd(III)-Loaded Anisotropic Micropatches.” Now, it was time to test them in a more realistic setting, for which they partnered with researchers and clinicians at Boston Children’s Hospital.
First, they injected mouse M-GLAMs macrophages into mice to see if they could visualize them in vivo. They were especially interested to see if they accumulated in the kidney, as existing gadolinium-based contrast agents like Gadavist® can cause health risks for patients with kidney disease. Their M-GLAMs did not accumulate in the mice’s kidneys, but persisted in their bodies for over 24 hours with no negative side effects. In contrast, mice injected with Gadavist® showed substantial accumulation of the contrast agent in their kidneys within 15 minutes of injection, and the substance was fully cleared from their bodies within 24 hours.
Then, they tested porcine M-GLAMs in a pig model of mTBI. They injected the M-GLAMs into the animals’ blood two days after a mock mTBI, then used MRI to evaluate the concentration of gadolinium in the brain. They focused on a small region called the choroid plexus, which is known as a major conduit of immune cells into the brain. Pigs that received the M-GLAMs displayed a significant increase in the intensity of gadolinium present in the choroid plexus, while those injected with Gadavist® did not, despite confirmation of increased inflammation macrophage density in the brains of both groups. The animals showed no toxicity in any of their major organs following administration of the treatments.
“Another important aspect of our M-GLAMs is that we are able to achieve better imaging at a much lower dose of gadolinium than current contrast agents – 500-1000-fold lower in the case of Gadavist®,” said Wang. “This could allow the use of MRI for patients who are currently unable to tolerate existing contrast agents, including those who have existing kidney problems.”
A new study from researchers at the University of Colorado Anschutz Medical Campus finds that older adult drivers who are recently diagnosed with migraines are three times as likely to experience a motor vehicle crash. Older adult drivers who reported having ever had migraines in the past were no more likely to have a motor vehicle crash than those without migraines.
The study, published in the Journal of the American Geriatrics Society, also explored the relationships medications commonly prescribed for migraine management have with increased crash risk.
“Migraine headaches affect more than 7% of US adults over the age of 60,” says Carolyn DiGuiseppi, MPH, PhD, MD, professor with the Colorado School of Public Health and study lead author.
“The US population is aging, which means increasing numbers of older adult drivers could see their driving abilities affected by migraine symptoms previously not experienced. These symptoms include sleepiness, decreased concentration, dizziness, debilitating head pain and more.”
Researchers conducted a five-year longitudinal study of more than 2500 active drivers aged 65-79 in five sites across the United States.
Participants were categorised as having previously been diagnosed with migraine symptoms (12.5%), no previous diagnosis but experienced symptoms during the study timeframe (1.3%) or never migraine respondents.
Results indicate those with previous diagnosis did not have a different likelihood of having crashes after baseline, while those with new onset migraines were three times as likely to experience a crash within one year of diagnosis.
Previously diagnosed drivers nevertheless had experienced more hard braking events compared to adults who had never experienced a migraine.
Additionally, researchers examined the role medications commonly prescribed for migraines have in motor vehicle events and found that there was no impact on the relationship between migraines and either crashes or driving habits.
Few participants in the study sample were using acute migraine medications, however.
“These results have potential implications for the safety of older patients that should be addressed,” says DiGuiseppi. “Patients with a new migraine diagnosis would benefit from talking with their clinicians about driving safety, including being extra careful about other risks, such as distracted driving, alcohol, pain medication and other factors that affect driving.”
A review in the Journal of Internal Medicine explores the potential of non-invasive interventions such as light, sound, and magnets to stimulate gamma brain waves for the treatment of Alzheimer’s disease. Such strategies may be beneficial because Alzheimer’s disease is characterised by reduced fast brain oscillations in the gamma range (30–100Hz).
The authors note that recent studies reveal that it is feasible and safe to induce 40Hz brain activity in patients with Alzheimer’s disease through a range of methods. Also, preliminary evidence suggests that such treatment can yield beneficial effects on brain function, disease pathology, and cognitive function in patients.
Various cells in the brain beyond neurons, including microglial cells, astrocytes and vascular cells, seem to be involved in mediating these effects.
“We found that increased gamma activity elicited by the non-invasive 40Hz sensory stimulation profoundly alters the cellular state of various glial cell types,” said corresponding author Li-Huei Tsai, PhD, of MIT. “We are actively investigating the mechanism by which the 40Hz brain activity recruits diverse cell types in the brain to provide neuroprotective effects.”