In South Africa, where the burden of HIV remains high, women living with HIV face a disproportionately increased risk of cervical cancer, around six times higher than women without HIV. This heightened risk is driven by persistent infection with high‑risk strains of human papillomavirus (HPV). In settings where access to HPV vaccination, cervical screening and treatment is uneven, the impact on women’s health and lives is profound.
New research published in The Lancet Global Health provides the first population‑level evidence globally that a national HPV vaccination programme can be highly effective in a high HIV‑prevalence setting. The study was led by researchers from Wits RHI at the University of the Witwatersrand in partnership with the Kirby Institute (University of New South Wales).
The study evaluated South Africa’s free, school‑based national HPV vaccination programme, introduced in 2014, which offers HPV vaccination to girls in Grade 4 (aged nine years and older) attending public schools across the country. Crucially, the research assessed vaccine impact among adolescent girls and young women both living with HIV and without HIV, reflecting the realities of South Africa’s dual HIV and cervical cancer burden.
Until now, most evidence on HPV vaccine effectiveness in people living with HIV has come from studies where vaccination occurred after HIV infection, often after exposure to HPV and in the presence of immune suppression. This South African study, led by Professor Sinead Delany-Moretlwe at Wits RHI, Director of Research, is the first to demonstrate the real‑world impact of vaccination delivered early, before most girls are exposed to HPV, within a national public‑health programme in a high HIV‑burden context.
The findings show that the HPV vaccine provides excellent protection, including among girls living with HIV. Researchers observed substantial reductions in vaccine‑type HPV infections, demonstrating that high‑coverage HPV vaccination programmes can deliver strong population‑level benefits, even in settings with widespread HIV.
“For the first time, we can demonstrate at a population level that HPV vaccination delivered early, through a national public programme, provides excellent protection in a high HIV‑prevalence setting. This is a major public‑health success for South Africa and sends a clear message globally: investing in early, school‑based HPV vaccination can dramatically reduce future cervical cancer risk, including among girls living with HIV,” said Professor Sinead Delany-Moretlwe.
These results have major global implications. They reinforce the critical importance of early, school‑based HPV vaccination and provide compelling evidence for countries, particularly those with high HIV prevalence, to implement and sustain national HPV vaccination programmes. Such programmes have the potential to dramatically reduce cervical cancer risk, improve women’s health outcomes, and ultimately save lives worldwide.
From genetics to stress myths, researchers reveal what really drives greying and the breakthroughs pointing to natural colour restoration
Photo by Ravi Patel on Unsplash
Grey hair is more than a cosmetic concern – it drives a booming industry, influences how people are perceived, and can affect confidence. Globally, the hair colour market was valued at nearly USD 28 billion in 2025, with over half of purchases linked specifically to concealing greys. In South Africa, spending on hair colourants is projected to grow from roughly USD 172 million in 2021 to over USD 228 million by 2028, highlighting the demand for solutions that go beyond temporary cover-ups.
By age 50, roughly 50-70% of adults have visible grey hair, while premature greying can appear in some as early as the 20s. The psychological weight is clear: studies indicate grey hair can make people appear 20-30% older, influencing workplace perception, social interactions, and self-esteem. Studies show faces with grey hair are consistently perceived as more subdued than the same faces without greys, confirming that hair colour alone can shape social impressions.
“Many popular beliefs about greying hair are misleading,” says Dr Kashmal Kalan, Medical Director at Alvi Armani. “Stress does not turn hair grey overnight, plucking one strand won’t trigger several more, and no supplement or home remedy has been proven to restore pigment reliably. The reality is far more biological – genetics and pigment cell behaviour are the keys we are finally beginning to understand.”
At the heart of greying are melanocyte stem cells (McSCs) within hair follicles. In youth, these cells migrate and maintain melanin production, the pigment responsible for hair colour. With age, many become inactive or “trapped,” interrupting pigment delivery and causing grey strands. In mouse models, freeing these cells restored pigment production in roughly half of cases – a major step toward therapies that could reawaken natural colour without dyes.
Emerging research aims to tackle the root cause rather than just the appearance of grey hair. Scientists are exploring topical agents that target dormant pigment cells, metabolic modulators that influence follicle behaviour, and activation therapies designed to revive pigment production. These innovations could allow hair to regain its natural shade – not just cover it – while supporting overall follicle health.
“We are witnessing science that was once purely theoretical become reality,” says Dr Sunaina Paima, aesthetic and hair-restoration physician at Alvi Armani Johannesburg. “For patients, this could mean seeing grey strands regain their original shade naturally – a moment the hair science world has long dreamed of. The potential impact on confidence and self-esteem is enormous, because this isn’t just about covering colour, it’s about restoring it at a biological level.”
While most pigment-restoring therapies remain in development, advances in genetics, dermatology, and biotechnology are converging at unprecedented speed. “For decades, grey hair was seen as an irreversible hallmark of ageing,” adds Dr Kalan. “Today, that assumption is being seriously challenged. We’re on the brink of options that rejuvenate hair from the inside out, not just cosmetically.”
These breakthroughs signal a new era in hair science: ageing hair may no longer be inevitable or purely cosmetic, but a biological process that can be understood, guided, and ultimately restored.
A new open-access 3D portal that allows users to explore human organs in unprecedented detail, from the whole organ to individual cells, has been launched by an international team led by UCL scientists.
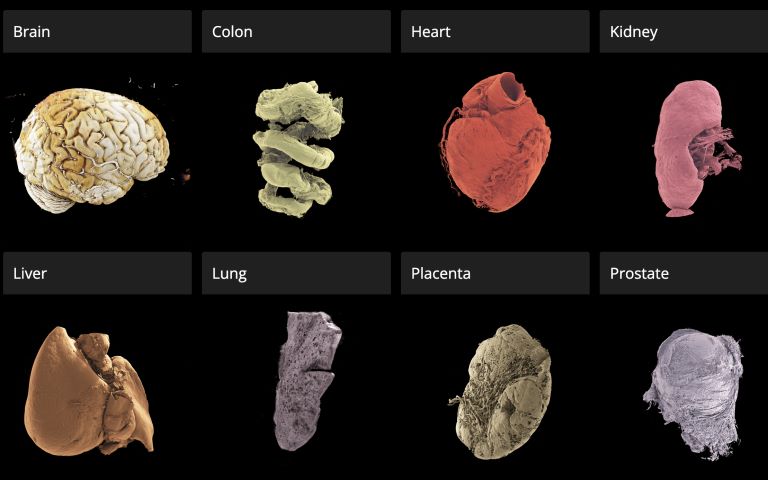
The Human Organ Atlas, described in a new paper in the journal Science Advances, brings together some of the most detailed images of 3D organs ever produced. It enables scientists, doctors, educators, students and the wider public to interactively “fly through” organs such as the brain, heart, lungs, kidney and liver, providing a new way of understanding human anatomy and human diseases.
The resource can be accessed directly through a standard web browser, without specialist software, at this link.
The Atlas is powered by an advanced X-ray imaging method called Hierarchical Phase-Contrast Tomography (HiP-CT), developed at the European Synchrotron (ESRF) in Grenoble, France. HiP-CT uses the ESRF’s Extremely Brilliant Source – a new generation of synchrotron source – which is up to 100 billion times brighter than conventional hospital CT scanners.
This allows researchers to scan entire intact ex vivo human organs (i.e., donated organs) non-destructively and then zoom in to near-cellular resolution (down to less than one micron, 50 times thinner than the size of a human hair).
The technique bridges a century-old gap in medicine between radiology and histology, and represents a major advance in biomedical imaging.
Professor Peter Lee (UCL Department of Mechanical Engineering), principal investigator of the Human Organ Atlas beamtime, said: “To create the Human Organ Atlas, we brought together scientists and medics from nine institutes worldwide. This grouping is continuing to expand, helping gain new insights into diseases from osteoarthritis to heart disease and changing how we learn about the human body.”
Dr Claire Walsh (UCL Department of Mechanical Engineering), Director of the Human Organ Atlas Hub, said: “The Human Organ Atlas shows what team science can achieve at its best – we went into this project wanting this data to be used by others and to help further the understanding of human physiology. The Human Organ Atlas is an incredible resource that will continue to grow. I am personally hugely excited to see how the AI community use the Human Organ Atlas in AI foundation models.”
From Covid-19 to cardiac and gynaecological disorders
Professor Judith Huirne, based at Amsterdam UMC, said: “The virtual 3D histological data derived from Human Organ Atlas hub provides us with valuable insights into the pathogenesis of gynecological disorders. This knowledge is crucial to bridging the current gaps in both understanding and gender disparities.”
This Human Organ Atlas portal is the result of more than five years of collaborative effort betweenmany researchers, engineers, clinicians, and infrastructure specialists, united within the Human Organ Atlas Hub, a consortium involving nine institutes across Europe and the United States.
Since its inception, the team has been committed to open science. Dr Paul Tafforeau, ESRF scientist and pioneer of the imaging technique used to create the Human Organ Atlas, said: “From the beginning, we wanted these data to be accessible to everyone and build an open, shared scientific infrastructure at a global scale. This is a resource for researchers, doctors, educators – but also for anyone curious about how the human body is built.
A unique tool for AI, medicine and education
To the team’s knowledge, this is the highest-resolution open 3D dataset of intact human organs currently available. The Human Organ Atlas currently provides access to: (to be updated)
62 organs, 319 full 3D datasets from 29 donors
12 organ types, including brain, heart, lung, kidney, liver, colon, eye, spleen, placenta, uterus, prostate and testis
Multiscale scans, from whole-organ views down to near-cellular resolution (routinely down to 2 µm, as fine as 0.65 microns for some organs)
The portal has been designed to extend far beyond specialist research laboratories. Each dataset can reach hundreds of gigabytes or even over a terabyte in size. The largest one (a brain) is 14 Tb. To make the data usable worldwide, the portal provides:
Interactive browser-based visualisation (no special software required)
Downloadable datasets at multiple resolutions
Tutorials and software tools for analysis
Regular addition of new data
Beyond advancing anatomical and biomedical research, the atlas is expected to become a major resource for artificial intelligence. Large, high-quality 3D datasets are rare – limiting the development of advanced medical AI systems. The Human Organ Atlas provides a curated, hierarchical dataset ideally suited for training machine-learning models for segmentation, disease detection and super-resolution analysis.
At the same time, it offers powerful new opportunities for medical education and public engagement with science, allowing anyone to explore the human body out of curiosity.
One in ten emergency patients with visible blood in their urine die within three months of presenting at A&E, new research has found. The WASHOUT study, presented Monday 16 March at the European Association of Urology Congress (EAU26) in London, found that a scan within 48 hours could reduce this risk.
Such a scan also ensured patients with cancer were diagnosed significantly faster. Around 1 in 4 people who presented at A&E with visible blood in their urine had an underlying cancer, with the most common being bladder cancer, the study found.
Around 25 000 people visit UK A&E departments each year because they have blood in their urine. Currently, patients receive different care depending on which hospital they visit or even which doctor they see. This is because there are no guidelines built on real-world evidence for doctors to follow. Based on global figures, only around half (53%) of patients receive a scan and a third (35%) receive surgery, with others discharged home or admitted to the ward to watch how their symptoms progress, says the WASHOUT study.
The WASHOUT study drew on global data to show that rapid action is critical for better patient outcomes. A CT scan or cystoscopy to look inside the bladder within 48 hours of arriving at A&E should determine the most appropriate next steps – such as whether the person should be treated for bladder cancer. Patients who didn’t receive investigative tests or appropriate treatment were 2.5% more likely to die within the next three months compared to those who did. They also spent more time in hospital and were more likely to be readmitted with the same problem within three months.
For patients with an underlying cancer, those who received investigative tests within the first 48 hours of admission were diagnosed within one day on average. In contrast, patients who were discharged without investigation faced a significantly longer wait, with diagnosis taking on average three weeks.
The research team is now taking steps to incorporate their findings into clinical guidelines, to help hospital staff provide the best treatment for these patients.
The study looked at data from more than 8500 people across 380 hospitals around the world and followed their journey for 90 days after arriving at A&E with blood in their urine. It also considered other factors that might have affected results, including age, frailty and other underlying conditions.
Nikita Bhatt, consultant urologist at St Vincent’s University Hospital, Dublin, led the research being presented at EAU26. She said: “This is the largest study exploring how we should treat people who present at A&E with blood in their urine. It’s a common problem affecting thousands of people around the world, and these patients are usually very unwell. But too often they fall through the gaps because it isn’t obviously tied to a specific disease. Our findings show how important it is that doctors take the necessary steps to identify the cause of the problem. For patients, the message is clear: if you have visible blood in your urine, don’t ignore it. See your doctor as soon as you can. If it doesn’t clear up, keep pushing until you find an answer. I hope our study gives patients the encouragement to do that.”
Jacqueline Emeks, a patient advocate on the WASHOUT study, who was diagnosed with a kidney infection and sepsis after arriving at A&E with visible blood in their urine, agrees: “These findings highlight that blood in the urine should trigger immediate action. It’s not something to watch and wait. For patients, this should mean quicker triage, earlier investigations and faster treatment, translating into safer care, fewer delays, and a better chance of avoiding severe illness or long-term harm. Patients know their bodies and deserve to be taken seriously. Blood in urine is a red flag until proven otherwise.”
Prof Dr Joost Boormans, a member of the EAU Scientific Congress Office and a urologist at the Erasmus University Medical Center, Rotterdam, said: “This is an important study highlighting the scale of the problem that emergency blood in the urine presents, both for patients and our already over-stretched healthcare systems. It’s difficult to draw strong conclusions about specific conditions because blood in the urine can be caused by many things, including cancer, and this group of patients is very diverse. But this study shows that timely investigative tests can accelerate diagnosis and reduce patients’ risk of readmission and long hospital stays, both being significantly high as shown in the WASHOUT study. As urologists in emergency care, we should be aware of these numbers and do more to get an immediate diagnosis for people with blood in urine, to reduce the burden on our healthcare systems and give our patients the best outcomes.”
Credit: Darryl Leja National Human Genome Research Institute National Institutes Of Health
Prostate cancer screening compares favourably to screening for breast cancer in identifying significant cancers, reducing mortality and avoiding unnecessary harms, according to new research. The findings are presented on Sunday 15 March 2026 at the European Association of Urology Congress (EAU26) in London. The research is also accepted for publication in European Urology.
The researchers maintain that the similarities between the two forms of screening mean it is no longer rational to reject prostate cancer screening on one hand while endorsing screening for breast cancer on the other. Nevertheless, they recommend some caution given their research compares a trial with a population-based screening programme and across two different cancers.
Although breast and prostate cancer are the most commonly diagnosed cancers in Europe amongst men and women respectively, screening for the diseases is vastly different. Organised breast cancer screening programmes have been established across Europe for more than three decades. Prostate cancer screening has lagged behind, primarily due to concerns around the effectiveness of the PSA blood test and the risks of overdiagnosis and overtreatment. Nevertheless, many men undergo variable, ‘opportunistic’ screening for the disease, mostly based on self-referral.
Several prostate cancer screening trials in Europe have now reported long-term outcomes, showing a reduced risk of death from prostate cancer [1]. This risk reduction is similar to that seen in breast screening programmes.
The new analysis compares the two types of cancer screening in terms of the effectiveness of the diagnostic tests and levels of overdiagnosis. The researchers, from the German Cancer Research Centre in Heidelberg, Germany, drew on data from the PROBASE prostate cancer screening trial in Germany and the country’s breast cancer screening programme.
They used data from 39,392 men who underwent an initial PSA blood test as part of the PROBASE trial at age 45 or 50. They compared this with data from just over 2.8 million women, aged 50–69, who had a mammography as part of Germany’s organised breast cancer screening programme. They found:
PSA blood testing followed by an MRI scan leads to a higher number of false positives than mammography (37-42% vs 10%).
A similar proportion of men and women were referred for biopsy (0.8-2.4% for men and 1.1% for women) as men in the PROBASE trial were triaged before referral using various factors to determine the likelihood of significant cancer (known as risk stratification)
Biopsies were far more likely to identify significant cancer in prostate screening than in breast screening (50-68% vs 10%), indicating that fewer men were referred for biopsy unnecessarily.
The percentages of invasive cancers identified were similar across both prostate and breast cancer screening (60-74% vs 73%).
Prostate cancer screening was more likely to identify non-aggressive cancers than breast cancer screening (26-31% vs. 22%). However, in prostate cancer the option of active surveillance is well-established, and the researchers maintain this would limit the risk of overtreatment. Active surveillance involves monitoring lower grade cancers and only starting treatment (radiotherapy or surgery) if they progress.
Dr Sigrid Carlsson, who leads Clinical Epidemiology of Early Cancer Detection at the German Cancer Research Centre (DKFZ) in Heidelberg, is lead author of the research. She said: “Until we have a population-based screening programme for prostate cancer, we can’t make an exact like-for-like comparison with breast cancer. But we can make some informed assumptions based on the data from our trial, which shows that if prostate cancer screening were extended to the wider population, then the outcomes are likely to be very similar to breast cancer. Although our study used German data, the findings are applicable to other countries. The final question we now need to answer is: what will this cost compared to what we are already paying for opportunistic screening? And that work is already underway.”
Tobias Nordström is a clinical urologist and Associate Professor at the Karolinska Institute, Sweden and a member of the EAU Scientific Congress Office. He said: “There is much that prostate cancer screening can learn from breast cancer screening and that is why this analysis is an important addition to our knowledge base. As these kinds of comparisons are very challenging, the results do need to be taken with a level of caution. That said, the clear overall similarities between the outcomes for breast and prostate cancer screening show that we are moving in the right direction, ensuring prostate cancer screening offers more benefits than harm.”
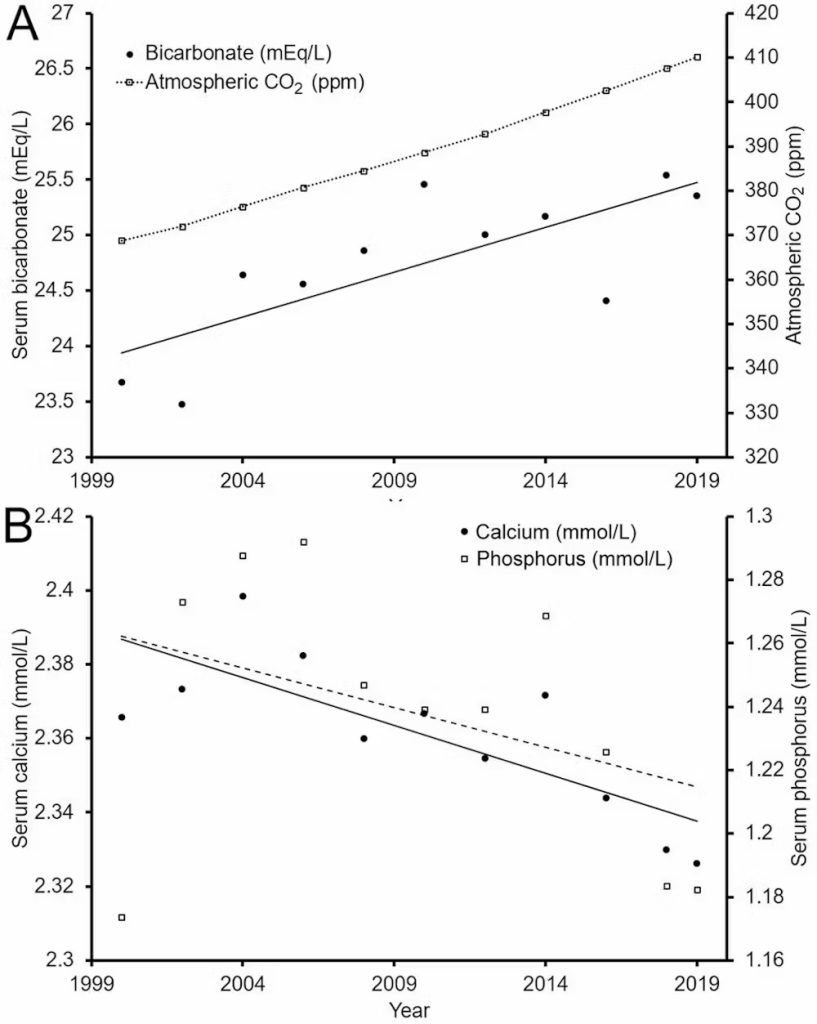
Humans evolved in an atmosphere containing roughly 200–300 parts per million (ppm) of carbon dioxide (CO₂). Today, that figure sits above 420 ppm, higher than at any point in the history of our species.
We know this extra CO₂ is contributing to climate change, but could it also be changing the chemistry of our bodies?
In our recently published research we looked at two decades of information from one of the biggest health datasets in the world to start answering this question. We found some concerning trends.
What we found
We analysed blood chemistry data from the US National Health and Nutrition Examination Survey (NHANES), which collected samples from about 7000 Americans every two years between 1999 and 2020. We looked at three markers: CO₂, calcium and phosphorus.
When CO₂ enters the blood, it is converted to bicarbonate. This process largely occurs inside red blood cells, and also produces hydrogen ions.
During short-term exposure to increased CO₂, this can make blood more acidic, and result in a modest increase in bicarbonate levels in the blood (to reduce acidity).
If the exposure continues for a long time the kidneys reduce the amount of bicarbonate lost in urine and also produce more bicarbonate. This has the net effect of higher bicarbonate levels in the blood, to counteract the persistent acidity.
Levels of calcium and phosphorus in the blood may also be affected, as they too play a role in regulating acidity in the blood. These processes are completely normal.
Over the 21 years from 1999 to 2020, we found that average blood bicarbonate levels rose by about 7%. Over the same period, atmospheric CO₂ concentrations rose by a similar proportion.
Meanwhile, blood calcium levels dropped by about 2% and phosphorus by around 7%.
If these trends continue, blood bicarbonate levels may exceed healthy levels in around 50 years. Calcium and phosphorus levels may fall below healthy levels, too, by the end of the century.
Our hypothesis is that rising CO₂ exposure could be contributing to these trends.
What’s causing the changes?
It’s important to be clear about what this study does and doesn’t show. It identifies population-level trends in blood chemistry that parallel rising atmospheric CO₂.
But correlation is not causation. The study does not adjust for factors such as diet, kidney function, diuretic use or obesity, which can influence the measurements and should be considered in future analyses.
There are other plausible contributors. One important consideration is indoor air.
Participants in the NHANES study likely spend most of their time indoors, where CO₂ concentrations often exceed 1000 ppm in poorly ventilated spaces. Other studies show time spent indoors has increased over the past two decades.
The NHANES dataset doesn’t capture this parameter, so we can’t directly assess this contribution. However, if more time indoors is contributing, it means total CO₂ exposure is rising even faster than atmospheric trends suggest. This arguably reinforces rather than alleviates the concern.
Other factors, such as shifting dietary patterns, changing rates of obesity, differences in physical activity and even variations in sample collection or processing across survey cycles, could also be important.
Can our bodies cope?
Some critics have argued that, based on what we know about how our bodies manage blood chemistry, we should have no trouble compensating for future increases in atmospheric CO₂, even under worst-case climate scenarios. For example, the lungs can increase ventilation and the kidneys can adjust to produce more bicarbonate.
For most healthy individuals, small long-term increases in outdoor CO₂ are not expected to meaningfully change the levels of bicarbonate, calcium or phosphorus in the blood.
This makes the population-level trends we observed puzzling. They could reflect a confounding rather than a direct CO₂ effect, but they do highlight how little data we have on long-term, real-world exposure.
A lack of long-term data
The argument that we can cope easily with higher CO₂ is based on short-term responses. Whether the same reasoning applies when CO₂ levels are higher across a person’s entire life remains largely untested.
There is, however, a growing body of evidence across many species which shows that even modest, environmentally relevant increases in CO₂ can produce subtle but measurable physiological effects.
In humans, short-term exposure at concentrations commonly found indoors (1000–2500 ppm) has been linked to reduced cognitive performance and changes in brain activity, though the mechanisms aren’t fully understood.
These new findings highlight a gap in evidence about long-term, real-world CO₂ exposure and human physiology. Unfortunately, there simply aren’t any studies assessing the physiological effects of breathing slightly elevated CO₂ over a lifetime.
This is particularly important for children, who will experience the longest cumulative exposure. And that’s why it’s vital to investigate this area further.
What this means
Our findings are not suggesting people will become suddenly unwell when atmospheric CO₂ reaches a certain level. What the data show is a signal that warrants attention.
If rising atmospheric CO₂ is contributing to gradual shifts in blood chemistry at a population level, then the composition of the atmosphere should be monitored alongside traditional climate indicators as a potential factor in long-term public health.
Reducing CO₂ emissions remains crucial for limiting global warming. Our findings suggest it may also be important for safeguarding aspects of human health that we’re only just beginning to understand.
A University of Pretoria study has revealed troubling ethical and procedural gaps in the way medical schemes conduct forensic audits of physiotherapists, showing how practices intended to prevent billing irregularities are often leaving practitioners fearful, stigmatised and traumatised without proving guilt.
Audits of healthcare professionals are designed to detect billing irregularities and protect medical scheme funds. However, research conducted by Lesley Meyer, an extra-ordinary lecturer at University of Pretoria’s Department of Physiotherapy, explored the lived experiences of physiotherapists who have undergone such audits, and found that the audit practices conducted were experienced as punitive and harmful to practitioners rather than corrective.
Forensic audits in the healthcare sector are, in principle, supposed to protect medical scheme funds and by extension, patients’ contributions. In practice, however, Meyer’s research study, published in the latest edition of The South African Journal of Physiotherapy, found that these audits often extend beyond their legal scope and adversely affect the profession, while pocketing patient’s savings instead of returning these funds to the patients in accordance with the Medical Schemes Act.
Under Section 59(3) of the Medical Schemes Act of 1998, schemes may investigate inconsistencies in claims, but when alleged fraud, waste or abuse exceeds R100 000, the matter should be referred to the Health Professions Council of South Africa (HPCSA) or the South African Police Service. However, the study found that schemes mistrust these authorities, so they bypass that requirement by reclassifying potential fraud as administrative billing errors. This practice allows them to conduct internal investigations without external oversight, creating a loophole that has opened the door to misuse, coercive practices and a lack of accountability.“
Participants reported feeling unfairly targeted and singled out, describing the audit process as unfairly conducted. Many felt they were subjected to a witch hunt,” Meyer says, who is also a physiotherapist and runs a private outpatient practice with a special interest in chronic pain and trauma management. Participants described being treated as suspects rather than professionals and reported severe distress caused by a process that offers no transparency or recourse.
The study found that the problem is exacerbated by South Africa’s outdated billing system. The gazetted tariff codes, last updated by the Competition Commission in 2006, have remained unchanged. Due to the fact that medical aid schemes don’t accept new, unlisted codes, practitioners are forced to use outdated tariffs to describe modern, evidence-based treatments. In some instances, practitioners leave those treatments unbilled altogether.
The study found that practitioners were sometimes accused of overbilling or coding errors without being given access to the evidence used against them. Some described being pressured to sign an Admission of Debt (AOD) to avoid escalation, leading to payments that varied from R54 000 in a solo practice to R4,5 million for one group practice.
As reported in the study, the investigators’ tactics were perceived as coercive and participants were forced to either sign AODs or face continued blockages on payments, effectively turning them into cash practices. Physiotherapists operating as cash-based practices were blacklisted because scheme administrators could not use offset controls to manage claims.
Meyer explains: “For those who sign the AOD it means they’re admitting that they’re guilty, which is against the Health Professions Act, because if you are guilty, it means you’ve committed fraud, and you can lose your licence. But participants felt like they didn’t have a choice, because they weren’t getting any money from the schemes.”
The impact on clinical care
One of the key problems highlighted in the research is the lack of external oversight over medical schemes’ auditing procedures. While the Health Professions Council of South Africa regulates practitioner conduct, schemes are governed by the Council for Medical Schemes (CMS), however, a physiotherapist who participated in the study, who complained to the CMS received no response. This gap leaves practitioners vulnerable to arbitrary decisions and offers no appeal mechanism when they believe they have been treated unfairly.
Meyer says the distress caused by the audits has clear hallmarks of trauma with participants describing the trauma they experience being akin to post-traumatic stress disorder, triggering physical reactions such as going into a cold sweat when encountering reminders of the medical fund and enduring stigma from being blacklisted.
One participant said: “Seven months of watching my father die was easier than this experience.
”Meyer’s research shows that these experiences aren’t isolated incidents but systemic. Interviews revealed a pattern of practitioners who felt coerced into compliance due to their fear of professional ruin.
The study revealed that physiotherapists perceived the audit process as vindictive rather than beneficial. The physiotherapists also felt that the forensic investigators perceived them as being guilty from the start, without considering alternative reasons for irregular billing patterns.
These hostile auditing processes contradict the principle of procedural fairness, Meyer says, which requires fair treatment, transparency, impartiality and an opportunity to be heard.The way forwardThe study recommends teaching undergraduate and registered physiotherapists about forensic literacy. Therefore, Meyer created five lectures based on her findings’ which have been implemented with the fourth-year physiotherapy students as part of the IHL module at the University of Pretoria, to empower students and increase their resilience when faced with forensic audits in private practice.
Moreover, the study recommends a framework that allows practitioners to be heard and protected while ensuring that accountability remains central. Such a framework includes establishing an independent oversight body, standardising investigative procedures and ensuring audited practitioners can access evidence, respond to allegations and appeal decisions. Meyer will continue with this framework through a PhD.
A significant development since Meyer’s study was completed, is the release of the final report by an independent legal panel that reviewed how Section 59(3) of the Medical Schemes Act is applied in forensic audits of healthcare professionals. Meyer says the report confirmed many of the issues raised in her research, including retrospective audits, a lack of transparency and potential misuse of power by medical schemes.“
The release of this report is an important step toward institutional accountability and reform,” Meyer says. “However, the full implementation of its recommendations remains critical to ensure fair audit practices and to restore trust among healthcare providers.”
“The people I interviewed were not trying to avoid accountability. They wanted fairness. They wanted to be heard. If we don’t address the lack of oversight, we risk losing good practitioners and damaging trust in the healthcare system itself.”
Elevated Lipoprotein(a) [Lp(a)] is an independent, genetically determined risk factor for atherosclerotic cardiovascular disease (ASCVD), with levels >50mg/dL affecting 20–30% of the global population. Despite therapeutic limitations, interest in Lp(a) has increased, driven by its prognostic value and the emergence of targeted therapies. However, with increasing guideline-directed Lp(a) testing, clinician response to elevated concentrations, especially in the absence of guideline-based treatment indications, remains unclear.
In a new study and presentation at the American College of Cardiology, researchers found that elevated Lp(a) was associated with earlier and more frequent initiation of preventive pharmacotherapy. These response rates were modest in a low-risk, primary prevention study population.
Specifically, nearly 80% of patients with elevated Lp(a) > 50mg/dL did not initiate lipid-lowering therapy in the absence of other ASCVD risk factors. Drugs that drastically lower “bad” LDL cholesterol (PCSK9 inhibitors) and aspirin initiation was even less common, suggesting selective rather than systematic responses to elevated Lp(a). Together, these findings suggest that elevated Lp(a) appears to only occasionally influence prescribing behaviour – behaviour consistent with previous reports.
“While not currently a standard indication for statin therapy alone, elevated Lp(a) is increasingly used by clinicians as a “risk enhancer” to guide more aggressive, albeit often unstandardised, preventive measures,” says corresponding author Sheilah A. Bernard MD, associate professor of medicine at Boston University Chobanian & Avedisian School of Medicine.
The researchers conducted a multicentre retrospective observational cohort study evaluating initiation of preventive pharmacotherapy following Lp(a) measurement among nearly 15 000 patients at low risk for ASCVD. Within 90 days of Lp(a) measurement, lipid-lowering therapy initiation was uncommon but more frequent among patients with elevated Lp(a) compared to those with non-elevated Lp(a). PCSK9 inhibitor initiation was rare but more frequent among patients with elevated Lp(a). Similarly, aspirin initiation was uncommon but more frequent among patients with elevated Lp(a).
According to the researchers, these findings should not be interpreted as indicating that such prescribing is guideline-directed. “Current recommendations recognise Lp(a) as a risk-enhancing factor rather than as a treatment target, and no therapy is approved solely for Lp(a) elevation. Our analysis describes contemporary practice rather than appropriate management,” adds Bernard who also is a cardiologist at Boston Medical Center.
The first major update to resistance-training guidelines in 17 years delivers one clear message: any amount of resistance training improves strength, muscle size, power and physical function.
The new recommendations, published by the American College of Sports Medicine (ACSM) as a Position Stand, are based on 137 systematic reviews involving more than 30 000 participants, making them the most comprehensive resistance-training guidelines to date.
“The best resistance training programme is the one you’ll actually stick with,” says Stuart Phillips, distinguished professor in the Department of Kinesiology and an author on the Position Stand. “Training all major muscle groups at least twice a week matters far more than chasing the idea of a ‘perfect’ or complex training plan. Whether it’s barbells, bands, or bodyweight, consistency and effort drive results.”
This update has been a long time coming. ACSM last published a Position Stand on resistance training for healthy adults in 2009, predating the explosion of research on muscle health, aging and the role of strength in long-term wellbeing.
“The new document reflects that surge in evidence and expands its recommendations to include more people and more types of training than ever before,” Phillips says.
A central theme of the new Position Stand is that the most meaningful gains come from a simple shift: moving from no resistance training to any form of it. While training variables such as load, volume, or frequency can be fine-tuned, the primary goal for most adults should be to build a consistent routine.
One of the greatest changes is the recognition that meaningful results don’t require a gym. Elastic bands, bodyweight training and home-based routines offer clear and measurable improvements in strength, muscle size and functional performance.
Rigid rules and prescriptive ideal programs are no longer supported by evidence, explains Phillips. Instead, personal goals, enjoyment, and long-term adherence matter most, especially for adults looking to stay strong, healthy and functional as they age.
Athletes and highly trained individuals will still require more specialized, sport-specific programs, but for the average adult, the message is simple: find a resistance-training routine you enjoy and stick with it.
Countries like South Africa benefited in very concrete ways from multilateral forums. Photo by Kindel Media
By Marcus Low
Funding cuts over the last year or so have created a crisis for multilateral health institutions. Which institutions emerge from this crisis, and in what form, will have real consequences for the health of people in South Africa, argues Spotlight editor Marcus Low.
In recent weeks, there has been a glut of articles from global health big-hitters, all concerned with how multilateral health institutions should, or should not be re-designed. These include articles from Philippe Duneton, Executive Director of UNITAID, Sania Nishtar, CEO of GAVI, and one co-authored by, among others, Anders Nordström, a former acting Director-General of the WHO, Helen Clark, a former New Zealand Prime Minister, and Peter Piot, the driving force behind UNAIDS from the mid-90s to 2008.
The immediate cause of all this debate is the stark reality that funding for multilateral health institutions have been cut dramatically in the last year, mainly, but not exclusively, due to the United States’ retreat from such international forums in favour of bilateral agreements. Even before the funding cuts, the financial outlook at entities like the World Health Organization (WHO) and UNAIDS was bleak. Over the last year, it has tipped over into outright crisis.
The WHO has already undertaken drastic organisational restructuring. Last year, a UN document raised the possibility of “sunsetting” UNAIDS by the end of 2026. It is likely that we will see several more organisations shrinking or disappearing altogether in the coming years.
Why does this matter?
The multilateral health institutions we’ve had in recent decades have not been perfect. They were often overly politicised, fraught with power imbalances, and not always capable of responding quickly and effectively to health emergencies.
But even so, it is unequivocally true that when it comes to healthcare, multilateralism has yielded many tangible benefits that are helping keep people alive. In a world where every country stands alone, these benefits will simply fall away.
There are many examples of such benefits. The WHO’s treatment guidelines for diseases like HIV and TB are public goods that are invaluable in many countries – here in South Africa they were particularly important as an antidote to the crackpot science that flourished in the period of state-sponsored AIDS denialism. The sharing of genomics data between countries was critically important at the height of the COVID-19 pandemic. Over an even longer period, the sharing of data on influenza strains has enabled the rational selection of vaccine components for each hemisphere each year. Medicines regulators in different countries increasingly share some of their work in order to speed their processes up and avoid duplication.
This year, a new HIV prevention injection containing the antiretroviral lenacapavir is being rolled out in South Africa and several other countries, largely with the help of the Global Fund, another international entity. A stable supply of low-cost lenacapavir should be available in around a year or two from now, due to market-shaping work done by UNITAID, the Gates Foundation, the Clinton Health Access Initiative, and Wits RHI. Such market-shaping often involves committing ahead of time to purchase certain volumes of a product to incentivise manufacturers to invest in production capacity, thus kick-starting the market for the product.
Then there is the recent history of how rapidly a new antiretroviral medicine called dolutegravir was rolled out in South Africa from 2019 – today over five million people here are taking it. The Geneva-based Medicines Patent Pool (MPP) negotiated licenses that allowed generic competition to start years earlier than would otherwise have been the case. That enabled the low prices and supply security that has facilitated the massive uptake of dolutegravir here and in dozens of other countries.
It is clearly in South Africa’s interest to help keep mechanisms like the above going.
But to reduce the value of these institutions to purely the technical would miss the essence of what animates them in the first place. The reality is that multilateral health institutions have often been at their most effective when people were driven by the need to address urgent health needs, as for example in the early days of UNAIDS. The belief that people’s health matter, no matter who they are, or where they live – essentially a belief in human rights – can make the difference between an ineffectual bureaucracy and a vital health movement. Our current crisis is not only one of technical capacity, but also one where the animating power of human rights-based thinking is being challenged.
How then should we think about redesigning global health?
There are some tensions between fighting to keep what we currently have and embracing big reforms. For example, on the one hand, given the aid cuts of the last year, people have good reason to be concerned about the potential closure of UNAIDS being a precursor to the further unravelling of the global HIV response. On the other hand, there are legitimate questions as to whether UNAIDS is still fit for purpose, given how the HIV epidemic has changed over the last three decades.
One of the most useful contributions in how to think about all this comes from Nordström and his co-authors. They outline four key paradigm shifts that help bring the current moment into focus. Their paper is worth reading in full for the nuances, but here is a brief paraphrasing of the four paradigm shifts:
The first shift is about recognising the fundamental changes underway in the global burden of disease and in demography. In short, while the key threats in the last three decades were the infectious diseases malaria, tuberculosis, and HIV, they are increasingly being overtaken by non-communicable diseases (like diabetes and hypertension) and mental health disorders. This shift is not yet reflected in the architecture of multilateral health institutions.
The second shift relates to the recentring of power from Geneva in Switzerland and New York and Washington in the USA to countries and regions, giving rise to an increasingly multipolar world. “This shift does not imply that multilateral cooperation is obsolete,” write the authors, “however, it requires a clarification of which future functions should be performed at the global level, and which should be performed by national and regional bodies.”
The third shift refers to the growing push to modernise the landscape of global health institutions. The authors write: “Leaders from low-income and middle-income countries have repeatedly critiqued the dearth of systemic support, the inefficiencies of vertical initiatives, and the resource-intensive bureaucratic processes that accompany them”. Considering these external and internal pressures, they argue there is a need to move from a complex and competitive system to a simpler, needs-based, and agile system.
The fourth shift is linked to the declining relative importance of development assistance, coupled with countries’ rising commitments to increase domestic financing for health. Although some international support will remain essential for low-income countries and humanitarian responses, the authors argue that domestic resources must be the engine of a new ecosystem and ways of working together.
All of these shifts are now occurring within the broader geopolitical context of what Canadian Prime Minister Mark Carney recently described as a “rupture in the world order”. He stressed that the great powers have turned their backs on the rules-based world order and have “begun using economic integration as weapons, tariffs as leverage, financial infrastructure as coercion, supply chains as vulnerabilities to be exploited”. This shift can already be seen in the US’s pivot from multilateralism to bilateral health agreements.
As Carney put it: “The multilateral institutions on which the middle powers have relied – the WTO, the UN, the COP – the architecture, the very architecture of collective problem solving are under threat.”
He argues that middle-powers like Canada, and I’d argue South Africa should aspire to be part of this group, should chart a way forward where they are not overly reliant on super powers like the US and China. Avoiding such an over-reliance is of course also an obvious lesson to take from the US’s abrupt cuts to health aid last year.
Maybe a first harsh reality to come to terms with then is that the rupture that is taking place in global geopolitics is also occurring in the world of global health. To think that we can go back to the way the WHO or UNAIDS were twenty years ago, is wishful thinking. The “rupture” might take time to propagate, but it will extend all the way.
What then is to be done?
Carney also makes the point that the rules-based order wasn’t in fact working as well for everyone as we liked to pretend. To a lesser extent, something similar could be said for multilateralism in health. Getting things done was often hard, the politics was often tricky, and when it came to the crunch, say on something like patents on medicines, the US and Europe almost always held sway.
As outlined above, countries like South Africa benefited in very concrete ways from multilateral forums, but somehow those benefits were never widely appreciated. Ultimately, it is telling that so many national governments have failed to put up the money the WHO requires to do its work – even before the current US withdrawal.
Maybe then, to make a reset of multilateral health institutions a success, will require that governments reassess and newly appreciate why it is that we need multilateral health institutions in the first place.
This will require a thorough and honest assessment of what we have gained from these institutions in recent decades. Things like market-shaping, patent pooling, pooled procurement, sharing of genomics and other data, regulatory harmonisation, guideline development, research cooperation, and multilateral fund raising have all been important and will continue to be so. We must make sure that in whatever emerges in the next few years, we have multilateral mechanisms that can deliver in all these areas.
But we will have to accept that those entities might look quite different from what we’ve come to know in recent decades. There will certainly be areas in which we still need global institutions like the WHO, but for some issues we might get more done by working with coalitions of the willing, or collaborating at a regional level – as we’re already seeing with the African Medicines Agency (although South Africa rather inexplicably hasn’t yet ratified the related treaty).
The reality is that apart from governments just not being willing to spend more on health at the moment, the enabling geopolitical substructure that we’ve been relying on for decades has given way. In many respects, this has been a disaster for our common good, but it is also an opportunity to craft new and more fit-for-purpose multilateral health institutions that are animated by a shared commitment to human rights. This is an opportunity that countries like South Africa must grasp.
As Carney put it: “We know the old order is not coming back. We shouldn’t mourn it. Nostalgia is not a strategy, but we believe that from the fracture, we can build something bigger, better, stronger, more just. This is the task of the middle powers, the countries that have the most to lose from a world of fortresses and most to gain from genuine cooperation.”
*Low is the editor of Spotlight.
This article was jointly published with Health Policy Watch, a global health news platform.
Disclosure: The Gates Foundation is mentioned in this article. Spotlight receives funding from the Gates Foundation, but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council.