Johannesburg, 11 November 2025:As we approach World Diabetes Day on November 14, civil society organisations warn that the cost of inaction on non-communicable diseases (NCDs) such as diabetes is already being paid for in lives, livelihoods and lost potential. The Healthy Living Alliance (HEALA) is calling on the South African government to increase the Health Promotion Levy (HPL) on sugary drinks from 11% to 20%, to help curb sugary drinks consumption and reduce the financial burden on the health system from rising non-communicable diseases.
“Diabetes is now the second leading cause of death in South Africa,1 yet every year we allow preventable diseases to claim more lives,” says Nzama Mbalati, CEO of HEALA. “Raising the Health Promotion Levy is one of the simplest, most effective steps government can take to protect people’s health, especially children, who are consuming sugar at dangerous levels.”
Since the introduction of the HPL in 2018, beverage companies have reduced the sugar content of their drinks, leading to cuts in average per-capita sugar consumption. But the gains have stalled. HEALA and its partners warn that without further cuts in consumption, the policy’s impact will fade, while rates of diabetes will continue to climb.
South Africa’s obesity rate is already twice the global average, and even one sugary drink a week raises a child’s risk of obesity and diabetes.2,3 One in four diabetes cases in the country is caused by sugary drink consumption.4 These numbers are not just statistics; they represent real people and families forced to navigate lifelong illness and financial hardship.
The economic toll is equally alarming. Treating obesity related conditions such as diabetes already costs South Africa more than R33 billion each year or about 15% of total government health spending.5 Modelling by PRICELESS SA (University of the Witwatersrand) shows that increasing the levy to 20% could save approximately 72 000 lives and prevent 85 000 strokes over two decades while easing the fiscal pressure on a health system already stretched beyond capacity.5
HEALA’s new national campaign, which launched in November, brings this message to the fore in two phases. The first calls for stronger health taxes across sugary drinks, alcohol and tobacco, continuing South Africa’s proven track record of using taxation to advance public health. The second sharpens focus on raising the HPL, calling for its increase as part of a consistent, evidence-based approach to protecting lives.
Through personal stories of South Africans living with diabetes, the campaign reveals the real cost of inaction and unites civil society under the banner #OneVoice, calling on government to put public health before profit.
Alphinah Setumo, a 52-year-old mother from Mathibestad, lost both her legs and her eyesight after years of consuming sugary drinks without understanding the risks. “Back then, drinking two litres of a sugary drink a day was nothing,” she recalls. “If I had known what I know now, my life would be different.”
Mpho Thebe, a maths and science tutor from Kroonstad, tells a similar story. Once a daily consumer of fizzy drinks, he lost his left leg to diabetes at 45. Today, he walks with a prosthetic leg and teaches children about perseverance and prevention. “I thought sugar was harmless,” he says. “Now I know it can take everything from you.”
These stories mirror thousands of others across the country, where diabetes silently devastates families, especially in low-income communities where affordable, healthy food and clean water remain scarce.
The campaign, supported by actress and mother Samela Tyelbooi, urges government to act. “As a parent, I worry about how sugar can make my kids sick,” says Tyelbooi. “We need government to increase the HPL, protect our children’s future, and stop putting profit before people.”
HEALA’s coalition partners, including health advocates, researchers and civil society organisations, are speaking with one voice ahead of the Medium-Term Budget Policy Statement and the 2026 Budget Speech. Their collective message is clear: the HPL is not just another tax, it’s a health tax, like those on alcohol and tobacco, designed to save lives, prevent disease and safeguard South Africa’s future.
“This is not about taking away people’s choices, it’s about giving South Africans the chance to make healthier, more informed choices,” adds Mbalati.
Diabetes and other NCDs already account for over 50% of deaths from preventable diseases in South Africa.5,6 Without decisive fiscal measures, the burden will continue to fall on the households least able to bear it.
Globally, countries from Mexico to the UK have proven that health taxes reduce sugar consumption and improve health outcomes.
HEALA is urging citizens to join the call by signing the petition and demanding that government increase the HPL to 20%.
“We have the evidence, we have the stories, and we have the will,” concludes Tyelbooi. “Now we need action.”
Fundi, South Africa’s leading education finance and student solutions provider, has launched FundiHealth: a healthcare platform designed to meet the unique needs of students, young professionals and organisations committed to supporting the health and wellbeing of their people.
As part of its digital transformation and enablement strategy, Fundi has launched its own healthcare platform: FundiHealth.
Born out of Fundi’s deep understanding of the challenges students face and the recognition that health is a critical enabler of success, the platform offers affordable quality healthcare solutions for students and young professionals. “We’ve always believed that education unlocks potential, but we also see every day how poor health and the inability to afford care can derail even the most promising futures,” explains Benedict Johnson, Fundi Executive Head: EBS and New Initiatives. “Our platform was created with one clear purpose in mind: to remove healthcare as a barrier to education, productivity and meaningful participation in the economy.”
Fundi CEO Mala Suriah, moderator on the day ,Thembekile Mrototo and Fundi Executive Head Benedict Johnson at the FundiHealth launch.
The solution has been launched at a time when South Africa is grappling with a significant gap in healthcare coverage. According to the Council for Medical Schemes (2024), over 80% of South Africans do not belong to a medical aid scheme and rely entirely on the overstretched public health system. Young people are particularly vulnerable notes Charles Irumba, FundiHealth Executive: “Research from the Board of Healthcare Funders (2023) shows that fewer than 12% of students and young professionals under the age of 30 have adequate medical cover. This lack of access has serious implications not only for individual wellbeing but also for South Africa’s productivity and growth.” Data from Statistics South Africa (2024) further supports this; with absenteeism due to preventable illness costing the economy over R16 billion annually, with students and entry-level workers among the most affected.
“When students drop out of school because of untreated illnesses – including stress, depression or anxiety – or when young professionals miss work and lose income as a result, it has a detrimental effect on them as well as their families,” says Irumba. “FundiHealth ensures that young South Africans stay healthy in class and at work, contributing meaningfully to their futures and to our country’s growth and development.”
The new platform offers affordable, accessible medical cover that includes access to private doctors, medication, mental health support and preventative care services, all designed to fit the budgets of students, families and young professionals. “Critically, we’ve also created an option that allows organisations to offer their entry-level staff healthcare benefits at a fraction of the cost of traditional schemes. This is ideal for SMMEs and growing businesses, as it will assist them improve staff retention, morale and productivity,” adds Johnson. “Employers often underestimate the economic impact of poor health among their youngest and most vulnerable employees. By offering a healthcare solution like FundiHealth, they’re not just supporting their people, they’re strengthening their businesses too. Healthy employees are more engaged, more present and more productive. It’s a win-win.”
Beyond immediate productivity benefits, FundiHealth also has the potential to alleviate pressure on South Africa’s public health system by shifting some demand into the private sector and by promoting preventative care among young people. “If we want to grow as a nation, we have to keep our young people healthy in body, mind and spirit,” notes Irumba. “That’s what FundiHealth is all about. Good health is not a ‘nice-to-have’. It is a fundamental part of what it takes to succeed.”
FundiHealth is available to students, their families, young professionals and organisations at fundihealth.co.za. Customers can both explore different plan options and sign-up online.
“With FundiHealth, we’re tackling one of the most overlooked challenges to achieving one’s full potential: health. Good health underpins everything. By keeping our students and young professionals healthy, we’re keeping their dreams alive and South Africa moving forward,” Johnson concludes.
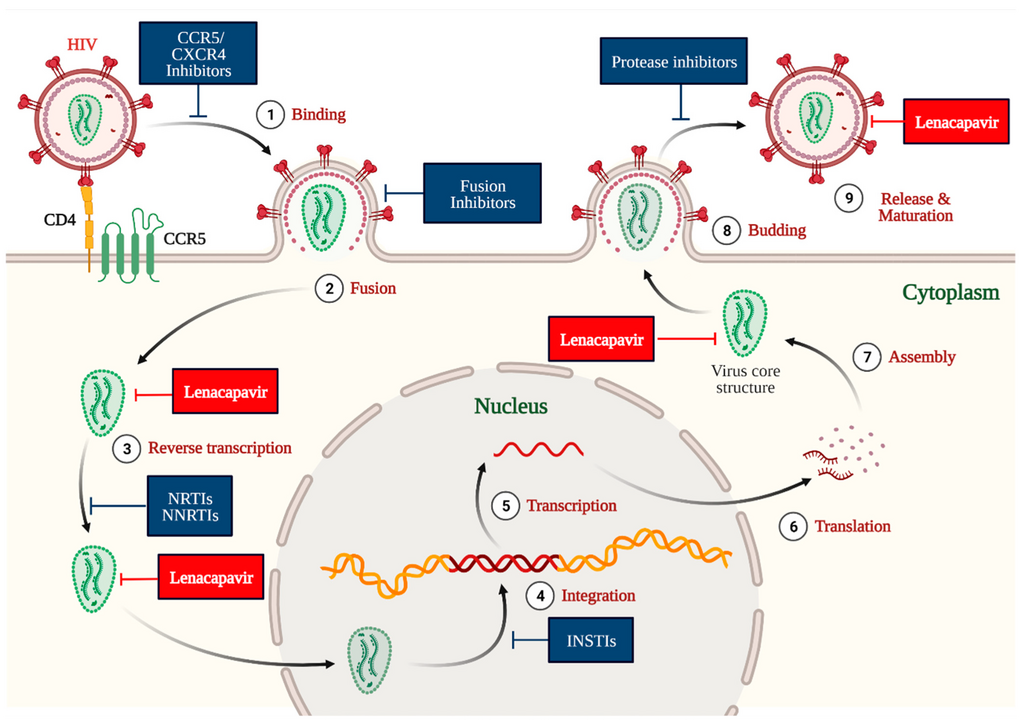
Pretoria, 27 October 2025 – The South African Health Products Regulatory Authority (SAHPRA) is pleased to announce the registration of Lenacapavir. Lenacapavir is an antiviral medicine that is recommended, in combination with safer sex practices, for pre-exposure prophylaxis (PrEP) to prevent HIV-1 infection in adults and adolescents weighing at least 35kg.
An application by Gilead was submitted to SAHPRA in March 2025. The SAHPRA review process was done in collaboration with the European Medicines for All Procedure (EU-M4all). This procedure enables the European Medicines Agency (EMA), together with the participating regulatory authorities, to provide scientific opinions on high-priority medicines, such as Lenacapavir, intended for markets outside the European Union. The benefits of this pathway are to strengthen regulatory systems and accelerate access to essential medicines.
This product, developed to prevent new HIV infections, is a six-monthly injection. There is an initiation dose of a subcutaneous injection (administered just under the skin) with tablets (taken on days 1 and 2). It is used to reduce the risk of HIV in adults and adolescents who weigh at least 35kg, are HIV negative, and are at risk of getting HIV. Lenacapavir for PrEP should always be used in combination with safer sex practices, such as using condoms, to reduce the risk of getting other sexually transmitted infections.
“The registration of Lenacapavir is a game-changer, given the high prevalence rate of HIV in South Africa. This product is the most effective HIV prevention measure thus far,” indicated Dr Boitumelo Semete-Makokotlela, CEO: SAHPRA.
ThriveLink to connect patients, doctors, caregivers, and medical schemes in a seamless digital platform
The last thing someone dealing with a life-threatening disease wants is the pain of endless administrative paperwork and confusion that arises when aspects of their care are not easily coordinated. Altron HealthTech is set to pilot a solution designed to minimise these burdens by integrating various aspects of care management into one solution.
The company announced today that it will soon begin piloting ThriveLink, South Africa’s first platform to connect patients, doctors, caregivers, and medical schemes in one integrated digital space. The oncology companion app is designed to help cancer patients flourish during a trying time by providing seamless care coordination, access to key information and educational content and removal of administrative obstacles.
“We’ve built this tool with the ultimate goal of making life easier for cancer patients to be empowered throughout managing their treatment journey,” says Altron HealthTech MD Leslie Moodley. “They’ll receive appointment tracking, medication reminders, and secure communication with their care team – all customised for their unique treatment plan in one digital space – so they can focus on what matters most: their health and wellbeing.”
Addressing a growing crisis
The development team was inspired to create ThriveLink after frontline agents logged an alarming increase in cancer diagnoses. Cancer cases in South Africa are projected to nearly double from 62 000 in 2019 to 121 000 nationally by 2030 based on data compiled by the SA Journal of Oncology, driven by an aging population and increased lifestyle risks.
“We have insight into anonymised and aggregated data, and were shocked at the increase in cancer volumes,” says Moodley. “We realised there was value in developing a tool that could span the entire healthcare value chain and all the various touchpoints, to solve for a very real issue. This insight sparked a critical question: how can we make it easier for oncologists, our key stakeholders, to focus on what matters most – patient care?
ThriveLink brings together data from specialists, medical aids, pharmacies, and other relevant sources to coordinate care to connect healthcare providers. Beyond appointment tracking and medication reminders, the app offers educational content, emotional support tools, and secure communication channels.
“The solution enables these data points to collaborate in a technical sense to coordinate care,” explains Moodley. “Our response was to build a technology-driven platform that not only streamlines authorisations and treatment protocols but also enables real-time interoperability. This empowers oncologists to coordinate care more efficiently, track treatment pathways, and adapt plans based on patient-specific outcomes. Patients won’t have to worry about burdensome details and will get reminded when it’s time to take their medication or schedule a follow-up.”
Built on medical expertise and security
The app serves as the vital link in a complex ecosystem, ensuring secure information flow, informed decision-making, and trust at every stage.
Altron HealthTech consulted widely with oncologists, patients, and other medical professionals before beginning development. A base application was rolled out to specialists about a year ago, and feedback from that pilot informed the expanded platform now ready for patient testing.
The app has been built on secure, cloud-based software-as-a-service architecture in compliance with the Protection of Personal Information Act and all relevant regulatory requirements. Patients must provide informed consent before signing up.
Beyond supporting patients directly, ThriveLink is designed to help control healthcare costs. Cancer is among the most expensive therapeutic burdens, with the Cancer Alliance having predicted that this disease will cost the public sector an additional R50 billion between 2020 and 2030.
“By streamlining processes and integrating claims, authorisations, and clinical data, we remove duplication and costs from the system,” says Moodley. “This can indirectly help keep medical aid premiums down, benefiting all medical scheme patients.”
Altron HealthTech is in early-stage discussions with medical aid schemes interested in integrating the app into their mobile solutions.
#InsideTheBox is a column by Dr Andy Gray, a pharmaceutical sciences expert at the University of KwaZulu-Natal and Co-Director of the WHO Collaborating Centre on Pharmaceutical Policy and Evidence Based Practice. (Photo: Supplied)
By Andy Gray
In several countries, the public is given an opportunity to share their views with regulators before new medicines are registered or to engage with those choosing essential medicines. In South Africa, however, opportunities for such public participation remains limited. In his latest #InsideTheBox column, Dr Andy Gray takes a look at how public participation is handled elsewhere and how it could be improved here.
One of the rallying cries of patient and community-based organisations has long been “nothing about us, without us”. The “patient voice” is, however, not always heard in medicines selection or medicines regulation.
How it works in the US and Europe
Recent highly contested medicines regulatory decisions in the United States, such as the warnings about paracetamol use in pregnancy, have highlighted the role of advisory committees to the Food and Drug Administration (FDA). The FDA relies on a number of such committees to provide advice on regulatory questions, such as whether to approve a new medicine or how to manage emergent safety signals. The FDA usually follows the advice provided by these independent structures, but is not bound to do so.
The fact that advisory committees meet in open session, and that their recommendations are transparent to the public, means that the final decision by the FDA can be contrasted with the scientific advice. The curricula vitae of advisory committee members are posted on the FDA website and updated annually. Critically, when an advisory committee meeting is scheduled, the date and time is announced at least 15 days in advance of the meeting, and this serves as an invitation to interested parties to register to make oral submissions during the Open Public Hearing portion of the meeting.
In addition to providing opportunities for public engagement in this manner, the FDA has also operated a Patient Representative Program since 2024. FDA Patient Representatives are appointed, provided with training, and may then engage with the scientific and other expert members of the advisory committees. Among the criteria applied in their selection are personal experience with a particular disease as a patient or primary caregiver, knowledge about the treatment options and research in that area, and the willingness and ability to communicate in public, as well as being objective while representing the concerns of others affected by the disease.
Similar mechanisms have been put in place in Europe. The European Medicines Agency (EMA) has enabled the appointment of patients as members of its management board and scientific committees. In addition, the EMA Patients’ and Consumers’ Working Party provides a venue for ongoing engagement. The EMA engagement framework explicitly aims to ensure “access to patients’ real-life experiences of living with a condition, its management and the current use of medicines, complementing the scientific evidence provided during the evaluation process” and “the generation, collection and use of evidence-based patient experience data for benefit-risk decision-making”.
How it works in South Africa
Section 3(9) of the Medicines and Related Substances Act, 1965, instructs the chief executive officer of the South African Health Products Regulatory Authority (SAHPRA) to appoint advisory committees. The wording is peremptory, but also broadly enabling: “The Chief Executive Officer shall, in consultation with the Board, appoint committees, as he or she may deem necessary, to investigate and report to the Authority on any matter within its purview in terms of this Act.” Provided there is consultation with the Board of the Authority, the number of committees and their membership is left to the CEO to decide.
To date, however, there has been no deliberate effort to include patient or consumer representatives on any of the advisory committees.
More importantly, meetings of the committees are not open to the public, nor are their recommendations to the regulatory authority placed in the public domain. The “patient voice” is therefore potentially missed, and stakeholders are unable to determine when or how final decisions taken by the Authority may differ from the recommendations made by the technical advisory committees. In that sense, SAHPRA is no more transparent than its predecessor the Medicines Control Council, which also laboured under the same antiquated secrecy provision in the Act. Section 34 of the Act is actually labelled “Preservation of secrecy”.
Similar concerns with medicines selection
Medicines regulators determine whether medicines should be allowed onto the market and how those should be controlled. Similar dynamics are at play in determining which medicines are “essential” and should be procured or reimbursed by health systems.
At a global level, the World Health Organization (WHO) updates its Model List of Essential Medicines every two years. The Model List is a starting point for many countries’ efforts to develop national essential medicines lists, guiding procurement in their public sectors. Although the expert committee responsible for this work does not explicitly include patient representatives, all proposals submitted are placed in the public domain, as are the reviews conducted, and an account of the final decisions. On the first day of the meeting, an open session is held at which stakeholders are invited to apply to present.
One of the most trusted medicine selection bodies is the UK National Institute for Health and Care Excellence (NICE), which also has a deliberate process for stakeholder engagement at multiple steps in its guideline development. For example, right at the outset, this invitation is issued: “NICE invites all stakeholder organisations to attend a scoping workshop. You will be sent a first draft of the scope, which will be discussed at the meeting. We encourage you to send someone who knows about and can represent patients and carers’ interests.”
Medicines selection in the South African public sector is evolving, embracing the challenge of health technology assessment. While there are as yet no patient representatives on either the Expert Review Committee or the National Essential Medicines List Committee, there are opportunities for stakeholder engagement with draft guidelines and increasing transparency, with medicines evaluation reports posted on the Department of Health website.
Full medicine reviews follow an evidence-to-decision framework that was first piloted during the height of the COVID-19 pandemic. One of the questions posed reads: “Is there important uncertainty or variability about how much people value the options?” This question is aligned with what the WHO Handbook for Guideline Development refers to as “values and preferences”. For example, the WHO guidance calls for evidence of the “values and preferences of the people receiving the intervention or experiencing the outcomes the intervention can affect”. While that evidence may sometimes be reported in the scientific literature, all too often it is lacking.
Ultimately, “nothing about us, without us” should not only be a demand made by patients, but also by those who care about the quality, reliability and acceptability of medicines selection and regulatory decisions. Improving the transparency of decision-making processes is critical, but so is creating, promoting and protecting the spaces for an effective “patient voice”. Doing so is a critical investment in building trust, which is so easily eroded.
*Dr Gray is a Senior Lecturer at the University of KwaZulu-Natal and Co-Director of the WHO Collaborating Centre on Pharmaceutical Policy and Evidence Based Practice. This is part of a series of #InsideTheBox columns he is writing for Spotlight.
Disclosure: Gray is a member of South Africa’s National Essential Medicines List Committee and co-chairs its Expert Review Committee.
Note: Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.
Both Leathan (L) and Godfrey (R) have aplastic anaemia, which can treated with a stem cell donation. Leathan received stem cells from his twin sister, who is a perfect match. But Godfrey must travels from KwaMhlanga to Pretoria for life-sustaining blood transfusions.
When aplastic anaemia struck two young South Africans, their fates diverged dramatically. While one received a life-saving stem cell transplant, the other continues to fight every day. The rare blood disease affects fewer than six people per million, but for Leathan and Godfrey, the statistics became deeply personal.
Understanding Aplastic Anaemia: When Hope Meets Science
Aplastic anaemia is a devastating condition where the bone marrow fails to produce sufficient blood cells, leaving patients vulnerable to infections, bleeding, and severe anaemia. Given this rare disease’s high mortality rates, prompt recognition and immediate action are critical for survival. “The challenge with aplastic anaemia is that early symptoms can be subtle,” explains Dr Gugulethu Jali, a Clinical Haematologist and Haematopathologist at the Department of Health Kwa-Zulu Natal. “However, advances in treatment, particularly hematopoietic stem cell transplantation (HSCT), have transformed the prognosis, with survival rates now exceeding 80% when matched donors are found.”
Leathan’s Journey: From Crisis to Recovery
Seventeen-year-old Leathan had his whole life mapped out. The passionate soccer player dreamed of becoming a criminal lawyer, balancing his love for the game with serious academic ambitions. But subtle symptoms began to appear, including weight loss and nosebleeds that seemed minor at first.
When he suddenly collapsed at home, his family rushed him to hospital where doctors discovered his blood levels were critically low. Tests revealed that his bone marrow had completely stopped producing blood cells. Without immediate intervention, he would need blood transfusions and platelets for the rest of his life.
But Leathan had something that changes everything in aplastic anaemia cases: a perfect genetic match. His twin sister, without hesitation, donated her stem cells , giving her brother the ultimate gift of life.
Today, Leathan represents the success story that medical advances have made possible. Since the transplant, he has not needed further transfusions, and his blood counts are steadily stabilising. However, he may still need additional stem cell support to fully restore his health.
Currently, he’s on the path back to his soccer dreams and law school aspirations, a living example of what’s achievable when the right match is found.
Godfrey’s Battle: The Same Disease, Different Circumstances
While Leathan’s recovery shows what’s possible, eleven-year-old Godfrey from KwaMhlanga, Mpumalanga, is still living with the daily reality of aplastic anaemia. Like Leathan, Godfrey was once full of energy and loved soccer.
Then the familiar pattern began to emerge: Godfrey started moving more slowly, struggling with everyday tasks that once came easily. When uncontrollable bleeding began, his family knew something was seriously wrong. After a long diagnostic journey that began in 2019, Godfrey received the same diagnosis Leathan had faced: aplastic anaemia.
Unlike Leathan, Godfrey doesn’t have a twin sister who’s a perfect match. Instead, every month, he travels from KwaMhlanga to Pretoria for life-sustaining blood transfusions. The physical and emotional toll has been devastating. He was unable to pass Grade 5 last year, not because he lacks ability, but because fighting for your life leaves little energy for schoolwork.
Your Role in Changing Godfrey’s Story
For Godfrey to follow the same path as Leathan, he needs his genetic match. That person could be you.
Compatible donors are often found within similar ethnic backgrounds, making diversity in donor registries crucial for patients like Godfrey. If you’re between 17 and 55 and in good health, registering as a stem cell donor takes minutes and costs nothing. Register today at https://www.dkms-africa.org/save-lives.
Webber Wentzel’s Pro Bono team represented Mr and Mrs van Wyk in a landmark case that has resulted in the Constitutional Court confirming that South Africa’s statutory four months of parental leave may be shared between both parents. The ruling marks a significant step toward gender equality in the workplace and family law.
The case challenged the unequal parental leave provisions under section 25 of the Basic Conditions of Employment Act (BCEA), which granted birthing mothers up to four months of maternity leave while limiting fathers to only 10 days.
Webber Wentzel argued that section 25 of the BCEA unfairly discriminated against fathers and placed an undue burden on birthing mothers by not allowing families to decide who should be the primary caregiver. The court agreed and criticised the 10-day leave for fathers by rejecting the cultural norms that reinforce gendered parenting roles as inconsistent with constitutional values.
The application was supported by the Commission for Gender Equality (CGE) and Sonke Gender Justice (Sonke). CGE advocated for equal parental leave for adoptive and surrogacy-commissioning parents, which the court partially granted. Sonke’s request for an equal 16-week leave for both parents was not granted.
The Constitutional Court, in a unanimous judgment delivered by the Honourable Justice Tshiqi, confirmed that sections 25, 25A, 25B and 25C of the BCEA, along with corresponding provisions of the Unemployment Insurance Fund Act (UIF Act), are unconstitutional. The Court held that these provisions violate the rights to equality and human dignity under sections 9 and 10 of the Constitution.
The Minister of Employment and Labour accepted that differentiation exists between birthing mothers and other categories of parents is automatically unfair as it is based on grounds specified in section 9(3) of the Constitution. Further, the Minister acknowledges that there is a need for reform in the current legislation pertaining to the parental leave regime contained in the BCEA.
As a result of the ruling in the Constitutional Court, the 4 months of maternal and the 10 days of parental leave will be combined into a total of 4 months and 10 days, which parents may now share as they choose. If no agreement is reached, the leave will be split equally. Where only one parent is employed, that parent will be entitled to the 4 consecutive months of parental leave.
The Constitutional Court also confirmed that the same parental leave provisions apply to adoptive parents and commissioning parents in a surrogacy arrangement.
The Constitutional Court has suspended the declaration of invalidity of the relevant BCEA and UIF Act provisions for a period of 36 months, to allow the legislature to remedy the necessary constitutional defects. In the interim, the following principles will apply:
A single parent or a parent who is the only employed parent is entitled to four months’ consecutive parental leave.
Parents who are both employed may share the allocated parental leave of four months and 10 days between them, concurrently or consecutively.
An adoptive parent of a child younger than two years is entitled to four months’ consecutive parental leave.
If an adoption order is granted in respect of two parents, they may share the allocated parental leave of four months and 10 days between them, concurrently or consecutively.
A commissioning parent is entitled to four months’ consecutive parental leave.
Where there are two commissioning parents, they may share the allocated parental leave of four months and 10 days between them, concurrently or consecutively.
Employers are encouraged to review and, where necessary, update their leave policies and employment contracts to reflect the new parental leave framework.
“This judgment is a powerful affirmation of the constitutional rights to equality and dignity,” said Nkosinathi Thema, senior associate, Webber Wentzel. “It recognises that caregiving is not the exclusive responsibility of mothers and that both parents should have the freedom to decide how best to care for their child.”
The Webber Wentzel team comprised Ayanda Khumalo, Nkosinathi Thema and Lize-Mari Doubell. Counsel Nasreen Rajab-Budlender SC, Liam Minné and Sanan Mirzoyev appeared on a pro bono basis.
Founded in 1868, Webber Wentzel is a leading full-service law firm providing clients with innovative solutions to their most complex legal and tax issues across Sub-Saharan Africa. With over 450 lawyers, their multi-disciplinary expertise is consistently ranked top tier in leading directories and awards, both in South Africa and on the African continent. Their collaborative alliance with Linklaters and their deep relationships with outstanding law firms across Africa provide clients with market-leading support wherever they do business.
The country that performed the first successful heart transplant has very low organ donation rates. Now a student-run medical non-profit is hoping to make a difference. (Photo: Nasief Manie/Spotlight)
By Elri Voigt
Thousands of people in South Africa are waiting for a life-saving organ transplant, but our very low organ donation rates mean that many won’t get a transplant in time. Spotlight asks the experts why our donation rates are so low and what can be done about it.
Back in 2002, Rentia le Roux received a horrifying diagnosis that her kidneys were failing. “My kids still need me, they are still small, what are we going to do?” Le Roux recalls telling her doctor. After a long journey trying to manage her kidney failure, she would eventually get a kidney from her sister in 2011.
Le Roux, now the chairperson of the Western Cape Transplant Sports Association, is one of the lucky ones. She spoke to Spotlight ahead of a trip to Germany to take part in the 2025 World Transplant Games.
“There are so many people that are on the list waiting for an organ and the waiting period, it can take many years,” she says.
Incomplete data
While there isn’t a coordinated, centralised database of everyone in South Africa who needs a lifesaving organ transplant, various groups do collect data. This is according to Professor David Thomson, an abdominal transplant surgeon and a critical care sub-specialist. Thomson is also the head of the Transplant Centre of Excellence Project at Groote Schuur Hospital in Cape Town.
“Various entities do collect levels of data, but it’s not very centralised and coordinated, and it could be better…we do have the renal registry that’s trying to track the number of people on dialysis, that’s a good source of information,” Thomson says. The Renal registry is a not-for-profit database that collects and publishes data on dialysis and transplant patients in the country. The database itself is an initiative of the South African Nephrology Society, an NPO that aims to further the field of nephrology and improve patient care.
The society estimates that in 2022, just over 9000 people across the public and private healthcare system were receiving “kidney replacement therapy” – which were either medications to help kidney function, dialysis or a kidney transplant.
A report by the South African Transplant society, an NPO that seeks to advance tissue and organ donation and transplantation, estimated that in 2021, across South Africa’s private and public hospitals, 2 586 people were on a waitlist for a lifesaving organ. Of those, 2382 people were waiting for a kidney, 52 needed a liver, 108 needed a heart transplant, and 44 were waiting for a lung.
But in the same year, the report recorded only 229 transplants done across the country.
South Africa does not have a good organ donation culture, says Professor Mignon McCulloch, the head of paediatric nephrology and solid organ transplant at the Red Cross War Memorial Children’s Hospital. In fact, according to McCulloch, and other experts we spoke to, South Africa has some of the lowest transplantation rates in the world.
While we couldn’t find any straightforward ranking system of organ donation rates, reports by the Global Observatory on Donation and Transplantation (GODT) do provide some insight into how some countries compare to one other. In 2017, according to data from the GODT cited in this 2020 study published in the South African Medical Journal, South Africa had 91 deceased donors, which is a rate of 1.6 per million. By contrast, Spain, which is regarded as having one of the highest rates of organ donation in the world, had 2183 deceased donors, a rate of 47.05 per million.
How it works
Organ donation is broadly classified into living donation and deceased donation.
There are two scenarios where someone can become an organ donor. The first, Thomson explains, is when a healthy person donates an organ without which they can live a normal life, like one of their kidneys. The second is when someone has been declared brain dead and is on a mechanical ventilator or when someone has experienced circulatory death -meaning their heart has stopped beating and “futile non-beneficial treatments have been stopped”. The latter is less common in South Africa.
For deceased donation from a brain-dead patient to take place, the potential donor needs to be in an ICU facility on a mechanical ventilator and referred by their clinical team to a transplant coordinator, says Thomson. If that person is eligible, then the transplant team has to get permission from the next of kin who ultimately have the final say even if the potential donor is registered as an organ donor.
“Organ donation can only happen if someone is on a mechanical ventilator in the end-of-life care pathway, so that is always a complicated and emotional discussion,” he says. “Tissue donations such as corneas, bones, skin, that can happen at the mortuary afterwards and there’s a slightly longer period for when these can be successfully recovered but all donation still requires you to have conversations with and get permission from grieving families.”
Juggling resources
McCulloch describes organ donation as being a bit like “a silent Cinderella”, until someone needs a lifesaving transplant, “and then people suddenly start asking questions about why, why don’t we have more transplantation?”
One reason for this is the allocation of resources and competing priorities within the healthcare system.
Thomson says that organ transplants are a “health intensive resource”, and it’s important to acknowledge that it exists in the context of an already overburdened healthcare system. There is a Deputy Director of dialysis and transplantation within the National Department of Health, Thomson explains, but there isn’t an “overarching central coordinating authority supporting deceased donation”. Instead, he says it is driven by hospital groups and within the provincial healthcare departments by healthcare workers
Adding to this, McCulloch says that doctors are always having to “juggle resources” and if there is only one bed available in an ICU, weighing up whether to give it to someone who will potentially become an organ donor or someone with pneumonia and will likely have a good outcome, is difficult.
Another challenge is the limited number of surgeons, physicians, and hospitals with the skill and equipment to perform an organ transplant. This strategy roadmap document by the South African Transplant Society list 21 transplants centres across the whole country – 14 of them offer kidney transplants, six offer heart transplants, four offer lung transplants, four offer liver transplants, and only one offers pancreas transplants.
Graphic of transplant centres in South Africa. (Source: Organ and Tissue Donation in South Africa – Creating a National Strategy Roadmap)
One can save seven
Earlier this year, an unused room in Tygerberg Hospital got a face-lift and a new purpose from a student-run medical non-profit. The initiative called Save7 was kickstarted by a conversation on kidney donation on Stellenbosch University’s Medical Campus. Its initial goal was to raise awareness, particularly among students, that one donor can save up to seven lives. And if tissue like corneas, heart valves, bone and skin are donated, one person can improve the lives of around 50 people.
Jonty Wright, who cofounded Save7, tells Spotlight that the organisation’s founding group of four has now grown to over 200 across multiple universities countrywide. Among others, the group created a Lifepod to solve a transplant-related problem at Tygerberg Hospital. Doctors and staff involved in transplantation at the hospital were citing competing resources as the reason behind low referral rates of potential organ donors by healthcare providers.
The solution posed by Save7, professors on the campus and some of the doctors involved with transplantation was to create a designated bed space for patients who are brain dead and are potential organ donors. The hope was that referrals for potential organ donations would be increased.
The room, Wright says, was an old minor operating theatre and storeroom that belonged to the orthopaedic surgery department and was situated in an ideal spot – in a corridor between the emergency medicine and trauma admissions.
Three of the Save7 co-founders, from left to right Jonty Wright, Suhayl Khalfey and Sachen Naidu. (Photo: Nasief Manie/Spotlight)
About three months ago, after fundraising efforts and backing by the Health Foundation and other partners, the Lifepod opened. The room currently holds a hospital bed, a ventilator on lease from the surgical department, vitals monitor, cardiac monitor, infusion pumps, emergency trolley, fridge, and crash cart. All the things needed to keep someone who is brain dead’s body comfortable and allow the doctors to counsel their loved ones about potentially donating their organs.
So far, according to Wright, referrals of potential candidates for organ donation at Tygerberg have gone up by 500%, but at the time of the interview none of the next of kin have consented to donating their loved one’s organs. (Data on this has not yet been published).
This ties onto another layer of complexity around organ donation, the reasons why next of kin don’t always give permission.
Need for better education
Samantha Nichols, the executive director of operations for the Organ Donor Foundation, an NGO advocating for organ donations, tells Spotlight that the problem isn’t so much a lack of awareness of organ donation, as a lack of good education around it. She says this affects everyone, including healthcare workers.
Nichols says that “it’s almost like the stars have to align” for a deceased donor to donate their organs, because of how many steps and doctors are involved in the process.
“[W]hen a person is sent to an ICU or trauma unit, the team of doctors that work on that person to save their life is a totally different team to the transplant team,” she says. A transplant team is only ever called in if a potential donor has been declared brain dead by two different doctors who aren’t part of or affiliated with a transplant team.
“[O]nly then can they start the process of talking to the family, and then they still need to get consent from the family before the organs are removed,” she says.
The Opt-in versus Opt-out debate
When it comes to consent for organ donation, South Africa has what is referred to as an opt-in system. An opt-in system means that someone must provide explicit consent of their desire to donate an organ. While an opt-out system means all adults are automatically considered organ donors after death, unless they explicitly withdraw consent beforehand.
There has been some debate about whether switching to opt-out systems would improve organ donation rates. One recent study, in which researchers analysed deceased donor rates in five countries that had switched from an opt-in to an opt-out system, did not find an increase in organ donation rates.
“Unless flanked by investments in healthcare, public awareness campaigns, and efforts to address the concerns of the deceased’s relatives, a shift to an opt-out default is unlikely to increase organ donations,” the researchers concluded.
A 2024 editorial in the Lancet medical journal made a similar point, saying “a simplistic switch to the ‘opt-out’ model is alone not sufficient to boost donation”. Instead, it lists the three components that makes Spain’s transplant programme so successful. “A solid legislative framework, strong clinical leadership, and a highly organised logistics network overseen by the National Transplant Organization.” An opt-out system is also unlikely to work well in South Africa from a legislative perspective, since it might be seen by some to impinge upon an “individual’s rights to personal autonomy and bodily and psychological integrity”, as argued in this article in the Conversation.
The experts Spotlight spoke to instead point to several other changes that could be made to improve donation rates.
‘Everyone can do a bit better’
The responsibility around improving organ transplantation rests on us as society and as a coordinated healthcare system, according to Thomson.
“[E]veryone can do a bit better…and I don’t think you want to make it one person’s responsibility for the performance. It’s actually a collective and how we work together,” Thomson says. “…a lot of things like supporting donation actually links into good palliative care services, and that should be something we’re offering to everyone.”
Thomson advocates for upskilling healthcare workers to be able to better counsel families during end-of-life care, not necessarily just around organ donation but around “engaging humanely with “families and end of life and navigating that complexity with them as the healthcare team”.
He recommends making counselling of grieving families and palliative care discussion a hospital system issue, instead of an individual responsibility by adding it to institutional operating standards. “And then you actually need to audit it, measure it, reflect on it and monitor the outcomes,” he says.
Suhayl Khalfey, a Save7 cofounder, says now that the Lifepod is ready to use, their focus is shifting to educate people about the importance of organ donation. As part of its education efforts, Khalfey says Save7 is putting together a database of different religious leaders to help counsel families uncertain about their faith’s stance on organ donation.
Nichols stresses that transplant teams will honour different religious beliefs and funeral practises and that a donor’s body will not appear disfigured in any way after they’ve donated their organs.
Start by having the conversation
Anyone can register as an organ donor with the Organ Donor Foundation, says Nichols. The process is free and will take less than a minute (see their website here). If a situation arises where you are brain dead and you are a candidate for organ donation your family will still need to give permission.
This is why it is so important to have the conversation with your loved ones about what your wishes are, says Khalfey.
Sachen Naidu, another cofounder of Save7, adds to this saying that often with the students they’ve spoken to, organ donation is viewed as something to think about in the distant future. He encourages young people to reconsider this mindset.
Even children can learn about organ donation.
The non-profit organisation Transplant Education for Living Legacies (TELL) recently launched an educational campaign in South Africa aimed at children in the 5 to 11 age group. The initiative, called the Orgamites Mighty Education Programme, is an international child health education programme originating from Canada. At its heart, the programme is a conversation starter, says Thomson who spoke on a TELL webinar.
“All we want is for people to be having educated conversations about it [organ donations],” he says. “Children need transplants too.”
For McCulloch, organ donation goes beyond impacting just the recipients. She uses the example of families who have lost a child in a tragic accident.
“You had a completely well child five minutes ago and then something terrible happened, and now you’ve got a child who’s died and you’re going to go home with a gap in your heart. Whereas at least when you donate [the] organs to another child, something good can come of out of a really hopeless, tragic situation,” she says.
Thomson adds to this saying: “And that’s a memory that lives with that family for a long time afterwards …not just that time point. That’s what they’re going to remember as part of that event, and it really does offer them a degree of solace for a tragedy.”
And the difference to those receiving organs can obviously be life changing. Receiving a kidney gave Le Roux the chance to see her children grow up. “So, every [milestone] when they wrote matric, when they got their degrees, everything. It’s like a step forward, something I can tick off, I’m still here. I’m able, I’m healthy,” she says.
By Christina Mooki, Head of Acquisition Operations at Merchant Capital
Pharmacies, especially ones in rural areas, are often the cornerstone of their communities. Beyond filling prescriptions, they provide medication, medical equipment, and counselling, sometimes serving as multi-service clinics in small towns and outlying areas. When people cannot wait weeks for a doctor’s appointment or need trusted advice, the local pharmacy is their first stop.
In many outlying areas, it is not just the most practical option, but often the only one. With the country’s high and rising burden of chronic disease, this role will only grow in importance.
The sector is indeed expanding. In just two years, 2020 and 2021, about 648 new community pharmacies opened across South Africa. By 2021, the total number stood at roughly 3580 outlets, and nearly 70% of these were independent rather than corporate-owned. That is over 2000 small businesses carrying community healthcare.
Christina Mooki, Head of Acquisition Operations at Merchant Capital
But every pharmacy is also a business. Behind the scenes, owners are juggling supplier deliveries, unpredictable supply chain issues, negotiating credit terms, paying staff, and trying to keep overheads under control. Balancing that with the responsibility of keeping communities healthy makes pharmacy ownership uniquely challenging and uniquely important.
Why more pharmacies are needed
A growing number of South Africans are living with chronic illness such as diabetes, hypertension, and HIV. These patients cannot miss their repeat medications and local pharmacy access becomes essential. Independent outlets do more than only dispense medicine, they also cut travel time, keep treatment within reach, and help build local economies.
Around the world, the role of a pharmacy is expanding. They are no longer limited to handing out prescriptions. According to Deloitte, many pharmacies are transforming into community health hubs by adding point-of-care testing, preventative health screening, and digital services to meet the changing expectations of modern consumers. Locally, they are also incorporating retail services to diversify their offerings further.
Running a pharmacy like a retailer
Passion for helping people will take you far as a pharmacist, but on its own, it will not keep the doors open. Independent pharmacies need to be run with the same discipline as any other retailer. Cash flow must be watched so staff are paid and suppliers are not left waiting. Shelves must carry the medicines that matter most without tying up money in products that sit for months. Costs like rent and electricity creep up quickly, and if unchecked, margins vanish.
Strong supplier relationships also make a difference. Paying on time, negotiating fairly, and keeping that trust intact can protect a business when times are tough. And like any other retailer, pharmacy owners have to be careful about how much debt they take on. Too much, too soon, can put even a busy store under pressure.
When these basics are in place, a pharmacy is not just a trusted point of care. It is also a resilient business that can think about growing, instead of simply surviving.
Where funding helps
Growth always asks for money before it offers returns. Anyone who has opened a second branch, hired staff, or added delivery knows this reality. The bills arrive first, and only later does the revenue follow. For a small independent owner working on thin margins, that can feel like a brick wall.
This is also the point where funding can be an enabler rather than a burden. At Merchant Capital, we treat pharmacies like retail businesses because that is what they are. They need capital that moves quickly, without red tape, and repayment models that flex with real turnover rather than with a rigid schedule. That flexibility gives owners breathing space, the confidence to back their instinct, invest in a new outlet, upgrade systems, or respond to their community.
Looking ahead
Independent pharmacies have already shown how vital they are to South Africa’s healthcare system. The next step is ensuring more of them open in the areas where they are most needed. With sound business management and access to the right kind of funding, these enterprises can grow their footprint, create jobs, and continue to provide reliable access to healthcare.
Sceletiumtortuosum is a little succulent plant that grows in the semi-arid Karoo and Namaqualand regions of South Africa. It has a long history of traditional use among the hunter-gatherers of the region.
The plant, known as kanna or kougoed by the San and Khoikhoi people, was mainly chewed or smoked to stay alert and suppress appetite during long hunts. The San were traditionally hunter-gatherers, while the Khoikhoi were pastoralists who herded livestock.
The name kanna (meaning “eland” in the click language of the San), has a symbolic reference to this large antelope, as the “trance animal”, which was called upon during religious and spiritual gatherings. Kougoed is Afrikaans for “something to chew”. The plant can be chewed after being dried and fermented, which is believed to intensify its effects.
The first colonial governor of the Cape colony, Simon van der Stel, in 1685 wrote about kanna in his journal:
They chew mostly a certain plant which they call Canna and which they bruise, roots as well as the stem, between the stones and store and preserve in sewn-up sheepskins.
I’m part of a group of scientists from different disciplines with an interest in this plant and we pooled our expertise to understand its effects on neurochemical concentrations in different parts of the brain.
Our studies were done in mice, so there is caution about establishing effectiveness on humans. Still, the results are striking.
As a chemist with an interest in natural products, I wanted to know which alkaloids in the plant were important in bringing about these effects.
Our latest study explored the effects of Sceletiumtortuosum extracts on mouse brain chemistry.
We found that Sceletium increased the levels of certain brain chemicals which may balance mood and reduce stress. These findings lend support to the calming and mood-enhancing use of this plant in traditional medicine.
Plant chemistry
Our study examined how extracts from different chemotypes of Sceletiumtortuosum can have different effects on brain chemistry. Chemotypes are groups of the same plant species that differ in the alkaloids they produce. This is because plants often produce alkaloids in response to external cues such as the weather or the presence of a plant-eating animal or pathogen.
Alkaloids are carbon-based compounds produced by plants. They are often toxic or taste bitter, making the plants less appealing or even harmful to the predators or invaders that want to eat or inhabit them. Alkaloids generally have physiological effects of use to humans. Some commonly used ones include caffeine, morphine and quinine.
We harvested two chemotypes of kanna from the Touwsrivier and De Rust regions of South Africa. These areas were chosen because of their interesting and unusual alkaloid profiles. The chemotypes were given to healthy mice as a supplement once a day for one month. The mice were monitored every day for behavioural or unexpected adverse reactions but none were noted.
At the end of the month, the levels of chemicals in the mouse brain were measured. Both the chemotypes were found to cause a marked increase in noradrenaline and a decrease in GABA in all brain regions studied. Both molecules are neurotransmitters that transmit nerve signals in the brain affecting memory, mood, attention and sleep.
This effect on noradrenaline supports kanna’s traditional use as an appetite suppressing drug. Increased noradrenergic stimulation is also the basis of many anti-depressants as well as drugs that improve attention and alertness.
We also found an impact on the brain chemicals serotonin and dopamine which may act together to balance mood and reduce stress. Serotonin affects emotional well-being and mood; dopamine motivates feelings of pleasure and satisfaction. These findings lend support to the calming and mood-enhancing use of this plant in traditional medicine.
Importantly, the control kanna extracts that did not have the interesting alkaloid profiles did not cause any of these chemical changes in the mouse brain.
Most studies on kanna have focused on the alkaloid mesembrine. The two specific chemotypes of kanna harvested from the Touwsrivier and De Rust regions of South Africa do have the mesembrine, but they are also packed with some other lesser-known or “minor” alkaloids. These differences in alkaloids may arise from a combination of geographic, environmental and inherent genetic factors found in a particular subset of plants.
Both the Touwsrivier and De Rust plants contained higher levels of alkaloids called mesembrine alcohols, which are different from mesembrine, and were barely present in the control extract. Another minor alkaloid, known as sceletium A4, was also identified as possibly being important. Mesembrine alcohols and sceletium A4 may be the ones responsible for the activity.
This suggests that the source of the plant, and the area in which it is grown, can influence its potential as a natural treatment for mood disorders and sleep.
What the results tell us
Stress, anxiety and depression pose a risk to the ability to lead a meaningful life. The World Health Organization has reported a 25% increase in anxiety and depression worldwide since the emergence of COVID-19.
Our study showed that the plant extracts had a broad noradrenergic effect in mice. But we have to be careful about making connections between results in mice and in humans. We need to explore the behavioural impact of these extracts in both mice and humans, especially in relation to sleep, alertness and mood.
The results also highlighted that without understanding the complex chemical composition of these plants, we risk overgeneralising their benefits, or worse, using them inappropriately.
Our findings have two implications.
First, they point towards a future of precision phytotherapy (use of plants for medicinal purposes), where natural remedies are tailored not just to individuals but to selecting certain plant chemotypes that produce certain combinations of alkaloids. Manipulating the growing conditions and genetic make-up of plants to optimise for alkaloid content is an age-old art.
Second, they remind us of the enormous, still largely untapped potential of African medicinal plants in global health innovation if we invest in research that honours both indigenous knowledge and scientific rigour.
As the world searches for safer, more sustainable ways to treat mental health conditions, South Africa’s kanna plant may hold secrets worth rediscovering.