In a study published in Arthritis & Rheumatology, people with hand osteoarthritis, higher body mass index was associated with greater pain severity in the hands, feet, knees, and hips.
Osteoarthritis is one of the most debilitating joint disorders worldwide, affecting up to 10% of men and 13% of women. Osteoarthritis is characterised by a progressive onset of joint damage, commonly associated with pain. Joints commonly affected include the knee, hip and hand. Various stressors, risk factors and genetics may predispose an individual to developing osteoarthritis in a particular joint.
In a study of 281 patients, researchers noted that observed associations of body mass index with hand pain and total body joint pain seemed to involve certain inflammatory markers (leptin and high-sensitivity C-reactive protein, respectively).
The researchers suggest that systemic effects of obesity, measured by leptin, could have a larger mediating role for pain in hands than in lower extremities. Low-grade inflammation, measured by hs-CRP, may contribute to generalised pain in overweight or obese individuals.
“Our results highlight the complexity of pain in hand osteoarthritis. Obesity is not only leading to pain through increased loading of joints in the lower extremities, but seems to have systemic effects leading to pain in the hands and overall body,” said lead author Marthe Gløersen, MD, of Diakonhjemmet Hospital, in Norway.
By sequencing genes linked to cardiac arrhythmia risk in more than 20 000 people without an indication for genetic testing, scientists were able to identify possible pathogenic variants in 0.6% of individuals, according to a study published in Circulation.
This rate is higher than those previously reported, according to Carlos G. Vanoye, PhD, research associate professor of Pharmacology and a co-author of the study.
“This study suggests the prevalence of genetic susceptibility to cardiac arrhythmia may be underestimated,” Dr Vanoye said.
The American College of Genetics and Genomics (ACMG) currently recommends that incidentally discovered pathogenic or likely pathogenic variants in 73 Mendelian disease genes be reported back to patients. This includes many genetic variants associated with congenital cardiac arrhythmias, causing irregular heartbeats which can lead to stroke or sudden cardiac death.
However, the pathogenicity of many genetic variants in these known arrhythmia genes is uncertain, and classification of these variants is still in the early stages.
“A person can carry a disease-causing gene variant but exhibit no obvious signs or symptoms of the disease,” Dr Vanoye said. “Because the genes we studied are associated with sudden death, which may have no warning signs, discovery of a potentially life-threatening arrhythmia gene variant can prompt additional clinical work-up to determine risks and guide preventive therapies.”
The current study used data from the Electronic Medical Records and Genomics sequencing (eMERGEIII) study. The eMERGEIII study investigated the feasibility of population genomic screening by sequencing 109 genes implicated across the spectrum of Mendelian (single inherited gene mutation) diseases in over 20 000 individuals, returning variant results to the participants, and using Electronic Health Record (EHR) and follow-up clinical data to ascertain patient phenotypes.
In the current study, investigators analysed 10 arrhythmia-associated genes in individuals without an indication for genetic testing.
The researchers determined the functional consequences of these variants of uncertain significance and used the data to refine the assessment of pathogenicity. In the end, they reclassified 11 of these variants: three that were likely benign and eight that were likely pathogenic.
In all, 0.6% of the studied population had a variant that increases risk for potentially life-threatening arrhythmia and there was overrepresentation of arrhythmia phenotypes among these patients. This is a rate higher than previously known for genetic arrhythmia syndromes (approximately 1 in 2000) and illustrates the potential for population genomic screening, Dr Vanoye said.
“Population genomic screening can positively affect public health. Many rare, disease-associated variants can be found this way which can then help determine the disease-risk of the carriers of these variants,” Dr Vanoye said. “Although the costs of genomic screening may be currently high, assessing patient risk followed up by clinical care would reduce the financial and emotional cost of the disease.”
Almost a third of older adults infected with COVID in 2020 developed at least one new condition requiring medical attention in the months after initial infection, compared to only a fifth who were not infected, according to a study published by The BMJ.
Conditions involved a range of major organs and systems, including the heart, kidneys, lungs and liver as well as mental health complications. Some studies now examine the frequency and severity of sequelae after COVID infection, but few have described the excess risk of new conditions triggered by COVID infection in adults 65 and older.
Researchers used US health insurance records to identify 133 366 individuals aged 65 or older in 2020 who were diagnosed with COVID before 1 April 2020. Three (non-COVID) comparison groups were matched: from 2020, 2019, and a group diagnosed with viral lower respiratory tract illness.
The researchers then recorded any persistent or new conditions starting 21 days after a COVID diagnosis (the post-acute period) and calculated the excess risk for conditions triggered by COVID over several months based on age, race, sex, and whether patients were hospitalised with COVID.
The results show that among individuals diagnosed with COVID9 in 2020, 32% sought medical attention in the post-acute period for one or more new or persistent conditions, which was 11% higher than the 2020 comparison group.
Compared with the 2020 comparison group, COVID patients were at increased risk of developing a range of conditions including respiratory failure (an extra 7.55 per 100 people), fatigue (+5.66 per 100), high blood pressure (+4.43 per 100), and mental health diagnoses (+2.5 per 100). Similar findings were found for the 2019 comparison group.
However, compared with the group with viral lower respiratory tract illness, only respiratory failure, dementia, and fatigue showed increased risk differences of 2.39, 0.71, and 0.18 per 100 people with COVID, respectively.
Individuals hospitalised with COVID had a markedly increased risk for nearly all conditions. The risk of several conditions was also increased for men, for those of black race, and for those aged 75 and older.
Limitations include being an observational study – however, the authors warn that the number survivors with sequelae will continue to grow.
“These findings further highlight the wide range of important sequelae after acute infection with the SARS-CoV-2 virus,” they write. “Understanding the magnitude of risk for the most important clinical sequelae might enhance their diagnosis and the management of individuals with sequelae after acute SARS-CoV-2 infection.”
“Also, our results can help providers and other key stakeholders anticipate the scale of future health complications and improve planning for the use of healthcare resources,” they conclude.
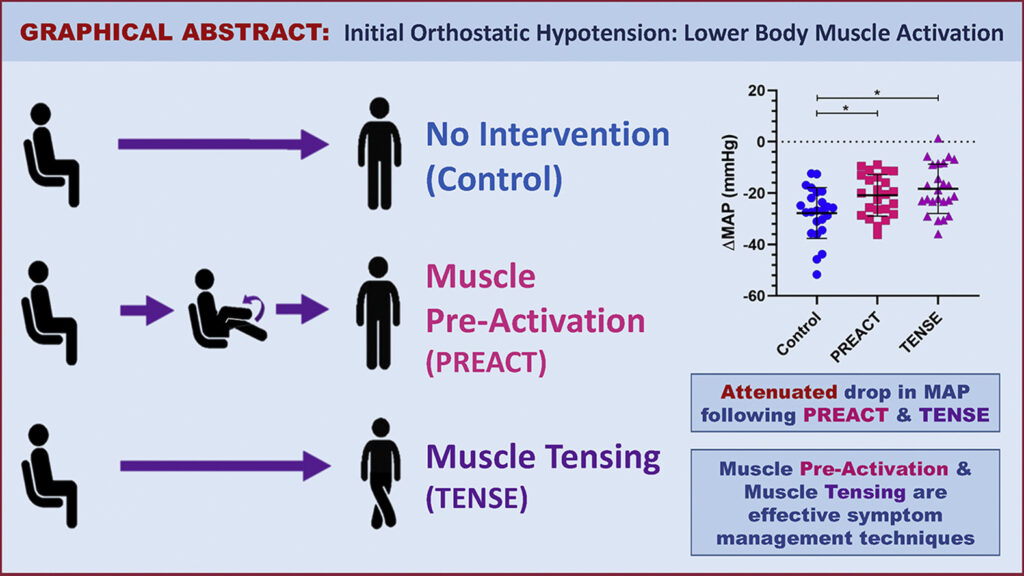
Light-headedness upon standing up due to initial orthostatic hypotension (IOH) is a common but poorly understood condition. A new study offers two simple techniques to effectively manage symptoms of IOH and improve quality of life by activating lower body muscle before or after standing. The research appears in Heart Rhythm.
IOH is a transient decrease in blood pressure and increase in heart rate. Syncope, light-headedness, dizziness, or loss of consciousness from IOH, affects up to 40% of the general population (all ages), while presyncope is probably even more common. However, the condition is under-studied and there are very few options currently available to patients with IOH and no pharmacological treatments. The most common recommendations have been to stand up slowly or sit up first before standing.
IOH symptoms often present during an active stand but not with a passive tilt-table test, suggesting that a muscle activation response plays an important role in the pathophysiology of IOH. This muscle activation response refers to the rapid and excessive vasodilation that occurs in response to the brief lower body muscle contraction required to stand due to local mechanisms. Additional factors involved in this response include the increase in heart rate, initially due to the muscle heart reflex and secondarily in response to the arterial baroreflex triggered by the drop in BP as well as the increase in peripheral resistance, which is also triggered by the arterial baroreflex.
This study investigated physical manoeuvres before or after standing and their efficacy in reducing the drop in blood pressure as well as the symptoms typically seen in IOH patients upon standing. Study participants included 24 young women with a history of IOH. Two participants had inadequate heart rate recordings and were excluded from the analysis. The interventions tested consisted of lower body muscle pre-activation (thighs) through repeated knee raises prior to standing (PREACT) and lower body muscle tensing (thighs and buttocks) through leg crossing and tensing immediately after standing (TENSE).
The 22 study participants completed three sit-to-stand manoeuvres including a stand with no intervention (control), and two interventions. Researchers found that both PREACT and TENSE effectively improve the blood pressure drop. This led to a reduction in symptoms upon standing. They found that the PREACT manoeuvre accomplished this by increasing cardiac output, while the TENSE manoeuvre did so by increasing stroke volume.
“Our study provides a novel and cost-free symptom management technique that patients with IOH can use to manage their symptoms,” noted first author Nasia A. Sheikh, MSc. “Since it is a physical manoeuvre, it simply requires the lower body limbs, which patients can utilise at any time and from anywhere to combat their symptoms.”
A clot within a blood vessel interrupting blood flow to the brain. Copyright American Heart Association
Ischaemic stroke patients previously considered unlikely to survive without severe disability may regain far more function if the blood clots are mechanically removed in addition to standard medical therapy, according to preliminary late-breaking research presented today at the American Stroke Association’s International Stroke Conference 2022.
In 2018, the American Heart Association’s stroke treatment guidelines were updated to recommend endovascular therapy (mechanical clot removal) for select stroke patients to improve the odds of functional recovery. This new study in Japan is the first randomised, controlled trial to demonstrate the effectiveness of endovascular therapy in patients with severe strokes involving clots in one or more large brain arteries, causing a large blood flow interruption in the brain. This approach had worked for patients with fewer areas of the brain disrupted, however, clinical experience was mixed for patients with more severe strokes.
Infarction area, or core area, estimates the volume of brain affected and describes the blockage location as seen on a brain CT. A lower number translates to a stroke affecting more core areas of the brain: 8-10=small core, 6-7=moderate core and 0-5=large core. Current US stroke guidelines recommend endovascular therapy for core areas 6-9. This study examined blockages that scored as 3-5. Strokes with blockages measuring 0-2 core areas are considered too severe and highly unlikely the patient would return to ambulatory independence.
“I have often encountered a dramatic improvement in a patient just after the mechanical clot removal procedure, even when the infarction area was large. Yet, patients sometimes also experienced severe haemorrhagic transformation [a life-threatening complication that occurs when blood from outside the brain crosses the blood-brain barrier and worsens stroke outcome] after the artery was reopened. So, in Japan, our stroke physicians are always cautious about endovascular therapy when the infarction area is large,” said Professor Shinichi Yoshimura, lead author of the study.
This randomised study included 203 stroke patients (average age of 76 years; 44% women). Most (71%) were examined and had MRI or a CT scan of the brain within 6 hours after stroke symptoms were first noticed, when patients are generally considered eligible for endovascular therapy. The other patients were seen between 6-24 hours after symptoms were noticed, and additional imaging showed areas of the brain that might benefit from prompt treatment.
On imaging, all patients were found to have clots blocking a large cerebral artery – either the internal carotid artery, the proximal middle cerebral artery or both. The strokes were rated as severe (median 22 on the National Institutes of Health (NIH) Stroke Scale,) and involved disrupted blood flow to large areas of the brain (about 7 out of 10 regions).
After imaging, the patients were randomly selected to receive either standard medical care for stroke (intravenous fluids, controlling blood pressure and other risk factors, and thrombolytics for lower bleeding risk patients) or standard medical care plus endovascular therapy performed within an hour after imaging to mechanically remove the clots. Due to bleeding concerns, intravenous thrombolytics were sparingly administered to select patients in a similar proportion in both treatment groups (27 of those who received endovascular therapy and 29 who received standard care).
Comparing the 100 patients who received endovascular therapy with 102 on standard therapy alone, the analysis found:
Patients who received endovascular therapy were 2.43 times more likely (31% vs 13%) to be able to walk unassisted and to have a residual disability rated as none to moderate 90 days later.
After 90 days, more of the patients (14% vs. 6.9%) who received endovascular therapy were considered functionally independent, meaning they were either able to carry out all their pre-stroke activities or to have a slight disability that did not require daily assistance.
At 48 hours after treatment, more of the patients (31% vs. 8.8%) who received endovascular therapy had major early neurological improvement.
“Our findings confirm that anyone who suffers from stroke should be transferred to a medical facility capable of endovascular therapy as soon as possible. The benefit of endovascular therapy is not limited by the severity or region of a stroke. These patients may have the chance to more fully recover from stroke and go back to their previous lives and activity levels,” said Professor Takeshi Morimoto, senior author of the study.
Several outcomes were compared to evaluate the safety of adding endovascular therapy to medical treatment, with researchers reporting:
Within 48 hours, scans revealed that more of the patients who received endovascular therapy had experienced some bleeding within the brain (with or without symptoms), 58% vs. 31%, respectively.
However, the number of patients who experienced other adverse outcomes was similar in the two treatment groups. The adverse events included brain bleeding within 48 hours that caused a worsening of neurological status (4 points or greater worsening on the NIH Stroke Scale); the need for surgery to relieve pressure on the brain in the first week; death within 90 days; or the recurrence of ischaemic stroke within 90 days.
“The finding of more intracranial bleeding in the patients who received endovascular therapy is very important. However, there were haemorrhages with symptoms and some that caused no symptoms. The haemorrhages with no symptoms were detected on imaging conducted for this study in the endovascular treatment group, not in the standard practice group. Symptomatic intracranial haemorrhage still occurred more commonly among patients in the endovascular group, however, it was not a statistically significant difference from the standard care group,” Morimoto said.
Due to different treatment protocols in Japan, where there is less use of intravenous thrombolysis than in the US and other western countries, and where more strokes are imaged with MRI than CT, this study’s results may over- or underestimate the effectiveness of endovascular therapy.
The researchers are currently performing sub-analyses to help identify factors that might signal which patients are more likely to have a greater return of function after the treatment. “In addition, tools, devices or rehabilitation methods that could potentially improve the likelihood for similar patients to recover with less disability should be investigated,” Morimoto said.
There is convincing evidence that micronutrients, such as iron, selenium, zinc, copper, and coenzyme Q10, can impact the function of cardiac cells’ energy-producing mitochondria to contribute to heart failure according to a review published in the Journal of Internal Medicine.
Research has established a relationship between poor cardiac performance and metabolic perturbations, including deficits in substrate uptake and utilisation, reduction in mitochondrial oxidative phosphorylation and excessive reactive oxygen species production. Together, these disturbances result in depletion of cardiac adenosine triphosphate (ATP) and loss of cardiac energy. Delivering more energy substrates such as fatty acids to the mitochondria will be worthless if the mitochondria can’t turn them into fuel.
Micronutrients are required to efficiently convert macronutrients to ATP. However, studies have shown that up to 50% of patients with heart failure have deficiencies in one or more micronutrients. “Micronutrient deficiency has a high impact on mitochondrial energy production and should be considered an additional factor in the heart failure equation,” the authors argued. Their findings suggest that micronutrient supplementation could represent an effective treatment for heart failure.
“Micronutrient deficiency has a high impact on mitochondrial energy production and should be considered an additional factor in the heart failure equation, moving our view of the failing heart away from ‘an engine out of fuel’ to ‘a defective engine on a path to self-destruction’,” said co–lead author Nils Bomer, PhD, of the University Medical Center Groningen, in The Netherlands.
An accompanying editorial suggests a large trial to see if there is indeed a clinical benefit.
More intensive hypertension treatment could help prevent or delay strokes in older adults, according to an analysis of results from randomised clinical trials published in the Journal of the American Geriatrics Society.
The researchers initially screened 22 trials for inclusion. Nine trials involving 38 779 adults with an average age ranging from 66 to 84 years were included in the analysis, with follow-up times ranging from 2.0 to 5.8 years.
On average, the researchers found that it took 1.7 years to prevent 1 stroke for 200 older persons treated with more intensive hypertension treatment.
For older adults with baseline systolic blood pressures below 150 mmHg, the time to benefit from more intensive hypertension treatment was longer than 1.7 years; for older adults with baseline systolic blood pressure above 190 mmHg, the time to benefit was shorter than 1.7 years.
In their discussion, the researchers noted the risks of aggressive hypertension treatment, including hypotension, syncope and falls. However, they noted that emerging evidence shows that the increase in fall risk is transient.
“While the 2017 American College of Cardiology/American Heart Association guidelines recommend individual risk discussions about hypertension treatment for primary prevention in older adults, there is a critical gap in data about how long a patient needs to receive blood pressure treatment before they will benefit – or the blood pressure treatment’s time to benefit,” said lead author Vanessa S. Ho, MS, of California Northstate University College of Medicine. “A treatment’s time to benefit is an especially important consideration for patients with a limited life expectancy who may experience immediate burdens or harms from any additional medication.”
Ebola virus (green) is shown on cell surface. Credit: National Institutes of Allergy and Infectious Diseases, NIH
A new study has shown that the Ebola vaccine known as rVSVΔG-ZEBOV-GP instils a robust and enduring antibody response among vaccinated individuals in areas of the Democratic Republic of Congo that are experiencing outbreaks of the disease.
The study, published in PNAS, is the first to examine post–Ebola-vaccination antibody response in the DRC, a nation of nearly 90 million. Long-term analyses of the study cohort will continue, but in the meantime, the findings will help inform health officials’ approach to vaccine use for outbreak control, the researchers said.
Ebola, one of the world’s deadliest viral diseases known to infect humans, was first identified in 1976 following an outbreak near the Ebola River in then Zaire (now DRC). Since then, outbreaks have occurred intermittently in sub-Saharan Africa, including 12 outbreaks in the DRC, where the disease remains endemic.
The single-dose rVSVΔG-ZEBOV-GP vaccine was administered to more than 300 000 individuals in the DRC during outbreaks between 2018 and 2020. However, studies examining the antibody response of vaccinated Congolese populations had been lacking.
US and DRC researchers studied individuals who received the vaccine during an Ebola outbreak in the DRC’s North Kivu Province. Between August and September 2018, 608 eligible individuals were vaccinated. In an approach known as “ring vaccination”, these participants were contacts of people infected with Ebola or contacts of those contacts as well as health care and frontline workers in affected or potentially affected areas. Blood samples were taken at the time of vaccination, 21 days later and again after six months. They found that after 21 days, 87.2% of the study participants showed an antibody response and antibody persistence was seen in 95.6% after six months.
A new study published in the Journal of Sleep Research found a complicated relationship between media use and bedtime and sleep quality and duration, with short, simple media use resulting in earlier bedtime and longer sleep duration.
Many factors contribute to sleep disturbance among young adults. Use of media is increasing rapidly, and little is known regarding its association with sleep disturbance. Previous research showed that social media use before bedtime in young adults resulted in reduced and poorer quality sleep.
The study examined how sleep might be impacted by media use – such as watching movies, television, or YouTube videos; browsing the Internet; or listening to music – before bed.
In the study, 58 adults kept a diary that recorded information related to time spent with media before bed, location of use, and multitasking. Electroencephalography captured parameters such as bedtime, total sleep time, and sleep quality.
Media use in the hour before sleep was associated with an earlier bedtime. If the before-bed use did not involve multitasking and was conducted in bed, it was also associated with more total sleep time. A long use of media associated with later bedtime and less total sleep time.
Sleep quality, operationalised as the percent of total sleep time spent in N3 and REM sleep, was unaffected by media use before bed.
“If you are going to use media, like watching TV or listening to music, before bed, keep it a short, focused session and you are unlikely to experience any negative outcomes in your sleep that night,” said lead author Morgan Ellithorpe, PhD, of the University of Delaware.
Despite the fact that hospitalised patients are in a monitored environment, stroke evaluation and treatment are often delayed compared to patients arriving with a stroke at the emergency department, contributing to higher rates of morbidity and mortality for in-hospital stroke.
This is according to an American Heart Association scientific statement published in Stroke. This scientific statement was discussed at the Association’s International Stroke Conference in New Orleans. An American Heart Association scientific statement is an expert analysis of current research and may inform future clinical practice guidelines. This follows on from a previous 2019 update on recommendations systems of care to improve patient outcomes in stroke.
The statement outlines five elements for the development of hospital systems of care and targeted quality improvement to reduce delays and optimise treatment to improve outcomes for patients who experience an in-hospital stroke. In-hospital stroke is a stroke that occurs during a hospitalisation for another diagnosis and affects between 35 000 and 75 000 hospitalised patients annually in the United States.
The five core elements of the statement are:
training all hospital staff on stroke signs, symptoms and activation protocols for in-hospital stroke alerts;
creating rapid response teams with dedicated stroke training and immediate access to neurologic expertise;
standardising the evaluation of potential in-hospital stroke patients with physical assessment and imaging;
eliminating and addressing potential treatment barriers including interfacility transfer to advanced stroke treatment; and
establishing an in-hospital stroke quality oversight program delivering data-driven performance feedback and driving targeted quality improvement efforts.
The statement encourages institutions to develop a plan for in-patient stroke response teams that includes education, quality review and specified oversight.
The statement was developed by the writing committee on behalf of the American Heart Association’s Stroke Council; the Council on Arteriosclerosis, Thrombosis and Vascular Biology; the Council on Cardiovascular and Stroke Nursing; the Council on Clinical Cardiology; and the Council on Lifestyle and Cardiometabolic Health. The diverse committee included experts in nursing, neurology, internal medicine, neurocritical care, neurosurgery and neurointerventional radiology. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists, and the American Association of Neurological Surgeons/Congress of Neurological Surgeons Cerebrovascular Section affirms the educational benefit of this statement.
American Heart Association scientific statements promote greater awareness about cardiovascular diseases and stroke issues and help facilitate informed health care decisions. Scientific statements outline what is currently known about a topic, and what areas need additional research. While scientific statements inform the development of guidelines, they do not make treatment recommendations. American Heart Association guidelines provide the Association’s official clinical practice recommendations.