Changing the amount of sweetness in a person’s diet has no impact on their liking for sweet foods, the results of a new trial suggest. The results also showed no difference in indicators of cardiovascular disease or diabetes risk between people who increased or decreased their intake of sweet-tasting foods over a six-month period.
The research team suggest that consequently public health organisations may need to change their current advice on reducing sweet food consumption to tackle the obesity crisis.
The study, published in the American Journal of Clinical Nutrition, was carried out by Wageningen University and Research in the Netherlands and Bournemouth University in the UK.
“People have a natural love of sweet taste which has led many organisations, including the World Health Organisation, to offer dietary advice on reducing the amount of sweetness in our diets altogether,” said Katherine Appleton, Professor in Psychology at Bournemouth University and corresponding author for the study. “However, our results do not support this advice, which does not consider whether the sweet taste comes from sugar, low calorie sweeteners, or natural sources.” she added.
During the trial, 180 participants were split into three groups. One group consumed a diet containing a high amount of sweet-tasting food, a second group consumed a low amount and a third consumed an average amount. The sweetness in the foods provided for their diets came from a combination of sugar, natural sweetness or low-calorie sweeteners.
After one, three and six months, participants were surveyed on whether their liking and perception of sweet foods had changed. They were also weighed and provided blood and urine samples to measure any changes in their diabetes risk and cardiovascular health.
At the end of the trial, the researchers found no significant differences in any of the measures across the three groups. Participants also reported a spontaneous return to their previous intake of sweet foods after the six months.
Based on their results, the study team are recommending that public health organisations may need to change their current advice on reducing sweet foods to tackle overweight and obesity.
“It’s not about eating less sweet food to reduce obesity levels,” Professor Appleton said. “The health concerns relate to sugar consumption. Some fast-food items may not taste sweet but can contain high levels of sugar. Similarly, many naturally sweet products such as fresh fruit and dairy products can have health benefits. Public advice therefore needs to concentrate on how people can reduce the amount of sugar and energy-dense foods they consume,” she concluded.
Underweight patients may face higher risk of poor outcomes after surgery
Source: Pixabay CC0
Higher BMI is not linked to increased risk of death or other complications following shoulder replacement surgery, according to a new study by Epaminondas Markos Valsamis from the University of Oxford, UK, and colleagues publishing November 20th in the open-access journal PLOS Medicine.
Joint replacement surgeries – including hip, knee and shoulder replacements – can significantly improve quality of life. Many patients with obesity are denied these procedures despite a lack of formal recommendations from national organisations. Evidence on the risks of joint replacement surgery in patients with obesity is limited and mixed.
In this study, researchers analysed more than 20 000 elective shoulder replacement surgeries performed across the UK and Denmark to see whether BMI was associated with death or other complications.
Compared to patients with a healthy BMI (21.75 kg/m2), patients with obesity (BMI 40 kg/m2) had a 60% lower risk of death within the year following surgery. Those considered underweight (BMI <18.5 kg/m2) had a slightly higher risk of death. The study does not support restricting patients with a high BMI from having elective shoulder replacement surgery, contrary to evidence that some hospitals are starting to restrict patients.
One main limitation of this study was the small sample size of the underweight population (131 for the UK data, 70 for the Denmark data). However, this was a large study that consistently showed a lower risk of death and complications in patients with obesity undergoing shoulder replacement surgery across multiple outcomes and two countries. The results can help patients, surgeons, and policymakers make informed decisions about who should be considered fit for these surgeries.
Lead author Epaminondas Markos Valsamis says, “Shoulder replacements offer patients the opportunity for excellent pain relief and improved quality of life. Our research shows that patients with a higher BMI do not have poorer outcomes after shoulder replacement surgery.”
Senior author Professor Jonathan Rees adds, “While BMI thresholds have been used to limit access to joint replacement surgery, our findings do not support restricting higher BMI patients from accessing shoulder replacement surgery.”
An illustration showing how Sirona works. Image credit: Oxford Medical Products
An innovative new pill could soon offer a new and affordable weight management treatment, following a successful clinical trial involving University of Bristol researchers and supported by the National Institute for Health and Care Research (NIHR). The results are published in the journal Obesity.
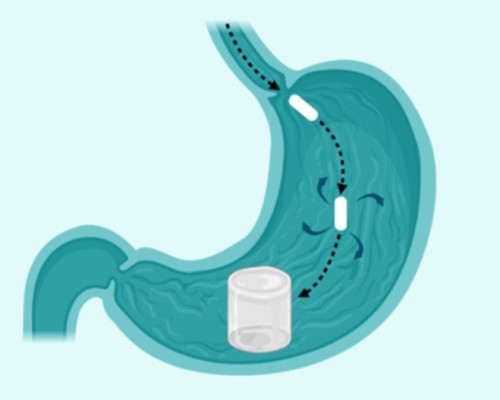
Sirona by Oxford Medical Products is a hydrogel-based pill that is designed to aid weight loss by reducing hunger. After it is swallowed, the pill expands in the stomach, leading to faster satiety. This helps individuals to eat less without needing strong medications or injections.
In the trial, funded by Innovate UK, participants lost up to 13.5% of their body weight in just six months. On average, people with class 1 obesity (BMI 30-35) lost 6.4% of their body weight.
Participants also ate on average 400 fewer calories per day compared to those taking a placebo. For context, recent Government-led research suggests that even a 216-calorie daily reduction could cut the UK’s obesity rate in half.
Mr Byrne, a consultant surgeon at University Hospital Southampton, said: “Obesity is a chronic and often progressive disease. With obesity rates continuing to rise, these results are an important step towards providing a different treatment option.
“This trial demonstrated Sirona could be a safe, affordable, and non-pharmacological treatment to support long-term weight management.”
Sirona will be accessible to anyone with a BMI 25-40, which means Sirona is particularly well-suited to help two key patient types. Firstly, for patients with an overweight BMI (25–30), allowing them to proactively manage their weight and to avoid progressing into obesity and the serious health problems it can bring. Secondly, it is suitable for use as an ‘off-ramp’ for GLP-1 users looking to come off treatment but prevent weight regain, which often occurs once GLP-1 medication ceases.
GLP-1 medications have become very popular for weight loss, with around 1.5 million users in the UK. However, a significant proportion of users pay out of pocket and prices have recently doubled in the UK for some doses of Mounjaro.
Camilla Easter, CEO of Oxford Medical Products, added: “GLP-1 medications perform an important role in helping those with a BMI in the obese range to lose weight and reduce weight-related health risks. There is, however, a real opportunity for a new style of treatment to work in a complementary way to GLP-1s, in a format that is significantly less expensive, and with better tolerability and therefore more accessible for the majority.
“Sirona has demonstrated amazing results during testing with UK hospitals, which have now been externally peer-reviewed. Next, we are setting sights on commercial UK release plans, targeting 2027 to make Sirona available.”
Sirona is a dual-polymer hydrogel pill. That means it’s made from two types of safe materials that expand in the stomach. It doesn’t use drugs or chemicals to change how your body works.
The pill was well tolerated during the 24-week study. There were no serious adverse events. Participants lost up to 13.5% of their body weight in just 24 weeks, and individuals with class 1 obesity (BMI 30-35) lost 6.4% of their body weight on average.
Importantly, no serious adverse events were reported during the trial. Sirona was well tolerated (95 percent of patients adhered to the dosing regimen at 12 weeks) and demonstrated a fantastic safety and side effect profile. This makes Sirona appropriate for patients who have struggled with adverse side effects when using GLP-1 medications.
OMP is planning a pivotal study in the UK and USA to further assess the effectiveness of Sirona and confirm these results. The novel weight loss treatment will aim for a 2027 UK commercial launch.
Mom’s genes play a larger role than dad’s in determining whether kids will be obese
A new study finds that kids with obesity are more likely to have obese parents because they inherit obesity-related genes, and to a smaller extent, are impacted indirectly by genes carried by the mother – even when those genes aren’t passed down. A new study led by Liam Wright of the University College London, UK, and colleagues, reports these findings August 5th in the open-access journal PLOS Genetics.
Studies commonly show that children with obesity often have parents with obesity, but the cause of this trend has been poorly understood. Children may inherit genes from their parents that increase their risk of obesity, or they could be shaped by conditions in the womb, or by the food and lifestyle choices their parents make.
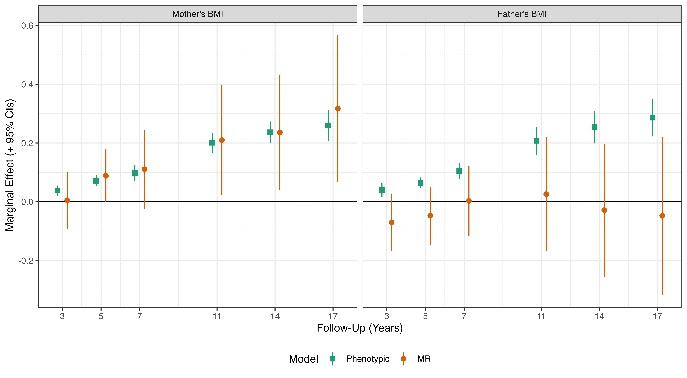
In the new study, researchers investigated the effects of the parents’ genetics on the weight and diet of their children. They looked at a measure of obesity called the body mass index (BMI), along with the diet and genetic data from more than 2500 mother-father-child trios. They focused on obesity related genes in the parents – both the ones that were directly passed down to their children, and the genes that weren’t, but that may indirectly impact weight by shaping the child’s environment, which are called genetic nurture effects. They found that, though mothers’ and fathers’ BMIs were consistently correlated with the child’s BMI, this trend could be mostly explained through the genes that children directly inherit. Genetic nurture effects from obesity-related genes in the mother that were not inherited had a smaller impact, only during the child’s adolescence.
The results suggest that a mother’s BMI may be particularly important for determining a child’s BMI, both due to the effects of genes that children directly inherit, and through indirect nurture effects from genes that weren’t passed down. Meanwhile, fathers had little impact on their child’s BMI, apart from the genes that were directly inherited. The study’s authors suggest that analyses that don’t consider the inherited genes are likely to give misleading estimates of the parents’ influence on a child’s weight.
The authors add, “Our results suggest mother’s weight could affect their children’s weight; policies to reduce obesity could have intergenerational benefits.”
Children born to obese mothers are at higher risk of developing metabolic disorders, even if they follow a healthy diet themselves. A new study from the University of Bonn published in the journal Nature offers an explanation for this phenomenon. In obese mice, certain cells in the embryo’s liver are reprogrammed during pregnancy. This leads to long-term changes in the offspring’s metabolism. The researchers believe that these findings could also be relevant for humans.
The team focused on the so-called Kupffer cells. These are macrophages that help protect the body as part of the innate immune system. During embryonic development, they migrate into the liver, where they take up permanent residence. There, they fight off pathogens and break down ageing or damaged cells.
“But these Kupffer cells also act as conductors,” explains Prof Dr Elvira Mass from the LIMES Institute at the University of Bonn. “They instruct the surrounding liver cells on what to do. In this way, they help ensure that the liver, as a central metabolic organ, performs its many tasks correctly.”
Changing the tune: From Beethoven to Vivaldi
It appears, however, that it is this conducting function that is changed by obesity. This is what mouse experiments carried out by Mass in cooperation with other research groups at the University of Bonn suggest. “We were able to show that the offspring of obese mothers frequently developed a fatty liver shortly after birth,” says Dr Hao Huang from Mass’s lab. “And this happened even when the young animals were fed a completely normal diet.”
The cause of this disorder seems to be a kind of “reprogramming” of the Kupffer cells in the offspring. As a result, they send out molecular signals that instruct the liver cells to take up more fat. Figuratively speaking, they no longer conduct one of Beethoven’s symphonies but rather a piece by Vivaldi.
This shift already seems to occur during embryonic development and is triggered by metabolic products from the mother. These activate a kind of metabolic switch in the Kupffer cells and change the way these cells direct liver cells in the long term. “This switch is a so-called transcription factor,” says Mass. “It controls which genes are active in Kupffer cells.”
No fatty liver without the molecular switch
When the researchers genetically removed this switch in the Kupffer cells during pregnancy, the offspring did not develop a fatty liver. Whether this mechanism could also be targeted with medication is still unclear. The teams now plan to investigate this in follow-up studies.
If new treatment approaches emerge from this, it would be good news. The altered behaviour of the Kupffer cells likely has many negative consequences. Fat accumulation in the liver, for example, is accompanied by strong inflammatory responses. These can cause increasing numbers of hepatocytes to die and be replaced with scar tissue, resulting in fibrosis. At the same time, the risk that hepatocytes degenerate and become cancerous increases.
“It is becoming ever more evident that many diseases in humans already begin at a very early developmental stage,” says Mass, who is also spokesperson for the transdisciplinary research area “Life & Health” and a board member of the “ImmunoSensation2” Cluster of Excellence at the University of Bonn. “Our study is one of the few to explain in detail how this early programming can happen.”
Intermittent energy restriction, time-restricted eating and continuous energy restriction can all improve blood sugar levels and body weight in people with obesity and type 2 diabetes, according to a study being presented Sunday at ENDO 2025, the Endocrine Society’s annual meeting in San Francisco, Calif.
“This study is the first to compare the effects of three different dietary interventions intermittent energy restriction (IER), time-restricted eating (TRE) and continuous energy restriction (CER) in managing type 2 diabetes with obesity,” said Haohao Zhang, PhD, chief physician at The First Affiliated Hospital of Zhengzhou University in Zhengzhou, China.
Although researchers identified improved HbA1c levels, and adverse events were similar across the three groups, the IER group showed greater advantages in reducing fasting blood glucose, improving insulin sensitivity, lowering triglycerides, and strengthening adherence to the dietary interventions.
“The research fills a gap in directly comparing 5:2 intermittent energy restriction with a 10-hour time-restricted eating in patients with obesity and type 2 diabetes. The findings provide scientific evidence for clinicians to choose appropriate dietary strategies when treating such patients,” Zhang says.
Zhang and colleagues performed a single-centre, randomised, parallel-controlled trial at the First Affiliated Hospital of Zhengzhou University from November 19, 2021 to November 7, 2024.
Ninety patients were randomly assigned in a 1:1:1 ratio to the IER, TRE or CER group, with consistent weekly caloric intake across all groups. A team of nutritionists supervised the 16-week intervention.
Of those enrolled, 63 completed the study. There were 18 females and 45 males, with an average age of 36.8 years, a mean diabetes duration of 1.5 years, a baseline BMI of 31.7kg/m², and an HbA1c of 7.42%.
At the end of the study, there were no significant differences in HbA1c reduction and weight loss between the IER, TRE and CER groups. However, the absolute decrease in HbA1c and body weight was greatest in the IER group.
Compared to TRE and CER, IER significantly reduced fasting blood glucose and triglycerides and increased the Matsuda index, a measure of whole-body insulin sensitivity. Uric acid and liver enzyme levels exhibited no statistically significant changes from baseline in any study group.
Two patients in the IER group and the TRE group, and three patients in the CER group, experienced mild hypoglycemia.
The IER group had the highest adherence rate (85%), followed by the CER group at 84% and the TRE group at 78%. Both the IER and CER groups showed statistically significant differences compared with the TRE group.
Zhang said these findings highlight the feasibility and effectiveness of dietary interventions for people who have obesity and type 2 diabetes.
A healthy lifestyle has important benefits, but weight alone might not give an adequate picture of someone’s health, say experts
Source: Pixabay CC0
Focusing solely on achieving weight loss for people with a high body mass index (BMI) may do more harm than good, argue experts in The BMJ.
Dr Juan Franco and colleagues say, on average, people with high weight will not be able to sustain a clinically relevant weight loss with lifestyle interventions, while the potential harms of weight loss interventions, including the reinforcement of weight stigma, are still unclear.
They stress that a healthy lifestyle has important benefits, but that weight alone might not give an adequate picture of someone’s health, and say doctors should provide high quality, evidence based care reflecting individual preferences and needs, regardless of weight.
Lifestyle interventions that focus on restricting an individual’s energy intake and increasing their physical activity levels have for many decades been the mainstay recommendation to reduce weight in people with obesity, explain the authors.
However, rigorous evidence has indicated that these lifestyle interventions are largely ineffective in providing sustained long term weight loss and reducing cardiovascular events (eg, heart attacks and strokes) or death.
Even though a healthy lifestyle provides important benefits, acknowledging that weight alone might not give an adequate picture of someone’s health, and recognising the limitations of lifestyle interventions for weight loss, could pave the way for more effective and patient centred care, they say.
Focusing on weight loss might also contribute to societal weight bias – negative attitudes, assumptions, and judgments about people based on their weight – which may not only have adverse effects on mental health but may also be associated with disordered eating, the adoption of unhealthy habits, and weight gain, they add.
They point out that recent clinical guidelines reflect the growing recognition that weight is an inadequate measure of health, and alternative approaches, such as Health at Every Size (HAES), acknowledge that good health can be achieved regardless of weight loss and have shown promising results in improving eating behaviours.
While these approaches should be evaluated in large clinical trials, doctors can learn from them to provide better and more compassionate care for patients with larger bodies, they suggest.
“Doctors should be prepared to inform individuals seeking weight loss about the potential benefits and harms of interventions and minimise the risk of developing eating disorders and long term impacts on metabolism,” they write. “Such a patient centred approach is likely to provide better care by aligning with patient preferences and circumstances while also reducing weight bias.”
They conclude: “Doctors’ advice about healthy eating and physical activity is still relevant as it may result in better health. The main goal is to offer good care irrespective of weight, which means not caring less but rather discussing benefits, harms, and what is important to the patient.”
For many, fitness trackers have become indispensable tools for monitoring how many calories they’ve burned in a day. But for those living with obesity, who are known to exhibit differences in walking gait, speed, energy burned and more, these devices often inaccurately measure activity – until now.
Scientists at Northwestern University have developed a new algorithm that enables smartwatches to more accurately monitor the calories burned by people with obesity during various physical activities.
The technology bridges a critical gap in fitness technology, said Nabil Alshurafa, whose Northwestern lab, HABits Lab, created and tested the open-source, dominant-wrist algorithm specifically tuned for people with obesity. It is transparent, rigorously testable and ready for other researchers to build upon. Their next step is to deploy an activity-monitoring app later this year that will be available for both iOS and Android use.
“People with obesity could gain major health insights from activity trackers, but most current devices miss the mark,” said Alshurafa, associate professor of behavioral medicine at Northwestern University Feinberg School of Medicine.
Current activity-monitoring algorithms that fitness trackers use were built for people without obesity. Hip-worn trackers often misread energy burn because of gait changes and device tilt in people with higher body weight, Alshurafa said. And lastly, wrist-worn models promise better comfort, adherence and accuracy across body types, but no one has rigorously tested or calibrated them for this group, he said.
“Without a validated algorithm for wrist devices, we’re still in the dark about exactly how much activity and energy people with obesity really get each day — slowing our ability to tailor interventions and improve health outcomes,” said Alshurafa, whose team tested his lab’s algorithm against 11 state-of-the-art algorithms designed by researchers using research-grade devices and used wearable cameras to catch every moment when wrist sensors missed the mark on calorie burn.
The findings will be published June 19 in Nature Scientific Reports.
The exercise class that motivated the research
Alshurafa was motivated to create the algorithm after attending an exercise class with his mother-in-law who has obesity.
“She worked harder than anyone else, yet when we glanced at the leaderboard, her numbers barely registered,” Alshurafa said. “That moment hit me: fitness shouldn’t feel like a trap for the people who need it most.”
Algorithm rivals gold-standard methods
By using data from commercial fitness trackers, the new model rivals gold-standard methods of measuring energy burn and can estimate how much energy someone with obesity is using every minute, achieving over 95% accuracy in real-world situations. This advancement makes it easier for more people with obesity to track their daily activities and energy use, Alshurafa said.
How the study measured energy burn
In one group, 27 study participants wore a fitness tracker and metabolic cart – a mask that measures the volume of oxygen the wearer inhales and the volume of carbon dioxide the wearer exhales to calculate their energy burn (in kilocalories/kCals) and resting metabolic rate. The study participants went through a set of physical activities to measure their energy burn during each task. The scientists then looked at the fitness tracker results to see how they compared to the metabolic cart results.
In another group, 25 study participants wore a fitness tracker and body camera while just living their lives. The body camera allowed the scientists to visually confirm when the algorithm over- or under-estimated kCals.
At times, Alshurafa said he would challenge study participants to do as many pushups as they could in five minutes.
“Many couldn’t drop to the floor, but each one crushed wall-pushups, their arms shaking with effort,” he said, “We celebrate ‘standard’ workouts as the ultimate test, but those standards leave out so many people. These experiences showed me we must rethink how gyms, trackers and exercise programs measure success – so no one’s hard work goes unseen.”
Health workers have long relied on Body Mass Index as a way to measure whether people are within a healthy weight range. Now, a collection of top researchers have made the case for a new way to understand and diagnose obesity. In part two of this special Spotlight series, we take a look at what this new framing might mean for South Africa.
If we are going to tackle the global rise in obesity, our understanding of the condition needs to change. That is according to a Lancet Commission convened by a global group of 58 experts from different medical specialties. While we have historically thought of obesity as a risk factor for other diseases like diabetes, the commission’s recent report published in the journal Lancet Diabetes and Endocrinology concludes that obesity is sometimes better thought of as a disease itself – one that can directly cause severe health symptoms (see part one of this series for a detailed discussion of this argument).
By categorising obesity as a disease, public health systems and medical aid schemes around the world would be more likely to cover people for weight-loss drugs or weight-loss surgery, according to the report. At present, these services are often only financed if a patient’s obesity has already led to other diseases. This is given that obesity is not viewed as a stand-alone chronic illness.
But if we’re going to redefine obesity as a disease, or at least some forms of it, then we need good clinical definitions and ways to measure it. For a long time, this has posed challenges, according to the Lancet report.
The perils of BMI
At present, health workers often rely on Body Mass Index (BMI) to gauge whether a patient is within a healthy weight range. BMI is measured by taking a person’s weight in kilograms and dividing it by their height in meters squared.
A healthy weight is typically considered to be between 18.5 and 25. A person whose BMI is between 25 and 30 is considered to be overweight, while someone with a BMI of over 30 is considered to have obesity. But according to the Lancet report, this is a crude measure, and one which provides very little information about whether a person is actually ill.
One basic issue is that a person can have a high BMI even if they don’t have a lot of excess fat. Instead, they may simply have a lot of muscle or bone. Indeed, the report notes that some athletes are in the obese BMI range.
Even when a high BMI does indicate that a person has obesity, it still doesn’t tell us where a person’s fat is stored and this is vital medical information. If excess fat is stored in the stomach and chest, then it poses more severe health risks than when it is stored in the limbs or thighs. This is because excess fat will do more harm if it surrounds vital organs.
The lead author of the Lancet report, Professor Frances Rubino, says that the pitfalls of BMI have long been understood, but practitioners have continued to use it.
“BMI is still by and large the most used approach everywhere, even though medical organisations have [raised issues] for quite some time,” he tells Spotlight.
“The problem is that even when we as individuals or organisations say BMI is no good, we haven’t provided an alternative. And so, inevitably, the ease of calculating BMI and the uncertainties about alternatives makes you default back to BMI.”
To deal with this problem, the report advocates for several alternative techniques for measuring obesity which offer more precision.
The first option is to use tools that directly measure body composition like a DEXA scanner. This is a sophisticated x-ray machine which can be used to distinguish between fat, bone and muscle. It can also be used to determine where fat is concentrated. It’s thus a very precise measurement tool, but the machines are expensive and the scans can be time-consuming.
Alternatively, the report recommends using BMI in combination with another measure like waist-to-hip ratio, waist-to-height ratio or simply waist circumference. If two of these alternative measures are used, then BMI can be removed from the picture.
These additional metrics are clinically useful because they provide information about where fat is stored. For instance, a larger waistline inevitably indicates a larger stomach. Indeed, studies have found that above a certain level, a larger waist circumference is linked to a higher chance of dying early, even when looking at people with the same BMI.
The report thus offers a more accurate way to measure obesity in the clinical setting. But its authors argue that this is only the first step when making a diagnosis. The second is to look at whether a patient’s obesity has actually caused health problems as this isn’t automatically the case. They acknowledge for instance that there are some people with obesity who “appear to be able to live a relatively healthy life for many years, or even a lifetime”.
The report refers to these cases as “preclinical obesity”. Such patients don’t have a disease as such, according to the report, but still have an increased risk of facing health issues in the future. As such, the report’s authors argue that they should be monitored and sometimes even treated, depending on factors like family history.
By contrast, cases of obesity which have directly caused health problems are referred to as “clinical obesity”. These cases, according to the report, should be treated immediately just like any other serious disease. It lists a series of medical symptoms associated with clinical obesity that would allow health workers to make an appropriate diagnosis.
The recommendation is thus for health workers to determine whether a person has obesity through the metrics listed above, and then to determine whether it is clinical or preclinical by evaluating a patient’s symptoms. This will inevitably guide the treatment plan.
How does this relate to SA?
Professor Francois Venter, who runs the Ezintsha research centre at WITS university, says the Lancet report offers a good starting point for South Africa, but it has to be adapted for our own needs and context.
“It’s a big step forward from BMI which grossly underdiagnoses and overdiagnoses obesity,” says Venter, who adds that additional metrics like waist circumference are a “welcome addition”.
The view that clinical obesity is a disease that needs to be immediately treated is also correct, according to Venter. Though he adds that the public health system in South Africa is not in a financial position to start handing out weight-loss medicine to everyone who needs it.
“The drugs are hugely expensive,” says Venter, “and they have side effects, so you need a lot of resources to support people taking them.” But while it may not yet be feasible to treat all cases of clinical obesity in South Africa, Venter believes we should use the diagnostic model offered by the Lancet Commission to begin identifying at least some people with clinical obesity so that they can begin treatment.
“You have to start somewhere, and for that you need a good staging system,” he says. “Let’s use the Lancet Commission and start to see if we can identify a few priority people and screen them and start to work on the drug delivery system.”
Yet while Venter believes that the commission makes important contributions, he also cautions that we need more data on obesity in Africa before we can apply all of its conclusions to our own context.
“If you go to the supplement of the Lancet Commission, there’s not a single African study there. It all comes from Europe, North America and Asia. It’s not the commission’s fault but [there is a lack of data on Africa].”
This is important as findings that apply to European or Asian populations may not necessarily hold for others. Consider the following case.
As noted, the commission states that BMI is not sufficient to determine whether someone is overweight and must therefore be complemented with other measures. But it states that if someone’s BMI is above 40 (way above the current threshold for obesity), then this can “pragmatically be assumed” without the need for further measures.
But this may not hold in Africa, says Venter.
“The commission says that if your BMI is over 40, which is very big, you can infer that this person has got obesity and they are sick and need to lose weight. I don’t know if we can say that in Africa, where we often have patients who are huge, and yet they are very active, and when you [look at] their blood pressure and all their metabolics, they’re actually pretty healthy,” he notes. “So, I think they’re sometimes jumping to conclusions about African populations that we don’t have data on,” adds Venter.
Is South Africa ready to move past BMI?
Another concern is that while the Lancet Commission may offer useful recommendations for advanced economies, its starting assumptions may not be as relevant for countries like South Africa.
For instance, while specialists agree that BMI is a crude measure of obesity, direct measures like DEXA scans are “out of our reach economically”, according to Professor Susan Goldstein, who leads PRICELESS-SA, a health economics unit at the South African Medical Research Council.
And while supplementing BMI with the other metrics like waist circumference may be doable, health experts told Spotlight that at present healthcare workers in South Africa aren’t even measuring BMI alone.
Dr Yogan Pillay, a former deputy director-general at the national health department who now runs TB and HIV delivery at the Gates Foundation, told Spotlight: “I can’t tell you how few people in the public sector have their BMI monitored at all. Community health workers are supposed to be going out and measuring BMI, but even that’s not happening”.
Goldstein also suggests that the monitoring of BMI in South Africa is limited. “If you go into the clinic for your blood pressure, do they say: ‘How’s your BMI?’ No, I doubt that,” says Goldstein. “It’s just not one of the measures that [gets done].”
She adds that South Africa could introduce the combination of metrics proposed by the commission, like waist circumference combined with BMI, but says it would simply require “a lot of re-education of health workers”.
Prevention vs treatment
For Goldstein, the commission is correct to regard clinical obesity as a disease which needs to be treated, but we also shouldn’t view medication as the only way forward.
“We have to remember that prevention is very important,” says Goldstein. “We have to focus on food control, we have to look at ultra-processed foods, and unless we do that as well [in addition to medication] we are going to lose this battle.”
The National Health Department already has a strategy document for preventing obesity, but some of its recommendations have been critiqued for focusing on the wrong problems. For instance, to prevent childhood obesity, the strategy document recommends reforming the Life Orientation curriculum and educating tuck shop vendors so that both students and food sellers have more information about healthy eating. But as Spotlight previously reported, there are no recommendations to subsidise healthy foods or to increase their availability in poor areas, which several experts believe is more important than educational initiatives.
Venter also highlights the importance of obesity prevention, though he emphasises that this shouldn’t be in conflict with a treatment approach – instead, we need to push for both.
“The [prevention] we need to do is fix the food supply… and the only way you do that is to decrease the cost of unprocessed food.” But while this may help prevent future cases of obesity, it doesn’t help people who are already suffering from obesity, says Venter. And since such people comprise such a large share of the population, we can’t simply ignore them, he says.
“Even if you fix the entire food industry tomorrow, those [people who are already obese] are going to remain where they are because simply changing your diet isn’t going to do diddly squat [when you already have obesity],” he adds. (Part 1 discusses this in more detail).
Goldstein adds that increasing access to treatment would also inevitably reduce the costs of “hypertension, diabetes, osteoarthritis, and a whole range of other illnesses if it’s properly managed”.
One way to advance access to medication would be for the government to negotiate reduced prices of GLP-1 drugs, she says. (Spotlight previously reported on the prices and availability of these medicines in South Africa here.)
Funding
A final concern that has been raised about the Lancet commission is about its source of funding.
“I don’t know how one gets around this,” says Goldstein, “but there were 58 experts on the commission, 47 declared conflicts of interest.”
Indeed, the section of the commission that lists conflicts of interest spans over 2 000 words (roughly the size of this article). This includes research grants and consulting fees from companies like Novo Nordisk and Eli Lilly, which produce anti-obesity drugs.
In response, Rubino told Spotlight that “people who work in the medical profession obviously work and consult, and the more expertise they have, the more likely they are to be asked by somebody to advise. So sometimes people have contracts to consult a company – but that doesn’t mean that they necessarily make revenue if the company has better sales. You get paid fees for your services as a consultant”.
Rubino says this still has to be declared as it may result in some bias, even if it is unconscious, but “if you wanted to have experts who had zero relationship [to companies] of any sort then you might have to wonder if there is expertise available there… the nature of any medical professional is that the more expertise they have, the more likely that they have engaged in work with multiple stakeholders”.
For Venter, there is some truth to this. “It’s very difficult to find people in the obesity field that aren’t sponsored by a drug company,” he says. “Governments don’t fund research… and everyone else doesn’t fund research. Researchers go where the research is funded.”
This doesn’t actually solve the problem, says Venter, as financing from drug companies can always influence the conclusions of researchers. It simply suggests that the problem is bigger than the commission. Ultimately, he argues that the authors should at least be applauded for providing such granular details about conflicts of interest.
Rubino adds that while researchers on the commission may have historically received money from drug companies for separate research studies or consulting activities, none of them received money for their work on the commission itself.
“This commission has been working for more than four years since conception… An estimate of how many meetings we had is north of 700, and none of us have received a single penny [for doing this],” he says.
Disclosure: The Gates Foundation is mentioned in this article. Spotlight receives funding from the Gates Foundation but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council.
Eating a high-fat diet containing a large amount of oleic acid – a type of fatty acid commonly found in olive oil – could drive obesity more than other types of dietary fats, according to a study published in the journal Cell Reports.
The study found that oleic acid, a monounsaturated fat associated with obesity but also tentatively linked to cardiovascular benefits and often touted as a ‘healthy’ fatty acid, causes the body to make more lipid cells. By boosting a signalling protein called AKT2 and reducing the activity of a regulating protein called LXR, high levels of oleic acid resulted in faster growth of the precursor cells that form new lipid cells.
“We know that the types of fat that people eat have changed during the obesity epidemic. We wanted to know whether simply overeating a diet rich in fat causes obesity, or whether the composition of these fatty acids that make up the oils in the diet is important. Do specific fat molecules trigger responses in the cells?” said Michael Rudolph, PhD, assistant professor of biochemistry and physiology at the University of Oklahoma College of Medicine.
Rudolph and his team fed mice a variety of specialised diets enriched in specific individual fatty acids, including those found in coconut oil, peanut oil, milk, lard and soybean oil. Oleic acid was the only one that caused the precursor cells that give rise to fat cells to proliferate more than other fatty acids.
“You can think of the fat cells as an army,” Rudolph said. “When you give oleic acid, it initially increases the number of ‘fat cell soldiers’ in the army, which creates a larger capacity to store excess dietary nutrients. Over time, if the excess nutrients overtake the number of fat cells, obesity can occur, which can then lead to cardiovascular disease or diabetes if not controlled.”
Unfortunately, it’s not quite so easy to isolate different fatty acids in a human diet. People generally consume a complex mixture if they have cream in their coffee, a salad for lunch and meat and pasta for dinner. However, Rudolph said, there are increasing levels of oleic acid in the food supply, particularly when access to food variety is limited and fast food is an affordable option.
“I think the take-home message is moderation and to consume fats from a variety of different sources,” he said. “Relatively balanced levels of oleic acid seem to be beneficial, but higher and prolonged levels may be detrimental. If someone is at risk for heart disease, high levels of oleic acid may not be a good idea.”