Scanning electron micrograph of a T cell lymphocyte. Credit: NIH / NIAID
A study initiated by a University of Arizona Comprehensive Cancer Center physician-scientist has for the first time defined how loss of the Y chromosome in male immune cells negatively affects immune system function. The findings, published in Nature, may explain why loss of Y is associated with lower cancer survival rates.
In males, each cell in the body usually contains one X and one Y chromosome. “Loss of Y” is a common, nonhereditary genetic change in men in which an immune cell in the blood loses its Y chromosome. It is often associated with aging. Loss of Y has been linked to increased mortality from carcinomas for many years, though no one knew why.
This study is the first to identify and define the relationship between loss of Y in white blood cells, immune cells and tumours, providing insights as to why men with loss of Y have increased cancer risks and poorer outcomes.
“These findings represent a big step forward in our understanding of why men with loss of Y in their blood cells have a higher mortality from cancer. It turns out it’s because these cells make the immune system infiltrating the cancer less effective,” said Dan Theodorescu, MD, PhD, director of the Cancer Center and a professor in the College of Medicine – Tucson.
“We hope this provides a solid lead and framework for the nascent Y chromosome field to pursue so we can collectively better understand all the possible biological implications of this finding and how to use them to develop more effective approaches in prevention, treatment resulting in higher survival rates for patients.”
The research team discovered that loss of the Y chromosome – previously identified in malignant epithelial cells by the Theodorescu lab – also occurred in nearby noncancerous tissues, including connective tissue and immune cells.
Most notably, the team found that this chromosomal loss in helper and cytotoxic T cells, which are responsible for attacking cancer cells, was associated with a reduced ability to kill those cancerous cells. The findings suggest a mechanism by which tumours may evade immune detection and suppression.
Finally, the research team found that loss of Y in epithelial cells, combined with loss of Y in T cells, resulted in more aggressive cancers and lower survival rates in patients.
“The study has potential implications for current immunotherapies, including CAR T therapy,” Theodorescu said. “Further research is clearly needed but perhaps immunotherapies using cells from a patient’s immune system could be screened for loss of Y before being used in treatment.”
A breakthrough study from the Hebrew University of Jerusalem, published this week in the prestigious journal PNAS (Proceedings of the National Academy of Sciences USA), reveals a previously unknown peripheral mechanism by which paracetamol relieves pain.
The study was led by Prof Alexander Binshtok from the Hebrew University’s Faculty of Medicine and Center for Brain Sciences (ELSC) and Prof Avi Priel from its School of Pharmacy. Together, they uncovered a surprising new way that paracetamol, one of the world’s most common painkillers, actually works.
For decades, scientists believed that paracetamol relieved pain by working only in the brain and spinal cord. But this new research shows that the drug also works outside the brain, in the nerves that first detect pain.
Their discovery centres on a substance called AM404, which the body makes after taking paracetamol. The team found that AM404 is produced right in the pain-sensing nerve endings – and that it works by shutting off specific channels (called sodium channels) that help transmit pain signals. By blocking these channels, AM404 stops the pain message before it even starts.
“This is the first time we’ve shown that AM404 works directly on the nerves outside the brain,” said Prof Binshtok. “It changes our entire understanding of how paracetamol fights pain.”
This breakthrough could also lead to new types of painkillers. Because AM404 targets only the nerves that carry pain, it may avoid the numbness, muscle weakness, and side effects that come with traditional local anaesthetics.
“If we can develop new drugs based on AM404, we might finally have pain treatments that are highly effective but also safer and more precise,” added Prof Priel.
Cells taken from the lungs of people with chronic obstructive pulmonary disease (COPD) have a larger accumulation of soot-like carbon deposits compared to cells taken from smokers without COPD, according to a study published in ERJ Open Research. Carbon can enter the lungs via cigarette smoke, diesel exhaust and polluted air.
The cells, called alveolar macrophages, normally protect the body by engulfing any particles or bacteria that reach the lungs. But, in their new study, researchers found that when these cells are exposed to carbon they grow larger and encourage inflammation.
The research was led by Dr James Baker and Dr Simon Lea from the University of Manchester, UK. Dr Baker said: “COPD is a complex disease that has a number of environmental and genetic risk factors. One factor is exposure to carbon from smoking or breathing polluted air.
“We wanted to study what happens in the lungs of COPD patients when this carbon builds up in alveolar macrophage cells, as this may influence the cells’ ability to protect the lungs.”
The researchers used samples of lung tissue from surgery for suspected lung cancer. They studied samples (that did not contain any cancer cells) from 28 people who had COPD and 15 people who were smokers but did not have COPD.
Looking specifically at alveolar macrophage cells under a microscope, the researchers measured the sizes of the cells and the amount of carbon accumulated in the cells.
They found that the average amount of carbon was more than three times greater in alveolar macrophage cells from COPD patients compared to smokers. Cells containing carbon were consistently larger than cells with no visible carbon.
Patients with larger deposits of carbon in their alveolar macrophages had worse lung function, according to a measure called FEV1%, which quantifies how much and how forcefully patients can breathe out.
When the researchers exposed macrophages to carbon particles in the lab, they saw the cells become much larger and found that they were producing higher levels of proteins that lead to inflammation.
Dr Lea said: “As we compared cells from COPD patients with cells from smokers, we can see that this build-up of carbon is not a direct result of cigarette smoking. Instead, we show alveolar macrophages in COPD patients contain more carbon and are inherently different in terms of their form and function compared to those in smokers.
“Our research raises an interesting question as to the cause of the increased levels of carbon in COPD patients’ macrophages. It could be that people with COPD are less able to clear the carbon they breathe in. It could also be that people exposed to more particulate matter are accumulating this carbon and developing COPD as a result.
“In future, it would be interesting to study how this carbon builds up and how lung cells respond over a longer period of time.”
Though blood clots can form in both arteries and veins, the reasons behind them differ, as do the consequences and the chances of preventing blood clots. In Sweden, almost half of all cases of venous thrombosis have a genetic explanation. A team of researchers from Lund University in Sweden has now discovered three gene variants that increase the risk of blood clots in the leg by up to 180%.
There is a difference between arterial and venous blood clots. Blood clots in the arteries form when plaque in calcified vessels bursts and the body perceives it as an injury. This activates the platelets, which clump together and form a clot. In the worst case, it can lead to a stroke or heart attack. A venous thrombus, on the other hand, usually forms in the leg when the blood stagnates for too long. This can activate the body’s coagulation system, allowing the clotting system to be activated and the blood to clot, blocking blood flow. If the clot breaks loose and travels with the blood to the lungs, it can lead to pulmonary embolism, a life-threatening condition.
“Venous thrombosis is in fact one of the most common causes of death in the world. It is a common disease that has always been somewhat overshadowed by arterial blood clots,” says Bengt Zöller, a specialist in general medicine at Skåne University Hospital and professor of general medicine at Lund University.
In Sweden, more than 10 000 people suffer from venous thromboembolism each year and that number appears to be increasing. Several factors are contributing to this increase. One of the strongest risk factors is age, and as the number of older people in Sweden grows, the number of clots is also increasing. Ten per cent of 80-year-olds experience a blood clot at some point. The risk also increases if you are overweight or tall.
“The muscles control the blood flow in the veins and the legs become like columns of fluid where the force of gravity is strong. Too much sedentary and inactive behaviour, then, is harmful. Only the valves of the veins prevent backflow and if these are damaged, the risk of blood clots can increase. Therefore, tall people are more prone to blood clots, as their larger veins provide less blood flow, combined with the fact that blood must travel a greater distance back to the heart.”
Because the heart pumps blood out into the arteries, there is much higher blood pressure in the arteries than in the veins, which can contribute to atherosclerosis. High blood pressure, high levels of blood lipids and smoking are all risk factors for atherosclerosis of the arteries. But because the veins are a low-pressure system, the vessels do not become atherosclerotic. Therefore, neither high blood pressure nor blood lipids are associated with venous clots and smoking is considered only a weak to moderate risk factor. Being overweight, on the other hand, is a very significant culprit. Obesity has a negative impact on venous circulation, especially when combined with the fact that overweight people are often less active. Some clotting factors are also affected by obesity.
“In terms of diet, there are fewer studies, but ultra-processed foods have been associated with a slightly increased risk of blood clots, and plant-based, healthy foods with a reduced risk. In our studies, we have also seen that commercial fishermen have a lower risk, which may be due to a higher omega-3 content in their diet.”
There are also specific situations in which the risk of venous blood clots is particularly high. The risk of blood clots increases when blood flow is reduced, such as when travelling by air for long periods of time or when lying in bed for several days. Surgery or inflammation that damages the vessel wall can also lead to an increased tendency to clot. Particularly during pregnancy, blood clotting factors increase and levels of some protective proteins may decrease.
“In these risk situations, prophylaxis in the form of blood thinners may be particularly important if other risk factors are also present.”
Other risk factors are the genetic variants that affect different parts of the blood’s clotting ability. In Sweden, we have a high prevalence of APC (activated protein C) resistance due to an inherited mutation in the gene for coagulation factor V, called Factor V Leiden. About 10 per cent of Swedes have this mutation, which is considered the most common coagulation mutation among Indo-Europeans.
“Evolutionarily, bleeding less has been an advantage, but in our modern, sedentary society, APC resistance is becoming a risk factor.”
Bengt Zöller and his fellow researchers have now identified the strongest genetic risk factor since Factor V Leiden was discovered. They used data from the population-based Malmö Kost Cancer study, involving 30,000 Malmö residents. By selecting 27 genes previously associated with clotting disorders, they found three variants that, when taken together, were as significant a risk factor for venous blood clots as Factor V Leiden: ABO, F8, and VWF each increased the risk of venous blood clots by 10 to 30 percent.
“And the more of these variants a person has – the higher the risk. An individual with five of these gene variants has a 180 per cent higher risk of venous thrombosis. Unlike Factor V Leiden, which is only found in Indo-Europeans, these three different mutations are found in between five and fifty per cent of various populations around the globe.”
As these genetic variants are present in all populations, the next step is to investigate how the number of risk genes affects the duration of treatment with anticoagulants after a blood clot.
“I think tailoring treatment based on risk assessment will become increasingly important,” concludes Bengt Zöller.
A new study led by Keck Medicine of USC researchers may have uncovered an effective combination therapy for glioblastoma, a brain tumour diagnosis with few available effective treatments. According to the National Brain Tumor Society, the average survival for patients diagnosed with glioblastoma is eight months.
The study, which was published in the journal Med, finds that using Tumour Treating Fields therapy (TTFields), which delivers targeted waves of electric fields directly into tumours to stop their growth and signal the body’s immune system to attack cancerous tumour cells, may extend survival among patients with glioblastoma, when combined with immunotherapy (pembrolizumab) and chemotherapy (temozolomide).
TTFields disrupt tumour growth using low-intensity, alternating electric fields that push and pull key structures inside tumour cells in continually shifting directions, making it difficult for the cells to multiply. Preventing tumour growth gives patients a better chance of successfully fighting the cancer. When used to treat glioblastoma, TTFields are delivered through a set of mesh electrodes that are strategically positioned on the scalp, generating fields at a precise frequency and intensity focused on the tumour. Patients wear the electrodes for approximately 18 hours a day.
Researchers observed that TTFields attract more tumour-fighting T cells, which are white blood cells that identify and attack cancer cells, into and around the glioblastoma. When followed by immunotherapy, these T cells stay active longer and are replaced by even stronger, more effective tumour-fighting T cells.
“By using TTFields with immunotherapy, we prime the body to mount an attack on the cancer, which enables the immunotherapy to have a meaningful effect in ways that it could not before,” said David Tran, MD, PhD, chief of neuro-oncology with Keck Medicine, co-director of the USC Brain Tumor Center and corresponding author of the study. “Our findings suggest that TTFields may be the key to unlocking the value of immunotherapy in treating glioblastoma.”
TTFields are often combined with chemotherapy in cancer treatment. However, even with aggressive treatment, the prognosis for glioblastoma remains poor. Immunotherapy, while successful in many other cancer types, has also not proved effective for glioblastoma when used on its own.
However, in this study, adding immunotherapy to TTFields and chemotherapy was associated with a 70% increase in overall survival. Notably, patients with larger, unresected (not surgically removed) tumours showed an even stronger immune response to TTFields and lived even longer. This suggests that, when it comes to kick-starting the body’s immune response against the cancer, having a larger tumour may provide more targets for the therapy to work against.
Using alternating electric fields to unlock immunotherapy
Pembrolizumab, the immunotherapy used in this study, is an immune checkpoint inhibitor (ICI), which enhances the body’s natural ability to fight cancers by improving T cells’ ability to identify and attack cancer cells.
However, there are typically few T cells in and around glioblastomas because these tumours originate in the brain and are shielded from the body’s natural immune response by the blood-brain barrier. This barrier safeguards the brain by tightly regulating which cells and substances enter from the bloodstream. Sometimes, this barrier even blocks T cells and other therapies that could help kill brain tumours.
This immunosuppressive environment inside and around the glioblastoma is what makes common cancer therapies like pembrolizumab and chemotherapy significantly less effective in treating it. Tran theorised the best way to get around this issue was to start an immune reaction directly inside the tumour itself, an approach known as in situ immunisation, using TTFields.
This study demonstrates that combining TTFields with immunotherapy triggers a potent immune response within the tumour – one that ICIs can then amplify to bolster the body’s own defence against cancer.
“Think of it like a team sport – immunotherapy sends players in to attack the tumour (the offence), while TTFields weaken the tumour’s ability to fight back (the defence). And just like in team sports, the best defence is a good offence,” said Tran, who is also a member of the USC Norris Comprehensive Cancer Center.
Study methodology and results
The study analysed data from 2-THE-TOP, a Phase 2 clinical trial, which enrolled 31 newly diagnosed glioblastoma patients who had completed chemoradiation therapy. Of those, 26 received TTFields combined with both chemotherapy and immunotherapy. Seven of these 26 patients had inoperable tumours due to their locations – an especially high-risk subgroup with the worst prognosis and few treatment options.
Patients in the trial were given six to 12 monthly treatments of chemotherapy alongside TTFields for up to 24 months. The number and duration of treatments were determined by patients’ response to treatment. The immunotherapy was given every three weeks, starting with the second dose of chemotherapy, for up to 24 months.
Patients who used the device alongside chemotherapy and immunotherapy lived approximately 10 months longer than patients who had used the device with chemotherapy alone in the past. Moreover, those with large, inoperable tumours lived approximately 13 months longer and showed much stronger immune activation compared to patients who underwent surgical removal of their tumours.
“Further studies are needed to determine the optimal role of surgery in this setting, but these findings may offer hope, particularly for glioblastoma patients who do not have surgery as an option,” said Tran.
The researchers are now moving ahead to a Phase 3 trial.
A Durban-based cardiologist has secured a “gagging order” against Carte Blanche, stopping it from broadcasting a programme in which patients accuse him of medical malpractice for inserting stents unnecessarily.
Dr Ntando Peaceman Duze was given multiple opportunities for more than a week to respond to the allegations raised by his patients, which were corroborated by independent experts. But instead of responding, he launched an urgent application in the Kwazulu-Natal High Court in Pietermaritzburg on Friday.
He gave Carte Blanche only one day’s notice of the application.
Carte Blanche opposed it, arguing that Duze wanted to “bury these allegations for as long as possible if not indefinitely”, and that he was seeking an “unlawful prior restraint on freedom of speech and media”.
But Acting Judge Mpumelelo Sibisi granted an interim interdict, stopping the broadcast scheduled for Sunday 8 June.
Judge Sibisi said Duze needed to be given an opportunity to file a replying affidavit and that Carte Blanche had put a “gun to his head” to answer the questions posed to him. The judge said it would be appropriate to interdict the broadcast until the matter could be properly ventilated.
He set the return date for 13 June. But unless the matter is given a special allocation, it may not be argued and finalised on that day.
Cardiologists accused of defamation
Duze, who runs his practice from Life Westville Hospital, initially cited two other cardiologists in his application, seeking orders that they must desist from making “slanderous, insulting and defamatory remarks” about him.
He put this down to professional jealousy because their patients had moved over to his practice.
He alleged that the two cardiologists had instigated complaints laid by about seven of his patients against him with the Health Professionals Council of South Africa (HPCSA). He claimed that such was the professional jealousy, that he had been a victim of “witchcraft”, with chicken bones and red [Hindu] strings being left in the operating theatre.
He said the cardiologists had told his patients that “I had opened up their blood vessels” [an apparent reference to stent surgery], when it was unnecessary to do so.
Duze said the complaints to the HPCSA were “baseless”.
The cardiologists opposed the application.
Then on Friday, Duze’s legal team withdrew the claim against the cardiologists, and tendered to pay their legal costs. The lawyers gave no explanation for this. But it came in the wake of Carte Blanche, in its affidavit, saying they had not interviewed the cardiologists. Instead they had interviewed Duze’s aggrieved patients on camera and done follow-up investigations, including obtaining independent medical corroboration based on the patients’ medical records.
Gag order
Duze, in his application, said at any given time he had an average of 50 patients at the hospital, all with heart conditions. He had never before been reported to the HPCSA and, if the allegations against him continued and were made public on Carte Blanche, it would severely harm his reputation, “and may even lead to my financial demise”.
“Carte Blanche launched their own investigation and wants to broadcast a programme about this on Sunday 8 June, which I want to prevent, because it will be filled with untruths and defamation,” he said.
He said Carte Blanche had approached him for comment, and asked 14 specific questions, which he was not prepared to answer because the issue was “sub judice”.
“Once the [HPCSA] has completed its investigation, I will no doubt be willing to be interviewed and explain everything, because I will no doubt be cleared of these false allegations,” he said.
In her opposing affidavit, Carte Blanche producer Mart-Marie Faure said the application was an “abuse of process”.
“It is unsustainable on the facts and law and constitutes an impermissible attempt to obtain a pre-publication interdict in circumstances where no case has been made out for one and such an extreme order is not justified,” she said.
“The complaints, which form the subject matter of the inset entitled ‘Dr Stent’, were initiated by his patients, who had all, they allege, been subjected to unnecessary surgical procedures.
“Independent medical professionals who have been interviewed or consulted all confirm that the applicant [Duze] undertook unnecessary surgery that has had adverse consequences for his patients.
“This has nothing to do with jealous colleagues. The complaints are driven by his patients who allege serious medical malpractice with the most grave medical consequences.”
Faure said she had engaged with Duze and his attorneys for nine days in an attempt to secure answers to her questions “to no avail”.
“Carte Blanche was contacted by patients who claimed they were operated on unnecessarily. They consulted with other medical professionals who have said the insertion of stents was unnecessary. And in fact had caused heart disease when none was previously present.
“They will be required to take blood thinning and other medication for the rest of their lives.
“The HPCSA confirmed it received five complaints against the applicant.
“Life Healthcare has confirmed that it received information regarding allegations against the applicant from the HPCSA and has initiated an investigation.”
Faure said the complaints were not sub judice and that the explanation the doctor would advance to justify his conduct in that investigation would no doubt be the same he would give on camera or in a written response.
“If media houses were required to await the finalisation of proceedings before any professional or regulatory body, the public would be deprived of timely, relevant information on matters of pressing concern,” she said.
“This is antithetical to the very purpose of a free press.
“The patients’ accounts are based on their personal experiences and have been corroborated by independent experts. In every such story the person in respect of whom the investigation is conducted is unhappy. The remedy is to tell their side of the story, which the applicant has been repeatedly offered – not to gag the media.”
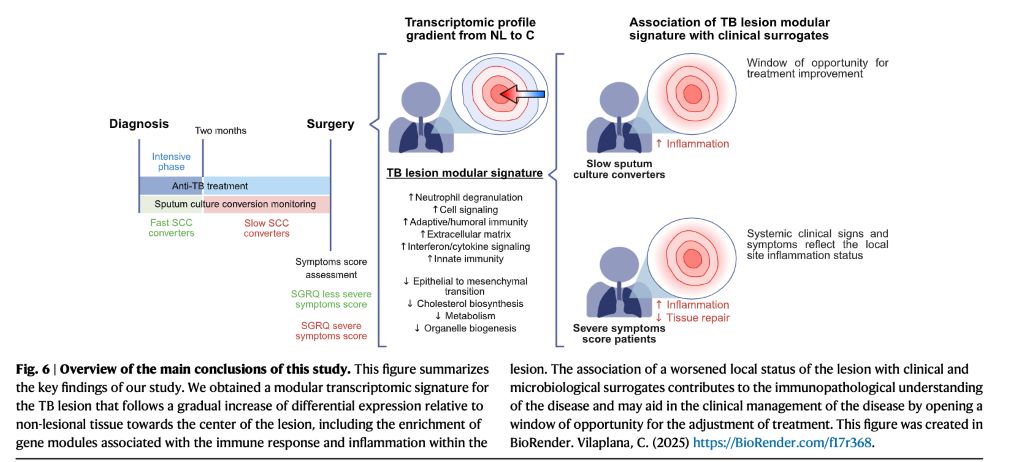
A study in Nature Communications reveals, for the first time, how the transcriptomic profile of human tuberculosis lung lesions is correlated with clinical data from the same patients. The work could potentially lead to improved prognosis by using personalised strategies.
Dr Cristina Vilaplana led researchers from the Experimental Tuberculosis Unit (UTE) at the Germans Trias i Pujol Research Institute (IGTP) and the Germans Trias i Pujol University Hospital.
The study applied RNAseq techniques to 44 fresh tissue samples from lesional and adjacent lung areas of patients with drug-sensitive and multidrug-resistant tuberculosis who underwent therapeutic surgery. The results show a clear separation between lesional and non-lesional tissue, with high expression of pro-inflammatory genes in the lesions.
Weighted gene co-expression network analysis (WGCNA) identified 17 differential transcriptomic modules and revealed a gradient of immune response elements depending on their location within the lesion.
Although lesion transcriptomics has been studied previously, this is the first work to associate these molecular profiles with clinical indicators from the same patients.
“Individuals with more severe forms of the disease present more inflamed lesions, while patients with better clinical outcomes show profiles compatible with tissue repair phases,” explains Dr Vilaplana.
The researchers used two clinical surrogates: a validated respiratory quality of life questionnaire (SGRQ) and sputum culture conversion.
“We confirmed that when a patient says they feel unwell, it is also reflected at the molecular level: their lesions show a stronger inflammatory response,” adds Vilaplana.
Furthermore, patients who take longer to achieve sputum culture conversion, a factor previously linked to worse prognosis, also show higher immune activation at the lesion site.
“These data open the door to personalised strategies: If after two months the patient hasn’t cleared the bacillus, we may need to adapt the treatment to modulate the inflammatory response and avoid a worse clinical outcome,” she concludes.
In the first peer-reviewed study to examine the potential risks and benefits of teen skin-care routines posted on social media, scientists at Northwestern Medicine found girls ages 7 to 18 are using an average of six different products on their faces, with some girls using more than a dozen products. These products tend to be marketed heavily to younger consumers and carry a high risk of skin irritation and allergy, the study found.
The findings are published in the journal Pediatrics.
Each teen daily skin-care regimen costs an average of $168 (which the authors estimate typically lasts a month depending on the size of the products), with some costing more than $500, the study found. As the summer nears, the study authors cautioned that only 26% of daytime skin care regimens included sunscreen – arguably the most important skin care product for any age range, but particularly for kids.
The top-viewed videos contained an average of 11 potentially irritating active ingredients, the study found, putting the content creators at risk of developing skin irritation, sun sensitivity and a skin allergy known as allergic contact dermatitis. Prior evidence has shown that developing such an allergy can limit the kinds of soaps, shampoos and cosmetics users can apply for the rest of their lives.
“That high risk of irritation came from both using multiple active ingredients at the same time, such as hydroxy acids, as well as applying the same active ingredient unknowingly over and over again when that active ingredient was found in three, four, five different products,” said corresponding author Dr. Molly Hales, a postdoctoral research fellow and board-certified dermatologist in the department of dermatology at Northwestern University Feinberg School of Medicine.
For example, in one video included in the study, the content creator applied 10 products on her face in six minutes.
“As she’s applying the products, she begins to express discomfort and burning, and in the final few minutes, she develops a visible skin reaction,” said senior author Dr. Tara Lagu, adjunct lecturer of medicine and medical social sciences at Feinberg and a former Northwestern Medicine hospitalist.
Videos ‘emphasized lighter, brighter skin’
“We saw that there was preferential, encoded racial language in some cases that really emphasized lighter, brighter skin,” Lagu said. “I think there also were real associations between use of these regimens and consumerism.”
These videos offer little to no benefit for the pediatric populations they’re targeting, the study authors concluded. What’s more, given how the algorithms work, it’s nearly impossible for parents or pediatricians to track exactly what children or adolescents are viewing. Lastly, there are dangers beyond skin damage, Hales said.
“It’s problematic to show girls devoting this much time and attention to their skin,” Hales said. “We’re setting a very high standard for these girls. The pursuit of health has become a kind of virtue in our society, but the ideal of ‘health’ is also very wrapped up in ideals of beauty, thinness and whiteness. The insidious thing about ‘skin care’ is that it claims to be about health.”
Studying teens in the TikTok environment
In the study, Hales and another researcher each created a new TikTok account, reporting themselves to be 13 years old. The “For You” tab was used to view relevant content until 100 unique videos were compiled. They collected demographics of content creators, number and types of products used and total cost of regimens and then created a list of products used and their active and inactive ingredients. The Pediatric Baseline Series used in patch testing was used to identify ingredients with elevated risk of inducing allergic contact dermatitis.
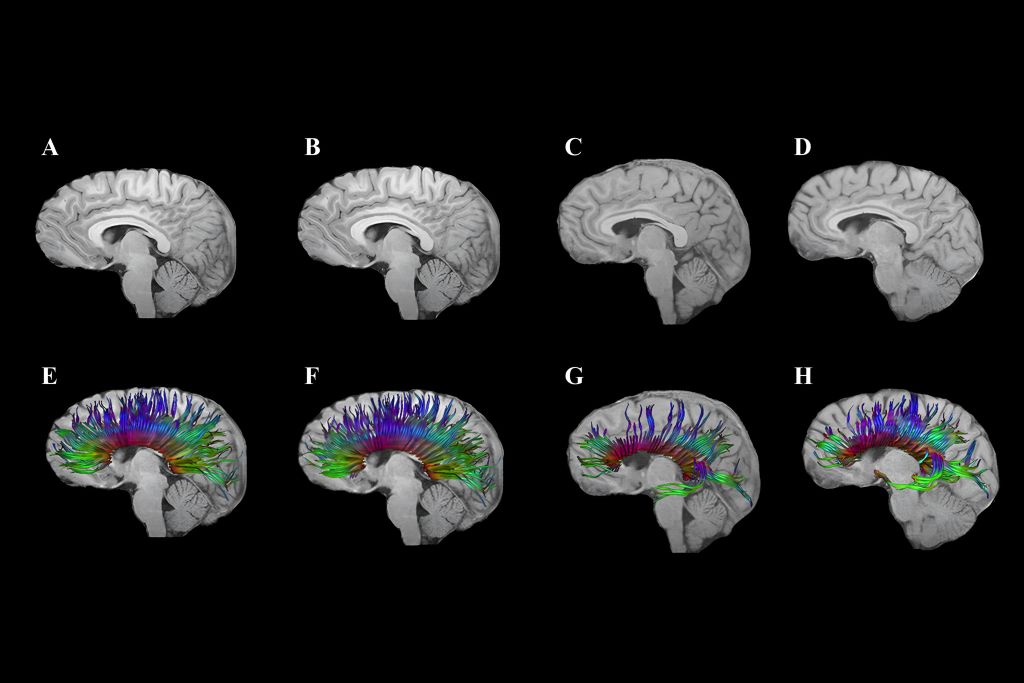
Diffusion tensor imaging shows corpus callosum fibre tracts in two adolescents: One with traumatic brain injury (TBI; G and H) and one with an orthopaedic injury (E and F). At 3 months post-injury (E, G), early degeneration and loss of fibre tracts are visible, especially in the TBI case. At 18 months (F, H), some recovery or reorganisation occurs, but persistent loss and thinning of tracts remain, particularly in the frontal regions, indicating lasting white matter damage after TBI.
By Kathy Malherbe
A silent but devastating brain disease is casting a shadow over contact and collision sports, particularly rugby. Traumatic Brain injuries (TBIs) as a result of an impact to the head, cause a disruption in the normal function of the brain. Repeated TBIs are linked to an increased risk of neurodegenerative diseases like early-onset dementia which has the highest prevalence and is the most concerning. Others include Parkinson’s disease, Alzheimer’s and Chronic Traumatic Encephalopathy, better known as CTE.
How head injuries happen
Dr Hofmeyr Viljoen, radiologist at SCP Radiology, says that there are several types of head injuries common in rugby. ‘The most frequent being TBIs which occur when the impact and sudden movement results in the brain shifting rotationally, sideways or backwards and forwards within the skull. This stretching and elongation causes damage to nerve fibres as well as blood vessels. Surprisingly, a direct blow isn’t always necessary. Rapid acceleration and deceleration, such as during a tackle or fall, can also result in an injury. More severe head injuries may include skull fractures, bruising or bleeding around the brain, all of which require urgent diagnosis and intervention.’
Riaan van Tonder, a sports physician with a special interest in sports-related concussion and radiology registrar at Stellenbosch University, explains that concussions and, even more so, repetitive sub-concussive impacts, result in a cascade of changes at a cellular level, gradually damaging the nervous system.
Although rugby is notorious for heavy tackles and collisions, it took a lawsuit to prompt more widespread awareness. A class-action suit filed in the High Court in London, by former union and league players, accused World Rugby of failing to implement adequate rules to assess, diagnose and manage concussions. Steve Thompson’s, the legendary English hookers, early onset dementia has been one of the sports’ biggest talking points. He was diagnosed in 2020 with this neurodegenerative disease, purportedly as a result of repeated trauma to the brain. The claimants argue that the governing bodies were negligent and that their neurological problems stem from years of unmanaged head injuries. The outcome of this case to be heard in 2025, could significantly reshape the legal and medical responsibilities of sports organisations globally.
What is Chronic Traumatic Encephalopathy (CTE)
CTE is a progressive neurodegenerative condition strongly linked to repeated head impacts. It has been implicated in memory loss, mood disturbances, psychosis and, in many cases, premature death. It can only be diagnosed after death at autopsy, where researchers examine brain tissue for abnormal protein deposits and signs of widespread degeneration. Despite this limitation, mounting evidence is forcing sports organisations, including rugby authorities, to confront uncomfortable truths about how repeated head trauma can alter lives permanently.
Uncovering the extent of the problem
In 2023, the Boston University CTE Centre released updated autopsy findings from its brain bank. Of 376 former NFL player’s brains studied post-mortem, 345 had been diagnosed with CTE, a staggering 91.7%. While brain banks are inherently subject to selection bias, the results remain alarming. For comparison, a 2018 study of 164 randomly selected brains revealed just one case of CTE.
This brain disease isn’t new. Its earliest descriptions date back to Dr Harrison Martland in 1928, who studied post-mortem findings in boxers and coined the term ‘punch drunk’ to describe their confusion, tremors and cognitive decline. What was once confined to boxing is now known to affect athletes in rugby, football, ice hockey and even military personnel exposed to repeated blast injuries.
Radiology’s role in determining head injuries
Although Computed Tomography (CT) scans are not designed to specifically diagnose concussions, they are crucial to imaging patients with severe concussion or atypical symptoms. ‘CT scans rapidly detect serious issues like fractures, brain swelling and bleeding, providing crucial information for urgent treatment decisions,’ explains Dr Viljoen.
‘Magnetic Resonance Imaging (MRI) is used particularly when concussion symptoms persist or worsen. It excels in identifying subtle injuries, such as microbleeds and brain swelling that may have been missed by CT scans,’ he says.
‘CTE is challenging because currently, it can only be definitively diagnosed after death,’ he explains. ‘However, ongoing research aims to develop methods to detect CTE in living patients, potentially using advanced imaging techniques like Positron Emission Tomography (PET).’ Most research is focused on advancing non-invasive methods to see what is happening inside the brain of a living person and to track it over time.
Advanced imaging methods
Emerging imaging techniques, such as Diffusion Tensor Imaging (DTI), show promise for better understanding and management of head injuries, especially the subtle effects of concussions. ‘DTI helps identify damage to the brain’s white matter, potentially guiding return-to-play decisions and treatment strategies,’ notes Dr Viljoen.
The biomechanics of brain trauma
Former NFL player and biomechanical engineer, David Camarillo, explains in a TED talk that helmets, although effective at preventing skull fractures, do little to stop biomechanical forces from affecting the brain inside the skull.
Camarillo highlights that concussions and the stretching of nerve fibres are more likely to affect the middle of the brain, the corpus callosum, the thick band that facilitates communication between the left and right brain hemispheres. ’It’s not just bruising,’ he says, ‘we’re talking about dying brain tissue.’
Smart mouthguard technology in rugby
‘Presently,’ says Van Tonder, ‘smart mouthguards are mandatory at elite level. These custom-fitted mouthguards contain accelerometers and gyroscopes that detect straight and rotational forces on the head. Data is transmitted live to medical teams at a rate of 1 000 samples per second.
‘If a threshold is exceeded, an alert is triggered, prompting an immediate Head Injury Assessment (HIA1). Crucially, the system can identify dangerous impacts, even when no symptoms or video evidence is apparent. This is an essential shift in concussion management,’ says van Tonder. ‘It allows proactive assessments rather than waiting for visible signs.’ World Rugby has committed €2 million to assist teams in adopting this technology and integrating it into HIA1.
Brain Health Service
The really good news is that in March this year, World Rugby and SA Rugby launched a new Brain Health Service to support former elite South African players. It’s the first of its kind in the world and South Africa is the fourth nation to establish this system that supports players to understand how they can optimise management of their long-term brain health. It includes an awareness and education component, an online questionnaire and tele-health delivered cognitive assessment with a trained brain health practitioner. This service assesses players for any brain health warning signs, provides a baseline result, advice on managing risk factors and signposts anyone in need of specialist care.
Super Rugby and smart mouthguards
Super Rugby has revised its smart mouthguard policy, no longer requiring players to leave the field immediately for a HIA when an alert is triggered. The change follows criticism from players and coaches, including Crusaders captain Scott Barrett, who argued the rule could unfairly affect match outcomes. Players must still wear the devices but on-field doctors will assess them first; full HIAs will be conducted at half-time or full-time, if necessary. Further trials are planned to improve the system before reinstating immediate alerts.
Where to from here?
Researchers continue to explore ways to reduce brain movement inside the skull during collisions. One innovative idea includes an airbag neck collar for cyclists, which inflates around the head upon impact. It’s closer to the goal of reducing the brain’s movement – and therefore the risk of concussion. However, regulatory hesitation remains a barrier, with no formal cycling helmet approval process currently in place.
The evidence linking repetitive head impacts to long-term brain degeneration is too compelling to ignore. Rugby, like other contact sports, must continue evolving its protocols, technology and player education to protect athletes at all levels … starting at schools.
While innovations such as smart mouthguards mark significant progress, much remains to be done: From regulatory reform to changing the sporting culture that once downplayed the severity of concussion. Van Tonder notes, ‘We’re behind, but it’s not too late to catch up.’
In rugby, the HIA protocol now consists of three stages:
HIA1: Immediate, sideline assessment during the match.
HIA2: Same-day evaluation within three hours post-match.
HIA3: A more detailed follow-up, typically done 36-48 hours later.
The Health Funders Association (HFA) has launched a legal challenge against the National Health Insurance (NHI) Act. The organisation filed its application on the 4th of June in the Pretoria High Court, challenging the Act on constitutional grounds. This marks the sixth legal challenge against the Bill, with others being brought by professional medical associations and other healthcare funding associations.
“South Africa needs a healthcare system that delivers equitable, quality care to all. We fully support that vision,” said Thoneshan Naidoo, the HFA’s chief executive. “However, in its current form, and without private sector collaboration, the NHI Act is fiscally impossible and operationally unworkable, and threatens the stability of the economy and health system, impacting everyone in South Africa.”
Prior to this, the Board of Health Funders had launched its own legal effort to have President Cyril Ramaphosa make public his decision-making process for approving the NHI Bill. So far, he has refused, arguing that opponents would lead to a courtroom “fishing expedition” in search of flawed reasoning.
HFA pointed to research that it had commissioned from economic consultancy Genesis Analytics. The Genesis report showed that unsustainable tax increases were necessary to fund NHI, while also reducing healthcare access for members of medical schemes.
NHI unaffordable even with generous assumptions
Assuming a cost efficiency of 45.5% from state-centralised healthcare funding, R15 432 per capita expenditure would be required, which works out to R941 billion for South Africa’s 61 million. (For comparison, the 2024 budget for US space agency NASA was R440 bn.) This is a 77% increase over SA’s total of R532.2bn for public and private healthcare expenditure in 2022, making healthcare 33% of the budget. Personal income tax rates would rise to over 40% for even the lowest income bracket – more than doubling from 18.5%. The highest income bracket would increase from 45% to 68.4%. Those earning R92 000 a year would have R10 000 less income – if they were already paying for medical aid. If not, that would be R21 000. [One wonders how South Africa can afford this when we cannot easily replace the US$500 million worth of US aid for HIV and other healthcare programmes under PEPFAR. – Ed.]
“Such tax increases are fiscally impossible, particularly given South Africa’s narrow personal income tax base of 7.4 million taxpayers,” the HFA said.
The HFA also argued that the NHI is not a reasonable solution to the constitutional requirement for progressive realisation of the right to healthcare. By making private healthcare only valid for conditions not covered by the NHI, its much-maligned Section 33 infringes on individuals’ healthcare access. Legislative authority is delegated to the Minister of Health, violating the constitutional separation of legislature and executive power. It is fertile ground for tenderpreneurs, as discussed by Jeff Wicks in a News24 article (paywalled). The HFA also notes that the government has admitted in legislation brought by Solidarity that no thorough NHI costing was performed.
Healthcare quality impacted
Even if South Africa were to find the money for NHI between the couch cushions, there have to be skilled people who can provide the services. Nearly 300 000 healthcare professionals would be required, and given the time needed to train new ones, there would be a huge strain.
Worse, analysis shows that the NHI will make things even worse than they currently are. According to Naidoo, “what NHI will do actually is worse than healthcare for the uninsured because combining your medical scheme population, who are older, within a single risk pool, will actually usurp more funds and actually disadvantage the vulnerable.”
But the country is not without options and inherent advantages, Naidoo says, citing the strengths of its private healthcare system. “We can bring to the table the skills, the knowledge and experience on how to build a sustainable funding solution for the entire country. So that’s what we can bring, and we want to make sure we build this country for everyone.”